
Abstract
Hydrogen sulfide is a relatively common, frequently lethal, and unique occupational hazard for which research since 1990 has uncovered many anomalies and subtleties and a previously unsuspected physiological role for the endogenous agent. The result has been uncertainty and misunderstanding, particularly for persons new to the literature. This review addresses evidence that settles past controversies, guides practical issues in evaluating human toxicity, addresses unresolved issues involving chronic exposure, and points the way to a deeper understanding of the agent and its effects.
Keywords
Hydrogen sulfide (H2S) is an important and frequently lethal occupational and environmental hazard that has a unique and consistent pattern of toxicity. Over the last decade, much more has been learned about this gas. Remarkably, hydrogen sulfide is now known to play an important physiological role in several organ systems. However, progress in understanding the toxicology of this agent has lagged in recent years, after a flurry of activity in the 1980s and 1990s led to new but incomplete insights. 1 This article revisits what is known regarding the toxicology of hydrogen sulfide, particularly as it applies to human health outcomes in occupational settings, in light of new information and reexamines the toxidrome. Reproductive, developmental, and carcinogenicity issues are not considered in this review.
The clinical picture of hydrogen sulfide toxicity remains familiar and well known. The clinical picture of acute toxicity from hydrogen sulfide has been described over and over again over the centuries, since it was first described in 1700 (and probably recognized well before). 2,3 Atypical presentations are so uncommon as to call the diagnosis into question in highly unusual cases. 4 The mechanism of hydrogen sulfide toxicity was long assumed to be analogous to cyanide but previous theories could not explain the many observed anomalies and departures from the model of cyanide toxicity. 5 –7
Hydrogen sulfide is the second most common cause of fatal gas inhalation exposures in the workplace (at 7.7%, second to carbon monoxide at 36%) and has unique features that make hydrogen sulfide cases toxicologically unusual, distinctive, and very similar from one case to another. As in most such incidents, casualties usually occur in 2s or more as would-be rescuers rush to save their coworkers and in their haste neglect to protect themselves with a self-contained breathing apparatus. Intensive training and ready availability of personal protective equipment are required to prevent such situations. 8
Attitudes toward hydrogen sulfide among occupational health professionals have swung in recent years from a sense that the toxicity was a settled issue a few years ago to a sense that we know nothing, particularly regarding chronic effects. This is not due to ignorance but, increasingly, to an overload of confusing data combined with a paucity of interpretation and integration. The accumulated knowledge on toxicology of this agent is much greater than for most toxic substances because cases are still relatively common and those outside agriculture tend to occur where other people are present, so most cases are observed.
Acute hydrogen sulfide toxicity cases are sporadic, unpredictable, and relatively uncommon in absolute terms and when compared to traumatic injuries, as are most acute toxic events in occupational settings. Clinical information must come from individual case reports, generally without informative exposure assessment and with outcome measures conducted long after the fact and without baseline preexposure benchmarks. There is always uncertainty regarding a participants' preevent condition, especially for neurobehavioral studies and pulmonary function. Often there is no mention of or effort to rule out confounding factors, such as trauma and anoxic atmospheres in confined spaces.
The exposure-response curve for lethality is extremely steep for hydrogen sulfide. 9,10 Concentration is much more important than duration of exposure. Compared to other inhaled toxic substances, hydrogen sulfide gives little margin of safety. One can visualize an encounter with concentrations of hydrogen sulfide above 500 parts per million (ppm) as hitting a wall, with the degree of damage having more to do with concentration, analogous to the speed with which one hits the wall, than with the duration of contact with the wall. Fatal exposures to hydrogen sulfide in humans, for example, in theory may take place at 150 ppm for 6 hours (concentration × time product = 0.252) or 650 ppm for 8.5 minutes (0.005). This means that, for hydrogen sulfide, higher concentrations are much more toxic, even with proportionally shorter exposure levels, for both mortality and experimental pulmonary edema induced in the rat. Table 1 provides approximate thresholds for the major effects. 9,10 Occupational exposure levels based on time-weighted averages do not take this into account. Many current models for risk assessment for hydrogen sulfide use a concentration-time constant for lethality of the general form Cn × t, where n ranges from 1.43 to more than 4.36, but the empirical evidence strongly favors the higher exponents. 10
Health Effects of Hydrogen Sulfide at Various Approximate Exposure Levels 10
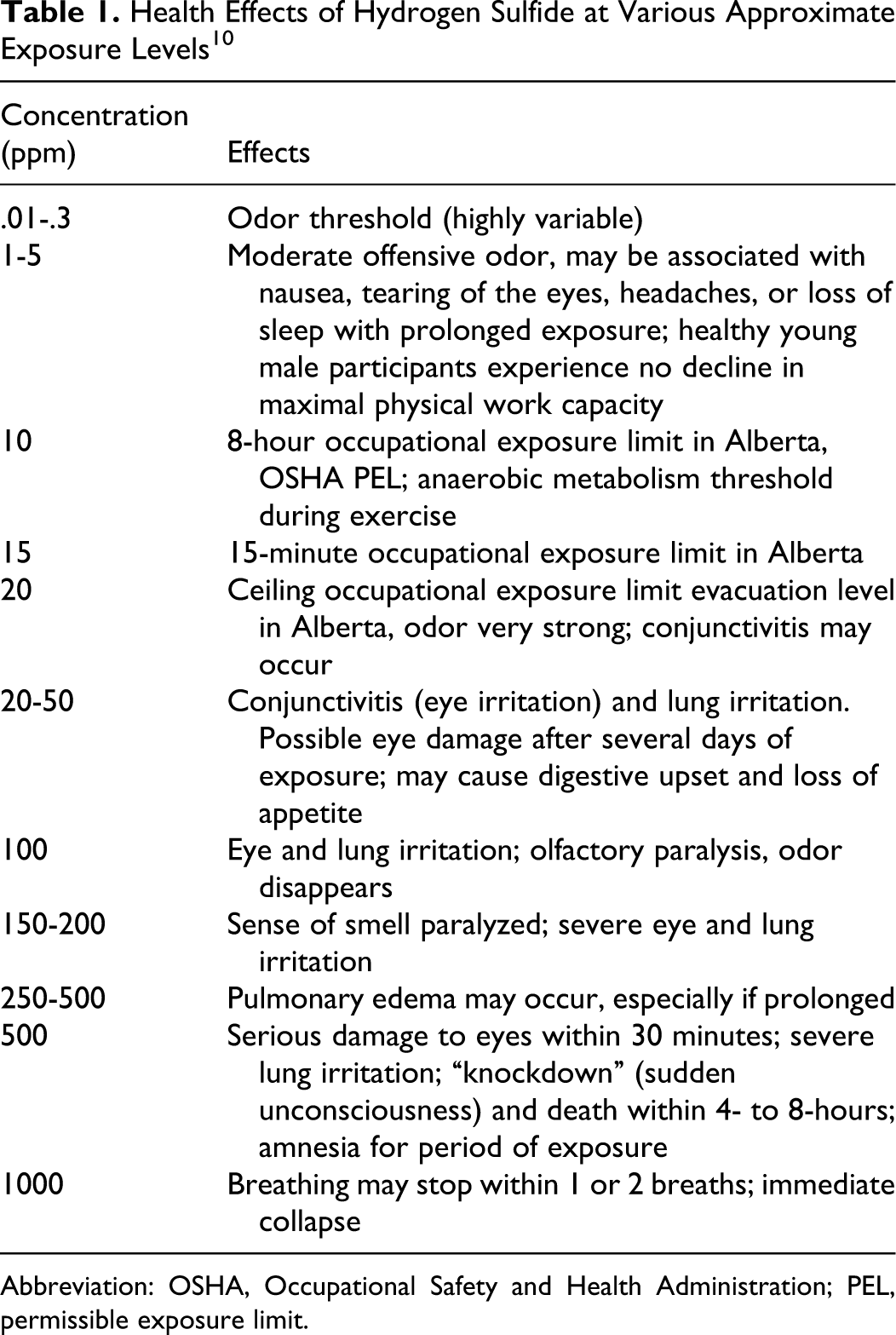
Abbreviation: OSHA, Occupational Safety and Health Administration; PEL, permissible exposure limit.
Table 2 lists current exposure standards and guidelines for hydrogen sulfide promulgated by various authorities, beginning with occupational exposure standards and progressing to community standards. These permissible exposure levels benchmark the ranges of exposure that will be discussed in this review. A graphic representation and summary of many of these same guidelines and standards has recently been published. 11
Applicable Standards and Guidelines for Hydrogen Sulfide a
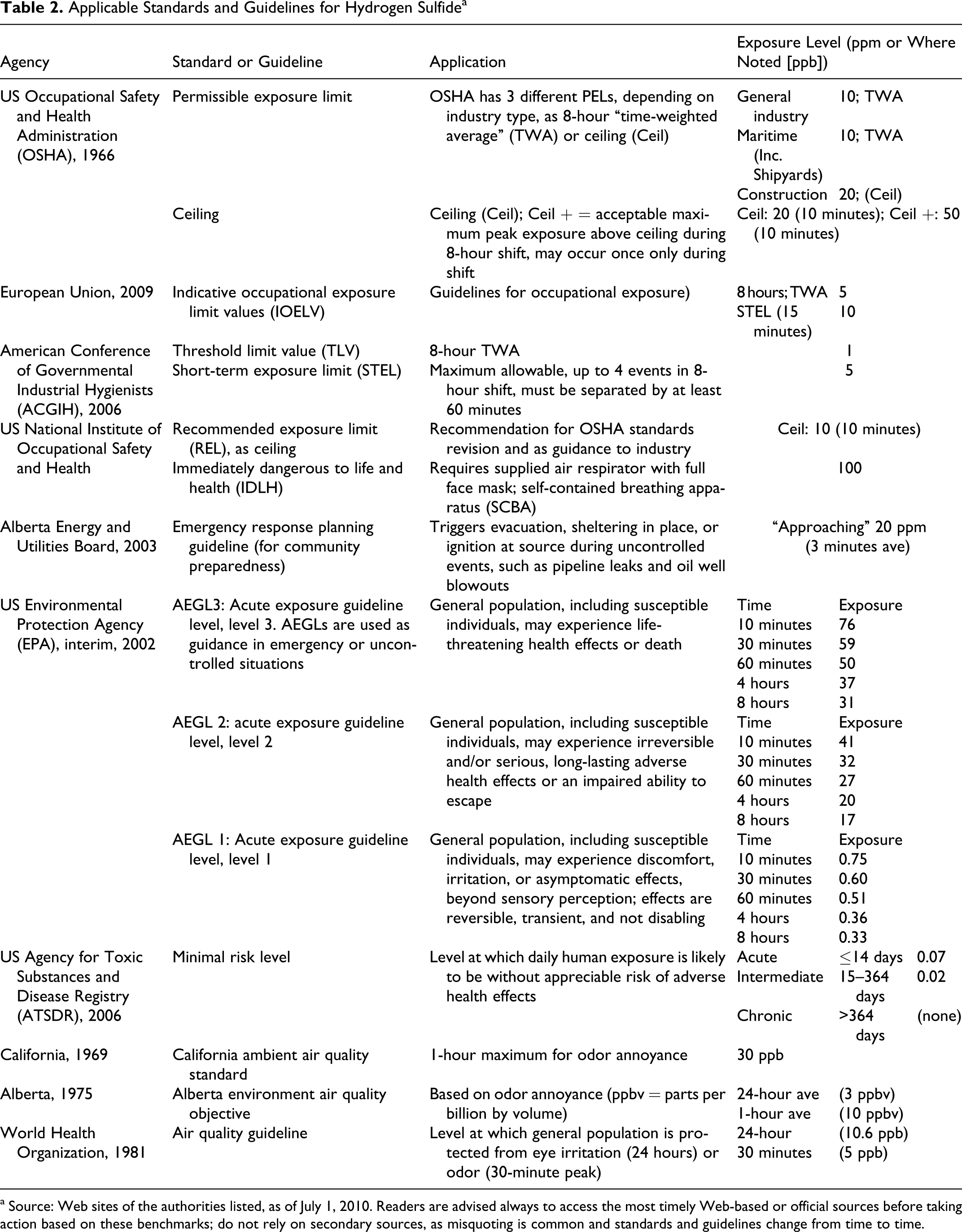
a Source: Web sites of the authorities listed, as of July 1, 2010. Readers are advised always to access the most timely Web-based or official sources before taking action based on these benchmarks; do not rely on secondary sources, as misquoting is common and standards and guidelines change from time to time.
Toxidrome
In clinical medicine, a set of characteristic symptoms and signs that occur together in a predictable or meaningful pattern is called a “syndrome.” In toxicology, a syndrome that is associated with a particular poison is called a “toxidrome.” Most toxidromes are nonspecific, such as the nausea and light headedness that follows ingestion of many new medicines, such as antibiotics, that are not particularly toxic. In contrast, hydrogen sulfide toxicity is one of the most unusual and reliable toxidromes in medical toxicology (and clinical medicine in general)
1,2,10,12
–22
: “Knockdown” (acute central neurotoxicity) Pulmonary edema Conjunctivitis Odor perception followed by olfactory paralysis
Cases of toxicity from hydrogen sulfide always show these features, singly or in combination, regardless of the susceptibility or characteristics of the victim or participant. Approximate thresholds for each cardinal effect are given in Table 1.
Most standards for the protection of occupational and community populations are based on prevention of conjunctivitis (eye irritation), knockdown, and respiratory tract irritation. 23 –25
Knockdown
Hydrogen sulfide-induced acute central toxicity leading to reversible unconsciousness is colloquially called a “knockdown.” 10 This is an abrupt loss of consciousness and collapse, often described by those who witness it as like turning off a switch. Knockdowns can be acutely fatal as a consequence of respiratory paralysis and cellular anoxia. A knockdown may easily be fatal if exposure at a high concentration (roughly 500 to 1000 ppm) is prolonged, but if exposure is transient, as it often is in an oil field due to air movement, it may also be quickly reversible. The victim typically falls down as if letting the strings loose on a marionette.
If exposure is transient, as usually happens in the oil patch, recovery may be equally rapid and apparently complete in functional terms. 18,21 Those who witness or experience recovery from a knockdown often describe it using the metaphor of someone turning a switch back on. Those who experience it and recover have sometimes said to the author that it was not an unpleasant sensation and that they woke up immediately without mental confusion. Some veteran oil-field workers have returned to what they were doing without reporting the event and without treatment, considering the experience all in a day's work.
There is now clear evidence that individuals who recover from a knockdown have a high risk of residual impairment. However, brain damage may also result from anoxia or acute traumatic brain injury, because many victims fall down. 15 The problems associated with attributing neurological impairment to hydrogen sulfide are discussed later in this review.
Pulmonary Edema and Irritant Toxicity
Hydrogen sulfide is irritating to mucous membranes, although this feature of hydrogen sulfide exposure may have been overly emphasized in the literature with respect to pulmonary edema, as discussed below. 26 This mostly affects the deep lung and the epithelium (outer lining) of the eye.
Pulmonary edema is a well-recognized acute effect of hydrogen sulfide toxicity, especially when exposure is prolonged. Hydrogen sulfide penetrates deeply into the respiratory tract because its solubility is relatively low, rendering it capable of causing alveolar injury leading to acute pulmonary edema. Older studies suggest that 20% of cases of hydrogen sulfide toxicity reaching the emergency department showed at least some evidence of pulmonary edema. 27 Compared to other toxic gases, however, death by pulmonary edema seems to be quite unusual in hydrogen sulfide toxicity, probably because at concentrations high enough to induce it the central effects would be lethal first. In 1 series of 152 cases from China, an overall mortality of only 5% was reported 14 ; mortality from toxic pulmonary edema overall is usually closer to 50%. Experimental studies have shown that hydrogen sulfide is only moderately cytotoxic for pulmonary cells and does not seem to disrupt the basement membrane of the alveolar endothelium. Thus, the ultimate prognosis for recovery and lung remodeling may be good if the patient can be supported through the acute episode. 21,22,28
Gas Eye (Irritative Conjunctivitis)
“Gas eye” is a superficial inflammation of the cornea and conjunctiva due to the irritant effect of hydrogen sulfide. 7,19,27 It is often recurrent in workers who are exposed for prolonged periods to relatively low concentrations, 20 ppm and possibly lower. 29 Some workers have said to the author that they relied on eye irritation as a second warning sign of exposure over the permissible occupational exposure limit, occurring at a lower level than loss of olfaction, which is discussed next.
A peculiar feature of conjunctivitis due to hydrogen sulfide exposure is that it can be associated with reversible chromatic distortion and visual changes. It has been suggested that the corneal epithelium develops a fine punctate stain, becomes edematous, and that small vesicles form that act as a diffraction grating. This results in a colored halo surrounding the object. This effect is sometimes accompanied by blepharospasm (acute and severe spasm of the orbicularis oculi muscle), tearing, and photophobia. 12,13,19
In Rotorua, New Zealand, where eye disorders including conjunctivitis were clearly in excess (a statistically significant doubling of risk for hospitalization), community levels averaged close to 5 ppm and may peak in places and times at 100 ppm due to geothermal activity. 30
Olfactory Effects
Hydrogen sulfide is very odorous, with a low olfactory threshold, from less than 0.01 to 0.3 ppm depending on individual sensitivity. By 1 to 5 ppm, the odor is very offensive, like rotten eggs. Thus, at lower levels, the gas has excellent warning properties. However, the gas has poor warning properties at high exposure levels because perception of the odor disappears due to olfactory paralysis. At relatively high concentrations (about 100 ppm), hydrogen sulfide paralyzes the olfactory mechanism, preventing perception of any smell. This phenomenon removes the primary warning sign of hydrogen sulfide exposure and the principal warning to, say, oil-field workers suddenly caught in a plume. 10,12,17,22,31,32
Disturbingly, this has led more than 1 oil-field worker to observe to the author that “you’re not really in trouble until you can’t smell it anymore.” Obviously, the sudden absence of an odor is not a good warning sign because it can easily be overlooked and because the disappearance of perceived smell (as opposed to a specific odor) is not absolute. Some nasal sensation may persist, mediated by other pathways, as in the perception of ammonia and solvents.
There are 2 distinct mechanisms involved in loss of olfactory acuity with exposure to hydrogen sulfide. As with most strong odors, workers may experience olfactory fatigue at lower levels of exposure and may become accustomed to them in the short term, a phenomenon known as olfactory fatigue, which is common to the sensory processing of many strong odors. There is also a mechanism specific to hydrogen sulfide known as olfactory paralysis, with which it is often confused. Olfactory fatigue is a sensory adaptation. Olfactory paralysis is a sensory manifestation of neurotoxicity. Unfortunately, they are often confused in the literature.
Olfactory paralysis due to neurotoxicity affecting both the olfactory bulb and fibers may be followed by hyposmia or anosmia, a permanent loss of the ability to perceive odor. This pattern of toxicity was demonstrated experimentally to be attributable to selective toxicity to olfactory mucosa in the nasal passages and to olfactory neuron loss after subchronic inhalation. 33,34 Hyposmia has been found to be present in most men who recovered from severe, potentially lethal hydrogen sulfide toxicity. 23
This may explain why human participants exposed to transient high levels of hydrogen sulfide have been reported to show deficits on standardized tests of smell and taste years later. 23 This is not invariable, however, because tolerance can be induced in the short term and the olfactory mucosa can recover if exposure does not persist too long. 33
Secondary Symptoms and Signs
As with all toxic conditions, there are secondary symptoms and signs of hydrogen sulfide toxicity that variably accompany or that in some cases are complications of toxicity rather than direct effects. The literature documenting the prevalence and profile of these secondary effects is much weaker than that reporting the cardinal effects, not surprisingly.
Nonspecific Symptoms and Signs
Critically, the literature does not usually distinguish among secondary symptoms that occur in exposed persons who do not experience knockdown or conjunctivitis (2 benchmark clinical symptoms that establish exposure levels) and those that do, and almost never is there an exposure assessment refined enough to establish an exposure-response relationship.
Headache and short-term cognitive changes, such as short-term memory loss, are common but very nonspecific, as they may occur in many other situations and as a response to distraction and posttraumatic stress. 35 Nevertheless, at 26% of cases, headache is probably a reliable association although not part of the characteristic toxidrome. More detailed clinical descriptions suggest that headache is a very transient phenomenon, only lasting a day or so. 36
Seizure disorders are only reported for 2% of cases, historically, but most cases are probably associated with anoxic brain damage in near-lethal cases. 15 In at least 1 case in which detailed clinical description is available, an apparently new-onset seizure occurred during a knockdown and resolved without evolving into a chronic seizure disorder. 36
Gastrointestinal symptoms (including jaundice and diarrhea) have been reported in the older literature but are not validated in more recent, systematic case series. 15 Nausea and vomiting are to be expected given the malodorous exposure, which most people find disgusting. Similar nonspecific patterns are found in many settings in which participants feel anxious, threatened, or apprehensive about poisoning. 37 In 1 case study of workers overcome by an acute, lethal release, 1 of the workers “vomited blood and collapsed” [quotation marks in the original, suggesting uncertainty], but the paper did not document the actual presence of blood in the vomitus, the absence of preexisting bleeding ulcer, and the absence of nosebleed. True hematemesis is highly unlikely, because although it is irritating, inhaled hydrogen sulfide would not have access to the stomach or esophagus or time to act in an erosive manner on the gastric mucosa in an acute situation. Furthermore, levels of endogenous and dietary sulfide are already very high in the gut and may play a protective role in the gastrointestinal tract.
Acute Respiratory Effects
Shortness of breath is to be expected for a respiratory irritant and may be a sign of the onset of pulmonary edema. However, in at least 1 case, dyspnea and cough were relieved during hyperbaric oxygen treatment following hydrogen sulfide exposure, suggesting that shortness of breath may reflect cellular hypoxia, possibly at the tissue level in the lung receptors or the carotid body, rather than deep lung injury. 38
Exposure in the short term does not appear to be associated with reduced lung function or increased airways reactivity. 39,40 However, other studies have suggested that a reduction in residual volume is a subclinical effect. 41 If so, this may be related to effects on pulmonary receptors and reflex activity rather than lung mechanics. 42,43
Chronic Respiratory Effects
It is not clear whether prolonged or repeated hydrogen sulfide exposure is associated with chronic respiratory impairment. A single case report has suggested that interstitial fibrosis followed exposure to hydrogen sulfide but this has not been reported in other cases. 44
Cross-sectional studies of sewer workers, who are exposed to hydrogen sulfide but also have other risk factors, suggest that lung function is significantly reduced after accounting for smoking and may show an accelerated rate of decline; however, the longitudinal studies required to confirm this are not available. 27
Available studies are prone to strong selection bias. One cross-sectional study that reported normal pulmonary function in a crew of oil-field workers should not be relied upon as evidence that there is no respiratory function effect attributable to hydrogen sulfide. 45 The participants were originally recruited to serve as normal controls for a study of workers in another occupation and so they were prescreened to exclude respiratory disease, removing those workers most likely to have abnormal pulmonary function. Workers who had developed significant respiratory impairment would also migrate out of the physically demanding work of drilling and oil well servicing in remote locations, leaving behind a “survivor group.” The cross-sectional study design, selection bias, and retention bias of this study would all underestimate the prevalence of reduced lung function. The article also did not include an exposure assessment. One or more of these limitations affect other papers in this literature.
It is a paradox of the hydrogen sulfide literature that exposure is not known to induce airways reactivity or the condition known as “reactive airways dysfunction syndrome” (RADS) although this might be expected based on the gas's known irritant effect. There is an intriguing possibility that this is because hydrogen sulfide appears to serve as an endogenous anti-inflammatory agent in various tissues and the gas may be exerting this effect in the lung during exposure.
Chronic Effects of Higher Sublethal Exposure
Neurotoxicity
The neurotoxicity of hydrogen sulfide is not simple. The cardinal effect of knockdown from acute, reversible toxicity occurs at lower levels than those that induce apnea and profound hypoxia, which can lead to anoxic brain injury, but the two may coexist. A central issue in studying neurotoxicity associated with hydrogen sulfide has been to differentiate between the primary effects of toxicity in the vicinity of 500 ppm, which cause the knockdown as a neurological event, and the effects of anoxia.
It is now accepted that neurological sequelae can follow knockdown in the context of acute high-level exposure. Evidence remains weak for effects associated with chronic, low-level exposure, discussed below. It would be expected that if these effects occur, they would be observed first and most consistently at higher exposures. However, in the case of hydrogen sulfide, exposures that result in knockdown may easily be confounded by head trauma during falls, which is common, 14,15,46 and hypoxemia from apnea or seizure activity. 13,14,24,47 –51 Even so, oil-field workers often go back to work after a knockdown.
Hydrogen sulfide toxicity is the result of several effects, including interference with oxygen uptake and metabolism and also hypoxia from oxygen deprivation due to apnea or respiratory insufficiency. 12 These 2 mechanisms would produce the constellation of findings identified in anoxic brain injury. There may also be other, direct mechanisms of neurotoxicity. An unknown contributing factor may be systemic or local hypotension due to the neuromodulatory effect of sulfide, a factor that is virtually unstudied.
The accumulated record of these individual cases suggests that chronic brain injury following recovery from acute hydrogen sulfide toxicity is predominantly the result of anoxic brain damage, which clearly can occur in the context of a knockdown when there is apnea or hypoxemia. 52 –54 Whether similar brain injury occurs due to toxicity alone is less clear. In the absence of apnea or hypoxemia, recovery following a knockdown of potentially lethal severity may be associated with nonspecific changes (personality changes, depression, broad reductions in cognitive ability) but apparently not the characteristic pattern observed in anoxic brain damage, which preferentially affects the basal ganglia (resulting in movement disorders), and cortical white matter. 48,51,55 It is known that at extreme concentrations, well above lethal, there is selective green-colored staining of the putamen and basal ganglia, suggesting anatomical localization. 15
In 1 case for which follow-up data are available, a young man with no premorbid history experienced a prolonged knockdown with no apparent head injury and demonstrated a normal head computerized tomography (CT) scan but experienced profound deficits after recovery. 48,50 The history is given that “There is no indication that the patient had stopped breathing at any time” but it is not clear how this is known because his rescuers themselves were overcome. He developed extrapyramidal signs and impaired movement accuracy but no seizure disorder. A PET scan performed after the event showed abnormal uptake in the basal ganglia. A cerebral perfusion SPECT (single-photon emission computed tomography) scan performed three and one-half years after the incident showed diminished oxygen uptake in the putamen but no anatomic lesion visible in the basal ganglia on magnetic resonance imaging (MRI). A similar case from Korea, however, showed abnormal MRI findings in the basal ganglia and motor cortex, despite a higher Glasgow Coma Scale score on presentation. 54
Neurobehavioral studies have focused on sensory defects and subtle changes in individuals who were probably not hypoxic, at least for prolonged period. 1 Occupational exposure to hydrogen sulfide in 4 workers did result in loss of consciousness during a release; however, these workers had persistent neuropsychiatric complaints associated with abnormal evoked response potentials (assessing cortical function) and subclinical neuropsychiatric clinical findings without overt disease. The participants had cardinal symptoms (eye irritation), confirming that that exposure had occurred, possibly repeatedly, at levels that must have exceeded 50 ppm; at times, exposures may have reached 243 ppm, as noted in other incidents at this refinery. The pattern of symptoms and impairment was not uniform among participants. However, these same participants also had evidence of posttraumatic stress disorder, which can influence neurobehavioral testing, and were not representative of the exposed population, having been selected precisely because they demonstrated abnormalities. 56 Thus, selection bias must be considered in interpreting these findings.
The Medical Diagnostic Review, a population-based prevalence survey and clinical screening conducted in southern Alberta in the mid-1980s, found no evidence of a excess in prevalence of neurological signs and findings, both soft and hard, in populations living downwind of sour gas facilities. 57
Insights From Animal Studies
The available animal evidence points to injury to the cerebral cortex, cerebellum, and possibly the brainstem and spinal cord at concentrations approaching those that humans might encounter. The lesions are similar to those seen in oxygen deficiency and in poisoning by other cytochrome oxidase inhibitors. 48,58 Thus, a cyanide-like effect does occur, but it is not clear that it is the main mechanism for acute neurotoxicity.
Anoxic brain injury characteristically affects parts of the brain with high metabolic activity, particularly the basal ganglia, causing extrapyramidal movement disorders such as chorea or athetosis and, in milder cases, a disorder resembling Parkinson disease. Extrapyramidal symptoms resembling Parkinson diseases may appear during the recovery from a prolonged hydrogen sulfide-induced coma, and in that situation probably represent secondary anoxia rather than toxicity. 27,48,59 Severe cases of hydrogen sulfide have been associated with cortical necrosis. 60 The anoxia can be aggravated by ischemia due to hypotension, which may be focal because of the vasorelaxation effect of hydrosulfide, but it is not known whether exogenous hydrosulfide from hydrogen sulfide inhalation modifies the effects of local endogenous hydrosulfide as a vasoregulatory mechanism.
Could a toxic effect of hydrogen sulfide induce cellular anoxic brain injury or an effect mimicking it at lower sublethal concentrations? Early demyelination has been observed in experimental studies of exposures in rat brain at 30 ppm, repeated for 1 hour per day for a month, not enough to cause an anoxic effect. 61 Cumulative cytochrome oxidase inhibition has also been observed in mice following repeated exposure to hydrogen sulfide (100 ppm for 2 hours on 4 consecutive days), with secondary and adaptive changes. 62
Experimental neurobehavioral studies in rats show effects on motor activity and water maze performance at 80 ppm but not at 30 ppm or below, and no effect was observed on regional brain catecholamine levels. 63 Rats exposed to 125 ppm show a pattern of impaired performance on the water maze that is better explained by slowed overall performance and greater susceptibility to distraction than by impaired memory or cognition. 64
There is emerging evidence that endogenous hydrogen sulfide modulates the immune response in the central nervous system and that its role is anti-inflammatory. 65 What this means for toxicity from exogenous hydrogen sulfide is not clear, but it is conceivable that suppression of inflammation could actually be a mitigating factor for chronic central nervous system toxicity.
Peripheral Neuropathy
Peripheral neuropathy is not often or consistently reported in cases of hydrogen sulfide toxicity but some well-documented cases have featured a tingling paresthesia that does not appear to be associated with chronic neuropathy. 66 The finding does not necessarily imply selective neurotoxicity because a paresthesia of this type could also be central or mediated by vascular changes.
At much lower levels of exposure, but certainly elevated compared to most communities, is the city of Rotorua, in New Zealand, a cultural center for the Maori people where there are also many sulfur springs and geothermal sources. Ecological studies of residents of Rotorua suggest some excess morbidity in both the central and peripheral nervous system disorders, 30 but the pattern suggests that the association is not causal. The association is strongest for mononeuritis, which would not appear to be a plausible outcome for hydrogen sulfide.
Paresthesias and mononeuritis are also cardinal symptoms of carbon disulfide toxicity, although that agent acts by different mechanisms. It is possible that there could be confounded exposures in some cases or that there are similarities in some effects between hydrogen sulfide and carbon disulfide. This seems unlikely but cannot be ruled out at this time.
Chronic Effects of Lower-Level Exposure (<10 ppm)
Exposures on the order of 5 to 10 ppm are sometimes encountered in community settings, although they are more common as background in workplaces such as oil refineries. Levels above 1 ppm are very uncommon in the community, where concentrations above the odor threshold (generally above 0.05 ppm for most people) are normally unacceptable and prosecuted as a nuisance. It has been alleged that health effects may be observed at exposures <1 ppm, but the evidence is weak.
General
At 10 ppm, hydrogen sulfide exposure appears to induce an earlier transition from aerobic to anaerobic metabolism in resting and exercising adults, consistent with partial inhibition of aerobic metabolism, but this is not associated with subjective symptoms or clinically evident effects. 39,67 By comparison, exposure at 5 ppm resulted in an increase in uptake, using similar methods. 68,69
In Rotorua, there was an elevated risk of cardiovascular disease observed but a lower risk for stroke and evidence for an elevated prevalence of high blood pressure, which is inconsistent, unless somehow reflecting the agent’s physiological mechanisms. The study did not take into account a variety of potential confounders, including mercury (which was not measured) and other sulfides (not reported). 30 Ecological studies of this type are an intrinsically weak study design for etiological investigation and should not be considered strong evidence of causation. Hospital admissions for respiratory illness in children only, but not adults, has been shown to be associated with the ambient level of hydrogen sulfide the previous day at levels <100 ppb, using a cutoff for dichotomizing high and low exposure that was close to the odor threshold in a community highly sensitized to issues involving hydrogen sulfide toxicity. 70 Although this could be evidence of a triggering effect on childhood asthma, it could also be evidence for a bias on the part of parents in response to their children’s symptoms, driven by odor perception.
Odor
Because of its very-low odor threshold, hydrogen sulfide provokes complicated psychological and physiological responses associated with perception of noxious stimuli. 1 The odor and irritation associated with hydrogen sulfide cannot be masked, making it impossible to blind challenge studies, and these factors are likely to be the explanation for an observed increase in symptoms of anxiety at 5 ppm, which is noxious. 71 The sense of smell (and bitter taste) evolved in human beings in large part as protection against toxic or spoiled food. A foul odor, therefore, is perceived as a threat or signal of danger that induces a defensive response. The odor of hydrogen sulfide at that level is perceived by most people as disgusting and may therefore provoke both aversion and physiological responses (nausea and increase in vagal tone), which directly affect health status and comfort at the moment. Odor may also be a false warning sign, triggering maladaptive anxiety, when the odor threshold is well below the threshold for toxicity and this is not consciously understood by the participant, who may perceive a health threat where one may not exist or may experience subliminal feelings of discomfort. 72 These effects may be difficult to separate from toxic effects and complicate the evaluation of effects on communities. 70
Neurological Effects
Well-designed experimental studies have not shown evidence of neurotoxic sensory or cognitive effects associated with acute exposure to hydrogen sulfide at 5 ppm and below, notwithstanding the apparent physiological shift to anaerobic metabolism at 10 ppm. 39,67 –69 This, again, suggests that the mechanisms are not the same.
Sewer workers have been a popular group to study for evidence of neurological impairment due to hydrogen sulfide at levels near 10 ppm. Egyptian sewer workers in Cairo exposed to levels estimated to be near 10 ppm were found to have evidence of “cognitive impairment” compared to a control group, for which no description was provided. However, the symptom profile reported was very nonspecific (headache, memory deficits, and lack of concentration) and commonly seen as secondary effects of psychological factors (stress, job dissatisfaction, sleep disorder, low socioeconomic status, or education). As may be imagined, sewer workers in a city such as Cairo are likely to have low socioeconomic status and other issues that confound standardized psychometric tests. More persuasive was the difference in P300 latency, suggesting slowing of cognitive function. 73
The most difficult studies to interpret come from one investigator. 25,49,74,75 They require evaluation as a group and close attention because of issues regarding quality assurance and testing methodology, some of which were revealed at a major conference in 2000 1 and in legal proceedings since then. 76 The intellectual problem with this body of work is that despite questions with respect to validity, it cannot be summarily dismissed. Findings of neurobehavioral impairment that suggest impairment in highly exposed workers who had been rendered unconscious are plausible. 74 However, findings of similar or more severe impairment at much lower concentrations in the context of prolonged, community exposure have not been reproduced when the same population was studied by other experienced investigators. 70,77
A precedent for this situation occurred in the 1980s when studies conducted by one principal investigator, a research cardiologist, on carbon monoxide and its cardiovascular effects were suspected of major deficiencies. The US Environmental Protection Agency funded studies to replicate the key experiments and in so doing clarified and corrected the record. 78 A similar action may be helpful in this case.
Insights From Studies of Mechanism
The physiological role of hydrogen sulfide, as opposed to its toxicological role, is only now emerging. 79,80 Perturbation in this physiological role is likely to have consequences in both exacerbating and limiting injury. Hydrogen sulfide is a vasorelaxing agent, immune modulator, and may also be a neuromodulator. Toxic exposure that interferes with these functions may involve direct effects on the nervous system, perhaps mediating cell toxicity in stroke 80 as well as in other organ systems (for example, possibly contributing to inflammation in the pancreas but suppressing it in the stomach and bowel). The state of “suspended animation” induced during knockdown is showing promise as a therapeutic intervention, because in some experimental situations it is protective against mortality. For these reasons, hydrogen sulfide is being evaluated for therapeutic use. 79 –86
Hydrogen sulfide disassociates in blood to hydrosulfide (HS−), which is delivered to tissues by the circulation and raises sulfide levels in tissue, but effectively only during exposure. The residence time of hydrogen sulfide in tissue is very short and hydrosulfide is quickly cleared, so the effects of exogenous hydrogen sulfide in the form of blood hydrosulfide are brief. It is now known that the endogenous level of sulfide in the human brain is relatively high, so the flux may not be detectable. It is likely that the addition of a transient sulfide load could push the level past a threshold of narcosis or anesthesia but must do so very abruptly and reversibly. 87
One lethal endpoint of hydrogen sulfide exposure, and the usual experimental endpoint in rats, is respiratory paralysis, a dose-dependent reduction in ventilatory drive resulting in apnea, which follows an initial reflex hyperpnea. 58,88 Infusion of the hydro sulfide ion alone into the circulation mimics the systemic effects of hydrogen sulfide inhalation. The apneic response to hydrogen sulfide in rats is not enhanced by intrarterial injection of sulfide into the carotid artery, which delivers blood directly to the brain, compared to intravenous injection into the femoral artery, in which mixing occurs in the general circulation and the concentration delivered to the brain is correspondingly lower. The apneic response can also be blocked by paralysis of the vagal nerve by lidocaine or by infusion of sodium bicarbonate solution, in the absence of acidosis. These findings strongly suggest that a peripheral receptor in the lung is responsible for the apneic response. 42
Because hydrosulfide binds to cytochrome c, it has always been assumed to act in the same way as cyanide, causing anoxia at the cellular level. 7,17,28 It probably does, at high exposure levels, and there may be enough of inhibition at lower levels to serve as a histological biomarker. 89 However, this cannot be the only significant mechanism and may not even be the predominant toxic effect. 90 Cytochrome oxidase is not upregulated, as would be expected, following repeated high but nonlethal exposure to hydrogen sulfide in rats despite many other changes in gene expression. 91 As noted earlier, there is no consistent pattern of anoxic brain injury following knockdown, as there is with coma equivalents following cyanide and carbon monoxide.
There are clearly other mechanisms of toxicity that are likely to be at least as important. 42,86 The anoxic aspect of hydrogen sulfide toxicity, developed on analogy with hydrogen cyanide, does not explain the full range of effects of the agent nor its unique and stereotypical toxidrome. Measurable brain levels of sulfide may or may not change appreciably following inhalation of hydrogen sulfide (even as high as 400 ppm in the rat, which is equivalent to a much higher concentration in humans), as reports disagree 88,89 and concentrations in other tissues increase only transiently. 89 Even so, electroencephalographic changes are detectable even at lower concentrations (25 ppm) in the rat and persist for weeks. 92 In addition, peripheral reflex mechanisms may play an important role in the intact animal and in the observed clinical syndrome. 42,81
Hydrogen sulfide does poison cytochrome activity at high concentrations and so it is classified as a cellular asphyxiant, together with carbon monoxide, cyanide, and azide. The effect of hydrogen sulfide in disrupting cytochrome c oxidase activity is the same at a mitochondrial level as oxygen deprivation or asphyxiation except that it may act more quickly. This was long thought to be the primary mechanism of action of characteristic reversible neurotoxicity, the “knockdown”. 10 However, this explanation does not make sense because the resulting cellular anoxia (inability to use oxygen) would be devastating to the brain, quickly irreversible (because energy utilization by the cell would be blocked), and if the victim recovered would consistently result in anoxic brain damage of the type seen following recovery from severe carbon monoxide toxicity or the rare occasions of recovery from acute cyanide toxicity.
Hydrogen sulfide clearly can poison cytochrome c in vitro at physiologically relevant concentrations and can inhibit aerobic metabolism even at relatively low levels. In studies designed to explore the use of hydrogen sulfide in inducing suspended animation on a mouse model, conducted at 80 ppm (comparable to much higher levels in humans), the gas was found to be a rapidly reversible inhibitor of heart rate, cardiac output, core body temperature, and respiratory rate while preserving stroke volume and blood pressure. 93 In healthy, fit human volunteers, hydrogen sulfide exposure as low as 5 ppm during exercise (30 minutes) is associated with an early shift from aerobic to anaerobic metabolism, as indicated by increasing blood lactate levels, but without symptoms. 69 This observation precipitated a review of occupational exposure levels in the United Kingdom. 26
Until recently, there was no suggestion that hydrogen sulfide might play a role in gastrointestinal physiology. However, as the physiological role of hydrogen sulfide is elucidated, it has been demonstrated to play a role in maintaining the integrity of the gastrointestinal mucosa, inhibiting motility, and suppressing inflammation. 84,94,95 This is leading to new avenues for therapeutics, in much the same way that knowledge of the surprising physiological roles of nitric acid has and that of carbon monoxide will do.
In the past, there was a controversy over whether sulfhemoglobin occurs following high-level hydrogen sulfide exposure, but the weight of evidence is that it does not. 79,96
Treatment
Treatment of transient exposures, and of knockdowns in which the worker has regained consciousness, is not specific, hinges on rapid removal from exposure, and is currently unsatisfactory. 5,96,97 Overwhelming exposures and prolonged knockdowns may require aggressive treatment, but the circumstances in which these exposures occur often lead to delays in transport and treatment. There is a modest literature on antidotes, which is largely experimental or anecdotal except for nitrite administration. 5,98,99 Human experience is acquired one case at a time, because hydrogen sulfide toxicity cases, like most occupational toxicity situations, are infrequent and therefore difficult to prepare for and to study by protocol. 17,52,99 –106
Hyperbaric oxygen therapy is an attractive and logical option for treating hydrogen sulfide intoxication and anecdotal evidence suggests that it may be effective. 102 The use of oxygen is probably related to the oxygenation of marginally anoxic tissues and the displacement of sulfide from binding sites on cytochrome c oxidase, but this has not been worked out. A series of 3 treatments at 2.5 atmospheres for 90 minutes each has been recommended. 103 Hyperbaric oxygen treatment is safe in skilled hands but transport to a facility should not delay supportive care, which is a more important factor in survival. 48,107 –109
Nitrite treatment is based on the theory that methemoglobin generated by nitrite would displace the sulfide, as it does cyanide, and regenerate the active cytochrome oxidase. 99 Although methemoglobin is more effective in binding sulfide than oxyhemoglobin, the complex between sulfide and methemoglobin does not last long enough to make a difference. Sulfide disappears quickly from the circulation under conditions of good oxygenation anyway. The evidence suggests that nitrite can only be effective within the first few minutes following exposure and may actually slow sulfide removal thereafter. There are also reasons to believe that the methemoglobin hypothesis is insufficient to explain the action of nitrite even in the first few minutes. A further practical problem with this approach is that it may add to the anoxic burden that already may exist from the cytochrome poisoning, respiratory paralysis due to central toxicity, and ventilation-perfusion mismatch associated with pulmonary edema. It may also induce hypotension and further complicate the anoxia with hypoperfusion. Increased oxygen tension may overcome some of the physiological disadvantages of nitrite treatment.
Other pharmacological treatments have been proposed but efficacy has not been demonstrated. 5 Thiosulfite has been used as an antidote, on the presumption that treatment clears free sulfide, but the therapeutic rationale has been questioned and the treatment has been abandoned. 5,6 Pretreatment with several agents has been associated with increased survival in animal models, including pyruvate, 110 dithiothreitol, 111 and α-ketocarboxylic acids. 112 These have not shown therapeutic efficacy and will not be discussed further here.
There is a potentially promising lead involving 2 readily available agents, bicarbonate and glucose. 113 Almeida investigated the toxicity of dimethyl sulfide (Me2S), a less potent and more easily handled analogue of hydrosulfide, in Sprague Dawley rats. The incidence and duration of coma (the rat equivalent of knockdown) induced by this agent over a range of dose was determined and with this model the efficacy of purported antidotes for H2S was determined. Using a standard dose of dimethyl sulfide that reliably induced the coma effect, 3 agents proposed to protect against lethality from hydrogen sulfide, nitrite, pyruvate, and dithiothreitol, were found to have no significant effect in shortening duration of coma and preventing lethality, whether given at onset of coma or as pretreatment. Bicarbonate, however, reduced duration of coma by about 28% but did not affect lethality. Bicarbonate and glucose administered together, however, reduced coma duration 37% and mortality 50% if given at onset and the effect was even greater when given as a pretreatment, reducing coma duration by 80% and preventing mortality altogether. Sulfide toxicity in the central nervous system may therefore be associated in some way with the metabolism of glucose. Perhaps cellular hypoglycemia and carbonic anhydrase activity play a role in the pathophysiology of sulfide toxicity, although earlier studies have suggested a hyperglycemic response, 116 perhaps due to stress and catecholamine release.
These observations demonstrate that a treatment protocol for both knockdown and to prevent death from H2S may ultimately be possible, although the feasibility of administering bicarbonate and glucose in prehospital, field situations remains to be determined.
Conclusion
The secondary literature on hydrogen sulfide often contains and perpetuates various errors and sometimes describes the individual symptoms and signs of hydrogen sulfide out of context or inaccurately. For example, 1 popular, respected, and otherwise invaluable reference book (Goldfrank’s) speaks of “olfactory fatigue” (a general phenomenon of adjustment to intense odor, usually incomplete) rather than the more characteristic and serious effect of “olfactory paralysis” (an effect of direct neurotoxicity that nullifies the most important chemical warning signal to exposed persons). 115 This is a critically important distinction. The same reference also wrongly states that “Patients typically lose consciousness at the time of exposure from loss of central respiratory drive.” If knockdowns were caused by loss of respiratory drive, they would be fatal much more often. Loss of consciousness is a direct neurotoxic effect, although apnea may supervene later. These misstatements blur important distinctions.
Another common error, seen in the literature on chronic toxicity, is to suggest that short-term exposure to high concentrations may equate to longer-term exposure to lower concentrations. 75 This idea is particularly misleading for hydrogen sulfide because, as noted, toxicity for this agent is mostly driven by concentration.
Perhaps the most common error is overgeneralization or failure to appreciate that for hydrogen sulfide, as for most toxic agents, characteristic symptoms and signs occur in a pattern, not in isolation or arbitrarily. It is the toxidrome that matters, not the individual symptom or sign.
Footnotes
The author(s) declared a potential conflict of interest: Guidotti is a frequent consultant on related issues in the oil and gas industry and an expert in legal cases involving hydrogen sulfide. This review was prepared to address recurring questions arising from this work. Guidotti is not engaged in any current case involving parties named in this review and this review was not prepared for use in a legal action.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Development of this paper was internally supported by Medical Advisory Services, Rockville, Maryland, as background for a symposium on hydrogen sulfide at the Air and Waste Management Association annual meeting in Calgary, 2010.