
Abstract
Key Points
Female collegiate dancers displayed a critical gap in nutrition knowledge, widespread body distortion and increased eating disorder risk.
Collegiate dancers should be routinely screened for nutrition and eating disorder risk prior to and throughout program participation.
Collaborative education programs that focus on nutritional knowledge, body image, and diet quality in dancers may reduce risk for eating disorders, and promote mental and physical health, and overall well-being.
Introduction
Dance as a discipline necessitates a unique combination of athletic rigor and aesthetic appeal. The constant physical scrutiny, including self-scrutiny through mirrors, creates an environment that can engender negative body image perceptions. Dance as a discipline requires a blend of athletic rigor and aesthetic appeal, often placing an emphasis on leanness. This combination of artistic and physical demands creates a unique environment placing the dancer’s body under constant scrutiny, including self-scrutiny from mirrors used in training.1,2 Benn and Walters referred to this body culture as a “cult of slenderness,” terming the practices and pressures to obtain the ideal, slim body type associated with professional advancement and recognition.1 -3 As such, this environment can provoke negative body image perceptions and development of disordered eating behaviors that may transition into clinically recognized eating disorders (EDs), with estimates suggesting that nearly one-third of dancers are at an elevated risk for ED. 4 Likewise, the collegiate environment may also propagate a preoccupation with body image due to factors including competitive academia, newfound autonomy, and pervasive societal beauty standards.5 -7 The convergence of pressures found in dance and college life may compound the risk for negative body image perceptions and ED risk in the collegiate dance population.
The overarching ethos of perfectionism present within the dance environment may also fuel the adoption of maladaptive eating patterns, evident in the reportage of collegiate dancers’ diets meeting only a fraction of their nutritional needs. 8 Consequences of such nutrient imbalances, whether intentional or not, can induce Relative Energy Deficiency in Sport (RED-S), disturbing health and performance across multiple physiological systems. 9 This complex picture is further confounded by a general deficiency in health literacy reported among dancers.3,10 -14 Ballet dancers with higher levels of disordered eating exhibited lower nutritional knowledge 10 and female collegiate dancers in the United States reported poor nutrition intake and low knowledge of the consequences of nutritional deficiencies related to performance. 13
Though the relationship between nutrition knowledge and dietary behaviors is complex,15,16 college is a period of transition and an ideal time to develop improved dietary habits that persist into adulthood. 17 Unfortunately, collegiate dancers infrequently report receiving nutrition education from a formal nutrition course or nutrition professionals. 8 Despite multifaceted difficulties faced by collegiate dancers, evidence suggests a promising openness within this group toward improving nutritional literacy when offered the insights and mentorship of registered dietitian nutritionists (RDNs). 13 As part of an educational intervention aimed at enhancing female collegiate dancers’ nutrition knowledge, participants viewed a brief educational video featuring RDNs, who focused on RED-S symptoms and fueling strategies, and reported significant gains in knowledge afterwards. 13
The prevalence of poor body image and elevated ED risk in collegiate dancers underscores the urgency of this inquiry. This study aims to explore the intricate relationships between body image perceptions, ED risk, and nutrition knowledge among collegiate dancers, including an understudied demographic—male dancers. By utilizing standardized tools, we seek to fill the gap in current literature and suggest actionable strategies for education and prevention within the dance community. Body image perceptions, ED risk, and nutrition knowledge were measured by standardized tools. Assessment and comparison of these characteristics according to gender fills a gap in the current dance literature. Ultimately, our goal is to elucidate these interconnections and identify actionable educational and preventive strategies to support the wellbeing of dancers within the collegiate environment.
Methods
Participants
A convenience sample of approximately 100 dance majors (estimated from the University’s rolling enrollment numbers) was recruited from academic programs at a public university in East Texas during 2019. 18 The university’s enrollment at that time was around 20,000 students. Methods for recruitment included emails, campus flyers, and announcements within dance departments. Volunteers who met the inclusion criteria of being an enrolled dance major aged ≥ 18 years were eligible to participate. All levels of student classifications were included. Students currently pregnant or with electronic pacemakers or other medical implants were excluded from participation.
Study Design
An anonymous online survey, hosted using Qualtrics software (Provo, UT), 19 was provided to potential participants. They were informed of all study measures, including the estimated time for completion. Participation was voluntary, and participants were free to withdraw at any time without penalty. Following consent, participants proceeded to the questionnaire. The questionnaire, which took approximately 20 minutes to complete, assessed demographic information, nutrition knowledge, menstrual history (for female participants), records of injury, and ED risk factors. Subsequently, participants were asked to visit the campus nutrition counseling center for anthropometric measurements and body image assessments. Participants were asked to generate a code consisting of details, including the first letter of the middle name (if none, X), the day of the month they were born, and the house number of their childhood address. A secure, participant-generated code linked survey responses with measurement data while maintaining anonymity. 20 The study received approval from the university’s Institutional Review Board (IRB #37369).
Procedures
Nutrition Knowledge
The Nutrition Knowledge Questionnaire (NKQ) 21 was adapted to be more relevant to the study and to reduce participant burden. For instance, 15 original questions, including the two-part questions that were opinion-based and open-ended, requiring participants to articulate specific disease states, were eliminated. The remaining questionnaire consisted of 19 items on the Dietary Guidelines for Americans to assess diet principles and 26 on nutrient content knowledge of foods. Correct responses were awarded 1 point for a potential maximum score of 45. Internal reliability for the adapted questionnaire was calculated as part of this study with Cronbach’s alphas of .92, .70, and .91 for the total, dietary guidelines, and nutrient content sections, respectively.
Menstrual History
For female athletes, obtaining a history of missed menstrual cycles or delayed menarche offers insight on nutritional status, as both conditions can accompany RED-S. For female participants, data on menstrual history were collected using a combination of multiple-choice, yes/no, and open-ended formats, asking about the age of menarche, contraceptive use, menstrual cycle regularity, and any history of missing menstrual cycles.
Eating Disorders
Risk for EDs was evaluated using the Eating Attitudes Test (EAT-26), a condensed version of the original EAT-40 questionnaire. 22 This 26-item tool, which identifies potential eating disorders, uses a 4-point scale (ranging from 0-3) for responses, with 1 item being reverse scored. Scores of 20 or higher indicated a need for professional evaluation, while scores below 20 did not rule out the presence of an ED. Standards from the EAT-26 for body mass index (BMI) were applied to identify participants needing further referral based on low BMI or affirmative responses to behavioral questions, which were adapted for relevance to this group of collegiate dancers. For example, we assessed the longevity of behaviors like binging or vomiting, rather than frequency, to determine if these issues were longstanding or present before entering the collegiate environment.
Anthropometrics
Standard procedures were used for height and weight measurements to calculate BMI. Participants removed socks and shoes for height measurements using a stadiometer to the nearest 0.5 centimeter. Weight was set to display in kilograms, a system unfamiliar to participants in this region, using an Inbody 770 bioelectrical impedance analyzer, an accurate assessment of body composition, 23 and corresponding handouts were provided only upon participant request. These considerations were made to minimize emotional distress. Participants were advised to fast and avoid exercise, saunas, and showers and to urinate prior to measurements to standardize conditions. This recorded data was used to compare with the participants’ body image responses.
Body Image
The BIAS-BD was administered to assess body image distortion (perceived versus actual size) and dissatisfaction (perceived vs ideal). 24 Through this, participants sorted figural drawings corresponding to BMIs between 16.5 and 39 kg/m2, into sequence by size, then selected drawings reflecting their actual and ideal body images. They also categorized drawings by weight labels for their own and the opposite gender to determine the agreement of body image perceptions and ideals across genders, 25 aiding the calculation of body distortion and dissatisfaction metrics. Drawings of increasing BMIs were color-coded uniquely by gender in an attempt to limit inferences and minimize participant emotional distress, and ease researcher recording.
Data Analysis
Descriptive statistics and reliability measures (Cronbach’s alphas) were used to characterize the data. Independent samples t-tests explored relationships and mean differences among variables and between genders. No gender non-binary responses were collected. Due to the small number of male participants, descriptive statistics were calculated to characterize male and female responses. As each component of the study had a slightly different sample size, analyses were calculated only on completed responses. IBM SPSS version 28.0 Software was utilized for all analyses.
Results
A total of 47 dance majors attempted to participate and opened the questionnaire. This represents an approximate response rate of 47%. However, only 35 participants provided demographic details, 32 to 38 participants completed various other components of the study; 29 female participants completed the menstrual section of the questionnaire. Due to the sensitive nature of the topic, participants were allowed to stop participation in any component of the study at any point. All participants in this cross-sectional study adhered to a minimum of 15 hours per week of dance practice as mandated by the curriculum. 26 Most participants were upperclassmen (66%), engaged in modern dance (69%), and reported dancing ≥9 years (77%). Table 1 details the demographic breakdown.
Characteristics of Dance Majors (N = 35) a .
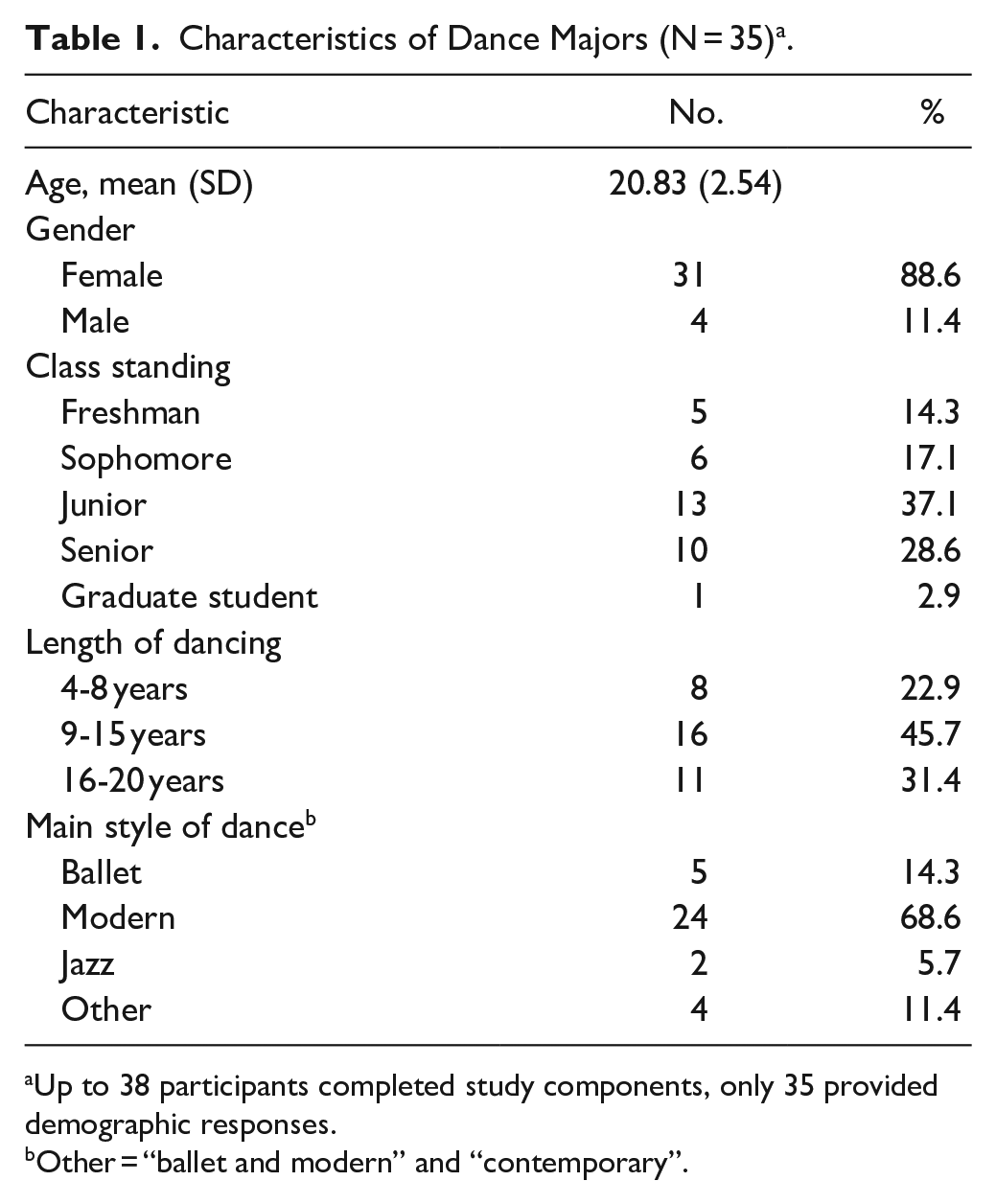
Up to 38 participants completed study components, only 35 provided demographic responses.
Other = “ballet and modern” and “contemporary”.
Nutrition Knowledge
The nutrition knowledge assessment was completed by 33 participants, yielding a 43.44% accuracy rate. Notably, only 12% surpassed a 60% correct response rate. Among the ten participants (30.3%) who had previously taken a formal nutrition course, the average score was slightly higher (mean 21.67 ± 6.10) compared to those without such coursework (mean 18.75 ± 9.39), although this difference did not reach statistical significance (t(31) = 0.86, P = .40).
Most of the 35 respondents to questions on nutrition information sources sought guidance from within their peer networks, with 65.7% consulting other dancers, 60.0% turning to family, and 57.1% to friends. Coaches or trainers (37.1%) and doctors (28.6%) were less commonly approached. A minority (14.3%) referenced receiving advice from an RDN or nutritionist.
Menstrual History
Menstrual history data were obtained from 29 female participants, revealing an average age of menarche at 12.86 ± 2.18 years. Late menarche (≥15 years) was reported by 24% (n = 7) of respondents which may occur with EDs. Additional statistical analysis of this sub-group was not possible due to sample size. Over half (51.7%) experienced regular menstrual cycles, while a significant fraction (24.1%) had missed more than 2 consecutive cycles. One-fourth reported using birth control, predominantly estrogen-containing preparations.
Eating Disorders
Overall, the total group (n = 32) had an EAT-26 score range of 0-30 out of a possible 0-78, mean 9.72 ± 8.75. Females (n = 28) scored an average of 11.82 (±9.53) on the EAT-26, higher than the average male score of 7.75 (±2.25), but this was not statistically significant, t19,2 = −1.86, (P = .079). EAT-26 subscales indicated mean scores of 6.09 (±6.08) for Dieting, 1.41 (±2.51) for Bulimia and Food Preoccupation, and 2.22 (±2.62) for Oral Control. Of those, the EAT-26 identified 6 participants (18.75% of those who completed the tool, n = 32) as having high ED risk (EAT-26 score was ≥20); all identified at risk were female, with 3 adhering to a vegan diet and 2 to a lactose-free diet. A sub-analysis of the 6 female participants scoring at high risk ≥ 20 on the EAT-26 reported using laxatives (33.3%), diet pills (50%) and having frequent feelings of being overweight (66%). Knowledge scores were similar to the entire sample. Notably, 53.8% of dancers not considered at risk with EAT-26 scores below 20 (n = 26), engaged in concerning behaviors, including binging (3.8%), dieting (23.1%), focusing on caloric expenditure (30.1%), diet pill use (3.8%), and frequent feelings of being overweight (38.5%).
Behavioral questions adapted from the EAT-26 suggested additional ED risk for those responding (n = 32) were binging (18.8%), laxative use (6.3%), and diet pills (15.6%). Nonclinical indicators of ED risk were prevalent; participants reported dieting behavior (40.6%), focusing on calories burned during exercise (46.9%), and frequently feeling “fat” (46.9%). Thirteen of 35 dancers (37.14%) who completed the behavioral questions reported adhering to self-restrictive diets including veganism (n = 5), lactose avoidance (n = 3), and other restrictions.
Perceived Body Image
Out of the 38 participants who completed the BIAS-BD, the majority were female (81.6%). Among females, the average measured BMI was 22.05 (±2.30), the perceived BMI was 23.27 (±3.74), and the ideal BMI was 21.78 (±3.47; Figure 1). The statistical analysis revealed a significant overestimation of body size (body distortion) t30 = −2.982, P < .01, but not body dissatisfaction t30 = −1.478, P = .150 when ideal body size was considered. Furthermore, males selected a notably heavier ideal body size for females (mean ideal BMI = 25.16 ± 4.36), compared to female selections of ideal female body size, t36 = −2.223, P < .05.
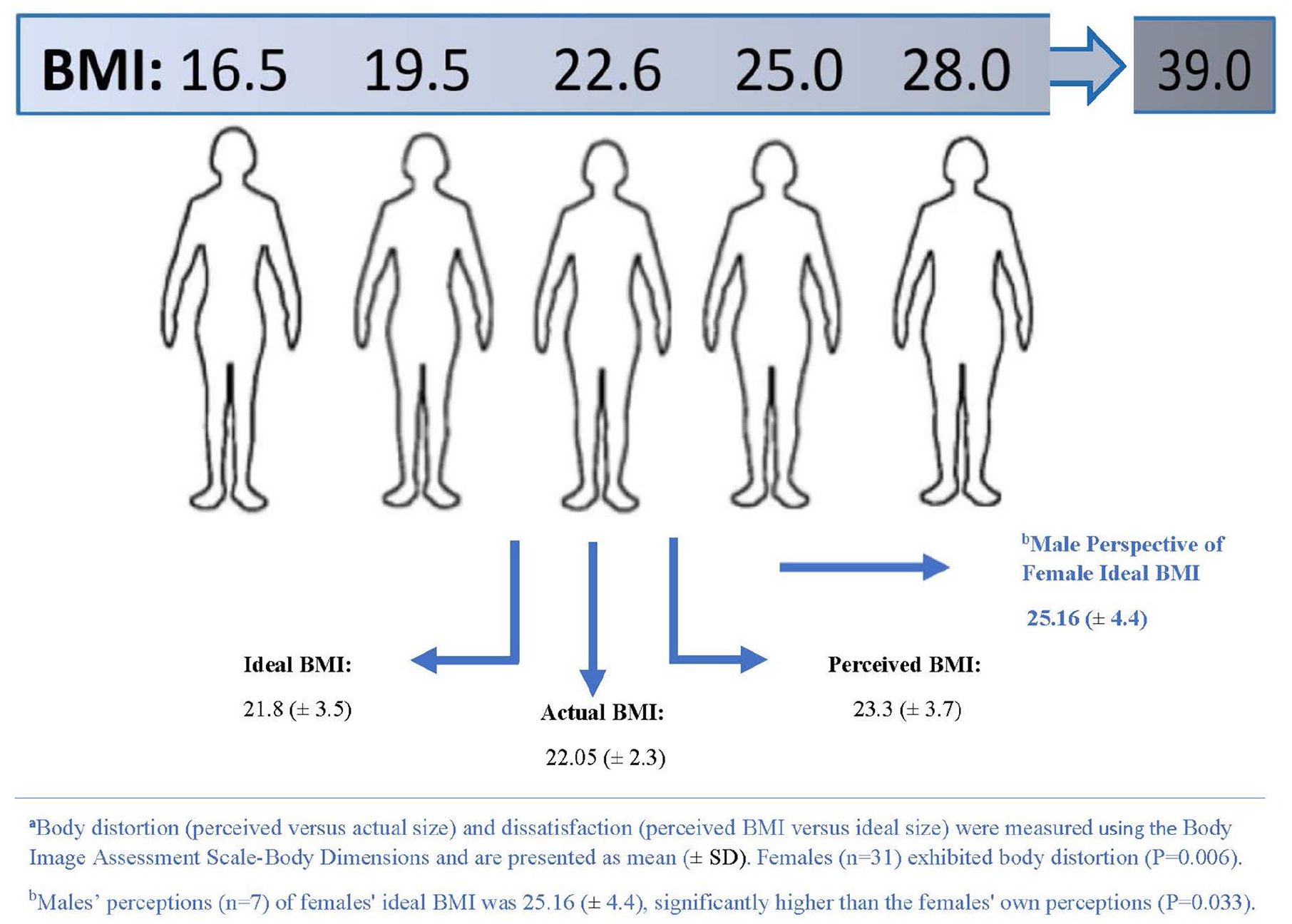
Overestimation of body size (body distortion) among female dancers using BIAS-BD (n = 31)a.
Male participants (n = 7) showcased a different pattern, with no significant indicators of body distortion or dissatisfaction (Figure 2). Their mean measured BMI was 23.61 (±3.1), perceived BMI was 23.18 (±2.02), and the ideal BMI selected was 24.30 (±3.93). Comparatively, the ideal male body size as perceived by females closely aligned with the male ideal (mean = 23.96 ± 2.66 vs. mean = 24.30 ± 3.93; t36 = .278, P = .782).
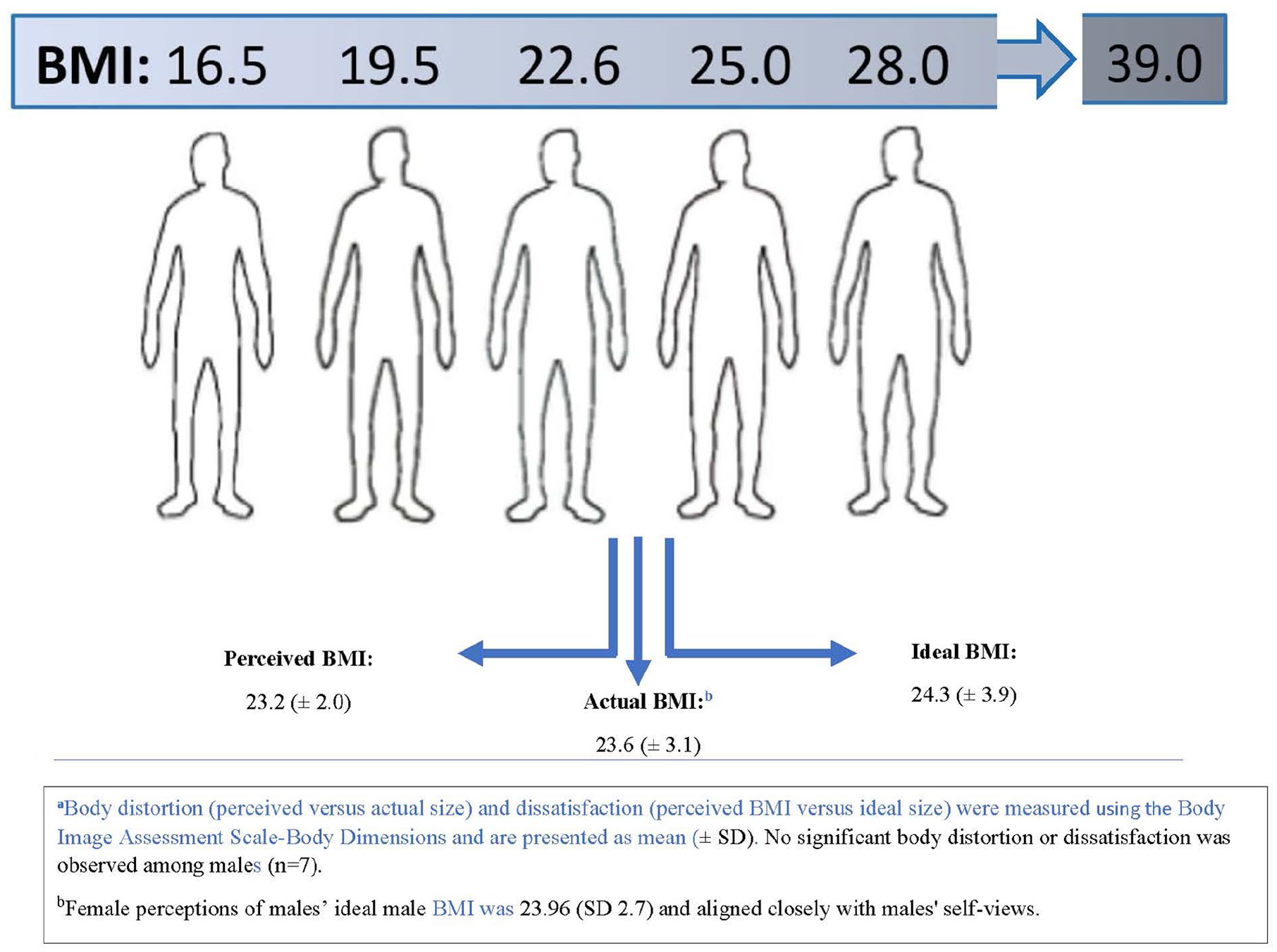
Body image assessment among male dancers using BIAS-BD (n = 7)a.
Discussion
In the hypercompetitive atmosphere of collegiate dance, where physical prowess intersects with aesthetic imperatives, dancers face multifaceted pressures that can engender adverse health behaviors and a predisposition toward EDs. The university setting compounds these risks through a confluence of academic competition, newfound autonomy, and amplified exposure to culturally entrenched beauty ideals. 5 This study advances the limited knowledge about the interplay between body image, nutrition knowledge, and dietary practices among male and female collegiate dancers, underscoring the necessity for targeted interventions.
The results of our nutrition knowledge questionnaire reveal a stark gap in the understanding of dietary guidelines among dancers. Although participants showed moderate familiarity with fundamental nutritional concepts, as evidenced by scoring around 50% for questions on recommended food groups, their proficiency markedly declined when addressing serving sizes and nutrient specifics—a worrisome trend given the critical role of diet in disease prevention and health promotions. These findings resonate with prior research indicating subpar nutrition literacy in dance populations and even among collegiate females with chronic disease at the same university.10,27 This is compounded by limited professional nutritional support and inaccurate and conflicting nutrition-related information available online, 28 with many dancers predominantly seeking advice from unqualified sources.
Concerning menarcheal timing, our study recorded a 26% incidence of late menarche, a symptom potentially indicative of existing EDs. Menstrual irregularities have been extensively documented among aesthetic athletes and are hallmarks of RED-S, a syndrome that wields detrimental ramifications across an athlete's performance and long-term health. 29
Our study also corroborates the negative body self-perception noted in other dance disciplines. 30 Employing the BIAS-BD, female dancers in our research cohort overestimated their body size, similar to patterns observed in other collegiate females participating in aesthetic lean sports31,32 as well as general university students. 25 Given the prevalent influence of beauty ideals, it is also possible the large discrepancy in actual versus perceived body size may, in fact, represent body dissatisfaction. Contrastingly, male dancers exhibited a discrepancy from female ideals, selecting a larger ideal body size—a divergence that was not statistically significant but nevertheless noteworthy. This finding has also been reported in university students, suggesting the belief that women think men prefer a thinner body size. In contrast to gender-neutral dissatisfaction in runners, 31 the findings suggest gender-specific body ideals within dance, with females striving for leanness and males for muscularity. Whereas Italian university male students using a similar-silhouette-matching process, reported a larger actual size than their ideal, or what was reported as attractive by female students. However, this population with similar BMIs did not assess perceptions according to sports engagement. 25
The influence of mirrors in dance studios, 33 performance-related emphasis on appearance, along with gendered performance roles necessitating lifts and support, may intensify the focus on body image within the domain of lean sports. It is plausible that these factors contribute to the pronounced gender differences in body perception observed in our study participants. The internalized ideal of thinness for women and muscularity for men in dance may possibly be informed by these environmental cues within the dance culture.
Given these concerns, it is imperative to develop and implement effective screening tools that can identify dancers at risk for negative body image, EDs, and related complications. Moreover, the provision of targeted nutrition education tailored to the unique demands of dancers should be prioritized. It would be beneficial for such educational interventions to be developed in collaboration with dietitians specializing in sports nutrition and, ideally, with experience in the performing arts.
It is worth highlighting that, while male dancers were fewer in number within our participant pool, the gender disparity in ideal body size preferences signals a nuanced dynamic that extends beyond the pursuit of leanness. This suggests that body image interventions in dance should be sensitive to the varying aspirations and pressures experienced by male dancers, which might differ from their female counterparts.
Lastly, the seemingly endemic reliance upon unspecialized peers for nutritional advice flags a broader issue of accessibility to expert nutrition counsel within collegiate dance programs. Enhancing the availability of RDNs who are versed in the needs of performing artists could bridge this critical gap, empowering dancers with the knowledge to support both their performance ambitions and their overall well-being.
In conclusion, the findings of the present study underscore a pressing need for concerted efforts to address the intertwined concerns of body image, nutrition, and eating behaviors among collegiate dancers. Collaborative initiatives between health professionals and dance institutions can potentially offer tailored support, mitigating the risks associated with the unique challenges faced by this population.
Limitations
Given the demanding schedules of collegiate dancers, particularly males, a limited response rate was observed, which may affect the representativeness and generalizability of the findings. The data collected from ballet and modern dance practitioners were not exhaustive due to incomplete participation in all research facets. Perhaps inter-institutional research would yield larger samples as would incorporating data collection into designated time periods within the dance program schedules.
Demographic information about race or ethnicity, diet details, and self-reported hours of physical activity were not captured, limiting the ability to provide a comprehensive contextual background for the findings. The absence of detailed activity data curtails the understanding of participants’ energy expenditure in relation to their body image and nutrition. Future research would benefit from including more detail on energy expenditure and energy intake, and its relationship with dietary behaviors.
Body composition assessment methods could have reflexive effects on self-reporting, potentially introducing response bias in assessments of body image and eating behaviors. It is possible that not all participants adhered to body composition preparation instructions, potentially influencing measured differences. The use of BIAS-BD figural drawings may inadvertently emphasize or exacerbate levels of perceived body dissatisfaction and distortion. 24 Additionally, while valuable for screening, the EAT-26 must be recognized as non-diagnostic, with caution exercised to avoid overinterpreting ED risk indications. Because studies in the literature are often limited in sample sizes, it is difficult to analyze individual behaviors. However, a more recent study conducted in South Carolina reported 19.2% binging behaviors, 8% diet pill usage, and no laxative use. These findings are considerably different than this study and most likely reflects sample sizes, differences in types of dance, and study designs. 34
Inherent risks of validity compromise accompany self-report measures, and the study results may have been influenced by tendencies to either overemphasize or underreport responses despite participant intentionality.
Practical and Clinical Applications and Implications
These limitations notwithstanding, the findings of this study contribute to the existing literature, highlighting a critical gap in nutrition knowledge, widespread body dissatisfaction, and a heightened risk of EDs in the collegiate dance community. These issues underscore the need for establishing routine nutrition screenings and ED assessments, critically at the introduction of college life and during other vulnerable periods.
Statistics indicating an alarming increase in ED prevalence among college students, with rates escalating to 51.8% for women and 31.3% for men, 6 reinforce the urgency for preventative action in all college students, which includes collegiate dancers. Systematic evaluations are advocated to enable the identification of dancers who might benefit from early, specialized interventions.
Education directed toward dance educators and students is vital to enhance nutritional understanding, mitigate ED risks, and counteract the proliferation of nutritional misinformation. The implementation of these educational endeavors may be most effective through partnerships with RDNs and by building on the nutritional services available on campus. Targeted nutrition education could include nutrition topics related to RED-S, performance enhancement, and injury prevention and recovery. Consideration should be given to both didactic and experiential learning strategies, and be incorporated into the dance curriculum to ensure participation. As part of the continuing education of dance educators, workshops or seminars on focused nutrition topics could be delivered either in-person or as webinars. A dance program’s involvement in the development and/or delivery of nutrition education would demonstrate support for the importance of nutrition to the well-being of the dancers.
School-based body image interventions led by experts have demonstrated success in youth, 35 but a united approach is critical as unrealistic body ideals may be unknowingly supported by the dance environment or leadership. Professional development aimed at leadership may enhance the efficacy of program interventions as dance educators are instrumental role-models and can uphold program policies on a day-to-day basis. 36 Integrating collaborative educational programs with additional assistance from trained psychologists, athletic trainers, and physicians could play a significant role in supporting the present and future needs of collegiate dancers for physical and mental health, injury prevention, optimal performance, career longevity, and overall well-being.
Conclusion
This study contributes to the body of evidence highlighting the necessity for enhanced nutritional support and screening within the dance community. The prevalence of distorted body perceptions, exacerbated by the rigorous scrutiny dancers face in appraising their physical form, both self-imposed and from external observers, has considerable implications for their well-being. Such continuous assessment has the potential to precipitate the development of disordered eating behaviors and amplify the risk of eating disorders EDs.
The employment of screening tools, exemplified by the Eating Attitudes Test-26 (EAT-26), emerges as a valuable strategy to timely identify individuals at heightened risk. Early detection is crucial in channeling these students toward appropriate support systems. The integration of an RDN into the health and wellness framework for the dance population is underscored as pivotal. An RDN can offer expert guidance, creating and administering scientifically grounded nutritional plans conducive to both the artist's health and performance as well as provide additional expertise as part of a dance education team. A collaborative and inclusive approach appropriate to the individual dance environments that tackles the mental and physical challenges may equip the collegiate dancer to overcome the complex challenges of dance and, possibly, support career longevity.
In light of these findings, it is recommended that dance programs proactively establish systematic nutrition screenings facilitated by collaborations with nutrition professionals. Fostering an environment that empowers dancers with the resources and knowledge to navigate dietary decisions promises to mitigate the risk of EDs and enhance overall physical health.
Footnotes
Author’s Note
All authors listed meet the criteria for authorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.