
Abstract
Life experiences, industrial/environmental exposures, and administration of Food and Drug Administration (FDA)-approved drugs may have unintended but detrimental effects on peripheral and central auditory pathways. Most relevant to the readership of this journal is the role that drug treatments approved by the FDA as safe and effective appear to interact with 3 independent modes of toxicity within the small compartment of the ear. What may seem to be trivial drug-induced toxicity has the potential to change important measures of quality of life and functional capacity of mid- to late-life patients. Drugs meant to treat can become the source of interference in the activities of daily living, and as a result, treatment compliance may be jeopardized. Ototoxicity has been defined as the tendency of certain therapeutic agents and other chemical substances to cause functional impairments and cellular degeneration of the tissues of the inner ear resulting in hearing loss. However, one of the largest contributors to hospitalizations is fall-related injuries in the elderly patients associated with disorders of vestibular function linked to progressive and drug-induced toxicities. Tinnitus affects 35 to 50 million adults representing approximately 25% of the US population, with 12 million seeking medical care and 2 to 3 million reporting symptoms that were severely debilitating. This review is intended to highlight these targets of neurotoxicity that threaten the usefulness of drug treatments deemed safe and effective prior to access by the general public.
Keywords
Introduction
Ototoxicity has been defined as the tendency of certain therapeutic agents and other chemical substances to cause functional impairments and cellular degeneration of the tissues of the inner ear. 1 Ototoxicity is usually iatrogenic, but it is well known that whole classes of compounds have shown to cause adverse effects. Many of these, such as aminoglycoside antibiotics and the anticancer agent cisplatin, have a critical role in the treatment of serious life-threatening diseases. Others, such as loop diuretics (Lasix, furosemide) and salicylates (aspirin), offer such important therapeutic effects that when compared to their secondary ototoxic effects, the risk has been considered to be of minor importance. 2 The significant damage to visual (nonarteritic anterior ischemic optic neuropathy [NAION]) and auditory systems (sudden deafness and sensorineuronal loss) induced by the newer class of compounds designed to treat male erectile dysfunction, Viagra (sildenafil), Levitra (vardenafil), and Cialis (tadalafil), came to light only following new drug application (NDA) approval and widespread sales of the drug. 3 -6 Even the inhaled antibiotic, tobramycin, used to target direct delivery of maximal concentrations at the site of infection in patients with cystic fibrosis and bronchiectasis has demonstrated a potential to induce hearing loss. 7
It seems intuitive that otic preparations would be the most likely candidates for direct toxicity if the compound easily crosses the tympanum (eardrum) or if the tympanum is ruptured or torn prior to dose administrations into the ear canal. However, it is the systemically administered prescription drugs such as furosemide (Lasix) or the common, over-the-counter, aspirin that can initiate the cascade of oxidative damage that causes tinnitus or the aminoglycoside antibiotics that initiate cytotoxicity in the cochlea. If the elderly patient knows that the pill that the doctor prescribed makes for an unstable gait and causes dizziness, which leads to a fall and broken hip, what is the likelihood he or she is going to continue taking the medicine—regardless of its efficacy to treat their condition?
A few years ago, incidence of cardiac crises were broadcast in mainstream media in response to men taking Viagra in combination with their normal daily compliment of nitroglycerin. This occurred only after Viagra was approved as safe and effective for the treatment of erectile dysfunction. In retrospect, it seems reasonably clear that the most likely candidates in need of pharmacotherapy for erectile dysfunction might also be a patient with cardiac disease or a diabetic. Similarly, what is the likelihood that the patient diagnosed with congestive heart failure and prescribed furosemide and once-a-day low-dose aspirin therapy (81 mg) will also develop a high-pitch ringing in the ears so debilitating that they no longer want to take the drugs? These instances illustrate that when we consider drug safety, we must include the assessment of off-target toxicities that may express as subtle, though nevertheless potentially seriously debilitating, sensory deficits that correspondingly represent a significant threat to patient compliance.
There are currently no systematic or regulatory-guided preclinical studies conducted that include analysis of all peripheral and central vestibular structures or auditory sensory organs prior to drug approval. Major obstacles in vestibular and hearing research include difficulties around postmortem tissue acquisition as well as adequate neuropathological characterization prior to NDA submission to the US Food and Drug Administration (FDA). Contributing to these difficulties are considerations that inner ear structures are enveloped in a bony encasement, and the cochlea and vestibular structures lie in different anatomical planes. 8 Any test article-related toxicity induced in the small compartment containing these critical tissues is rarely discovered during the execution of standard preclinical protocols on the course to drug approval.
Even in review of this article, a distinguished colleague reviewer stated, “This paper has very little toxicology focus after the section on drugs and hearing loss and needs to be refocused to be published in a toxicology journal.” We agree. But we counter this statement by highlighting that standard toxicology text/reference books, such as Casarett and Doull’s Toxicology: The basic science of poisons, 9 the primer for most D.A.B.T. test questions, or Derelanko and Auletta’s, Handbook of Toxicology, 10 fail to even list terms such as ototoxicity, otic administration, cochlea, auditory system, auditory, or vestibular toxicity in the subject indexes of either core textbook. The purpose of this article is to highlight what our distinguished colleague noted in his/her review: there is a general paucity of concern, focus, or directed studies by toxicologists, in general, targeting the underlying toxicity associated with the direct pharmacological insult to tissues associated with the eighth cranial nerve.
Hearing Loss
Impact
Drug-induced hearing loss is rarely identified during preclinical safety/toxicity testing. Among the reasons for this are findings that animals compensate for changes in auditory function in ways that often mask the loss even to trained observers who work with the animals on a daily basis. 11 Accordingly, it is often in the early marketing phase of a new drug’s history that adverse events induced by ototoxicity are reported for the first time. Under the impact of environmental or drug insult, sensitive cells of the auditory system are challenged and eventually overwhelmed to the point of inability to maintain cellular homeostasis. In the context of therapeutic drug development efforts, ototoxicity refers to pharmacological insult to the inner ear by systemically administered drugs (aminoglycoside antibiotics, erectile dysfunction drugs, etc) or by otically administered drugs (eg, dosed into the outer ear canal) gaining access to the middle and inner ear tissues by transtympanic absorption or due to breach of the tympanic membrane. Damage to the small bones of the middle ear (malleus, incus, and stapes) can produce conductive hearing loss and exposure of sensitive hair cells in the cochlea (inner ear) to toxins may engage mechanisms of toxicity ultimately resulting in cell death via apoptosis or necrosis, either of which may result in some level of potentially irreversible hearing loss.
Drug-induced damage to the auditory system is not a new phenomenon. In spite of the common belief that natural remedies are safe, some of the most prominent ototoxic drugs known today are derived from natural sources: the aminoglycosides, synthesized by soil-dwelling bacteria, and quinine and salicylates, both derived from tree bark.
In 1944, the drug, streptomycin, was hailed as the long-sought cure for tuberculosis and other gram-negative infections. Once on the market, streptomycin, an aminoglycoside antibiotic, quickly revealed its destructive power to the end organs located in the closed compartment of the inner ear. 12 Deafness and vestibular disorders have not diminished the use of streptomycin in 2016, and other antimicrobial agents such as chloramphenicol, erythromycin, polymyxin B, or vancomycin have a long history of initiating the cascade of homeostatic failure that results in cell death. And although some of these agents, for example, chloramphenicol, are restricted as alternative treatments (ie, as last resort treatments of meningitis, typhoid, or rickettsial infection), their therapeutic reward outweighs the targeted neurotoxicity in the small compartment of the eighth cranial nerve and associated receptor tissues. It has been well recognized that even topical application of disinfectants such as chlorhexidine can initiate ototoxic events. 13 The drug is found in many oral rinse products for gingivitis and periodontal disease and can be found in almost every presurgical scrub used in hospitals worldwide (Nolvasan or Hibiclens). Even the loop diuretic, furosemide (Lasix) has a long history of inducing deficits in hearing and balance (see below) in the patient population most likely to have the most adverse reactions to such loss (eg, home falls, tinnitus, etc; see below).
In 1993, a nucleotide mutation in the mitochondrial 122S ribosomal RNA gene at position 1555 was identified in 3 Chinese families with 15 deaf family members. 14,15 Since then, additional families with the A1555G mutation and ototoxic hearing loss have been identified in Japan, Zaire, Mongolia, Israel, Spain, and the United States. 15 -17 By reviewing the case files, it was believed that the inheritance of the predisposition was autosomal dominant with incomplete penetrance and most likely of maternal inheritance of a mitochondrial DNA defect. 15,16 The mitochondrial mutation appears to be a deafness-predisposing mutation only. Families with the mutation have been reported with hearing loss without any exposure to aminoglycosides. Over the years, it seems clear that high doses of aminoglycosides may induce toxicity in all patients, although patients with A1555G mutation may have a higher propensity for cell damage at lower doses. Important to note is the fact that A1555G can produce sensorineuronal loss without aminoglycoside exposures.
Today, combination chemotherapy is the mainstay of cancer treatment protocols. Cisplatin is an antineoplastic agent that was found to induce irreversible kidney damage even in phase I clinical trials—occurring in 25% to 61% of patients, depending on the dose. 18,19 Systemic cisplatin administration is also associated with bilateral hearing loss, primarily in the high-frequency ranges. 20,21 In spite of the fact that the well-known renal toxicity and ototoxicity may occur in up to 30% of patients, 22 the therapeutic benefits outweigh the impact of these direct effects of the drug on auditory tissues. Landier 23 has recently reported the prevalence of ototoxicity in patients who have received potentially ototoxic therapy ranges from 4% to 90% depending on factors such as age of the patient population, agent(s) used, cumulative dose, and administration techniques. The impact of ototoxicity on subsequent health-related and psychosocial outcomes in these patients can be substantial, and the burden of morbidity related to ototoxic agents is particularly high in very young children.
Johannes et al 24 have reported population projections for men 40 to 69 years old who have erectile dysfunction. Their risk assessment data suggest that over 600,000 Caucasian males living in the United States are expected to need pharmacological remedy annually. Overall, the risk of erectile dysfunction is about 26 cases per 1,000 men annually and increases with age, lower education, diabetes, heart disease, and hypertension. 24 In 2007, Selvin et al 25 estimated that erectile dysfunction affects 18 million men in the United States alone. The significant damage to visual (NAION) and auditory systems (sudden deafness and sensorineuronal loss) induced by the newer class of compounds designed to treat male erectile dysfunction, Viagra (sildenafil), Livitra (vardenafil), and Cialis (tadalifil), came to light only following NDA approval and widespread sales of the drug. 3 -6 In the 2007 FDA notice of labeling changes on these drugs, the agency stated, “though no causal relationship has been demonstrated, FDA believed that the strong temporal relationship between the use of phosphodiesterase-5 (PDE5) inhibitors and sudden hearing loss in these cases warranted revisions to the product labeling for the drug class.” In spite of these direct toxic effects of the compound class, sales of and requests for the drug seem to be unaffected by the public awareness of the connection between this drug class and ototoxicity.
Loci of Interest
There are many ways that drugs can affect hearing. The neural coding for frequency is owed largely to the physical properties of the ear. The external auditory canal transmits the sound to the eardrum. The shape and size of the canal serves as a preset resonator to selectively amplify sounds in the region of 2,000 Hz, which is why humans are most sensitive to these frequencies. It has been reported that the displacement of the eardrum (tympanic membrane) required to hear a 1,000 Hz tone at 74 dB is less than 1-millionth of an inch, illustrating that it does not require much change in the elastic properties of this thin membrane to ultimately affect hearing. 26
The ossicles are a tripartite set of bones of the middle ear that transmit the vibrations of the air pressure waves from the eardrum to the oval window of the cochlea (malleus [hammer], incus [anvil], and stapes [stirrup]). The construction of the ossicles and their functional articulations via associated muscles allow unwanted vibrations from the head or excessive noise in the environment to be dissipated without being transmitted fully to the fluid-filled cochlea. 27 Drugs (or excipients) that affect the structure or movement of the small bones of the ossicles or the muscles linking them together can produce deficits in transmitted air pressure wave changes from the eardrum to movement of the fluid in the cochlea, a condition referred to as conductive hearing loss.
The cochlea, located in the inner ear compartment, is a coiled canal that lies embedded within the bone of the skull. It is divided into 3 sections along most of its length by a tube, called the scala media. The scala media contains an endolymphatic fluid medium and the sensory hair cells that are responsible for signal transduction processes associated with audition. These sensory cells are physically affected by endolymph waveform movements produced by the pulsating oval window deflections associated with tympanic membrane and ossicular movements ultimately generated by air pressure waves. As the oval window is struck, a corresponding wave propagates through the endolymph of the scala media down the length of the cochlea. The propagating endolymph wave exerts sheering forces on the cilia of the hair cells, causing depolarization, and ultimately the transduction of air pressure waves to the neural code that is transmitted by the eighth cranial nerve. 27,28 Any event that changes the homeostatic environment of the inner ear has the potential to induce temporary or permanent hearing loss. Changes in fluid density, excessive sheering forces of the cilia of the hair cells, or direct cytotoxic events that target the internal biochemistry of the hair cells have the potential to induce such hearing losses.
The overproduction of reactive oxygen species (ROS) with the resulting ionic charge balance distortions within the cells of the inner ear (presence of free radicals) appears to be a common mechanism by which many forms of oxidative stress may cause damage to the inner ear. The 3 most common ultimate sources of cellular damage mediated by such mechanisms include normal aging, excessive noise, and drug administrations. 29 -31 Under normal conditions, mitochondrial respiration and oxidative enzymatic processes of all living cells produce ROS. Most of the time, ROS are simply byproducts of the normal cascade of events of metabolism within cells. It is the overproduction of ROS or the cells inability to neutralize or balance the negative and positive charges within the cellular environment that initiates a cascade of events to cell death—apoptosis. 32 Another source of charged particles (radicals) is the production of reactive nitrogen species (RNS). Nitric oxide is formed by a family of enzymes and directly serves signaling functions in cells. Nitric oxide plays an essential part of normal physiology and is a potential route to the pathophysiology associated with ototoxicity. From one perspective, the most significant reactions of RNS are those that occur with the highest yield. However, since cells have the capacity to amplify signals and select specific chemical species, then the reactions of RNS of most physiological or pathological significance can only be determined by examining their effects in a biological system. Reactions of nitric oxide (NO) ultimately lead to the oxidation, nitration (addition of NO2), nitrosation (addition of NO+), and nitrosylation (NO) of most classes of biomolecules. One of the best known interactions of NO leading to cell signaling is the reversible covalent binding, nitrosylation, with the ferrous heme in soluble guanylate cyclase. However, reactions of RNS derived from NO engage proteins, lipids, and carbohydrates. The different forms of nitric oxide synthase (NOS) isoenzymes serve a variety of physiological processes in normal tissue physiology, and the product of this cellular reaction is NO—an important second messenger molecule. The normal healthy cell maintains a balance between all of the positive- and negative-charged particles within it. When the maintenance of such balance is compromised, cellular damage is initiated. 33,34
Aging is a normal developmental process that is associated with hearing loss and represents the normal wear and tear on the metabolic cellular maintenance within all cells designed to balance the adverse potential of ROS and RNS within its internal milieu. Systemic administration of ototoxic drugs places a burden on the hair cells’ internal processes. Drugs such as cisplatin or aminoglycoside antibiotics produce increased formation of reactive oxygen and nitrogen species. As the cochlear hair cells are depleted of their natural antioxidant concentrations of glutathione or other enzymes such as superoxide dismutase, catalase, glutathione peroxidase, and glutathione reductase, the cellular balancing act between charged particles is disrupted and the cell triggers a pathway to its own cell death—apoptosis.
Recently, the administration of antioxidants such as α-tocopherol (vitamin E), ascorbic acid (vitamin C), salicylates, and the spin-trapping agent p-butyl-nitrone have shown promise in protecting hair cell loss when taken before, during, and even after pharmacological insults. 35
Tinnitus
Impact
The central nervous system (CNS) possesses a remarkable and often underestimated capacity to adapt to the world around us. This capacity to learn or to adapt to the constantly changing demands of the environment is a lifelong process that requires processing of neural circuits that are modified in response to short- and long-term changes in sensory inputs. One of the potential scenarios illustrating this adaptive process is rewiring of connections and alterations in the activity of neurons as a result of environmental insults, both internal (drugs) and external (noise). A classic example of such an adaptation is tinnitus—the conscious awareness of phantom sounds in the absence of an acoustic stimulus. A second example of CNS adaptation is hyperacusis—having a reduced tolerance of and increased sensitivity to sounds in your normal environment. People who have hyperacusis do not hear a sound that doesn’t exist (like patients with tinnitus), rather they complain of living in a world in which the volume of real sounds seems to be turned up too high. Although patients with tinnitus have a perception of sound in the absence of sensory input, the patient with hyperacusis hears sounds that most people hardly notice or seem to overreact to situations that most others hardly respond to (clanging of silverware or the sound of a baby crying). Tinnitus is an auditory perception of sound that originates in the head and not from an external sound source. Phantom sounds are similar to the phantom pain that can occur following physical trauma. These phantom events are part and parcel of how the brain works. Tinnitus, pronounced, “tin-eye’-tus” (United States) or “tin’-e-tis” (United Kingdom) occurs after peripheral trauma. It is presumed to derive from peripheral nerve damage and associated compensation for the damage by the CNS. Most contemporary researchers in the field of audition hold the position that tinnitus and hyperacusis are independent of hearing impairment. That is to say, tinnitus and hyperacusis often occur in conjunction with a loss of threshold hearing sensitivity, 36 but neither hearing threshold loss nor outer hair cell loss is essential to develop either condition. 37
The clinical diagnosis of tinnitus in humans relies on subjective measures such self-report, questionnaires, visual analog rating scales, and psychoacoustic matching. 38 -40 Tinnitus has both sensory and affective components that are somewhat refractory to management and has no direct, objective correlate. 41 The reactive component of tinnitus and hyperacusis is not directly related to the sensory features of the stimulus event that initiated the adaptation. The emotional impact of these disorders in perceptions of auditory stimulus inputs certainly affects measures of the quality of life and hinders work performance and social interactions that, in some cases, results in depression, anxiety, disordered sleep, and impaired concentration. 42 -48
Estimates suggest that 35 to 50 million adults representing approximately 25% of the US population have tinnitus, with 12 million seeking medical care and 2 to 3 million reporting symptoms that were severely debilitating. 44,49 -51 In 2007, Cave et al 52 reported that 49% of military personnel exposed to blast trauma reported tinnitus as their primary audiologic complaint. Hu et al 53 have reported that the US Department of Veterans Affairs tinnitus disability claims have exceeded 840,000 and the cost to compensate veterans for tinnitus is over US$1.28 billion annually. The prevalence of tinnitus tends to increase with age until the range of 60 to 69 years old, after which it decreases with increasing age. 44,48,54 -56
Loci of Interest
Tinnitus never occurs in isolation. It typically develops after somatic insults, stressful events, and hearing loss, including losses at frequencies not tested in clinical audiometry, and is often accompanied by hyperacusis. 57,58 As stated above, hyperacusis may reflect the central gain change in the auditory system that occurs after hearing loss. Studies on the mechanism of tinnitus have to take into account that neither hearing loss nor hyperacusis is a necessary condition for tinnitus to occur. 59 The data do show that auditory sensitivity is enhanced in tinnitus as compared with nontinnitus cohorts, including participants with normal audiograms. These findings further suggest some form of central-mediated gain change in tinnitus. Tinnitus might reasonably be called a CNS adaptation.
Muhlau et al 60 have reported structural changes in the auditory system of patients with tinnitus that were limited to thalamus with decreases in gray matter (GM) in the subcallosal region including the basal ganglia. Landgrebe et al 61 also found significant GM decreases in the right inferior colliculus (IC) and left hippocampus of patients with tinnitus; the degree of changes was not correlated with the duration or severity of tinnitus, and the structural changes reported by Muhlau et al 60 were not confirmed. Human brain imaging studies have identified altered tinnitus-related activity in auditory areas, including the IC and auditory cortex. 58,62 Magnetic resonance imaging has revealed differences in sound-evoked responses between tinnitus and nontinnitus groups in cortical and subcortical auditory nuclei and differences in thalamic and auditory brainstem and auditory cortex.
The cochlear nucleus (CN) is the first site of sensory convergence in the auditory system. The trigeminal nerve (the fifth cranial nerve or simply CN V) is the nerve responsible for sensation in the face and motor functions such as biting and chewing. The largest of the cranial nerves, it has 3 major branches: the ophthalmic nerve (V1), the maxillary nerve (V2), and the mandibular nerve (V3). The ophthalmic and maxillary nerves are purely sensory, and the mandibular nerve has sensory (or cutaneous) and motor functions. The dorsal column of the trigeminal nerve innervates the back of the head and pinnae as well as the neck and upper limbs. Axon terminals of the CN are derived from first-order dorsal root ganglia and trigeminal ganglia and second-order projections of the spinal trigeminal nucleus and dorsal column nucleus. 63,64 The convergence of auditory and somatosensory inputs also occurs in the midbrain. The IC receives inputs from the contralateral CN. Bipolar electrical pulses delivered to the trigeminal ganglia (facial sensory nerve) preceding broadband noise bursts by as much as 95 milliseconds were found to suppress or facilitate the sound-driven firing of over 78% of fusiform cells in the dorsal cochlear nucleus (DCN). 65
A growing body of literature supports the DCN as the site of tinnitus induction, where diminished auditory nerve input initiates hyperactivity, which then spreads within the brain. 66 The cells of the DCN are primed for such an induction process. The principal output neurons of the DCN express a high degree of synaptic plasticity, which facilitates integration of multisensory information (eg, trigeminal nerve). It is these somatosensory inputs that provide a reservoir of excitatory drive that can be recruited to maintain homeostasis. 11
Inferior colliculus hyperactivity is also observed with tinnitus, but ablation of the DCN before noise damage prevents hyperactivity and tinnitus 67 and ablation of the DCN after noise damage immediately and completely abolishes IC hyperactivity. 68 Therefore, the IC cannot independently generate the hyperactivity. 68,69 Wu et al 66 have recently proposed that elevated spontaneously activity in DCN is transmitted to the IC and, perhaps, independently to the medial geniculate nucleus of the thalamus 70 via direct projections where tinnitus-related hyperactivity is also observed. 71
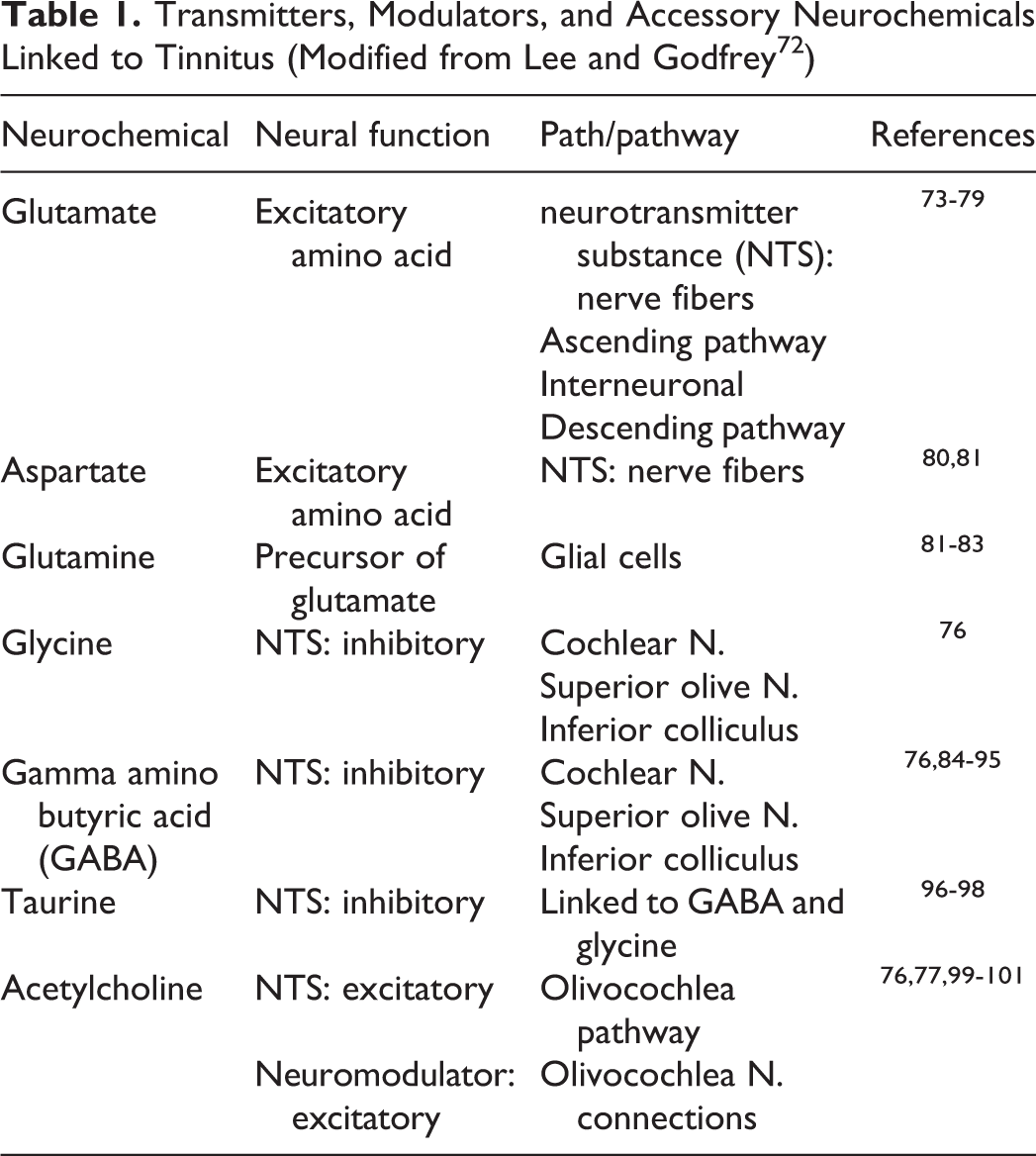
Many different neurotransmitter systems have been implicated in the auditory damage that is associated with reports of tinnitus. Table 1 highlights some of the myriad of transmitters, modulators, and accessory neurochemicals cited in a recent literature review by Lee and Godfrey 72 linked to tinnitus.
Transmitters, Modulators, and Accessory Neurochemicals Linked to Tinnitus (Modified from Lee and Godfrey 72 )
The management of tinnitus usually requires a multidisciplinary approach by family physicians, otorhinolaryngologists or ENT, otologists, neurotologists, neurologists, and psychiatrists in collaboration with allied health professionals, such as audiologists, psychologists, physical therapists, and hearing aid specialists. The 2 main options for managing tinnitus are masking using hearing aids or other masking devices and medications to address tinnitus major secondary symptoms: mainly poor sleep, anxiety, or depression. Pharmacological management is best handled by neurologists or psychiatrists.
Since tinnitus is a subjective phenomenon, the assessment of outcome is probably the single most important factor in conducting clinical trials. 102 Success in treating tinnitus is critically dependent on assessments of tinnitus loudness either by visual analog scales or by psychoacoustic measurements and assessment of tinnitus severity, which is usually assessed by validated questionnaires.
To date, no drug is available that has demonstrated reproducible, long-term reduction in tinnitus impact that is statistically greater than placebo. SPI-1005 Sound Pharmaceuticals (Seattle, WA, USA), AM 101 and AM 102 Auris Medical (Zug, Switzerland), Vestipitant GlaxoSmithKline (Brentford, London, UK), and EGb-761 (Tebonin™, Dr. Willmar Schwabe GmbH & Co KG, Karlsruhe, Germany) have all shown some level of efficacy, but none are currently approved. Although there is an urgent need for efficacious compounds, fortunately, there is no reason to believe that tinnitus cannot be effectively treated by pharmacotherapy.
Balance Disorders
Impact
Postural control is considered a complex motor skill derived from the interaction of neural and skeletal muscle systems. Persistent postural–perceptual dizziness (PPPD) is one of the most common causes of chronic vertigo in middle-aged patients 103 and the second most common diagnosis in patients presenting with vestibular symptoms with a high impact on functioning in daily living and quality of life. 104 The main clinical characteristics of this disorder include persisting subjective nonrotational vertigo or dizziness, hypersensitivity to motion stimuli, including the patients’ own movements or motion of objects in the visual field of the patient. 105 Most often, these patients have normal values in clinical balance tests, 106 and currently, there are no objective tests to establish a diagnosis of PPPD.
The diagnosis of PPPD is based on the clinical condition named “phobic postural vertigo (PPV)” by Brandt and Dieterich. 107 In 2007, Staab and Ruckenstein 108 refined and updated the concept of PPV and renamed it chronic subjective dizziness, and in 2014, the World Health Organization adopted the disorder as PPPD for the International Classification of Diseases to be released in 2017.
Disequilibrium of aging (presbyastasis) is linked to significant morbidity and limits the quality of life in the elderly patients. 109,110 Normal aging processes are directly related to the vestibular system, which may cause multiple otoneurological-associated symptoms such as vertigo and other types of dizziness, gait disturbances, and occasional falls. Repeated falls within the home is a common geriatric syndrome with age-related increases in the seriousness and complications associated even with what might seem a minor fall. One of the leading factors in the increase in home falls in the elderly patients is the presence of vestibular disorders due to the effects of these conditions on body balance. 111 Benign paroxysmal positional vertigo is the most common form of peripheral vestibular vertigo in adults 112 -114 with an incidence rate of 64 per 100,000 adults, with a higher incidence in 70-year-old or older population. 115,116 Arrhythmicity of gait has been related to falls in seniors, 117 -119 and there is a 12-fold increase in the odds of falling in persons older than 40 who have reported dizziness within the last year. 120 Mounting evidence also suggests that secondary factors such as fear of falling affect the recovery of patients with vestibular disorders. Anxiety and depression are also noted in persons with vestibular disorders, possibly as a result of their lack of movement, fear of becoming dizzy, and the social isolation that results from both. 121 -125
Intimately linked to the age-related changes in the vestibular system is the expression of vestibular migraine headaches, the most common cause of spontaneous episodic vestibular syndrome with a lifetime prevalence of about 1%. 126 Migraine and vertigo are common clinical conditions that affect approximately 14% and 7% of the general population, respectively. 127 Recent epidemiological surveys suggest that 3.2% of the general population have both migraine and vertigo. 128,129 Vestibular migraines are more common among migraineurs without aura and affect predominantly women, at a frequency of up to 5:1. 130,131
In 2009, Agrawal et al 120 estimated that as many as 35% of adults aged 40 years or older in the United States have experienced some form of vestibular dysfunction—a figure representing over 69 million Americans. The National Institute on Deafness and Other Communication Disorders estimates that 8 million (4%) American adults report a chronic problem with balance, whereas an additional 2.4 million (1.1%) report a chronic problem of dizziness alone. Eighty percent of people older than 65 years have experienced dizziness. These statistics would suggest that the full social and economic impacts related to the medical service providers for balance disorders are significantly underestimated. 132
Loci of Interest
Neuro-otological examination between episodes of dizziness is usually normal, and spontaneous and positioned nystagmus can be found during the attacks. Vestibular function tests are usually normal in almost half the patients, even though unilateral vestibular hypofunction and oculomotor disturbances are common. 133
The peripheral vestibular system is made up of 5 vestibular end organs. The 3 semicircular canals are responsible for angular acceleration; the 2 otolith structures, saccule and utricle, are responsible for linear acceleration (Figure 1).
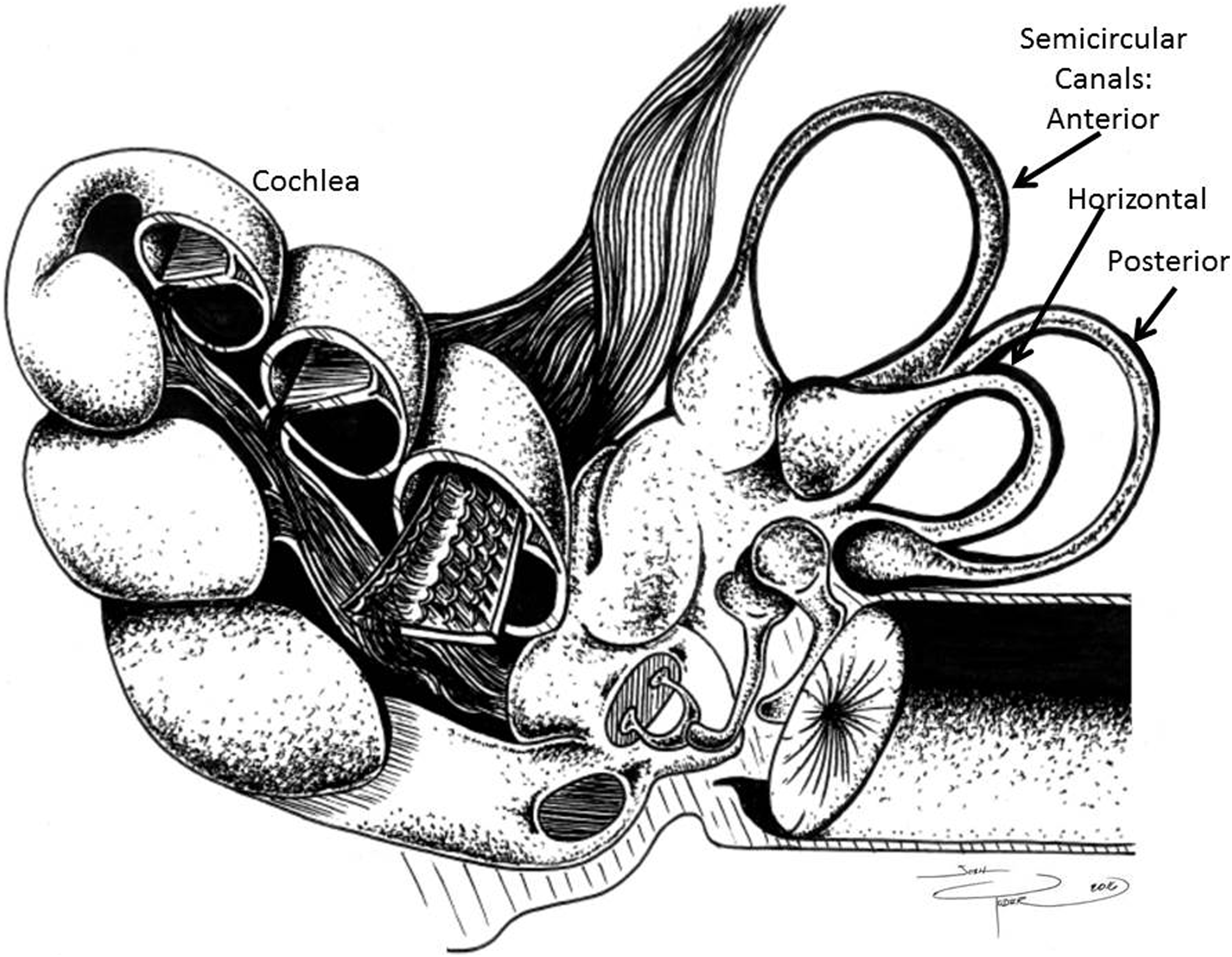
Diagram of inner ear organs to demonstrate differential axial planes of cochlea (auditory sensory organ) and vestibular otoliths. Drawn by J.D. Yoder, reprinted with permission of Elsevier (License Number 3851781511130).
Balance and vertigo are critically dependent on input from the otolith organs located in the auditory inner ear compartment. The semicircular canals and sacs in all vertebrates are attached to endolymphatic ducts. The saccule and utricle, in turn, together comprise the otolith organs. The otolith organs are sensitive to gravity and linear acceleration. Because of their orientation in the head, the utricle is sensitive to a change in horizontal movement, and the saccule provides information about vertical acceleration. Small crystals of calcium carbonate are found in the saccule and utricle, which under the influence of acceleration in a straight line, cause stimulation of the hair cells by their movement relative to the gelatinous supporting substrate containing the embedded cilia of the hair cells. The hair cells are made up of 40 to 70 stereocilia and 1 kinocilium, which are connected to an afferent nerve. When the body changes position or begins a movement, the weight of the membrane bends the stereocilia and stimulates the hair cells. Hair cells send signals down to sensory nerve fibers, which are interpreted by the brain as motion. The brain interprets the orientation of the head by comparing the input from the utricules and saccules from both ears to the input from the eyes, allowing the brain to discriminate head tilt from movement of the entire body. When the head is in a normal upright position, the otolith presses on the sensory hair cell receptors. This pushes the hair cell processes down and prevents them from moving side to side. However, when the head is tilted, the pull of gravity on otoliths shifts the hair cell processes to the side, mechanically distorting them and thereby initiating neuronal signaling that ultimately informs the CNS that the head is no longer level but now tilted.
The loss of vestibular hair cells from the mechanoreceptive sensory epithelia of the inner ear may result from several types of insult, leading to hearing loss and imbalance disorders. The mechanisms for hair cell death remain a topic of debate. There is some accumulating evidence that the initial and most extensive hair cell damage occurs in the apex of the cristae and in the striola regions of the utricular maculae. There has been mitochondrial swelling and extrusion of degenerating cells at the luminal surface that appear shortly following the onset of detectable changes in vestibular function. It is yet to be clearly demonstrated whether the extrusion is the actual mechanism of cell death induced by the cytotoxic drug or if it is a secondary response of the epithelium directed at tissue reorganization. Using terminal deoxynucleotidyl transferase dUTP nick end labelling immunocytochemistry, Lang and Liu 33 reported that apoptosis is a major path of cell death within mammalian vestibular sensory epithelium. The apoptotic labeling was most demonstrative at 3 to 7 days following pharmacological insult and appeared in the seminal layer of the cristae and utricular maculae, where only hair cell nuclei reside. The elimination of hair cells from the epithelium may occur through 2 different routes. One route involves extrusion and ejection to the luminal fluid. 134 -138 The second route occurs by expansion of supporting cells and removal of degenerating hair cells within the epithelium. 138 -140
Stance and gait are maintained by a complex neural network that can be disrupted by cerebrovascular accident (stroke), inflammation, trauma, toxicity, and neurodegenerative processes. 8 Movement is planned and initiated in the premotor, supplementary motor, and primary motor cortices. Cortical and subcortical frontal lobe dysfunction is considered to be an important factor in the age-related disequilibrium. 141 Inhibitory and stimulatory feedback loops involve the basal ganglia, cerebellum, brainstem nuclei, and the thalamus. 142 -144 Sensory input from the vestibular system is processed through the vestibular brainstem nuclei and projected to the cerebellum, reticular formation, the spinal cord, and the thalamus. 145 These integrated vestibular signals control automatic reflexes and motor coordination, and projections to the hippocampus and the vestibular cortex integrate spatial perception and orientation. 146
Studenski 147 suggested that gait speed alone is a powerful marker of patient health, regardless of diagnosis of a balance disorder. Generally, people who walk faster are healthier and live longer. Persons with vestibular disorders have disordered gait. Head movements during walking are particularly difficult for persons with vestibular disorders as they often veer with head movement and become dizzy. Persons with unilateral and bilateral vestibular loss often walk en bloc, with trunk and neck stiffness in order to minimize the amount of head movement during ambulation. This neck/trunk stiffness may result in a decreased vestibulo–ocular reflex (VOR) gain, which can lead to blurred vision when significant head movement occurs. Consequently, when engaging head movement during walking, many patients will become unstable and lose their balance, which increases the likelihood of falling. To promote recovery, head movements need to be encouraged, as patients can develop cervical pain from adopting a stiffened head/neck posture, and moving the head will improve the VOR gain, which will eventually improve overall gait function. 148
Conclusion
Direct, targeted, and toxic damage to the tissues in the small compartment of the eighth cranial nerve and associated sensory end organs is more than an inconvenience to those who have the consequences. Currently, there are no administrative guidelines from industry or US FDA on ototoxicity testing. The standard, core, text/reference books on toxicology, in general, do not even index the terms associated with ototoxicity screening or mechanisms of cell injury or death in any system related to auditory pathways, vestibular/balance control, or tinnitus.
The changes in a person’s quality of life, physical injuries linked to home falls, and the unrelenting and aversive noise of tinnitus or hyperacusis are a challenge for millions of patients who are prescribed drugs with the intent of improving their lives, yet toxicology textbooks don’t even mention the topic. Prescription compliance is in jeopardy when the physical and psychosocial costs of taking physician prescribed medications outweigh the benefits in terms of impact on quality of life. Pharmacological intervention directed toward the prevention or repair of drug-induced damage to the auditory system is ripe for targeting by drug development companies. There is a need for increased recognition that current therapeutic options must be expanded to truly fit the claim of safe and effective, including development efforts aimed at mitigating and eliminating adverse impacts on auditory and vestibular functions that are critical to an individual’s sense of well-being and quality of life.
Loss of balance, incoordination, and gait changes induced by prescription medicines are more than a nuisance to the patient. The inability to perceive auditory stimuli that may warn of impeding danger (ie, smoke alarms, car horns, the approach of emergency vehicles) poses a significant threat to those patients who, for example, complied with their doctor in taking a regimen of antibiotics for a recurring urinary tract infection. The onset of depression in the elderly patients who cannot escape the high-frequency sounds of tinnitus, awake, or asleep threatens their health-care compliance and may jeopardize the professional relationship between doctor and patient as well as the personal relationships between the patient and his or her family.
The small compartment of the eighth cranial nerve and sensory end organs of the inner ear serves functions that are subtly but inexorably linked to individual well-being and quality of life experience. Threats to the integrity of this small compartment, including those inadvertently associated with therapeutic drugs, accordingly pose considerable liabilities to the well-being of every patient taking approved pharmacological interventions that they expect to be safe as well as effective. As therapies in development continue to become ever more sophisticated and selectively targeted, reducing unwanted, off-target general toxicity, it is important that pharmaceutical developers carefully consider special categories of unintended toxicity that historically have drawn relatively little attention in safety testing and clinical practice. Ototoxicity is one such category of concern, which, if carefully considered and monitored in appropriate preclinical testing, clinical trials, and postmarketing phases, will yield significant gains in patient quality of life, consistent with the overall goals of drug development efforts.
Footnotes
Author Contributions
David Gauvin contributed to conception and design and acquisition. Joshua Yoder contributed to design, acquisition, analysis, and interpretation. Rachel Tapp contributed to conception and design and analysis and interpretation. Theodore Baird contributed to conception and design and acquisition, analysis, and interpretation. All authors drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy. All contributors assisted in literature review, consolidation, and preparation of the manuscript.
Authors’ Note
This manuscript was considered “work product” as a function of employment at MPI Research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.