
Abstract
Background:
Since their introduction in 2004, electronic cigarettes (e-cigarettes) have gained popularity worldwide. E-cigarettes are marketed as nicotine delivery devices. Commonly reported reasons for use include to quit smoking, to reduce urge to smoke, or the perceived lower risk alternative to smoking. But what are the actual amounts of nicotine delivered?
Aim:
This review summarizes all the published studies concerning nicotine or cotinine levels following e-cigarette use.
Methods:
A literature search was conducted from the PubMed database, from 1985 to January 2014, using the following terms: electronic cigarette(s), e-cigarette(s), electronic nicotine delivery system, cotinine, and nicotine. Articles were excluded if they were not pertinent according to our criteria. References of all relevant articles were also evaluated.
Results:
Eight studies were included in this review. The following information was extracted from the articles: population size, age of participants, recruitment, inclusion and exclusion criteria, concentration of nicotine in refills liquids, study sample design, and observed concentrations. Following design of studies, plasma nicotine Cmax was observed between 0 and 5 ng/mL (no significant changes) or between 13.9 and 16.3 ng/mL (similar to a tobacco cigarette) with a Tmax between 70 and 75 minutes. Cotinine levels after “vaping” an e-cigarette are similar to a tobacco cigarette.
Conclusion:
This review summarizes e-cigarette studies that contain information on nicotine or cotinine levels. The peak concentration of nicotine appears to be dependent on the use and dose level of e-cigarette cartridge. The value of this peak concentration is similar to the value found with a tobacco cigarette. However, the time corresponding to the peak concentration is delayed compared to a tobacco cigarette.
Introduction
Tobacco smoking constitutes a major public health crisis causing an estimated 73 000 deaths per year in France alone, 1 yet 34% of the population continue to smoke. 2
Use of electronic cigarette (e-cigarettes), referred to as vaping, is a relatively new phenomenon that is quickly gaining the interest of many long-time tobacco smokers. Since their launch in 2004, e-cigarettes, a diverse range of battery operated devices that vaporize nicotine for inhalation, have been purchased by millions of people. 3
E-cigarettes are becoming a preferred alternative for nicotine delivery among many smokers because of their realistic look, feel, and taste compared to traditional cigarettes. E-cigarette liquid contains glycerol and/or propylene glycol, flavorings, nicotine (0-24 mg/mL), and other additives.
Nicotine delivery via tobacco smoke (cigarette) is absorbed within 10 to 20 seconds in high concentration through the lungs into the bloodstream, reaching the brain in the same high concentration within 10 seconds. Within 10 minutes of smoking, plasma nicotine peak at 15 to 30 ng/mL. 4,5 By contrast, nicotine absorbed via commercially available nicotine replacement therapy (NRT) such as patch, inhaler, and gum is much slower or never reaching the peak achieved via tobacco smoking. 4 -6 Few studies have explored plasma nicotine and plasma and saliva cotinine levels via delivery from an e-cigarette. 7 -14
Nicotine is one of the major constituents of mainstream cigarette smoke. In humans, approximately 70% to 80% of absorbed nicotine is metabolized to cotinine. 4 The elimination half-life of cotinine is much longer than that of nicotine, 4 and diurnal variation in cotinine is smaller than that of nicotine in smokers. There is a good dose–response relationship of plasma cotinine to daily cigarette consumption. 15 Based on the fact mentioned earlier, plasma cotinine has been used as an exposure marker of cigarette smoke, including individuals’ smoking status. 15,16
In order to face this new challenge, health care professionals will need to be informed of the available scientific evidence-based literature concerning nicotine and cotinine levels after “vaping” an e-cigarette. Using an e-cigarette is known as “vaping,” and regular users often refer to themselves as “vapers.” The act of “vaping” has been portrayed as a nontobacco mimic that smokers can use to reduce the amount of cigarette consumption, almost like a smoking cessation tool. Consequently, the aim of this article is to provide a review of the current literature concerning nicotine and cotinine levels after “vaping” e-cigarettes.
Method
Inclusion Criteria
We included studies on e-cigarettes. The articles were accepted if they met the following inclusion criteria: - samples of nicotine and/or cotinine levels were analyzed, - all populations, and - all brands.
Exclusion Criteria
We excluded studies on e-cigarettes if they met the following exclusion criteria: - no samples of nicotine or cotinine levels were reported and - non-English written papers.
Data Extraction
A literature search of original articles was conducted using PubMed in January 2014, using the following key words: (electronic cigarette(s) AND nicotine) OR (electronic cigarette(s) AND cotinine) OR (e-cigarette(s) AND nicotine) OR (e-cigarette(s) AND cotinine) OR (Electronic Nicotine Delivery System (ENDS) AND nicotine) OR (ENDS AND cotinine). Then, based on the abstract, articles were selected according to our criteria of inclusion, that is, articles describing studies on e-cigarettes with nicotine and/or cotinine samples.
This review aims to evaluate all studies with reported nicotine plasma/cotinine plasma or saliva levels after e-cigarettes use. The following information was extracted from the articles: number of participants, age, sex, concentration of nicotine in liquids refills, samples design, and measured concentrations.
Results
A total of 120 citations were produced after the search was performed, and only 8 of these were included in relation to our inclusion criteria. These 8 remaining articles were then analyzed. 7 -14
Study Characteristics
The 8 articles described studies on nicotine and/or cotinine levels after e-cigarettes use and were published between 2010 and 2014. Table 1 shows study recruitment and demographics.
Demographic and Recruitment Data.
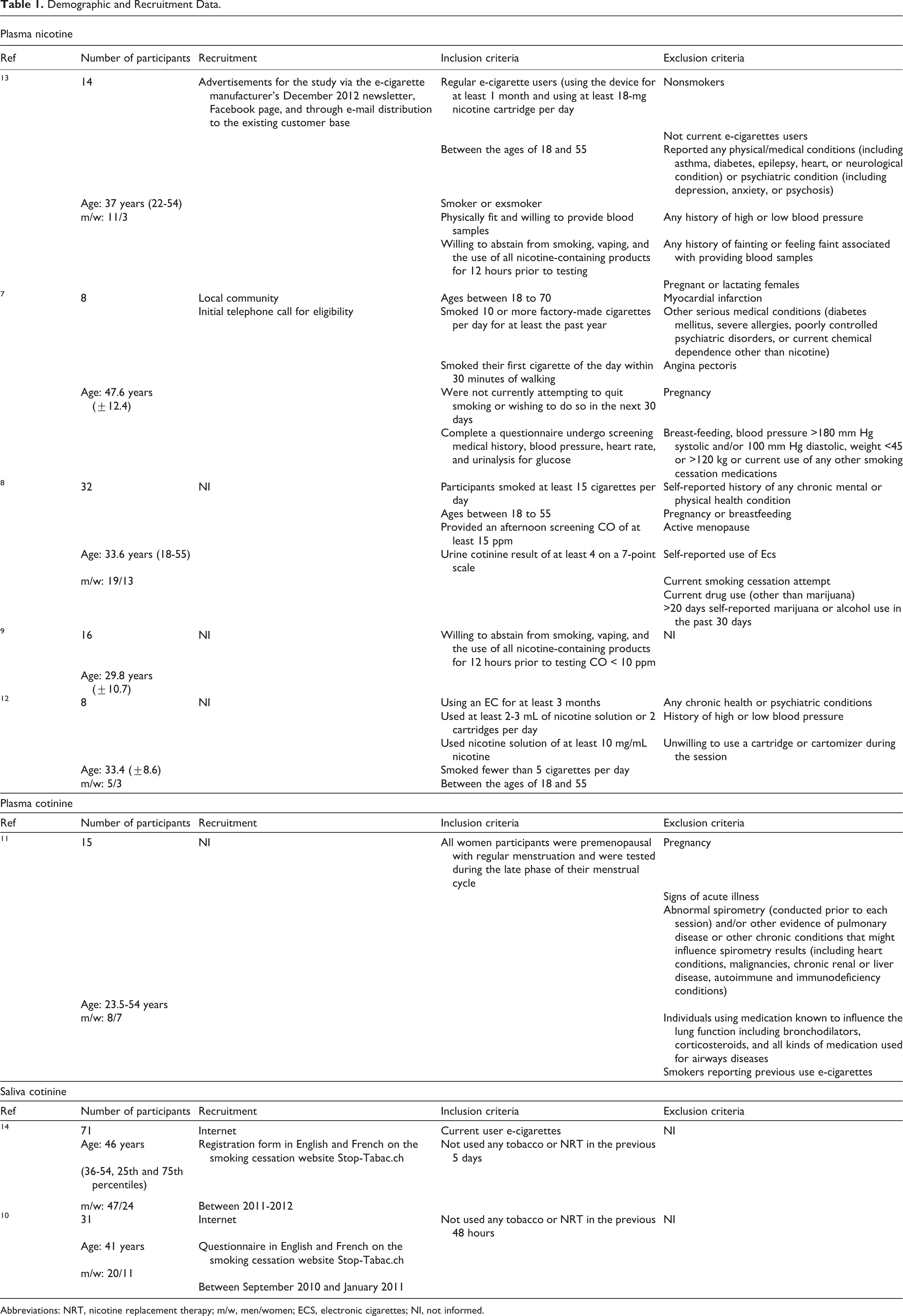
Abbreviations: NRT, nicotine replacement therapy; m/w, men/women; ECS, electronic cigarettes; NI, not informed.
Data Summary
Table 2 summarizes sample collection designs and measured concentrations of these 8 studies. There is a severe lack of published data regarding the levels of nicotine and/or cotinine after “vaping” an e-cigarette: only 5 studies on plasma nicotine levels, 1 on plasma cotinine levels, and 2 on saliva cotinine levels.
Sample Collection Designs and Measured Concentrations.a
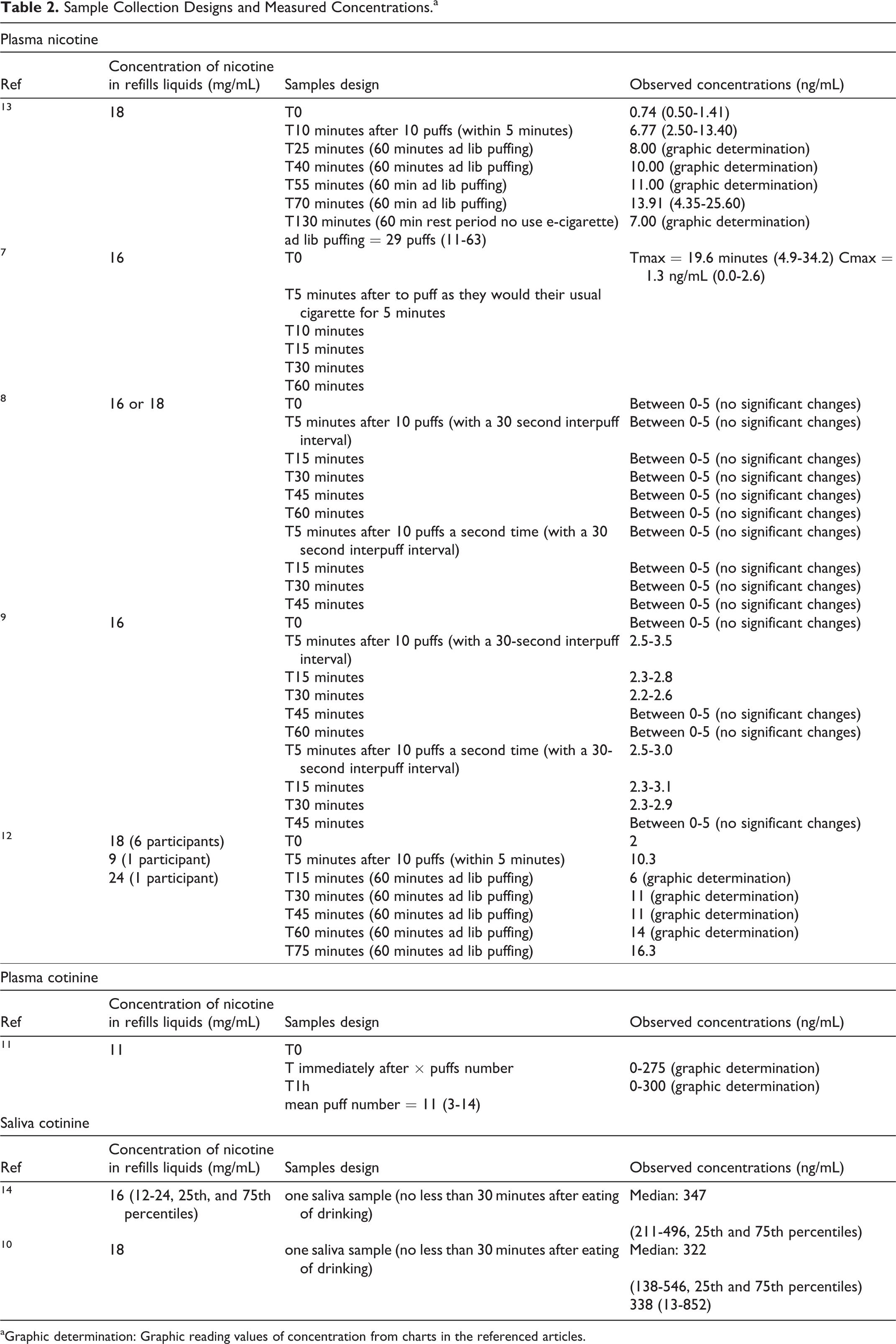
aGraphic determination: Graphic reading values of concentration from charts in the referenced articles.
Regarding the studied populations, they were similar for 6 articles. They were volunteers, male or female, aged approximately 18 to 55 years, and regular e-cigarettes users. 9 -14 For the 2 other studies, the participants were also volunteers, male or female, aged 15 to 55 years, but they were inexperienced e-cigarettes users. 7,8
A review of these 8 studies demonstrated that the dosages of nicotine in cartridges varied between brands ranging from 9 to 24 mg/mL (mean 16-18 mg/mL). In addition, the sampling time points were different according to the measured variable. For studies on plasma concentrations of nicotine, the pattern is similar for the different studies with time points at T0 and 5 or 6 samples between 5 and 130 minutes after different “vaping” patterns: a fixed number of puffs or a fixed number plus a 60-minute ad lib period or a free number of puffs. 7,8,9,12,13 For studies on plasma or saliva cotinine concentrations, the number of samples was much smaller with only a single saliva sample or 2 plasma samples. 10,11,14
In respect to the observed concentrations, the plasma nicotine concentrations were different depending on the design of the study. For the 3 studies where there was only 1 phase of 10 puffs and then a series of samples, the results were similar with plasma nicotine concentrations measured between 0 and 5 ng/mL. For the 2 studies in which there was a phase of 10 puffs and a 60-minute ad lib puffing period, we found similar kinetics with maximum plasma concentrations of nicotine ranging between 13.9 and 16.3 ng/mL. 12,13 Second, for the plasma cotinine concentrations, the measured concentrations were between 0 and 300 ng/mL after a number of free puffs. 11 Finally, for the saliva cotinine concentrations, the 2 studies followed the same design and had the same median measured concentrations ranging between 322 and 347 ng/mL. 10,14
Discussion
Electronic cigarettes are new products available on international markets. E-cigarettes look like cigarettes but do not burn tobacco, rather they vaporize it. Depending on the brand, cartridges contain nicotine or not and different flavors. In addition to the delivery of nicotine, the visual, sensory, and behavioral aspects of these devices are purported to be similar to tobacco cigarettes. The efficacy of e-cigarettes as a means of aiding smoking cessation is likely dependent largely on their ability to deliver nicotine to the brain at adequate doses and speeds, thus pharmacokinetic and pharmacodynamic studies are important in this regard.
First, regarding the cotinine levels, cotinine levels are roughly similar when measured in plasma or in saliva, 17 -19 so the 3 studies using cotinine in plasma and in saliva can be compared. Participants of each study had not used NRT or smokeless tobacco for ≥48 hours minimum (5 days for the study of Etter 14 ), about 3 times the half-life of cotinine in smokers 19 but had used e-cigarette. Thus, results are unlikely to be contaminated by other sources of cotinine. The 3 studies on saliva or plasma cotinine levels showed similar results with substantial amounts of cotinine in e-cigarette users (138-548 ng/mL). 10,11,14 These 3 studies concluded that the effect of e-cigarette smoking on plasma or saliva cotinine levels is similar to that generated by tobacco cigarette smoking. However, these studies demonstrate interindividual differences in cotinine levels. Interindividual differences in cotinine levels could result from several factors, some of which were measured in these studies (prior level of tobacco dependence, nicotine content in e-liquids, number of puffs, and e-cigarette brand), and some which were not assessed, for example, electric power of the device, vapor temperature and density, nicotine concentration in the vapor (vs in liquids), volume of puffs, depth of inhalation, duration of apnea between inhalation and exhalation, and each individual’s specific nicotine metabolism, but the major factor is the number of puffs. Indeed, the study of Etter et al 10 described a correlation between puff number and cotinine and concluded that “puffing topography is an important factor that should be controlled for in future studies p.1220” In the study of Flouris et al, 11 the puffs number is referenced but the presented data do not show the relationship between puffs number and cotinine level.
Regarding the nicotine levels, only 2 studies show reliable nicotine delivery after acute administration using e-cigarette. 12,13 These 2 studies show significantly elevated plasma nicotine levels and positive subjective effects (such as hit, satisfaction, pleasant, feels like smoking, … ) in regular e-cigarette users (using the device for at least 1 month and using at least one 18-mg nicotine cartridge per day). The design of these 2 studies was similar to that of a tobacco smoker, with a 10-puffs period (within 5 minutes) followed by a 60-minute ad lib puffing period. The observed nicotine concentrations from an e-cigarette were similar to a tobacco cigarette with a maximal concentration between 13.9 and 16.3 ng/mL with e-cigarette vaping 12,13 versus around 15 ng/mL from a tobacco cigarette smoking. 4,15 The main difference between plasma nicotine from the use of e-cigarette or tobacco cigarette is the time for which the maximum concentration is reached (Tmax). After 1 tobacco cigarette (5 minutes), the maximum concentration is reached in only 5 to 8 minutes, 4 whereas during use of an e-cigarette, the maximum concentration is reached in 70 to 75 minutes. 12,13 This difference in Tmax implies that e-cigarettes are likely to be less addictive than tobacco cigarettes because they deliver nicotine more slowly. 7 The study of Bullen et al 7 concluded that in the first hour, the e-cigarette showed a pharmacokinetic profile more like a nicotine inhaler than a tobacco cigarette. The 3 other studies followed a different design with only two 10-puffs bouts (with a 30 seconds interpuff interval) or to puff as they would their usual cigarette for 5 minutes. 7 -9 Conclusions from these studies are that no significant changes in nicotine levels are observed when e-cigarettes use is limited to use similar to that of a smoker. The plasma nicotine concentration increased more slowly and it took longer to reach Tmax in e-cigarette use compared to tobacco cigarette use. One of the reasons for this result could be the difference in the duration of the aspiration or puff time set for the study regimen: participants spent approximately 65 minutes for 40 puffs when using e-cigarette and approximately 5 minutes for 10 puffs of tobacco cigarette.
These different studies show a high variability in cotinine and nicotine levels. Occasional versus chronic use and/or more intensive puffing (ie, more puffs, greater puff volume) may influence nicotine delivery.
In summary, this review revealed that regular e-cigarette users have measurable plasma nicotine and cotinine levels after acute administration using e-cigarettes. The urge to smoke and nicotine-related withdrawal symptoms (irritability, restlessness, and poor concentration) could be reduced with e-cigarette use because e-cigarettes deliver nicotine more slowly, the Tmax is reached after 70 to 75 minutes of a continuous use compared to within 10 minutes with regular cigarettes. Even if e-cigarettes can reliably deliver nicotine in regular users, there is some variability. Other reports suggest that e-cigarettes are probably less addictive than tobacco cigarettes. 20 These results have important implications for the regulation of e-cigarettes, for smokers who want to quit, for clinicians, and for researchers.
Thus, an important area for future research is the parametric manipulation of devices characteristics (brand, content liquid, and nicotine concentration … ) and user behavior (ie, puff topography) that might contribute to safety and efficacy. Other studies are necessary to confirm these results.
Footnotes
Author Contributions
Marsot contributed to conception and design and contributed to acquisition, analysis, and interpretation. Simon contributed to design and contributed to analysis and interpretation; both authors drafted manuscript, critically revised manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.