
Abstract
Using chromium and nickel for electroplating is important in many industries. This process induces variable adverse health effects among exposed workers. The aim of this study is to detect the genotoxic effects of combined exposure to chromium and nickel among electroplating workers. This study was conducted on 41 male workers occupationally exposed to chromium and nickel in the electroplating section of a factory compared to 41 male nonexposed individuals, where full history and clinical examination were performed. Laboratory investigations included measurement of serum chromium, nickel, 8-hydroxydeoxyguanosine (8-OHdG), and micronuclei were measured in buccal cells. In exposed workers, serum chromium ranged from 0.09 to 7.20 µg/L, serum nickel ranged from 1.20 to 28.00 µg/L, serum 8-OHdG ranged from 1.09 to12.60 ng/mL, and these results were statistically significantly increased compared to nonexposed group (P < 0.001). Electroplaters showed higher frequencies of micronuclei in buccal cells when compared to nonexposed (ranged from 20.00 to 130.00 N/1,000 versus 2.00 to 28.00 N/1,000; P < 0.001). Linear regression models were done to detect independent predictors of 8-OHdG and micronucleus test by comparing exposed and nonexposed groups. The model found that exposure to chromium and nickel increases serum 8-OHdG by 4.754 (95% confidence interval [CI]: 3.54-5.96). The model found that exposure to chromium and nickel increases micronucleus by 35.927 (95% CI: 28.517-43.337). Serum 8-OHdG and micronucleus test in buccal cells were increased with combined exposure to chromium and nickel. The current research concluded that workers exposed to nickel and chromium in electroplating industry are at risk of significant cytogenetic damage.
Introduction
Electroplating is essential in various industries as it generally improves the mechanical and the chemical properties of the metal used, by increasing hardness, wear, and corrosion resistance of the metal. Using chromium and nickel in electroplating to prevent corrosion is important in many industries. 1 Workers can be exposed to hexavalent chromium (Cr [VI]) and nickel mostly through inhalation and dermal routes of exposure, which is associated with carcinogenicity and genotoxicity, especially in chronic exposures leading to lung cancers. 2 Chromium genotoxicity is mediated partly through reactive intermediates and oxidative reactions during intracellular reduction of Cr (VI) to trivalent chromium (Cr [III]) that is the final product. It forms complexes with peptides, proteins, and DNA, resulting in DNA–protein cross-links, DNA strand breaks, and alterations in cellular signaling pathways, which may contribute to toxicity and carcinogenicity of chromium compounds. 3 Regarding nickel, protein seems to be the primary target for nickel insult. Nuclear protein damage caused by nickel reduces the enzyme activity needed for DNA replication, transcription, recombination, and repair. It causes an increase in levels of endogenous cellular hydrogen peroxides and short-lived reactive oxygen species, which leads to oxidative DNA damage. 4 The International Agency for Research on Cancer classified hexavalent chromium and nickel compounds as group 1, carcinogenic to humans. Indeed, both short- and long-term exposure to chromium and nickel can cause several health problems, including respiratory and dermatological effects. 5 The micronucleus test in buccal mucosa is a potentially excellent biomarker that detects chromosomal loss or malfunction of the mitotic spindle. It has been accepted as a reliable biomarker of genotoxicity in occupationally exposed groups. 6 The 8-hydroxydeoxyguanosine (8-OHdG) is a major product of oxidative DNA damage and is frequently analyzed in the biological fluids as a biomarker of cellular oxidative stress related to carcinogenesis in clinical, 7 environmental, 8 and occupational settings. 9 Previous studies 10,11 were done to evaluate the relationship between chromium as a single exposure, urinary 8-OHdG, and micronucleus test in the chromate-exposed group. However, their conclusion has yielded conflicting results. Other studies 12 –14 have shown the cytogenetic effects in different populations having combined exposure to chromium and nickel.
There are limited studies 15,16 regarding the genotoxic effects of combined exposure to chromium and nickel in the electroplating industry. Most of these studied concentrated on cytogenetic points in the form of sister chromatid exchange, chromosomal aberrations, DNA strand breakages, DNA–protein cross-links, comet assay, and micronuclei in peripheral blood lymphocytes (PBL) that are relatively time-consuming tests. Therefore, the present study aimed at detection of the genotoxic effects of combined exposure to chromium and nickel, for early detection and better management of cancer. The research investigated the potential use of serum 8-OHdG as an indicator of oxidative DNA damage and micronucleus test in buccal cells as a screening test denoting chromosomal damage among the exposed workers to nickel and chrome in the electroplating industry.
Participants and Methods
The Study Population
A comparative cross-sectional analytical study was conducted in a major factory in Helwan, Cairo, Egypt, that contains many sectors; one of these is the electroplating sector where chromium and nickel are used. The study was performed during the period from February 2015 to April 2015. The study population comprised 2 groups: an exposed and a nonexposed group. Both groups were matched through selection criteria in the preparation phase of this study, restricting participants in this study to a certain age interval between 25 and 59 years (the age of working individuals at the factory). There was no female working at this section of the factory (exposed), so the unexposed were chosen to be males. The exposed group included 45 male workers who were the working population in the electroplating sector of the factory. Four workers were excluded according to the present exclusion criteria as 3 of them had chest X-ray 1 month before the study was conducted and 1 refused to do the micronucleus test. Inclusion criteria were all workers exposed to chromium and nickel in electroplating section for at least the preceding 2 years. Exclusion criteria for both exposed and nonexposed groups were workers who were exposed to any source of radiation in the preceding 3 months and alcohol consumers. Those having any chronic illness as cardiovascular, liver diseases, or receiving antioxidant drugs during the preceding 6 months were also excluded. The nonexposed control group included 41 male workers in the administration departments of the same factory, who have never been occupationally exposed to chromium or nickel.
Methods
The Ethical Committee of the Occupational and Environmental Medicine Department, Cairo University, approved the study, and then, an official approval from the factory authority to perform this study was obtained. The study was performed hand in hand with the annual periodic medical examination that was conducted by the Egyptian General Organization for Health Insurance. A written consent to participate in the study and an approval to give blood samples from each individual were obtained after explaining to them the aim and the importance of the study. In the study, the ethical guidelines of good clinical practices (GCP) have been explained. Strict confidentiality was observed throughout sample collection, coding, testing, and recording of the results. The studied groups were subjected to a specially designed detailed questionnaire including sociodemographic data including age, residence, smoking habits, present, past, and family history. Occupational history included current job and its nature, previous jobs, duration of employment in years, and using protective equipment or not. Health complaints were onset, duration, and relation to work. Upper respiratory tracts symptoms as headache accompanied by rhinorrhea, sneezing, and epistaxis and whether these symptoms are related to the exposure during the workday or not. Lower respiratory tract symptoms including cough, expectoration, dyspnea, and chest wheezes and whether these symptoms worsen over the workday and if improvement occurs on weekends and holidays. History of any skin complaint were irritation, pigmentation, eruption, its extent, distribution, onset, course, duration, effect of the weekends, using of protective measures, and if there was any treatment given or not. The nasal examination was done to detect nasal septal ulceration and perforation which results from chronic exposure to chromium and nickel. None of the workers was found to have any of these nasal lesions. The study was conducted using face-to-face interviews in the local language of the country.
Laboratory Investigations
From each participant, a sample of 5 mL of venous blood was taken using a dry plastic disposable syringe under complete aseptic condition. Three mL of blood was kept in a tube, allowed to clot, and then centrifuged for separation of the serum for determination of chromium and nickel. Two mL of blood was delivered in a tube containing dipotassium EDTA mixed promptly for determination of 8-OHdG. All samples were transported to the laboratory on the same day within 2 hours to be analyzed.
Determination of serum chromium and nickel
The serum chromium and nickel levels were measured by graphite furnace atomic absorption spectrophotometer with Zeeman background correction (Thermo elemental M6, Cambridge, England). External calibrators for chromium and nickel were used for plotting standards curves from which the concentration of each metal was interpreted. 17
Determination of serum 8-OHdG
Serum 8-OHdG was measured using a competitive enzyme-linked immunosorbent assay (ELISA) kit (My BioSource Inc, San Diego, California). The standard curve is used to determine the concentrations in the samples. A standard curve is plotted to relate the intensity of the color to the concentration of standards. The 8-OHdG concentration in each sample is interpolated from this standard curve. 18
Determination of micronucleus test in buccal mucosal cells
Each individual was asked to thoroughly rinse his oral cavity using an antiseptic mouthwash; after that, a small headed toothbrush was used to scrap against the inside cheeks several times in a circular movement. The head of the brush was put in a sterile 50-mL tube containing 10 mL phosphate-buffered saline (PBS) solution. The samples were immediately transferred to the laboratory within 2 or 3 hours for further handling. The procedure was done according to Thomas et al, 19 and the tubes were centrifuged at 1,500 rpm for 15 minutes. The cell pellet was transferred to a 15-mL falcon tube, and hypotonic solution (0.56 g potassium chloride dissolved in 100 mL distilled water) was added to the pellet, mixed well, and incubated for 3 hours at 37°C. The cells were then washed with fresh fixative (3:1 methanol and acetic acid) and then centrifuged. The supernatant was discarded and about 5 mL fixative was added to the cell pellet, mixed, and centrifuged. This was repeated 3 times before suspending in about 1 mL fresh fixative depending on the cell pellet size. Approximately 100-µL cell suspension was applied to each clean microscopic glass slide. Staining was done by Giemsa stain for 5 minutes, and 4′, 6-DiAmidino-2-PhenylIndole (DAPI) stain for 3 minutes. Slides were then placed on a slide tray and allowed to dry for about 10 to 15 minutes. Coverslips were then applied to the slides after complete dryness. The mounting medium is PBS solution. Slides were then stored in slide boxes at room temperature. Cells were scored manually according to the criteria provided by Fenech et al. 20 Only 2 persons scored the samples that are labeled with a code number, without knowing if each sample is for a case or a control. Slides were examined at 400 and 1,000 magnifications using a light microscope or a fluorescent microscope. A total of 1,000 normal differentiated cells per individual were analyzed. The frequency of micronucleus (%) was calculated. Photographs of the slides were taken by Zeiss image analyzing system.
Statistical Analysis
Data obtained from the study were coded and entered using the statistical package SPSS version 16. The mean values, standard deviations, median, and ranges were estimated for quantitative variables; qualitative data were represented as frequencies and percentages. Comparisons between exposed and nonexposed groups were carried out using independent sample t test for quantitative variables, which were normally distributed. Nonparametric Mann-Whitney U test was used for quantitative variables, which were not normally distributed. For comparing qualitative variables, χ2 test was performed. Fisher exact test was used when the expected frequency is less than 5. The correlations between individual variables were calculated using Spearman correlation coefficient, P values <0.05 were considered statistically significant, and P values >0.05 were not considered statistically significant. Linear regression models were done to detect independent predictors of 8-OHdG and micronucleus test by comparing exposed and nonexposed groups.
Results
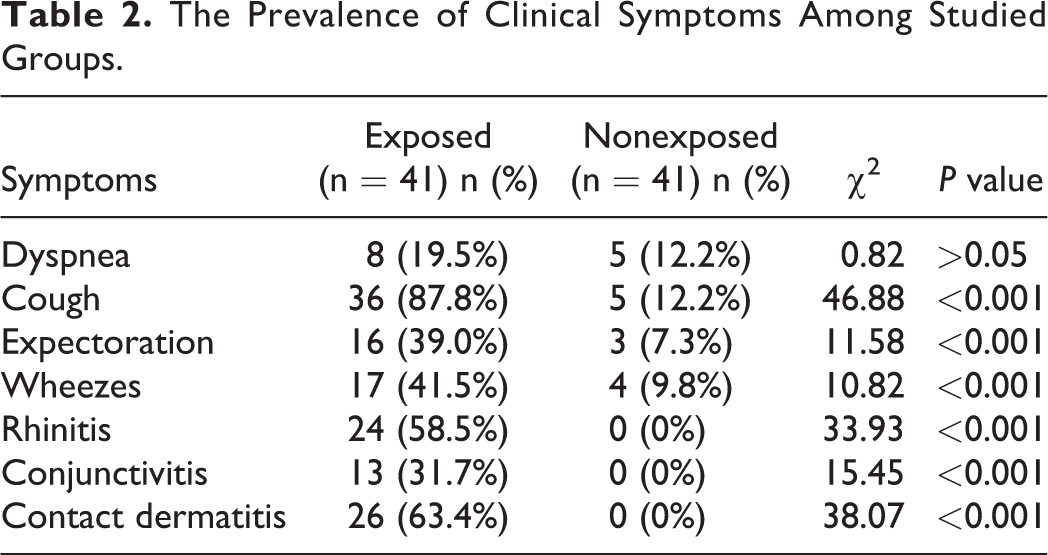
Table 1 showed nonstatistically significant differences among exposed and nonexposed groups as regards demographic characteristics. Table 2 shows the health complaints, clinical symptoms, and signs encountered due to exposure to both chromium and nickel during the electroplating process. The prevalence of a cough, expectoration, wheezes, rhinitis, conjunctivitis, and contact dermatitis was statistically significant higher among the exposed workers (Table 2). There were statistically significant increased levels of serum chromium, serum nickel, serum 8-OHdG, and micronuclei counts among exposed participants compared to the nonexposed group (Table 3). The frequency of using personal protective equipment (PPE; gloves, goggles, aprons) during shift work showed that 14 (34.1%) of exposed workers used PPE (Table 3). There was a statistically significant decrease in the levels of serum chromium and nickel among users of PPE. Regarding serum levels of 8-OHdG and buccal micronucleus test, they were decreased but the difference did not reach the level of statistical significance (Table 3). No correlations between different variables among exposed workers were found except for the statistically positive correlation between chromium and nickel (r = 0.37; P < 0.05). A statistically significant positive correlation was observed between serum chromium and micronucleus test in the exposed group for work duration more than 20 years, (r = 0.35; P < 0.05). For micronuclei counts, regression model Durbin-Watson estimate = 2.110. The Durbin-Watson estimate ranges from 0 to 4. Values hovering around 2 showed that the data points were independent. Values near 0 mean strong positive correlations and 4 indicates strong negative. For serum 8-OHdG, regression model Durbin-Watson estimate = 2.251 (Table 4).
Demographic Characteristics of the Studied Groups.
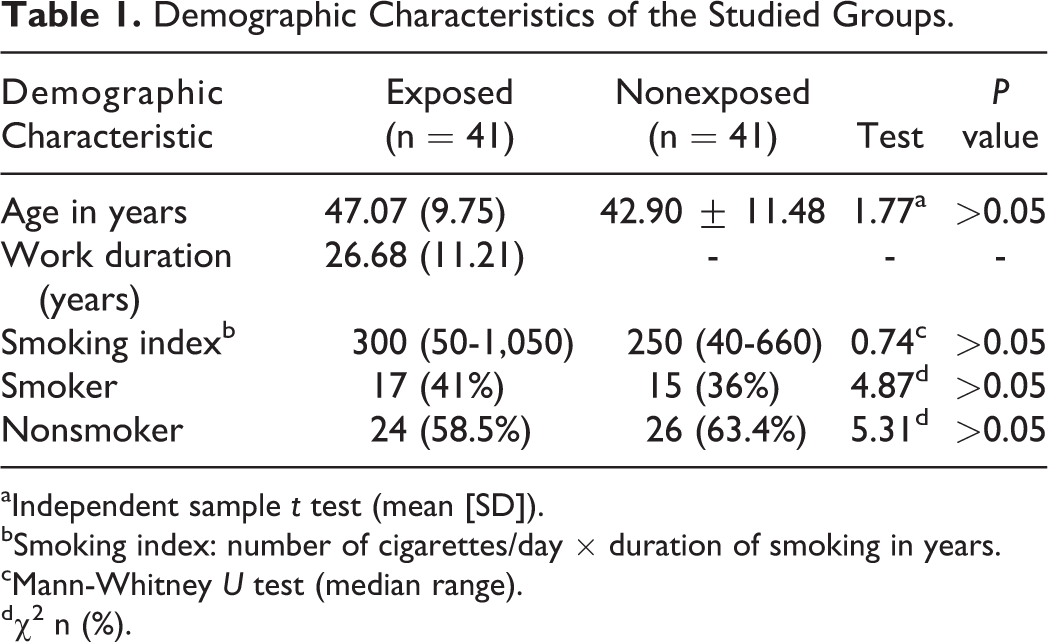
aIndependent sample t test (mean [SD]).
bSmoking index: number of cigarettes/day × duration of smoking in years.
cMann-Whitney U test (median range).
dχ2 n (%).
The Prevalence of Clinical Symptoms Among Studied Groups.
Serum Chromium, Serum Nickel, Serum 8-OHdG, and Micronucleus Test Among Studied Groups.a
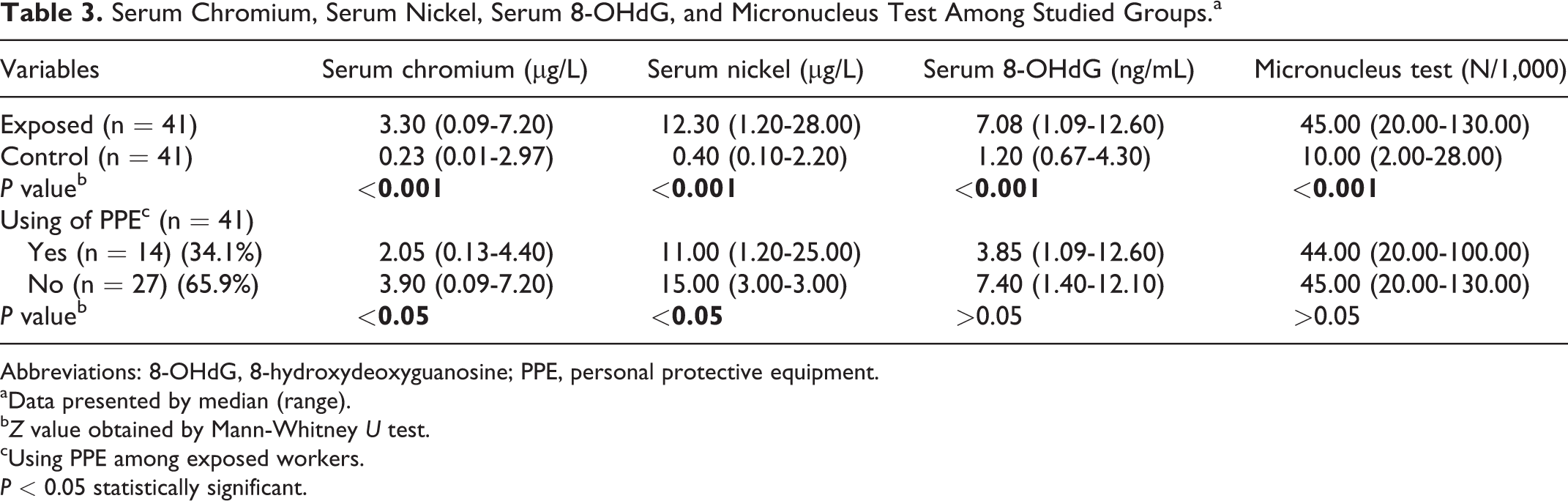
Abbreviations: 8-OHdG, 8-hydroxydeoxyguanosine; PPE, personal protective equipment.
aData presented by median (range).
bZ value obtained by Mann-Whitney U test.
cUsing PPE among exposed workers.
P < 0.05 statistically significant.
Multiple Regression Analysis to Test Predictor for 8-OHdG and Micronucleus Test in Exposed Workers.
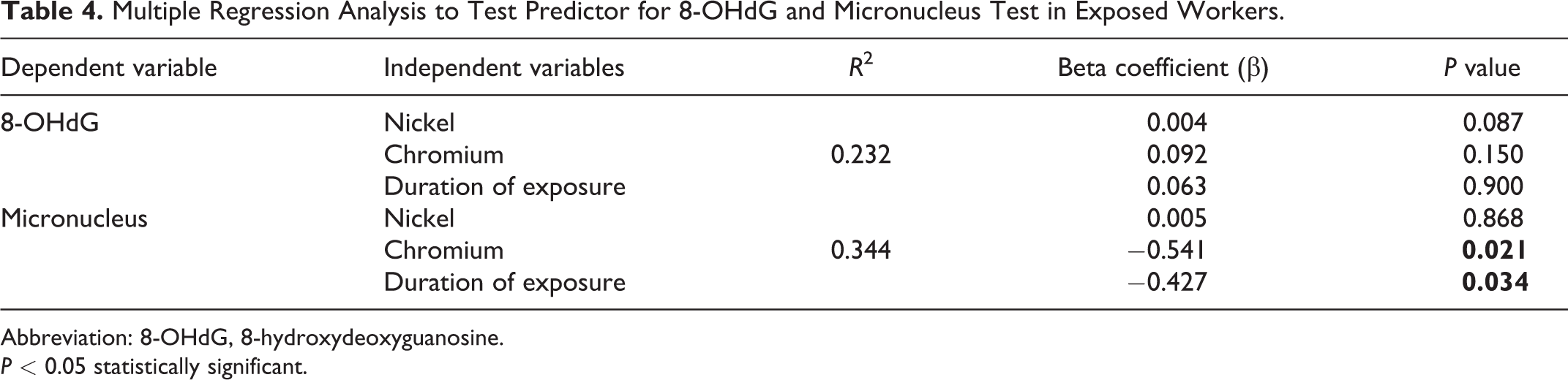
Abbreviation: 8-OHdG, 8-hydroxydeoxyguanosine.
P < 0.05 statistically significant.
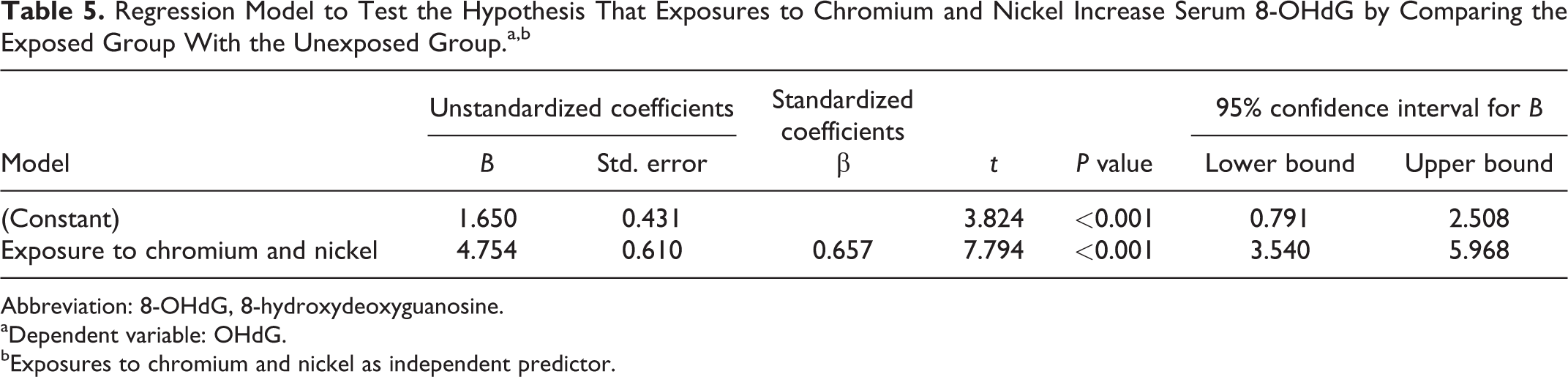
Linear regression models to test the hypothesis that exposures to chromium and nickel increased serum 8-OHdG and micronucleus test, by comparing exposed and nonexposed. The model found that exposure to chromium and nickel increases serum 8-OHdG by 4.754 (95% confidence interval [CI]: 3.54-5.968; Table 5]. The model found that exposure to chromium and nickel increases micronucleus by 35.927 (95% CI: 28.517-43.337; Table 6).
Regression Model to Test the Hypothesis That Exposures to Chromium and Nickel Increase Serum 8-OHdG by Comparing the Exposed Group With the Unexposed Group.a,b
Abbreviation: 8-OHdG, 8-hydroxydeoxyguanosine.
aDependent variable: OHdG.
bExposures to chromium and nickel as independent predictor.
Regression Model to Test the Hypothesis That Exposures to Chromium and Nickel Increase Micronuclei Counts, by Comparing the Exposed Group With the Unexposed Group.a,b
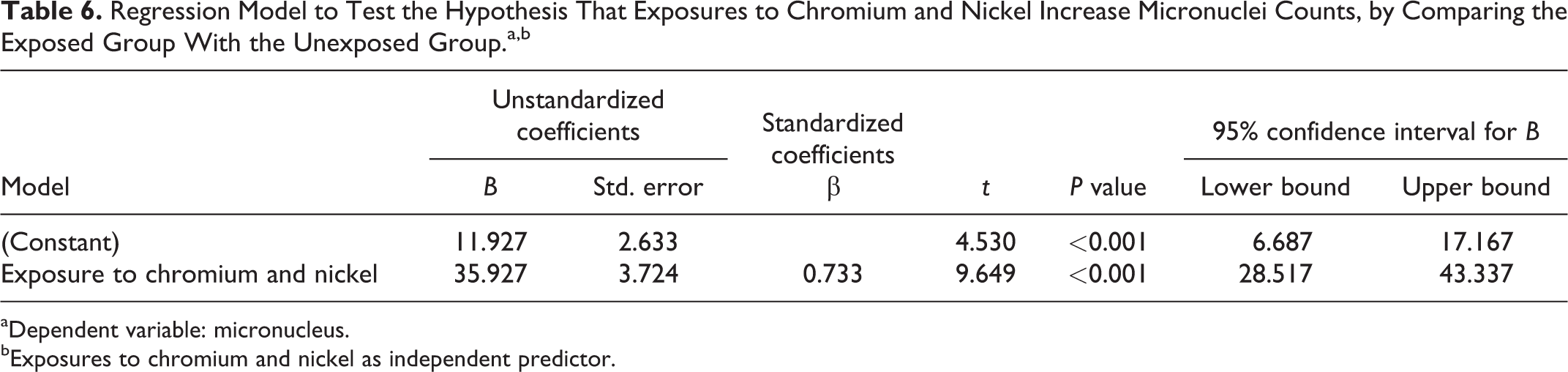
aDependent variable: micronucleus.
bExposures to chromium and nickel as independent predictor.
Discussion
The current study found that exposure to chromium and nickel among electroplating workers caused some adverse health hazards mainly respiratory, dermatological, nasal, and eye irritation. There were statistically significant increased levels of serum chromium, nickel, and 8-OHdG and micronucleus frequency in buccal cells among exposed workers compared to the nonexposed group. The prevalence of chest symptoms was higher among the exposed workers as compared to nonexposed workers. Eight (19.5%) workers had dyspnea, 36 (87.8%) had dry cough; 16 (39%) workers had a cough with expectoration for more than 2 years, and 17 (41.5%) participants had a wheezy chest. The prevalence of irritant effects in the form of nasal irritation 24 (58.5%), conjunctivitis 13 (31.7%), and contact dermatitis 26 (63.4%) was higher among the exposed group (Table 2). This could be attributed to the evolution of hydrogen, oxygen gas, chromic acid mists, and nickel fumes during the electroplating operation. The current study results agreed with that of Jeyamala et al 21 who found an increased prevalence of allergic bronchitis (17%), nasal irritation (35%), and allergic reactions of the skin (4.2%) among workers exposed to chromium and nickel in electroplating industries located in Madurai city, South India. A study by Were et al 22 found an increased incidence of wheezing, shortness of breath, and sneezing attacks among workers exposed to chromium and nickel in welding and leather tanning industry, in Kenya. They concluded that engineering controls and industrial hygiene in these industrial plants were inadequate. The fumes were observed building up in the workers’ breathing zones especially during welding processes. Not all welders and tanners provided with respirators; therefore, inhalation was a major intake of chromium and nickel from the breathing zones of these workers.
In this study, workplace monitoring was assessed by the industrial hygienist of the factory. It was performed according to the Occupational Safety and Health Administration (OSHA) standards and procedures. 23 The estimated geometrical means for Cr (VI) (0.05 mg/m3) and soluble nickel (0.1 mg/m3) as an 8-hour time-weighted average were below maximum allowable limits according to Egyptian law, 24 international regulations as the occupational exposure limit of the OSHA 23 and the Control of Substances Hazardous to Health, and regulations under Health and Safety Executive. 25 Adequate local exhaust ventilation was present at work site, and regular air samples were taken to assess the effectiveness of ventilation controls by industrial hygienist team of the factory.
Findings of the present study were in accordance with Kuo et al 10 who found higher urinary chromium concentrations among electroplating workers, in Taiwan, than those in the control group. Similarly, they found higher levels of urinary 8-OHdG among chromium workers as an indicator of oxidative DNA damage. Also, Setyaningsih and his co-workers 26 found an increase in chromium levels and urinary8-OHG as biomarker of oxidative DNA damage among 66 participants from electroplating home industry in Tegal, Central Java. Recently, Abd-El Maksoud et al 27 found an increased levels of serum chromium among 45 male tannery workers in Cairo. In contrary to the present study results, they found a nonsignificant increase in urinary 8-OHG among exposed workers.
Few biomonitoring studies of nickel exposure in electroplating industry have been conducted. One of these studies is that of Qayyum et al 28 they found that the concentration of plasma nickel among 150 electroplating workers was significantly higher in electroplaters of ≥10-year work duration. Similarly, plasma chromium levels were also significantly higher in electroplaters of ≥10-year work duration compared to workers electroplaters of ≥10-year work duration compared to worker of work duration <10 years and the control group.
Micronucleus frequency is a predictive biomarker for cancer risk. In the present study, the micronucleus test and serum 8-OHdG were statistically significant higher (P < 0.001) among exposed workers (Table 3). The current study revealed a clear evidence of genotoxicity in exfoliated buccal cells when evaluated by micronucleus test. The greater prevalence of micronuclei in platers implies that they are highly exposed to genotoxic insults and therefore are at a greater risk of developing cancer. Benova et al 29 agreed with the current study results; they studied the cytogenetic effects in Bulgarian chromium platers using micronucleus assay in peripheral lymphocytes. They found a significant increase in the number of cells with micronuclei in peripheral lymphocytes with respect to the values obtained from control. A statistically significant increase in the frequency of micronuclei in the exfoliated buccal cells of the chromium-exposed workers was observed as compared to the controls in Benova study.
Using PPE regularly can reduce direct contact with toxic chemicals and protection from dust containing respirable metal particles during electroplating. In this study, inquiring about regularly using PPE in exposed workers revealed that the minority of workers (n = 14, 34.1%) were using PPE in form of safety gloves, mask, and apron (work suit) during daily working hours. In the current study, using of PPE significantly decreased the levels of chromium and nickel (Table 3). This finding was in concordance to a study by Jelmert et al 30 who detected a decrease in the serum levels of chromium and nickel with the use of PPE among stainless steel workers. Hariyani et al 31 found a decrease in the level of chromium and nickel in the blood of 30 dental laboratory technicians with the use of PPE in the form of gloves, masks, and protective clothing. The present study found no statistically significant correlations between the age and each of serum chromium, serum nickel, serum 8-OHdG, and micronucleus frequency. In accordance with this study results, Setyaningsih et al 26 found that age and urinary chromium level were not associated with urinary 8-OHdG level among electroplating workers exposed to chromium. Abd-El Maksoud et al 27 found no correlation between both age and chromium levels in the blood. This could be explained by the fact that chromium has no cumulative effect on the body. Similarly, Jeyamala et al 21 concluded that nickel was found to accumulate at higher levels than chromium in electroplating workers than the control participants. The current results were consistent with Kiilunen et al 32 who found no correlation between micronucleus frequencies in buccal mucosa of nickel refinery workers in Finland and levels of nickel in air, urine, or blood. They attributed their findings to the efficiency of respirators used by the workers at the worksite. In the current study, there was limited number of workers who use PPE. Moreover, there was combined exposure to both chromium and nickel among the electroplating exposed workers.
A statistically significant positive correlation was found between serum chromium and micronucleus test among the exposed group with work duration more than 20 years. In agreement with the current study, Vaglenov et al 33 evaluated the genetic risk associated with occupational exposure to chromium in 40 electroplaters, in Bulgaria. Workers were classified as highly exposed (n = 24, 0.083 + 0.001 mg/m3 chromium in air) of longer duration of exposure >10 years and less exposed (n = 16, 0.043 + 0.001 mg/m3 chromium in air) exposure <10 years. A significant increase in the total number of micronuclei in PBL (53.08 and 29.06) and in BNMN (42.13 and 25.4) was reported in exposed workers as compared with the control group (n = 18, 21.05, and 19.8, respectively; 0.3 + 0.1 mg/m3 chromium in air). The authors suggested a direct correlation between chromium levels in air, erythrocytes, urine, and the frequency of BNMN (Binucleated cells containing micronuclei) and longer duration of exposure.
Conclusion
The present data revealed increased serum levels of both chromium and nickel among electroplating workers. The genotoxic damage in the form of micronuclei induction in exfoliated buccal cells and oxidative DNA damage expressed as 8-OHdG were observed among workers in the exposed group. This study attributed the genotoxic damage observed in the exposed workers to the combined effect of both chromium and nickel.
From the current study, we recommend the use of personal protective measures as respirators with specific filters, nonpermeating gloves, and aprons. Furthermore, applying administrative control measures in form of training for workers on safe work practices, limited time of exposures to hazards, providing health monitoring, appropriate counseling, and medical follow-up for workers who have positive findings as high levels of 8-OHdG and high frequency of buccal micronuclei are recommended. Further studies on larger numbers of combined exposure to chromium and nickel in electroplating industry are needed.
Footnotes
Author Contributions
ElSafty A contributed to conception and design; contributed to acquisition, analysis, or interpretation of data; and critically revised the manuscript. Samir A contributed to conception and design; contributed to acquisition, analysis, or interpretation of data; drafted the manuscript; and critically revised the manuscript. Mekkawy M contributed to acquisition, analysis, or interpretation of data, critically revised the manuscript, and gave final approval. Fouad M contributed to conception and design; contributed to acquisition, analysis, or interpretation of data; and drafted the manuscript. ElSafty A, Samir A, and Fouad M gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.