
Abstract
The cost of dexrazoxane, a drug used to provide protection from doxorubicin-induced cardiotoxicity, limits its use in low-income countries. We aimed to see whether schisandrin B, an inexpensive drug, could provide protection equivalent to that provided by dexrazoxane. New Zealand white rabbits were randomly divided into groups and treated with saline, doxorubicin, doxorubicin + dexrazoxane, or doxorubicin + schisandrin B. Doxorubicin-induced damage and the protective effects were studied by recording the echocardiographic parameters and serum levels of superoxide dismutase, malondialdehyde, cardiac troponin I, and brain natriuretic peptide and observing the histology and degree of apoptosis. Schisandrin B had dose-dependent effects in decreasing the magnitude of doxorubicin-induced indicators of cardiomyopathy to a degree that approximated the decrease produced by dexrazoxane treatment. Schisandrin B might be a useful, low-cost alternative drug for this application.
Introduction
The anthracycline anticancer drug doxorubicin (DOX) has been widely used to treat leukemia, lymphoma, breast cancer, and other malignant tumors. However, its clinical application is limited because of its cardiotoxicity.1–5 Doxorubicin-induced cardiotoxicity is thought to be mainly due to the production of free radicals both through a nonenzymatic pathway involving an anthracycline–iron chelate and through an enzymatic pathway utilizing the mitochondrial respiratory chain. 6 ,7 Doxorubicin also reduces myocardial levels of 2 major antioxidant enzymes, superoxide dismutase (SOD) and glutathione peroxidase (GSH-PX). The resulting imbalance between free radical production and antioxidant activity allows free radicals to accumulate and cause mitochondrial and microsomal lipid peroxidation, actions that eventually lead to cardiomyocyte injury and death. 8 Indirect evidence of free radical buildup and damage in DOX-caused cardiomyopathy is the increased production of malondialdehyde (MDA), a free radical lipid peroxidation product.
Dexrazoxone (DEX), a prodrug hydrolyzed enzymatically into an EDTA-like iron chelator, is a cardioprotective agent used clinically to prevent DOX-induced cardiotoxicity. However, its expense limits its use in low-income countries. Schisandra is a widely used Chinese herbal medicine with the effects of astringency and hemostasis. Schisandrin B (SchB), an active ingredient extracted from Schisandra (Figure 1 ), has a strong free radical elimination effect with few or no side effects and is easily available and less expensive than dexraxozone. 9 In China, 250 mg of DEX costs about $75, and although no therapeutic grade SchB is currently available for clinical use, the cost would be about $0.15 for a daily dose. Therefore, we hypothesized that SchB might be a clinically useful drug to prevent or eliminate DOX-induced cardiotoxicity.
Chemical structure of schisandrin B: CAS:61281-37-6, C23H28O6, molecular weight is 400.47.
In the current study, a rabbit model of DOX-induced cardiotoxicity 10 was used to compare the cardioprotective effects of SchB and DEX and to investigate their mechanisms, as a first step toward providing guidance for the development of clinically useful, cost-effective cardioprotective drugs.
Materials and Methods
Animal Selection
A total of 150 healthy New Zealand white rabbits, weight 1.98 ± 0.15 kg, male and female in equal numbers, were obtained from Animal Laboratory Center, West China School of Basic Medicine, Sichuan University. The study was approved by the Institutional Animal Care and Use Committee of our institution.
Research Methods
Reagents
Doxorubicin (lot number 070902A) was purchased from Zhejiang Hisun Pharmaceutical Co, Ltd (Taizhou City, Zhejiang Province, PR China); DEX (lot number 070901) from Yangzhou AoSaikang Pharmaceutical Co, Ltd (Nanjing, Jiangsu Province, PR China); and SchB (purity >99%) from Chengdu Mansite Pharmaceutical Co, Ltd (Chengdu, Sichuan, PR China). Schisandrin B was dissolved in 95% medical-grade ethanol after cobalt-60 radiation sterilization and diluted with injection-grade water, to make a final ethanol concentration of 10%. Superoxide dismutase and MDA assay kits were purchased from Nanjing Jiancheng Institute of Biology (Nanjing City, PR China); troponin I (TnI) and brain natriuretic peptide (BNP) assay kits were purchased from Chengdu BoRuike Biotechnology Co, Ltd, UTL; and terminal deoxynucleotidyl transferase (TdT)–mediated dUTP nick end labeling (TUNEL) kits were purchased from Roche in the United States.
Experimental Groups and Drug Administration Methods
A total of 150 New Zealand white rabbits were randomly divided into the following 6 groups: control, DOX, DOX + DEX, DOX + SchB1 (schisandrin B 5 mg/kg), DOX + SchB2 (schisandrin B 10 mg/kg), and DOX + SchB3 (schisandrin B 15 mg/kg). The normal control group (n = 24) received weekly intravenous (iv) injections of 1 mL of normal saline; and the DOX group (n = 26) received weekly iv injections of 3 mg/kg of DOX. The DOX + SchB1 group (n = 25) received weekly DOX injections, as above, and iv injection of 5.0 mg/kg of SchB, twice a week; the DOX + SchB2 group (n = 26), weekly DOX injections and iv injection of 10.0 mg/kg of SchB, twice a week; and the DOX + SchB3 group (n = 24), weekly DOX injections and iv injection of 15.0 mg/kg of SchB, twice a week. The DOX + DEX group (n = 25) had weekly intraperitoneal injection of 60 mg/kg of DEX for the first 4 weeks, after 30 minutes followed by iv injection of DOX. However, this caused peritoneal irritation and, starting from the fifth week, administration of DEX was changed to weekly iv injection. Dosage and usage of DOX were unchanged. The dosage of DEX used was the dose reported to give maximum protection in a dose-response study by Plande et al. 11 The doses of SchB were chosen based on a previous study that used an incompletely purified preparation and adjusted to take into account the >99% purity of our preparation. 12 Study duration for all groups was 10 weeks.
Observation and Detection Parameters
General
Rabbits in each group were observed daily for appetite and activity level. Body weight was measured once a week. The number of deaths was recorded and the survival rate was calculated.
Serum SOD, MDA, Cardiac TnI, and BNP Levels
At baseline and at the end of the 4th and 10th weeks, central artery blood was taken from the ear for determination of serum markers of cardiac function. Serum SOD levels were determined by a xanthine oxidase method, MDA levels by a thiobarbituric acid method, and cardiac TnI (cTnI) and BNP levels by an enzyme-linked immunosorbent assay (ELISA).
Cardiac Function Changes
Philip Sonos 7500 transthoracic echocardiography was used for detection of changes in cardiac function. A S12 type cardiac ultrasonic probe with a frequency of 8 MHz, superficial organ mode, and a scanning speed of 150 mm/s was chosen. The section for ultrasound was a parasternal left ventricular long-axis view. Ultrasonic measuring parameters included left ventricular diastolic dimension (LVDD), left ventricular systolic dimension (LVSD), interventricular septal thickness (IVST), posterior wall thickness (PWT), left ventricular ejection fraction (LVEF), left ventricular fractional shortening (LVFS), and heart rate (HR).
Myocardial Pathological Changes
At the end of the 10th week, rabbits were anesthetized by iv injection of 30 mg/kg pentobarbital sodium and sacrificed. The free wall of their left ventricular section was placed in 10% neutral formaldehyde solution, fixed, sliced following paraffin embedding, stained in hematoxylin and eosin (H&E), and observed under light microscopy. Pathological scores were calculated using the Billingham scoring method, which is based on vacuolization and/or percentage of cardiomyocytes with muscle fiber depletion. 1 In this method, 0 = no cardiomyocyte injury; 1 = ≤5%; 1.5 = 6% to 15%; 2 = 16% to 25%; 2.5 = 26% to 35%; and 3 = ≥36%.
Cardiomyocyte Apoptosis
The TUNEL assay was used to determine cardiomyocyte apoptosis. A total of 5 myocardial views were randomly chosen for each section, the TUNEL-positive cells and the total number of cells were counted in each high-resolution field, and the apoptotic index calculated. Average apoptotic index was calculated based on 5 views. Apoptotic index = (number of apoptotic cells/number of total cells) × 100.
Statistical Analysis
The mean and standard deviation of continuous variables were summarized for each time point. A linear mixed model with a Bonferroni correction was used to evaluate group effects on serum blood and cardiotoxicity parameters. The group effects were presented as estimated marginal means (EM means) and the corresponding 95% confidence intervals (CIs) with adjustment for time effects. To compare cell apoptosis, Billingham score, and the blood serum results at week 10 in each group, nonparametric Kruskal-Wallis tests were performed with a Bonferroni adjustment due to small sample size. To handle missing data due to mortality, the cases in the corresponding group were considered a random sample of the total number of levels in the population, that is, as a random effect in the linear mixed model. Analysis of deaths was performed using Kaplan-Meier survival curves, and Breslow test was used to compare these curves. Statistical significance was set at .05. Statistical analyses were performed with the SPSS 15.0 software package (SPSS Inc, Chicago, Illinois).
Results
General
Histology
Light microscopy of biopsy specimens from the normal control group (Figure 2A) showed a regular arrangement of healthy myocytes and no inflammatory cells. In contrast, in the DOX group (Figure 2B), the majority of the cardiomyocytes looked swollen and showed vacuolated degeneration. Some nuclei have degenerated and do not clearly pick up the hematoxylin stain well. The space between cardiocytes had significantly widened, due to interstitial fibrosis and a large infiltration of heterophils consistent with coagulative necrosis. Light microscopy in the DOX + DEX group (Figure 2C) showed partial vacuolated degeneration and edema in cardiomyocytes, accompanied by an inflammatory cell infiltration and a small amount of necrosis, but less than that in the DOX group. The degree of myocardial injury in each of the DOX + SchB groups (Figure 2D) was also less than that seen in the DOX group, and the higher the dose of SchB, the less the myocardial injury.
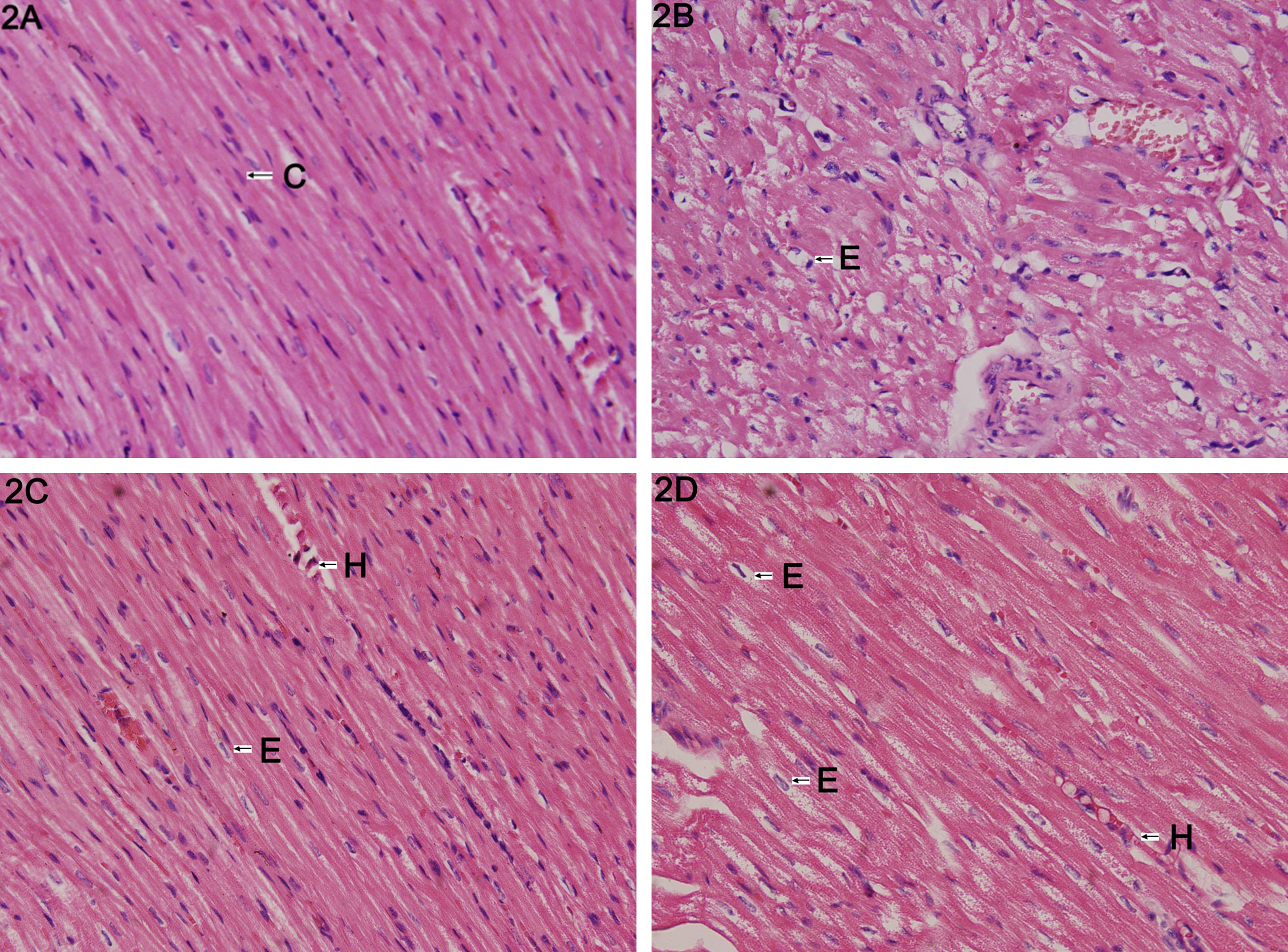
Light microscopy (×400) of hematoxylin and eosin (H&E)–stained biopsy specimens of rabbit cardiomyocytes from normal control (Panel A); following treatment with doxorubicin showing swollen cardiomyocytes with vacuolated degeneration and interstitial fibrosis (Panel B); following treatment with doxorubin + dexrazoxane showing changes less severe than those in Panel B (Panel C); and following treatment with doxorubicin + high-dose schisandrin B (Panel D). C indicates cardiomyocytes; H, heterophils; E, cellular edema.
Weight
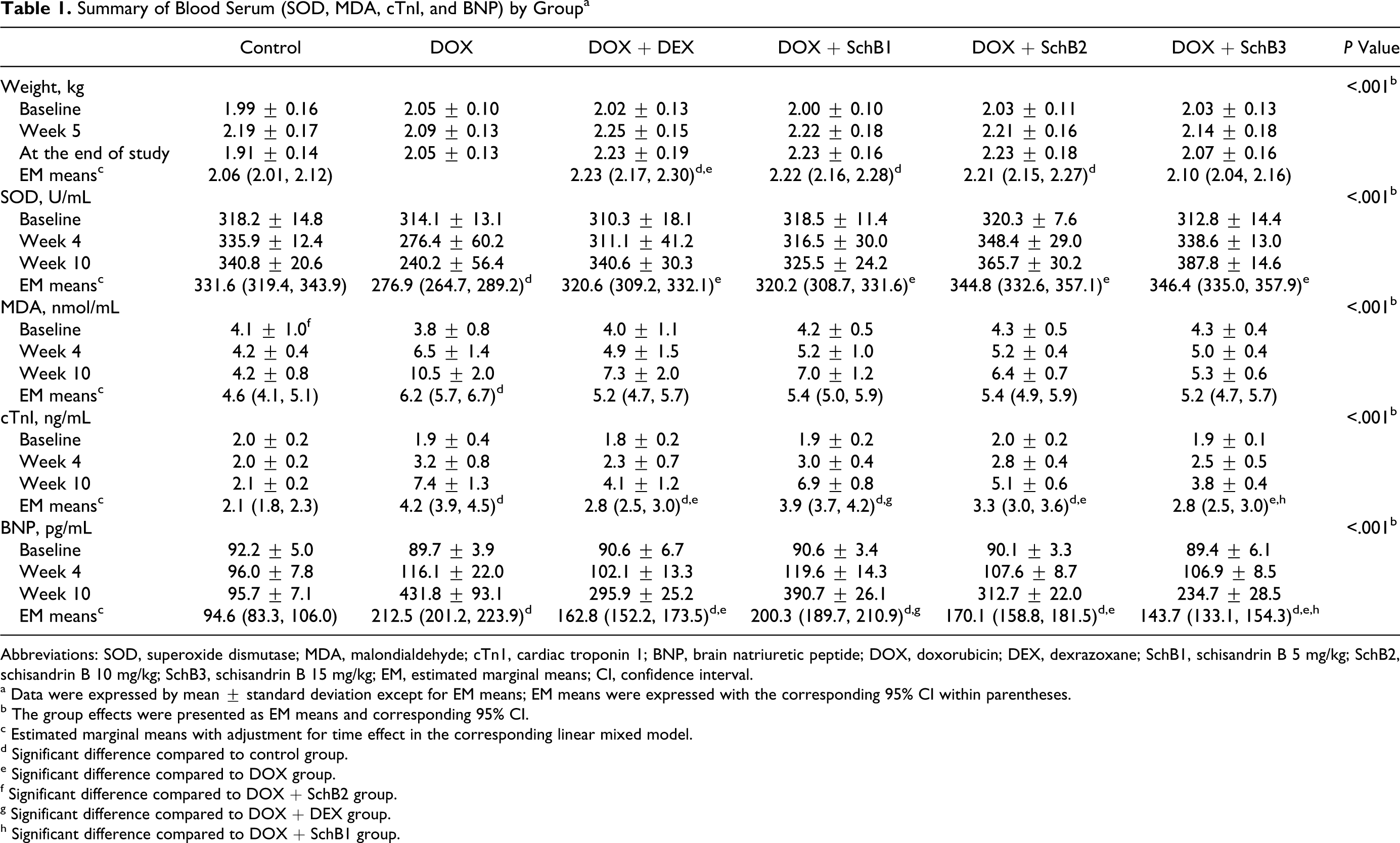
Animal weights in the control, DOX, and DOX + SchB3 groups were similar and did not change significantly from baseline during the study period. Animals in the DOX + DEX and 2 lower-dose DOX + SchB groups gained weight. In the case of the DEX group, the animal weights were also significantly higher than in the DOX group by the end of the study (Table 1 ).
Summary of Blood Serum (SOD, MDA, cTnI, and BNP) by Group a
Abbreviations: SOD, superoxide dismutase; MDA, malondialdehyde; cTn1, cardiac troponin 1; BNP, brain natriuretic peptide; DOX, doxorubicin; DEX, dexrazoxane; SchB1, schisandrin B 5 mg/kg; SchB2, schisandrin B 10 mg/kg; SchB3, schisandrin B 15 mg/kg; EM, estimated marginal means; CI, confidence interval.
a Data were expressed by mean ± standard deviation except for EM means; EM means were expressed with the corresponding 95% CI within parentheses.
b The group effects were presented as EM means and corresponding 95% CI.
c Estimated marginal means with adjustment for time effect in the corresponding linear mixed model.
d Significant difference compared to control group.
e Significant difference compared to DOX group.
f Significant difference compared to DOX + SchB2 group.
g Significant difference compared to DOX + DEX group.
h Significant difference compared to DOX + SchB1 group.
Survival
Figure 3 shows Kaplan-Meier survival curves for each group. There was no significant difference in mortality among the groups (P = .274).
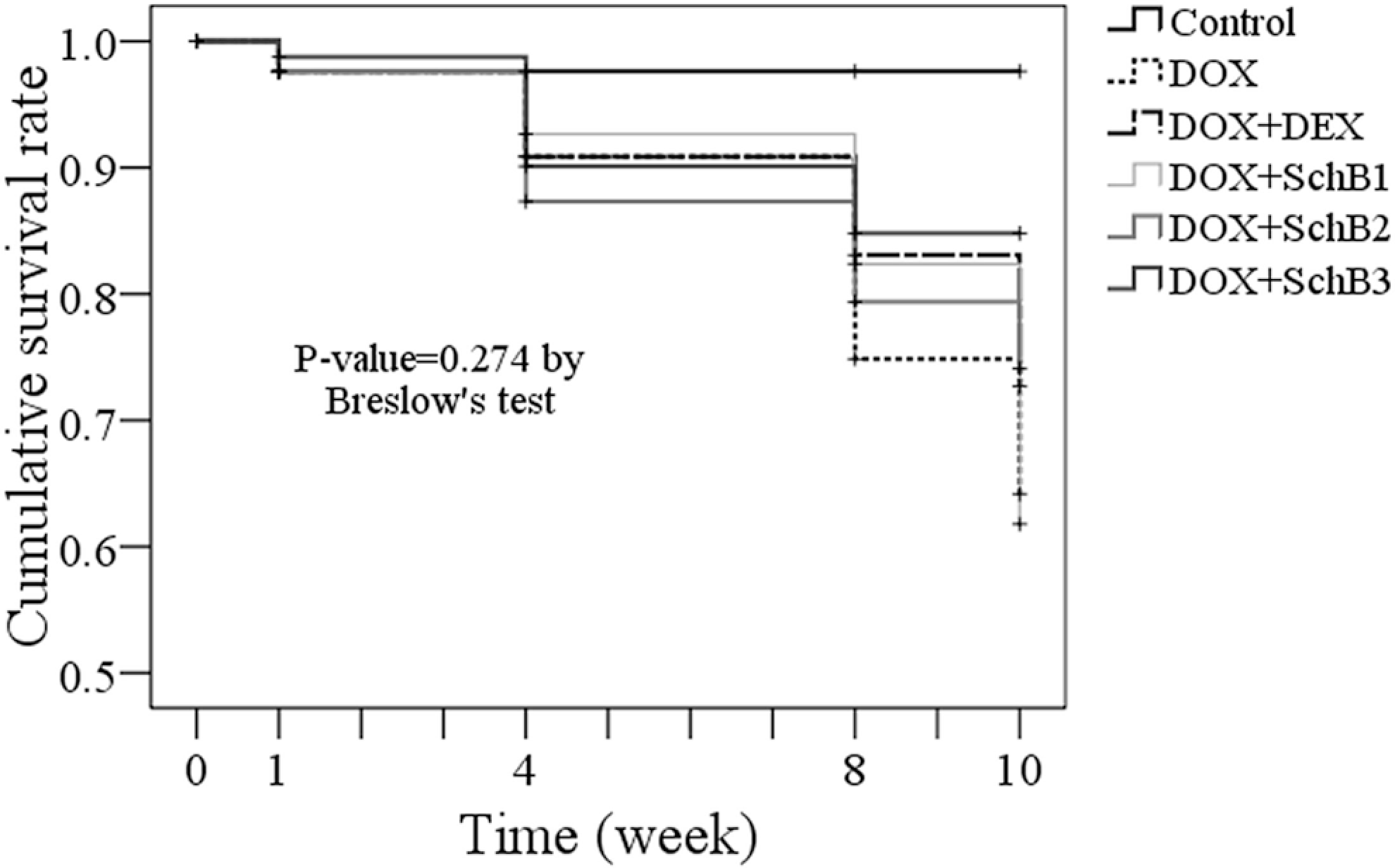
Kaplan-Meier survival curves for control, DOX, DOX + DEX, and DOX + SchB groups showing no significant survival differences among the groups. DOX indicates doxorubicin; DEX, dexrazoxane; SchB1, schisandrin B 5 mg/kg; SchB2, schisandrin B 10 mg/kg; SchB3, schisandrin B 15 mg/kg.
Blood Serum Biomarkers
Superoxide dismutase
Levels of the antioxidant enzyme, SOD, for the DOX group were significantly decreased compared to the control group. All 4 treatments (DEX, SchB1, SchB2, and SchB3) restored this enzyme to control levels, and a dose effect was seen with increasing doses of SchB (Table 1).
Malondialdehyde
Levels of the reactive oxygen species (ROS) marker, MDA, remained stable with time in the control group, and increased with time in the other 5 groups. Malondialdehyde levels in the DOX group were significantly higher than in the control group. The DEX and all 3 SchB-treated groups showed significantly lower increases in this marker compared to the DOX group, and a dose effect was seen with increasing doses of SchB. At week 10, the MDA level in the DOX group was significantly higher than in the control group; MDA levels in the DOX + DEX, DOX + SchB1, and DOX + SchB2 groups were significantly decreased compared to that in the DOX group but were still higher than that in the control group; in the high-dose, DOX + SchB3 group, the MDA level, although higher, was not significantly different from that of the control group (Table 1).
Cardiac troponin I
Levels of the marker for myocardial injury, cTnI, increased with time in the DOX group and became significantly higher than control levels. All 4 treatments reduced the elevated cTnI levels seen in the DOX group and this trend reached statistical significance in the DOX + DEX and the 2 higher-dose SchB groups. As in the SOD and MDA results, a dose effect was seen with SchB. However, cTnI was not reduced to control levels in any treatment group (Table 1).
Brain natriuretic peptide
Levels of the second marker for cardiomyocyte damage, BNP, also did not increase above baseline levels in control animals. In contrast, in the DOX group, the BNP levels increased more than 4-fold by the end of the experiment. All 4 treatments lessened this increase and a dose effect was seen with SchB. However, as with cTnI, no treatment brought the BNP levels completely back to control values (Table 1).
Echocardiography
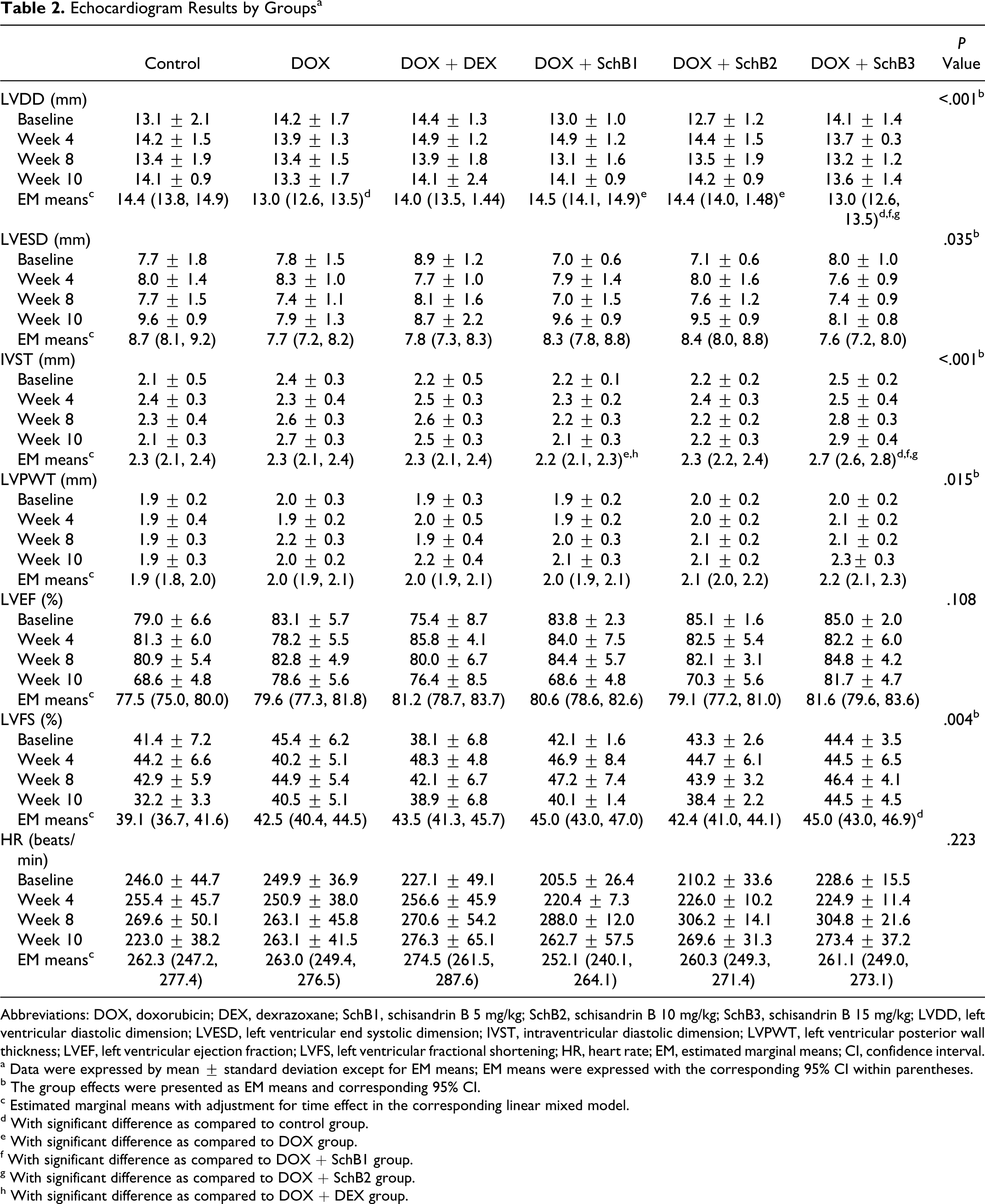
Echocardiogram results, including LVDD, left ventricular end systolic dimension (LVESD), IVST, left ventricular posterior wall thickness (LVPWT), LVEF, LVFS, and HR, are summarized in Table 2 . Doxorubicin treatment significantly decreased LVDD compared to control, and this DOX-induced decrease was lessened in the SchB1- and SchB2-treated groups.
Echocardiogram Results by Groups a
Abbreviations: DOX, doxorubicin; DEX, dexrazoxane; SchB1, schisandrin B 5 mg/kg; SchB2, schisandrin B 10 mg/kg; SchB3, schisandrin B 15 mg/kg; LVDD, left ventricular diastolic dimension; LVESD, left ventricular end systolic dimension; IVST, intraventricular diastolic dimension; LVPWT, left ventricular posterior wall thickness; LVEF, left ventricular ejection fraction; LVFS, left ventricular fractional shortening; HR, heart rate; EM, estimated marginal means; CI, confidence interval.
a Data were expressed by mean ± standard deviation except for EM means; EM means were expressed with the corresponding 95% CI within parentheses.
b The group effects were presented as EM means and corresponding 95% CI.
c Estimated marginal means with adjustment for time effect in the corresponding linear mixed model.
d With significant difference as compared to control group.
e With significant difference as compared to DOX group.
f With significant difference as compared to DOX + SchB1 group.
g With significant difference as compared to DOX + SchB2 group.
h With significant difference as compared to DOX + DEX group.
The EM mean for IVST was significantly lower in the DOX + SchB1 group than the DOX and DOX + DEX groups, and significantly higher in the DOX + SchB3 group than in the control, DOX + SchB1, and DOX + SchB2 groups. The EM mean for LVFS in DOX + SchB3 group was significantly higher than that in the control group.
Cell Apoptosis and Billingham Score
The addition of DEX significantly decreased the degree of apoptosis seen in the DOX-treated myocardium. Schisandrin B administration decreased apoptosis in a dose-dependent manner, the highest dose of this compound having an effect comparable to DEX (Figures 4 and 5).
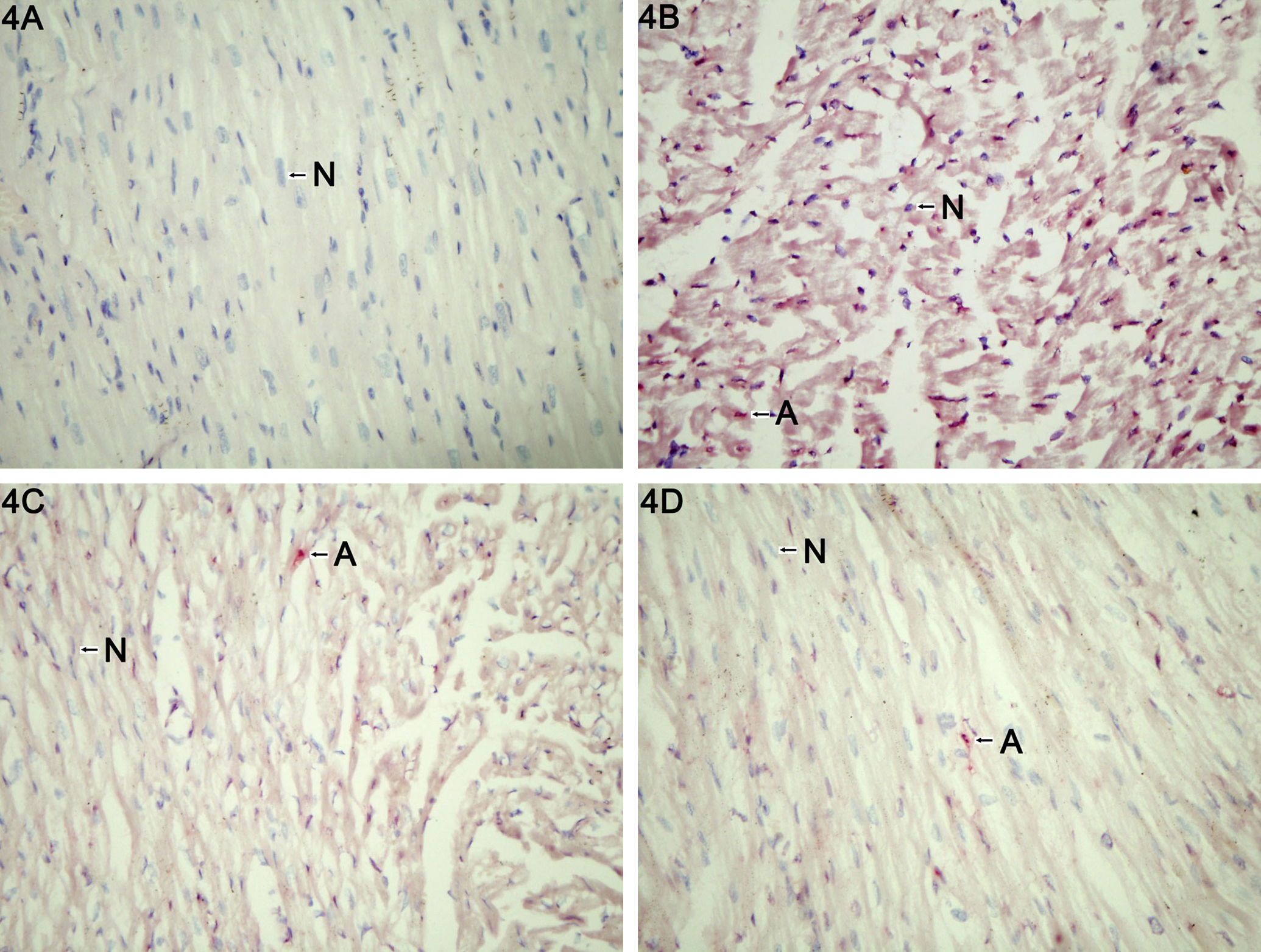
Light microscopy (×400) of terminal deoxynucleotidyl transferase (TdT)–mediated dUTP nick end labeling (TUNEL) assay for normal control (Panel A), DOX (Panel B), DOX + DEX (Panel C), and DOX + high-dose schisandrin B (Panel D) groups at week 10. A indicates apoptotic cells; N, normal cells; DOX, doxorubicin; DEX, dexrazoxane.
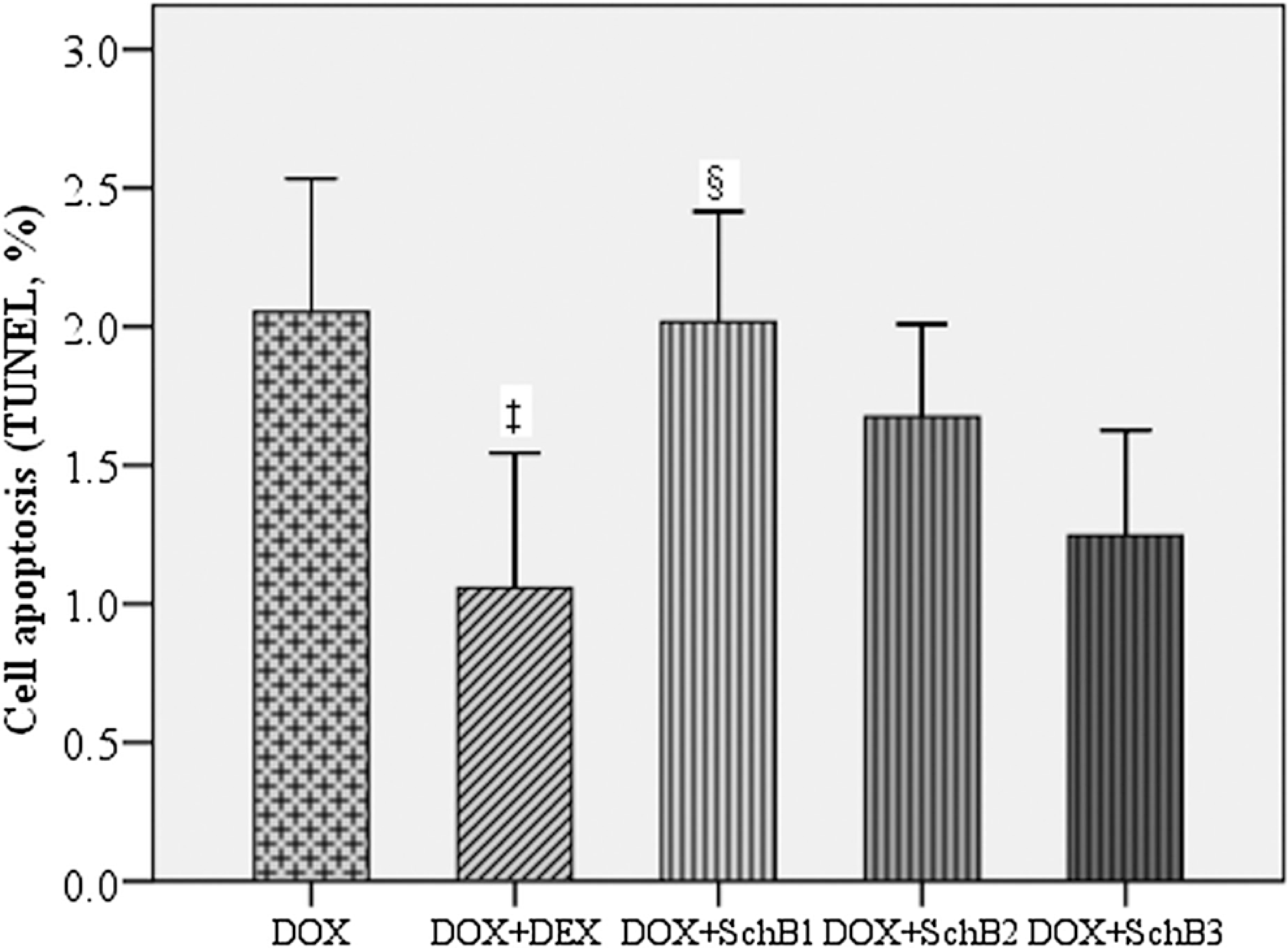
Bar chart for cell apoptosis (terminal deoxynucleotidyl transferase [TdT]–mediated dUTP nick end labeling [TUNEL]) at week 10. DOX indicates doxorubicin; DEX, dexrazoxane, SchB1, schisandrin B 5 mg/kg; SchB2, schisandrin B 10 mg/kg; SchB3, schisandrin B 15 mg/kg. ‡The DOX + DEX group showed significantly less apoptosis compared to DOX group; §The DOX + SchB1 group showed significantly more apoptosis compared to DOX + DEX group.
The Billingham score for cardiac pathology was significantly lower in both DOX + DEX and DOX + SchB2 groups than in DOX group (Figure 6 ).
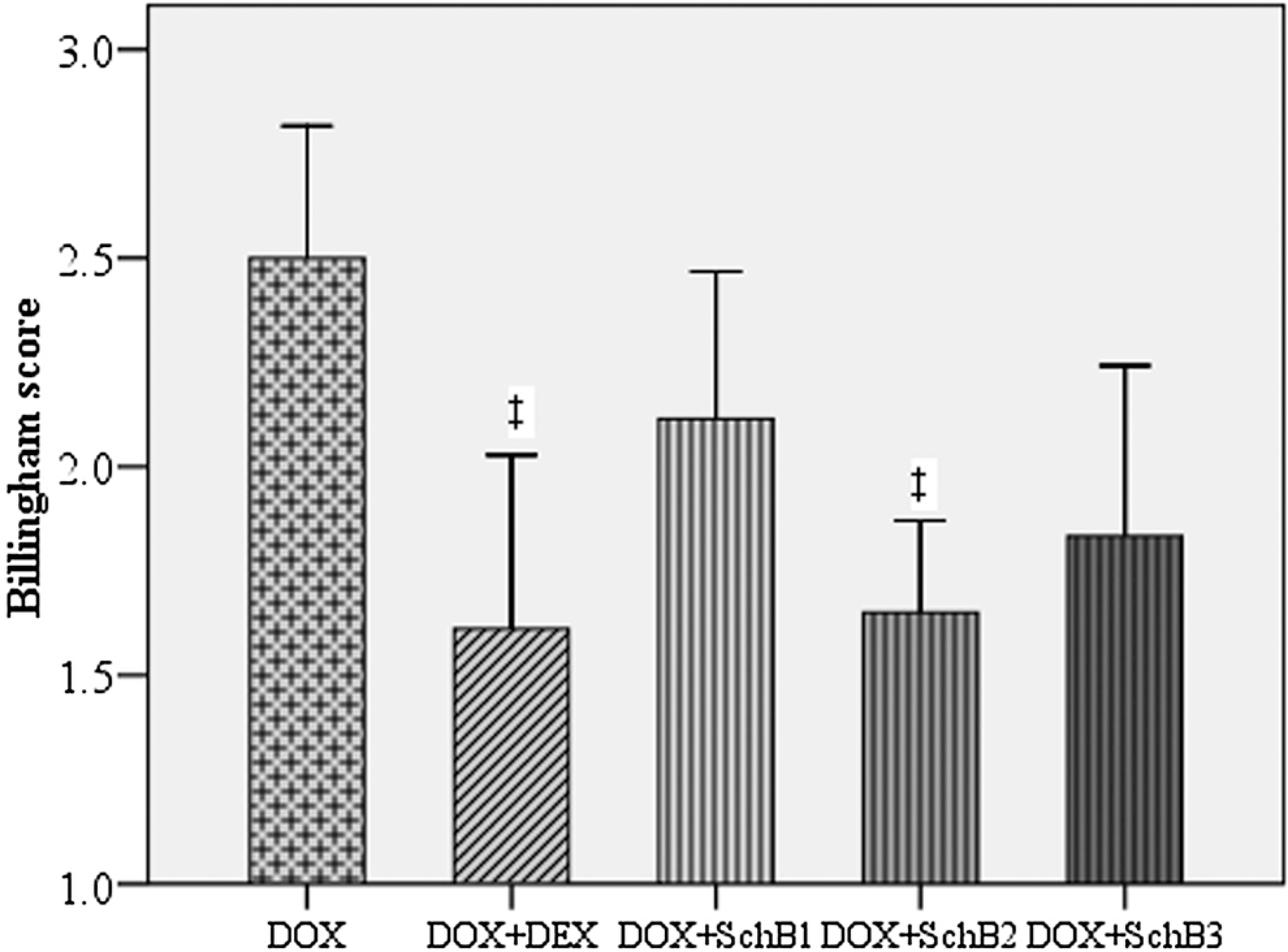
Bar chart for Billingham score at week 10. ‡The DOX + DEX and DOX + SchB2 groups showed significantly lower Billingham scores compared to DOX group; §Significant difference as compared to DOX + DEX group. DOX indicates doxorubicin; DEX, dexrazoxane; SchB1, schisandrin B 5 mg/kg; SchB2, schisandrin B 10 mg/kg.
Discussion
In the data presented in this report, SchB had dose-dependent effects in decreasing the magnitude of each DOX-mediated change in indicators of cardiomyopathy that we examined, to a degree that was approximately similar to that seen with DEX treatment. High-dose SchB was more effective than DEX in increasing the levels of the antioxidant enzyme, SOD, and in decreasing the levels of MDA, the biomarker for ROS, and was similar to DEX in decreasing apoptosis and in decreasing the serum levels of the 2 indicators of myocardial injury, cTnI and BNP. These results suggest that in the future, SchB might be a useful clinical alternative to DEX in preventing DOX-induced cardiomyopathy.
Both DEX and SchB act through different mechanisms and this might explain their slightly different effects. Doxorubicin is thought to cause cardiotoxicity by increasing free radical production by 2 mechanisms, one nonenzymatic and iron-dependent and the other enzymatic and involving the mitochondrial respiratory chain, and by decreasing levels of the antioxidant enzymes such as SOD. 7 Dexrazoxone acts through its active metabolite by chelating iron and interrupting the nonenzymatic pathway. 13 ,14 Schisandrin B increases the amount of reduced glutathione (GSH) available for defense against ROS. 9 ,12,15 Schisandrin B, therefore, acts against ROS produced by both pathways and this, perhaps, is why it was more effective than DEX in reducing the MDA levels. The somewhat greater effectiveness of high-dose SchB than DEX in improving the markers of antioxidant status, MDA and SOD, did not extend its effectiveness in improving the 3 markers of myocardial damage, BNP, cTnI, and apoptosis. DEX and high-dose SchB had similar effects with respect to these indicators.
Our results on the action of DEX are consistent with those reported by others. In previous results, DEX, when given in conjunction with anthracycline drugs such as DOX, has been shown to improve LVEF in experimental animals and reduce the myocardial pathological injury score, 10 ,16 to prevent the occurrence of DOX-induced delayed-type cardiomyopathy, and to protect against mitochondrial damage in cardiac muscle in mice. 17 In our study, we have shown DEX to improve antioxidant status and histological and biochemical signs of myocardial damage in DOX-treated animals. In addition, upon autopsy, the DOX + DEX group, unlike the DOX group, showed no obvious ventricular enlargement or pericardial effusion. Pathology scores in the DOX + DEX group were much lower than those of the DOX group, suggesting cardiac function of the DOX + DEX group was better than the DOX group, a result also consistent with previous animal experiment results. 10 ,16,17
Our results on the cardioprotective effect of SchB on DOX-induced cardiotoxicity are also consistent with the results of others. Schisandrin B administration has been reported to have a protective effect against myocardial ischemia–reperfusion injury in rats, 18 on DOX-induced myocardial injury in mice and rats, 12 and against carbon tetrachloride-caused free radical damage in mouse liver. 9 In our study, in addition to improving the biochemical markers of antioxidant status and myocardial injury, SchB improved myocardial pathology scores. Our study differed from other studies, in that other studies used oral administration of incompletely purified SchB, and we instead used pure compound and iv injection for the first time.
A weight increase in the DOX group rabbits occurred in the midstage of the experiment despite some of these rabbits having a reduced food intake and low vitality. These observations suggest that the weight gain might have been due to sodium–water retention caused by a DOX-linked deterioration in cardiac function. Rabbits in the late stage of the experiment in the DOX group had very low vitality, a further reduced food intake, slower activity, and a gradual weight loss. Early in the experiment, some rabbits in the DOX + DEX group showed decreased appetite accompanied by diarrhea. In the first 4 weeks of the experiment, some rabbits had ascites, suggesting that intraperitoneal injection of DEX had caused peritoneal inflammation. Starting from the fifth week of the experiment, when intraperitoneal DEX administration was replaced by iv injection, the condition of this group generally improved; diarrhea was significantly reduced; and vitality, appetite, and activity were all better than in the DOX group. The body weight of this group showed little change compared to predrug treatment. Some rabbits in the DOX + SchB groups had reduced appetite accompanied with diarrhea, but most rabbits in the group did not have significant changes in their vitality or their level of activity. Late in the experiment, rabbits in the DOX + SchB1 and DOX + SchB2 groups had significantly higher weights than the control group, possibly due to water–sodium retention related to decreased cardiac function.
Our results show SchB and DEX are comparable in reducing the indicators of DOX-caused oxidative stress and cardiomyopathy studied here. They differ, however, in their other effects. Dexrazoxone has the side effect of causing bone marrow suppression. 19 The SchB has the additional beneficial effect of inhibiting the transport system responsible for DOX resistance. 20 ,21 SchB is also less expensive than DEX. These considerations favor SchB over DEX. Further studies should be performed on dosage, efficacy, mechanism of action, and possible side effects to determine its clinical potential.
A limitation of the study was that the serum markers used to assess cardiotoxicity, BNP, and cTnI, are not completely specific. Another limitation was that echocardiography was probably not a sensitive enough method to detect early changes in cardiac dimensions that might have occurred.
In summary, in the study reported here, SchB showed effects similar to DEX in protecting rabbit heart against DOX-mediated cardiomyopathy and, because of its low cost, might become a useful drug in cancer treatment, especially in low-income countries.
Footnotes
Acknowledgments
We thank the assistance from Mr Shi-ping Liao, Lab of Functional Science, College of Basic and Forensic Medicine, Sichuan University.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received the financial support of application foundation grants from Science & Technology Department of Sichuan Province for the research.