
Abstract
Although the tobacco plant has been employed as a medicinal and sacred herb by Indigenous cultures across the Americas, its usage drastically changed after the 15th-century colonial arrival; its large-scale commodification and global marketing once brought to Europe lead to hedonic and addictive uses harmful to health. As a consequence, tobacco smoking is now one of the largest public health problems worldwide. However, in the Peruvian Amazon, a region of origin of tobacco species, Indigenous healers still know how to use the plant for therapeutic purposes. Due to a general disregard of Indigenous knowledge and stigma, these uses have however not so far been clinically investigated. We hence conducted for the first time a clinical field study assessing a sample of patients treated by a traditional healer specialized in tobacco in the Peruvian Amazon (observational design, pilot study, N = 27). The study was conducted within a transdisciplinary and multi-epistemic medical frame, in close partnership with an Amazonian healer. We used validated self-report scales to quantitatively assess mental health variables before and after the weeklong treatment, and mixed-methods to report experienced effects. Paired-samples t-tests comparing pre- and post-treatment scores revealed significant reductions in anxiety, depression, perceived stress, and general symptom indicators. Experienced effects included initial physical discomfort, followed by psychologically or existentially/spiritually significant insights. Our findings point to a sophisticated therapeutic approach based on Indigenous knowledge of tobacco applications, which should be further investigated. The study also contributes to the burgeoning scientific field on therapeutic uses of contentious psychoactive plants.
Although the tobacco plant (Nicotiana spp.) has been used as a sacred and medicinal herb by Indigenous cultures across the Americas (Dixon, 1921; Echeverría & Niemeyer, 2013; Russell & Rahman, 2015; Tushingham et al., 2018), its manner of usage drastically changed once it was brought to Europe, after the colonial arrival in the late 15th century (Nater, 2006; Oyuela-Caycedo & Kawa, 2015); in spite of initial interest in the plant’s medicinal properties also in Europe, tobacco’s subsequent large-scale commodification and global spread lead to recreational uses, later propagated by a growing transnational industry (Charlton, 2004; O’Keefe & Pollay, 1996; Proctor, 2004; Russell & Rahman, 2015), which developed tobacco products designed to increase consumption and, thus, economic profitability. As a consequence, harmful tobacco uses associated with addiction and health risks (non-communicable diseases) prevail today, representing one of the major global public health problems, with one billion smokers worldwide (Gowing et al., 2015; Martin-Soelch, 2013; Reitsma et al., 2021; World Health Organization, 2017). The most recent chapter of these developments is the transnational tobacco industry’s attempt to respond to new legal frames and trends in global tobacco management by now marketing nicotine products (e.g., e-cigarettes) made to appear to the consumer as quasi-pharmaceutical harm reduction devices, but in the absence of scientific evidence for such claims (Hendlin et al., 2017).
In some Indigenous-American cultures, however, especially in the Peruvian Amazon (the phytogeographic birthplace of N. rustica; Oyuela-Caycedo & Kawa, 2015), uses of tobacco as medicinal herb continue to exist (Berlowitz, García Torres, et al., 2020; Wilbert, 1993). The plant is highly esteemed in this region, described as “Master Plant” and main curing tool of traditional healers (Barbira-Freedman, 2015; Russell & Rahman, 2015); so fundamental is the plant to Indigenous Amazonian medicine that in various local languages the generic term for “traditional healer” is etymologically linked to tobacco, for instance in the language of the Ashaninka or Matsigenga, where “healer” (seripiari/seripigari) literally means “the one intoxicated by tobacco” (Russell & Rahman, 2015; Shepard, 1998), or for the Yuracaré, for whom the word for “healer” (korrë-n-chata) translates as “he who eats tobacco” (Thomas et al., 2011).
In spite of these descriptions, perhaps due to a widespread general disregard of Indigenous knowledge and associated stigma, Indigenous tobacco-based treatments have remained scientifically underexplored. This is the case in spite of the ongoing “psychedelic renaissance,” an exponentially growing scientific interest in psychedelics/psychoactives formerly considered harmful (e.g., psilocybin, cannabis, or ayahuasca), as potential therapeutics (e.g., for depression or PTSD), some of which now labeled “breakthrough therapies” by the FDA (Butler et al., 2020; Carhart-Harris et al., 2021; Chi & Gold, 2020; dos Santos & Hallak, 2021; Fisher et al., 2021; Kyzar et al., 2017; Luoma et al., 2020; Nichols, 2020; Nichols et al., 2017; Reiff et al., 2020; Siegel et al., 2021; Vermetten & Yehuda, 2020). However, although the same rational would apply also for tobacco, this psychoactive plant has thus far not been studied in the psychedelic renaissance. Furthermore, even though psychoactives like psilocybin or ayahuasca stem from Indigenous Latin America healing systems (Dillehay et al., 2010; Duke et al., 2021; El-Seedi et al., 2005; Gerber et al., 2021; Luna, 2011; Miller et al., 2019; Robinson et al., 2020; Zimmermann et al., 2021), corresponding practices, epistemologies, and local traditional healers are rarely included in current clinical research.
We have formerly reported findings from a qualitative ethnographic study employing a multi-epistemic pluri-medical approach in transdisciplinary collaboration with a Peruvian-Amazonian Maestro Tabaquero (traditional healer specialized in tobacco treatments; Valadeau et al., 2010), where we reported treatment concepts and associated epistemologies in conjunction with Amazonian tobacco uses including indications, contraindications, effects, risks, and safety profile, with a particular focus on the mental health domain for which a liquid preparation for oral ingestion was used (Berlowitz, García Torres, et al., 2020). The current observational field study aimed to assess patient outcomes and experiences in conjunction with this application. More specifically, using an observational pilot study design, we aimed to assess changes on mental health variables via validated self-report scales before and after a weeklong treatment delivered by a traditional-Amazonian Tabaquero, as well as report patient experiences of acute/subacute effects of tobacco-based ritual.
Method
Design
The research was approved by the responsible ethics committees (Peru: PRISMA Comité Institucional de Ética en Investigación, CE0724.20; Switzerland: University of Fribourg, 88-A1), conducted in accordance with the Declaration of Helsinki and international/national regulations. Given the “novelty” of the treatment from a scientific perspective, we used a pilot study approach with a naturalistic/observational field design (Leon et al., 2011). We assessed changes on 6 primary outcomes and 12 exploratory variables (see Measures section) by means of validated symptom scales and questionnaires before and after treatment (pre- and post-test, respectively), and subjective effects by means of a mixed-method assessment after the intervention. In keeping with the Amazonian emic understanding of the importance of the traditional manner of application, the study assessed the treatment as a whole (pharmacological and extra-pharmacological factors), also in line with general traditional medicines research guidelines (World Health Organization, 2000).
Treatment Setting
Data collection took place in the Peruvian Amazon (Loreto province, rural Maynas) at the practice of a traditional Amazonian Tabaquero, who collaborated in this study as part of a transdisciplinary research project that explored traditional Amazonian medicinal applications of the tobacco plant. Born in the Río Tigre area (Loreto Province, Peru), he had been raised by his maternal grandparents, who, themselves traditional healers and farmers, from an early age instructed him in traditional medicine. At age 12 he started specializing as a tabaquero and began to regularly attend to patients at age 15 while continuing his training. Over his adult years, he progressively attained the reputation of an accomplished Maestro Tabaquero. At the time of the study he possessed about 36 years of clinical experience (age ~51), treating local as well as international patients at his practice in the scope of one-time consultations, individual retreat-like treatments, or group work (for further descriptions of his practice and professional background see Berlowitz, García Torres, et al., 2020). The treatment in the current study consisted of daily tobacco ingestion administered by the Tabaquero in traditional ritual (ceremonial or retreat setting): In the ceremonial setting, the Tabaquero conducted daily ceremonies in a group context; participants would gather in the ceremonial space (maloca) before midday. The Tabaquero would open the ceremony using traditional ritual methods to serve each participant one or a few small sips of the remedy (dosage being determined based on clinical observations per patient and day). He used a standard tobacco remedy for all, but for some patients additionally reporting physical complaints in the initial diagnostic conversation he added a corresponding (tailored) plant, subsequently referred to as “tailored” tobacco remedy (for medicinal plant surveys of the region see e.g., Jovel et al., 1996; Sanz-Biset & Cañigueral, 2011; Sanz-Biset et al., 2009). Patients were encouraged to drink water after having taken the remedy (generally followed by emesis) and were subsequently asked to shower. At different stages of the ceremony the healer employed traditional Amazonian techniques like icaros (healing chants), shacapa (leaf rattle), or soplar (blowing tobacco smoke), toward the end also including brief individual curings. After about 3 hr, the ceremony was closed and participants instructed to rest. During the treatment week, patients were required to follow a strict dietary regime and refrain from sexual contact (for further descriptions on Peruvian-Amazonian dietary practices see Berlowitz et al., 2021). Similar restrictions with the addition of social seclusion applied also in the retreat setting, locally referred to as dieta (Spanish for “diet”): The patient would stay in a forest hut without contact with other people, except for the staff that would bring food twice a day and the Tabaquero to serve the tobacco remedy. He would offer instructions like in the ceremonial setting, but then would leave the patient to himself/herself to concentrate on their inner process. We have previously provided a detailed description of a tobacco-based dieta using a case report with ecological momentary assessment (Berlowitz et al., 2023). Upon treatment completion the Tabaquero checked in with all patients and let them know he remained available should they wish to consult him by phone but does not implement follow-up sessions per default.
Measures
We used the Symptom Assessment-45 (SA-45; Davison et al., 1997; Maruish et al., 1998; Sandín et al., 2008) to assess psychological symptoms in nine different domains: Anxiety, Depression, Obsessive–Compulsive, Phobic Anxiety, Hostility, Interpersonal Sensitivity (feelings of discomfort in relation to others), Paranoid Ideation, Somatization, and Psychoticism. To obtain domain scores, the corresponding five items were summed (0—not at all, 5—extremely; scale scores range from 0 to 20); a Global Severity Index that assesses overall psychiatric symptomatology was obtained by summing all 45 items. In the current work, we used the latter as one of six primary outcome measures. We further used the Hospital Anxiety and Depression Scale (HADS; Quintana et al., 2003; Zigmond & Snaith, 1983) to assess these variables especially central to public health (Santomauro et al., 2021; Vos et al., 2020). Items (range 0–3) were summed to obtain anxiety (seven items; range 0–21), depression (seven items; range 0–21), and overall emotional distress scores (14 items; range 0–42), serving as primary outcomes. The Patient Health Questionnaire-15 (PHQ-15; Cano-García et al., 2020; Kroenke et al., 2002) was used to assess self-reported somatic symptoms. All 15 items (rated 0–not bothered to 2–bothered a lot) were summed to form an overall somatic severity score (range 0–30) used as a primary outcome. Finally, we assessed psychological stress as primary outcome using the Perceived Stress Scale-10 (PSS-10; S. Cohen et al., 1983; Remor, 2006), items rated from 0—never to 4—very often (overall 0–40). For all primary outcomes, higher numbers indicated higher symptom severity. We additionally assessed the following exploratory variables: Positive And Negative Affect Scale (PANAS; Lopez-Gomez et al., 2015; Watson et al., 1988), each subscale (PA/NA) comprising 10 items ranging between 10 and 50 (items rated 1—very slightly or not at all to 5—extremely); the Five Facet Mindfulness Questionnaire (FFMQ; Baer et al., 2006; Cebolla et al., 2012) to assess cognitive tendencies related to mindful awareness. We used overarching mindfulness made of the sum of all items (rated 1—never or very rarely true to 5—very often or always true) corresponding to facets Describing, Acting with awareness, Nonjudging of inner experience, Nonreactivity, without items related to Observing as per authors (Baer et al., 2006, 2008). Finally, the Hallucinogen Rating Scale (HRS V.3.06; Bouso et al., 2016; Strassman et al., 1994) was used to assess experienced acute/subacute effects of the tobacco-based ritual. The HRS includes qualitative as well as quantitative items (0—not at all to 4—extremely), the latter computed into six effect clusters by averaging corresponding items (range: 0–4): Intensity (perceived intensity of experience), Somaesthesia (perceived somatic effects including visceral, tactile, and interoceptive aspects), Affect (alterations in emotions), Perception (alterations in sensory perception), Cognition (changes in process and content of thoughts), and Volition (capacity for willful actions).
Participants and Procedure
All participants were thoroughly informed about the study and signed an informed consent. Participation was voluntary and involved no monetary reimbursement. Included were all spontaneous treatment-seekers during the study period (May-July and October-December 2021) to whom the Tabaquero prescribed a tobacco-based treatment. Exclusion criteria included age below 18 and lack of either Spanish or English language skills. Due to confinement measures and travel restrictions linked to the Covid-19 pandemic, the number of spontaneous treatment-seekers was greatly reduced during the study period. A total of 28 treatment-seekers were approached to participate in the study; none were excluded based on age or language and none refused participation. One participant left the study site shortly after enrolling and thus was excluded (they explained they needed to travel to an activity elsewhere). The total sample hence consisted of N = 27 participants. Twenty-one were treated in group or personal ceremony and six in retreat setting (dieta). All participants filled in the PHQ-15, SA-45, HADS, PANAS, PSS, and FFMQ before initiating their treatment (pre-test) and again upon treatment completion (post-test, 1 to 3 days after treatment), taking overall 45 to 60 minutes to complete. The HRS was administered at post-test and participants were encouraged to elaborate on qualitative descriptions. Participants were recruited for the study in the context of their own treatment (naturalistic study design, observational), thus timepoints of treatment initiation varied between participants. During the study, the researcher remained available for questions from participants regarding the study in case necessary but did not act as intermediary in the liaison between healer and patients.
Data Analysis
All quantitative data were analyzed using SPSS Statistics for Windows (Version 27.0, released 2020, Armonk, NY: IBM Corp). Descriptive statistics were used to calculate sample characteristics and clinical cut-offs were used if available to estimate the proportion of clinical-level scores in the sample. For the comparison of health-related variables before and after treatment we compared the six primary outcome’s means (SA-45 general psychiatric symptom severity, PHQ-15 general somatic symptom severity, HADS emotional distress, HADS anxiety, HADS depression, PSS-10 overall stress) and additionally performed exploratory comparisons on the nine SA-45 psychiatric symptom domains, PANAS (PA/NA), and mindfulness (FFMQ). We thus conducted a total of 18 comparisons (i.e., 6 primary outcomes + 12 exploratory). A Bonferroni (BF)-adjusted alpha was used to account for multiple comparisons (i.e., significance level at p < .05/18 = .0028, two-tailed), thereby taking a relatively conservative approach for exploratory analyses. However, in view of the known methodological limitations of BF adjustment (Perneger, 1998), we also report results against the more lenient uncorrected significance level at p < .05. We first conducted Kolmogorov-Smirnov tests to know if the pre-/post-test difference scores and HRS clusters were normally distributed. Variables with normal distributions included the PHQ-15, D(26) = .13, p = .20; PANAS-PA, D(26) = .08, p = .20; PANAS-NA, D(26) = .14, p=.18; HADS-Depression D(27) = .16, p = .06; PSS-10 D(27) = .15, p=.15; SA-45 Global severity index D(27) = .15, p = .13; SA-45 Anxiety D(27) = .15, p = .10; SA-45 Depression D(27) = .13, p=.20; SA-45 Interpersonal sensitivity D(27) = .16, p = .07; SA-45 Somatization D(27) = .10, p = .20; FFMQ-overall mindfulness D(26) = .12, p = .20; HRS-Intensity D(26) = .16, p = .07; HRS-Somaesthesia D(26) = .10, p = .20; HRS-Affect D(26) = .10, p = .20; HRS-Perception D(26) = .12, p = .20; and HRS-Cognition D(26) = .08, p = .20. Conversely, non-normally distributed variables included HADS Emotional Distress, D(27) = .18, p<.05; HADS-Anxiety: D(27) = .17, p<.05; SA-45 Obsessive–Compulsive D(27) = .21, p<.01; SA-45 Phobic Anxiety D(27) = .26, p<.001; SA Hostility D(27) = .23, p<.01; SA-45 Paranoid Ideation D(27) = .23, p<.01; SA-45 Psychoticism D(27) = .27, p<.001; and HRS-Volition D(26) = .21, p<.01. We used paired-sample t tests to test if there were significant changes on outcomes and exploratory measures from pre- to post-test, and the Wilcoxon signed-rank test for non-normal variables. We calculated Cohen’s d as effect size measure for significant differences in the t tests and used r for the non-parametric Wilcoxon tests. Benchmarks for interpreting Cohen’s d are: ≥.8 as large, .5 as medium, and .2 as small effect; benchmarks for r are: ≥.5 as large, .3 medium, and .1 as small effect size (J. Cohen, 1988; Fritz et al., 2012). As a control subgroup analysis we tested if participants that received a tailored tobacco remedy (n = 14) differed on any of the variables (including HRS composites) from those that received standard tobacco remedy (n = 13). For this we used independent samples t-tests, and Wilcoxon rank-sum test in case of non-normal variables. Since we found no significant differences for any of the measures (see Supplemental Material for means and t test results), the distinction was not adopted in subsequent analyses and the two subgroups were pooled for all statistical analyses.
Finally, to analyze the HRS data we used descriptive statistics for quantitative items and summarized the qualitative responses along principles of qualitative content analysis (Mayring, 2008). For the latter, we used the six HRS clusters (Intensity, Somaesthesia, Affect, Perception, Cognition, Volition) as overarching themes in a similar manner as was done by Strassman and colleagues (1994) in their seminal work. The use of the HRS in the current study was intended to provide a first cognitive map for the nature of experienced effects of traditional tobacco ingestion, for which descriptions along single items were most useful. The quantitative HRS item scores reflect intensity (0—not at all to 4—extremely), but in order to additionally report the portion of the sample that did versus did not experience a given phenomenon (i.e., prevalence), we also reported percentages, subsuming the five-point Likert scale into a binary (yes/no) scale for better readability. In the absence of reference scores for the overarching clusters, cluster scores are less meaningful but for the sake of completeness, we nonetheless provide them along with Cronbach’s alpha.
Results
Sample Characteristics
Table 1 shows demographic and clinical characteristics of participants (N = 27). The mean age was 48.9 years (SD = 11.1, range 31–70 years), 15 were women. Most participants were European (85%) and the rest from the United States. The latter filled in the questionnaires in English, except for one all others preferred Spanish. Self-reported professions included schoolteacher, cook, baker, veterinary, engineer, nurse, medical doctor, psychologist, Pilates/Yoga instructor, osteopath, and so on. The baseline scores on the SA-45 general psychiatric severity index (Davison et al., 1997) pointed to psychological symptoms that for 18.5% were suggestive of psychiatric diagnosis (cut-off score at one SD above mean). The most common somatic complaints on the PHQ-15 were musculoskeletal (back/limbs/joints pain), gastrointestinal (constipation/ diarrhea), or feeling tired/low in energy but according to benchmarks by Kroenke et al. (2002) severity was low/minimal for most participants, medium for 34.6%, and severe for only 3.8%. Based on the HADS cut-off score (Bjelland et al., 2002; Zigmond & Snaith, 1983) about a quarter exhibited clinical-scale depressive symptoms, and anxiety symptoms were at clinical level for nearly half. Treatment motives were predominantly psychological, including a “lack of interest in life,” “depression,” “anxiety,” “negative thoughts and fears,” “I feel emotionally drained,” “I want to heal my fear, my guilt, and my lack of confidence,” “little care and respect for myself,” “lack of objectives in life,” “self-confidence,” “difficult family relationships,” wanting “emotional stability,” “to find serenity,” “I don’t know who I am,” or “personal growth.” Some participants also mentioned somatic complaints as secondary motives (musculoskeletal, digestive, gynecological) or reported a chronic condition (Parkinson’s disease, multiple sclerosis, irritable bowel).
Demographics and Clinical Features of the Sample at Baseline.
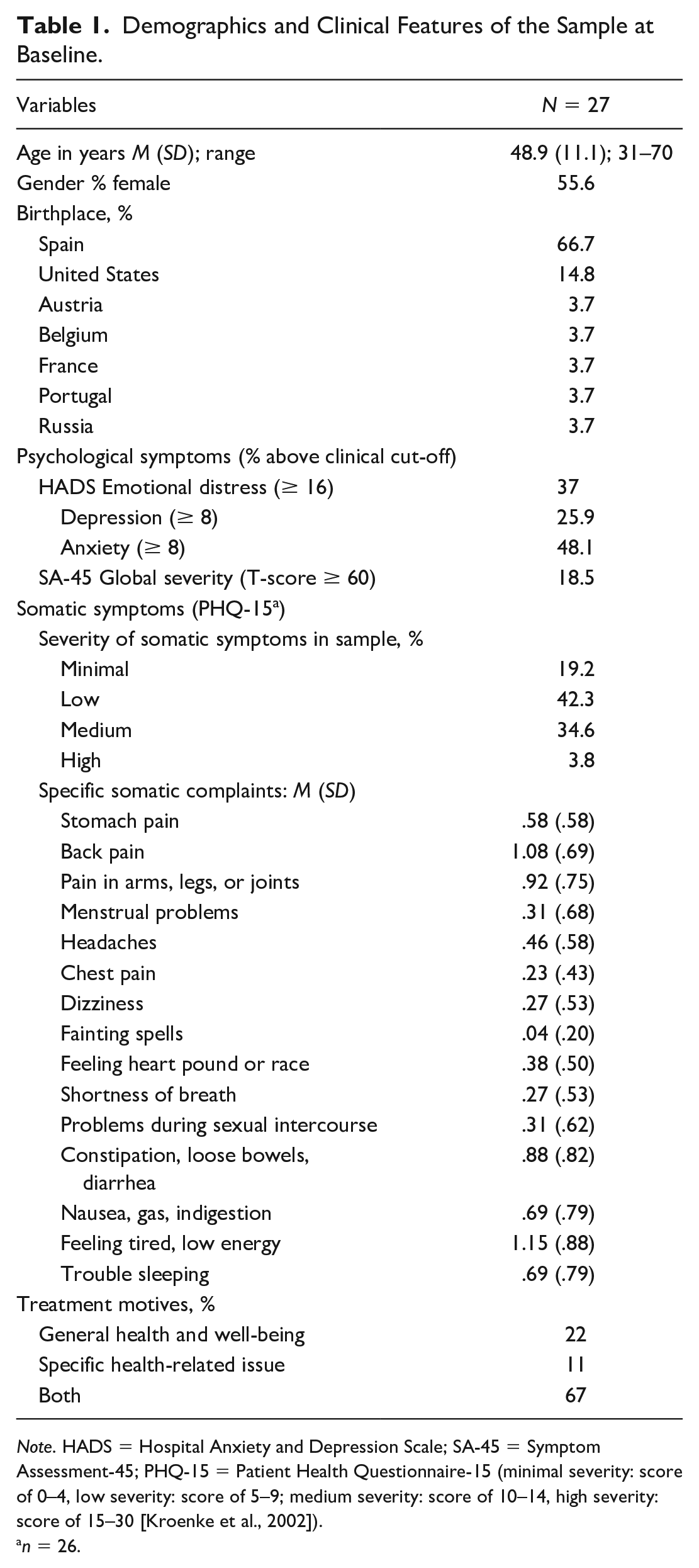
Note. HADS = Hospital Anxiety and Depression Scale; SA-45 = Symptom Assessment-45; PHQ-15 = Patient Health Questionnaire-15 (minimal severity: score of 0–4, low severity: score of 5–9; medium severity: score of 10–14, high severity: score of 15–30 [Kroenke et al., 2002]).
n = 26.
Subjective Experiences as per HRS
A descriptive account of subjective experiences in conjunction with the Amazonian tobacco-based therapy are given in Table 2, with HRS clusters as main themes (Intensity, Somaesthesia, Affect, Perception, Cognition, Volition); mean cluster scores and Cronbach’s alpha are reported in the right columns.
HRS per-Item Percentages, Means, and Qualitative Descriptions Organized by HRS-Clusters.
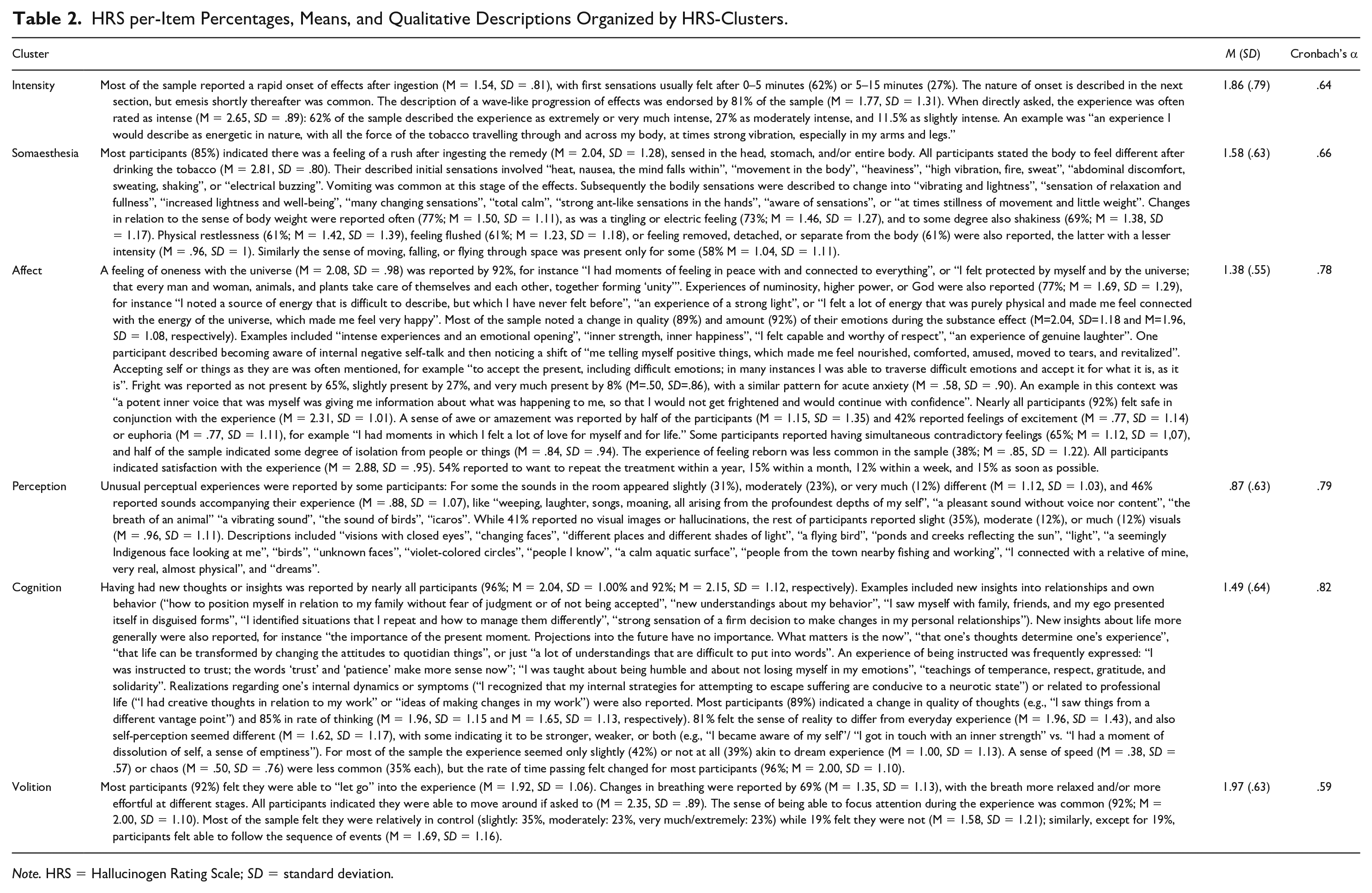
Note. HRS = Hallucinogen Rating Scale; SD = standard deviation.
Pre- and Post-Test Comparisons on Primary Outcomes and Exploratory Variables
Table 3 shows means and standard deviations for all health-related variables and pre-/post-test comparisons. All primary outcomes showed significant improvement post treatment at BF-corrected alpha of p < .0028: There was a highly significant post-treatment drop of general psychiatric symptoms (SA-45 global severity index; p < .00001, d = 1.08). The HADS anxiety and depression indices both significantly decreased (HADS-Anxiety p < .0001, r = −.59; HADS-Depression p < .001, d = .76), as did overall emotional distress (p < .0001, r = −.58). Perceived stress in the sample (PSS-10) was significantly lower at post-treatment (p < .0001, d = 1.73) and overall somatic symptoms (PHQ-15) also improved significantly (p < .0001, d = .95). Of the exploratory comparisons, improvements on seven SA-45 symptom domains were significant improved after treatment at corrected alpha (Anxiety: p < .0001, d = 1.00; Depression: p < .001, d = .77; Obsessive–Compulsive: p < .001, r = −.46; Hostility: p < .001, r = −.52; Interpersonal Sensitivity: p < .0001, d = .90; Paranoid Ideation: p < .001, r = −.50; Somatization: p < .001, d = .78). Psychoticism improved only without BF adjustment (p < .05, r = −.33), and Phobic Anxiety showed no significant change. Of the PANAS scales, NA was significantly lower post treatment compared to baseline at BF-corrected significance (p < .001, d = 1.58); PA was higher after treatment only at uncorrected alpha (p < .05, d = −.45). Finally, overall mindfulness (FFMQ) was significantly higher after treatment compared to baseline at BF-adjusted alpha (p < .0001, d = −.96). Figure 1 summarizes the changes on the primary outcomes and exploratory variables.
Comparing Primary Outcomes and Exploratory Variables Before and After Treatment (N = 27).
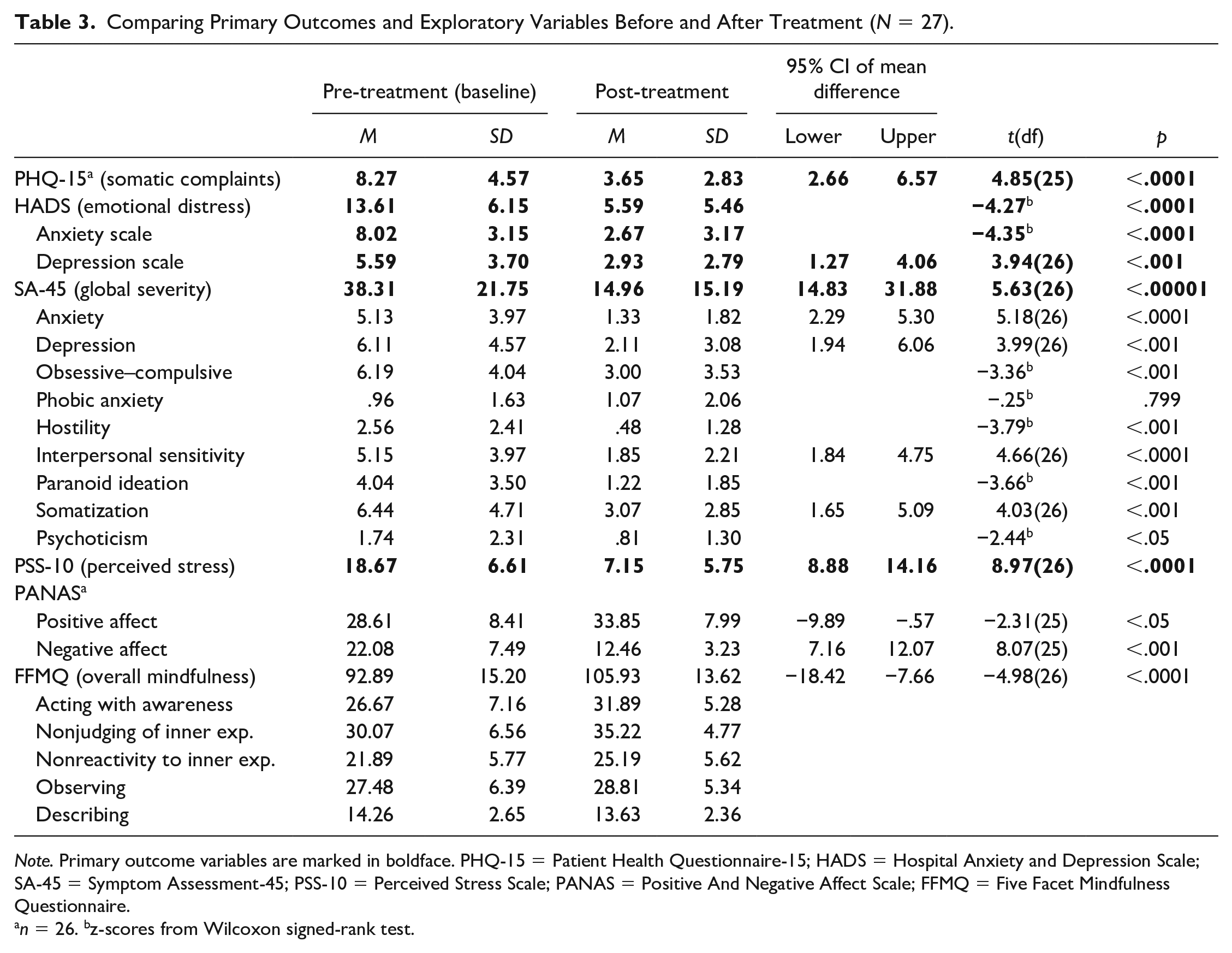
Note. Primary outcome variables are marked in boldface. PHQ-15 = Patient Health Questionnaire-15; HADS = Hospital Anxiety and Depression Scale; SA-45 = Symptom Assessment-45; PSS-10 = Perceived Stress Scale; PANAS = Positive And Negative Affect Scale; FFMQ = Five Facet Mindfulness Questionnaire.
n = 26. bz-scores from Wilcoxon signed-rank test.
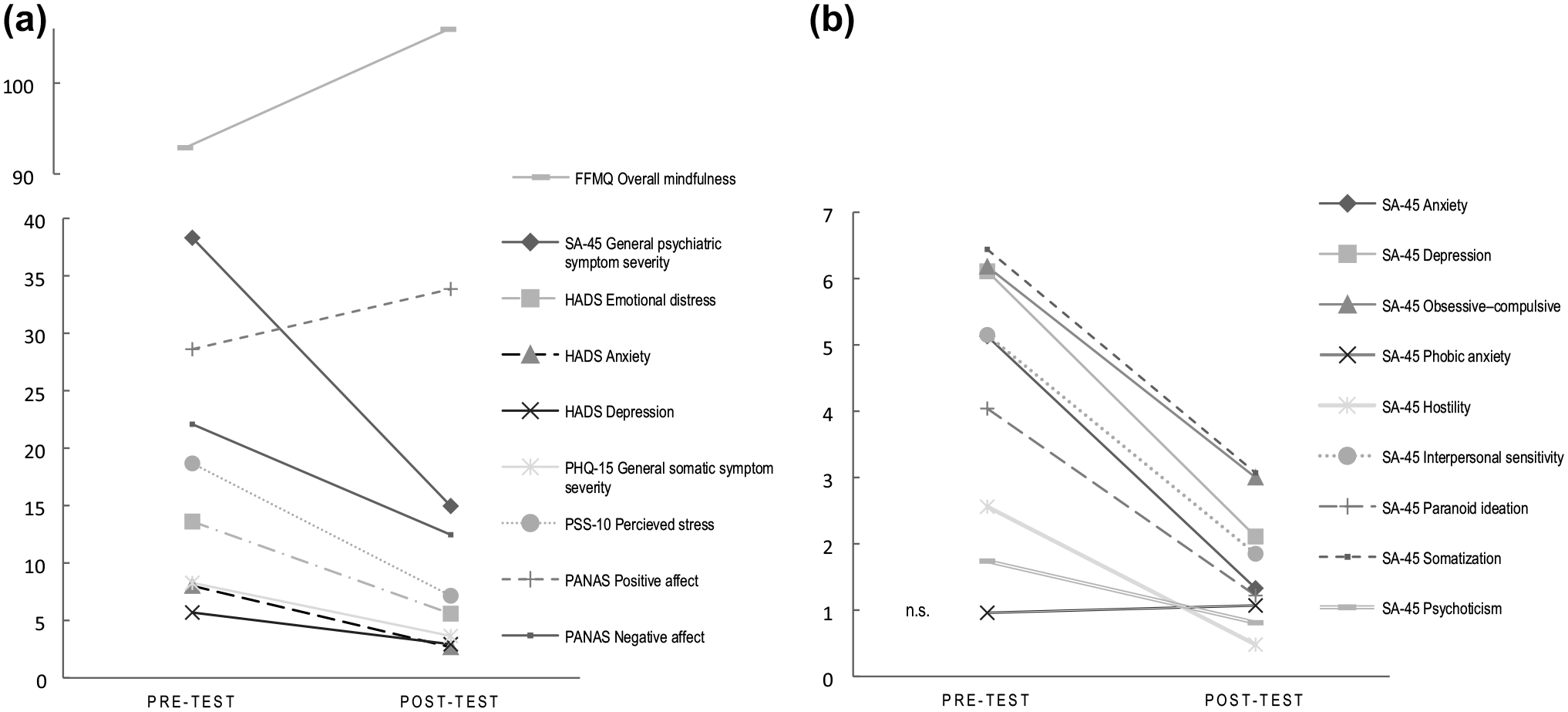
Pre-/Post-Treatment Differences on Primary Outcomes and Exploratory Scales.
Discussion
The current observational study for the first time statistically assessed outcomes of a traditional-Amazonian treatment involving tobacco as medicine. The study took place in the Peruvian Amazon at the practice of a specialized traditional healer (Tabaquero). The sample was international, to be understood against the backdrop of the psychedelic renaissance (global interest in therapeutic uses of psychoactives) and associated rise in treatment-seeking (or “shamanic tourism”) to the Peruvian Amazon (Berlowitz, Walt, et al., 2020; Fotiou, 2020b). The sample showed a range of mental health symptoms at baseline. Comparison of pre- and post-treatment symptom scores revealed statistically significant improvements in all primary outcomes (general psychiatric symptoms, depression, anxiety, perceived stress, general somatic complaints) and several exploratory variables (obsessive–compulsive symptoms, somatization, interpersonal sensitivity, hostility, and paranoid ideation) but controlled studies with larger samples will be needed to confirm these findings. With reference to possible mechanisms, the results on the PANAS could suggest a decrease in NA more pronounced to the beneficial outcomes than increase in PA, but additional data would be needed to test this. It would however be consistent with the Amazonian epistemological understanding of tobacco as cleansing, especially via its emetic effect, expelling negative thoughts and feelings related to energy-/spirit-related toxicities; tobacco-induced emesis in the Amazonian medicine view is considered an important therapeutic mechanism rather than an undesirable side-effect, which is also the case for instance for ayahuasca (Berlowitz, García Torres, et al., 2020; Fotiou & Gearin, 2019; Sanz-Biset & Cañigueral, 2013; Shepard, 1998). Similarly, the increase in mindfulness (FFMQ) is in line with the Tabaquero’s description of the plant as “clearing and centering the mind” (Berlowitz, García Torres, et al., 2020). From a pharmacological perspective, cognitive-enhancing effects could be associated with nicotine (Valentine & Sofuoglu, 2018); however, the polypharmacology of the plant’s ingestion and role of other tobacco constituents remains to be established (Berlowitz et al., 2022). Although often classified as stimulant/depressant based on nicotine (Benowitz et al., 2009; Levin et al., 1998; Picciotto et al., 2002; Valentine & Sofuoglu, 2018), some authors suggested it as hallucinogen based on Indigenous or “shamanic” tobacco uses involving visions and trance states, possibly linked to ß-carboline alkaloids also contained in tobacco (Elferink, 1983; Janiger & de Rios, 1973, 1976; Wilbert, 1993). Synergistic effects with ß-carbolines (e.g., harmine) are known to play a role in the psychopharmacology of ayahuasca for instance (dos Santos & Hallak, 2017; Farzin & Mansouri, 2006; Ferraz et al., 2019; Morales-García et al., 2017; Riba et al., 2003), and indeed the current participants’ reported effects suggest pharmacological action beyond mere stimulation. Descriptions included an onset involving physical discomfort and emesis, followed by enhanced affective states and novel insights (psychological, existential). From the emic Amazonian understanding, such novel insights are linked to the concept of tobacco as a “master” or “teacher plant” (Callicott, 2013; Dev, 2018; Jauregui et al., 2011; Luna, 1984): If applied according to the traditional methods (e.g., dieta), such plants are said to offer the person instruction and novel understandings, the plant understood as a conscious “other-than-human person,” with whom a respectful relationship is developed (Luna, 1984; Viveiros de Castro, 1998).
The current work has several limitations, among them the observational design, modest sample size, and lack of control group which limit the generalizability of findings. This is however normal for pilot studies, and future research should include a larger sample and control conditions such as waitlist or standard treatment comparison groups, with follow-up assessments after 3, 6, and 12 months to know if beneficial changes persist over time. This study employed a naturalistic approach to evaluate outcomes of the integral Amazonian intervention, including its traditional ritual elements and context. While this is a superior design in terms of epistemic/cultural fairness (Celidwen et al., 2023; Schenberg & Gerber, 2022) as it respects the treatment in its original epistemic context and form, as well as in view of ecological validity for it assesses the intervention in its natural occurrence (World Health Organization, 2000), it also implied that treatment parameters were determined based on clinical requirements and thus not uniform. Although all the remedies were based on tobacco, for some patients, a tailored remedy was prescribed, and the Tabaquero requested the recipe to remain confidential to protect intellectual property. However, since there were no statistical differences between participants who received standard versus tailored tobacco remedy on any of the test variables, their psychoactive effects were likely very similar. Nonetheless, it is important to stress that our results should not be understood as a function of tobacco alone, but of an integral traditional treatment consisting of a variety of pharmacological and extra-pharmacological factors, in which also the traditional dietary frame can be expected to have an important contribution. This is in line with the Peruvian-Amazonian epistemic understanding of the intervention, which considers the dietary procedure an active treatment component that is crucial in view of effectiveness and safety of such plants (Berlowitz et al., 2021; O’Shaughnessy & Berlowitz, 2021), thus the combination or interaction of factors seen as responsible for beneficial changes. The current sample reported high levels of perceived safety, and it is noteworthy that the discomfort and emetic properties in this application of tobacco make it unlikely for recreational usage. However, in view of the Tabaquero’s cautions regarding risks and the necessity of a trained Tabaquero for safe administration (for contraindications and risks see Berlowitz, García Torres, et al., 2020), and given the known toxicity of large doses of nicotine (Alkam & Nabeshima, 2019), assessing physiological safety parameters (blood pressure, respiratory, etc.) and pharmacokinetic profile will be a necessary next step, in close collaboration with an Amazonian Maestro Tabaquero.
Given the exploratory character and observational design of this study, the current findings are preliminary but overall point to a promising traditional treatment approach and epistemological perspectives on tobacco, which should be further investigated. The inclusion of traditional healers will be crucial in this context; although several psychoactives of the current psychedelic revival are originally derived from Indigenous healing systems (e.g., psilocybin, ayahuasca, iboga), emerging clinical studies tend to happen far removed from the cultures of origin (Bouso & Sánchez-Avilés, 2020; Fotiou, 2020a; George et al., 2020; Gerber et al., 2021). Debates on cultural fairness and intellectual property are thus pertinent in an ambiance of a rapidly growing for-profit industry around psychoactive compounds (Marks & Cohen, 2022; Phelps et al., 2022; Schenberg & Gerber, 2022), and it is also against this backdrop that the Tabaquero’s preference for non-disclosure of recipes should be understood. Forthcoming clinical research on Amazonian tobacco uses could in the long-term open new mental health therapies and alternative uses of a plant of which harmful uses currently prevail, thereby addressing ills of global modern society in collaboration with and acknowledgment of the expertise of Indigenous actors, otherwise notoriously underprivileged.
Supplemental Material
sj-docx-1-heb-10.1177_10901981231213348 – Supplemental material for Traditional Indigenous-Amazonian Therapy Involving Ceremonial Tobacco Drinking as Medicine: A Transdisciplinary Multi-Epistemic Observational Study
Supplemental material, sj-docx-1-heb-10.1177_10901981231213348 for Traditional Indigenous-Amazonian Therapy Involving Ceremonial Tobacco Drinking as Medicine: A Transdisciplinary Multi-Epistemic Observational Study by Ilana Berlowitz, Ernesto García Torres, Juan Celidonio Ruiz Macedo, Ursula Wolf, Caroline Maake and Chantal Martin-Soelch in Health Education & Behavior
Footnotes
Acknowledgements
We express our gratitude to the healer’s collaborators including WG, JG, LA, JP, and the VL family for supporting the logistics of this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that there is no conflict of interest. In keeping with the transdisciplinary approach, the Indigenous healer that provided the traditional Amazonian treatment is the second author of this work; data collection and analysis were performed independently by the scientific authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Swiss National Science Foundation (Grant No. 190428).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.