
Abstract
Introduction:
The importance and potential benefits of muscular strength in the adolescent’s development for health and fitness has been demonstrated in the literature. Maximal muscular strength and its assessment, however, is not a primary assessment criterium in the selection of young talented dancers.
Methods:
The present study evaluated the within- and between session reliability, variability, and minimal detectable change (MDC) of the isometric mid-thigh pull (IMTP). Thirty-five participants (female n = 17) participated in 2 identical assessments on the same day with 4-hour break in between. Three 3-second IMTP were performed, and the mean peak force value was used for the analyses.
Results:
Within-session the ICC indicated excellent reliability (ICC = .99, 95% CI: 0.98-0.99). Between-session reliability was excellent (ICC = .98, 95% CI: 0.95-0.99). The standard error of measurement was 4% (48 N), the minimum detectable change was 12% (134 N) and the CV was 3%. There were no within-session statistically significant differences, but statistically significant differences between-session were observed (P < .001). Limits of agreement ranged from −121 N (95% CI −186 to −56 N) to 307 N (95% CI 243-372 N).
Conclusion:
The observed results demonstrated excellent within- and between sessions reliability, low variability, and an MDC of 12%. The consistency of the within-session scores suggest that peak force data may be obtained with single try efforts. The statistically significant difference in the means of the retest session, however, suggests that the time of the day or the time since entrained awakening may be affecting performance in adolescent dancers. The results of the current study indicate that the IMTP is a reliable assessment tool for maximal muscular strength in adolescent dancers.
Key Points
The isometric mid-thigh pull is a reliable assessment tool for maximal muscular strength in adolescent dancers.
Providing that young dancers have enough time to familiarize themselves with the isometric mid-thigh pull protocol, single try efforts may suffice for peak force assessment.
Practitioners are advised to consider the time of the day as a confounder when they conduct the isometric mid-thigh pull test.
Introduction
The importance of physical fitness in children and adolescents has been clearly demonstrated in the literatures.1 -3 Over the last decade experts in youth development have published an international consensus on the importance of muscular strength in children and adolescents. 4 Empirical evidence further supports this, indicating that muscular strength enhancement in young athletes can improve physiological performance, 5 reduce associated injury risk factors, 6 and have a positive effect on health and well-being. 4
Numerous studies 7 have demonstrated that increased maximal strength relative to body mass can improve performance in explosive lower body movements, such as sprinting,8,9 agility, 8 and vertical jumping.10,11 Jumping is an integral part of the training of an adolescent dancer, with jumping rates similar to those that are observed in volleyball. 12 Jumping and landing have been identified as common mechanisms of injury in professional ballet dancers.13,14 Jumping is also regarded as a fundamental motor skill in youth development. 15 Higher levels of fundamental motor skills demonstrate higher level of sport specific skill.16,17
Research on the relationship between muscular strength and esthetic performance in esthetic sports and dance is limited. There is some evidence indicating that higher level gymnasts produce a greater rate of force development. 18 In dance, Blanco et al 19 suggest that a higher countermovement jump is associated with higher quality in the grande jeté, a ballet specific jump. Nevertheless, muscular strength and power assessment is not widely included in talent identification of youth dance. The appropriate assessment of these parameters in adolescent dancers can assist practitioners to monitor physiological development and performance. However, this may not always be feasible due to either financial (eg, lack of equipment) or personnel limitations.
There are several established methods of maximal muscular strength assessment; repetition maximum tests, predictive protocols, isometric assessments, and eccentric protocols. 20 It has been demonstrated that repetition maximum tests are safe and appropriate for adolescents, as long as they show technical competency and are supervised by qualified professionals. 21 When competency or training age is low, however, the use of multi-repetition maximum protocols seems a more plausible method of assessment. 4 The practitioners or researchers can then predict the 1 repetition maximum in youth. Multi-repetition maximum tests, however, are not as accurate as 1 repetition maximum for maximal strength evaluation and can increase the risk of fatigue accumulation. 22
The isometric mid-thigh pull (IMTP) is an assessment tool for maximal isometric strength frequently used in adult populations, 23 in a variety of sports.8,24,25 Even though the test is isometric, it correlates to dynamic athletic tasks such as vertical jump performance, 23 and sprinting. 26 The assessment has 2 primary applications, (1) the quantification of maximal force-generating capacity, known as peak force, and (2) to assess the rate at which force can be generated, known as rate of force development (RFD). 8 The IMTP has been established as highly reliable in trained adults,27 -29 and professional athletes. 30 Recent studies have utilized the IMTP to assess maximal isometric strength in young male soccer players, 24 young female athletes, 31 and young female gymnasts. 18
For an assessment tool to be deemed suitable for use, it needs to display the necessary level of reliability. 29 The aim of the study, therefore, was to investigate the within- and between-session reliability, variability, and minimal detectable change (MDC) of the peak force during the IMTP in adolescent dancers.
Methods
Experimental Approach to the Problem
The participants were required to attend 2 identical data collection sessions separated by 4 hours. Participants were given 24 hours rest following their last dance class and did not participate in any other form of training on the day.
Participants
An open invitation for participation was verbally given to 7 year groups (n = 160 participants) at a vocational dance school. The youngest year group was excluded as the students were not familiar enough with the testing protocol. Based on Morrow and Jackson 32 recommendations on establishing the reliability of a test or a measurement, the sample size target was >30 participants. Thirty-five adolescent dancers (male: n = 18, age: 14.0 ± 2.17 years, height: 160.0 ± 9.7 cm, mass: 46.0 ± 11.1 kg; female: n = 17, age: 14.0 ± 1.05 years, height: 156.0 ± 6.67 cm, mass: 40.0 ± 5.75 kg) volunteered for this study. Participants needed to be injury free prior to data collection, and they needed to have had experience in the IMTP test protocol, minimum 4 times within 1 academic year. Four testing sessions in an academic year would equate to minimum 24 isometric pulls (3 warm-up pulls plus 3 assessment pulls multiplied by 4 sessions). The participants were exposed to varied amount of dance hours per week (range: 17-27 hours per week). Parental informed consent was obtained for all the participants and ethical approval was attained from the University of Wolverhampton ethics committee.
Procedure
The sessions began with a warm-up that consisted of a 2-minutes light cardiovascular exercise and dynamic stretches targeting the large muscles of the lower body, the back, and shoulders. All participants were familiar with the IMTP test protocol as it was routinely used to monitor their fitness, typically 4 times in a year. A 3 second, as opposed to the customary 5 second8,33 IMTP was used as the measure of lower body strength. The decision was based on the coaching experience in adolescents of the lead author. Participants stood on a custom-made platform where a load cell (LCM Systems Ltd, Newport, UK) was anchored, and the signal was processed by Powerlab (AD Instruments, Dunedin, New Zealand). On the other end of the load cell there was a chain and at the end of the chain a small bar that was placed at mid-thigh. They were asked to assume the position by self-selecting their hip and knee angles 8 whilst following the instructions, to place the chain between their feet, and their feet underneath their hips, to keep their knees soft, their back flat (neutral) and upright, and their chest out. The height of the bar was recorded for the re-test assessment (Figure 1).
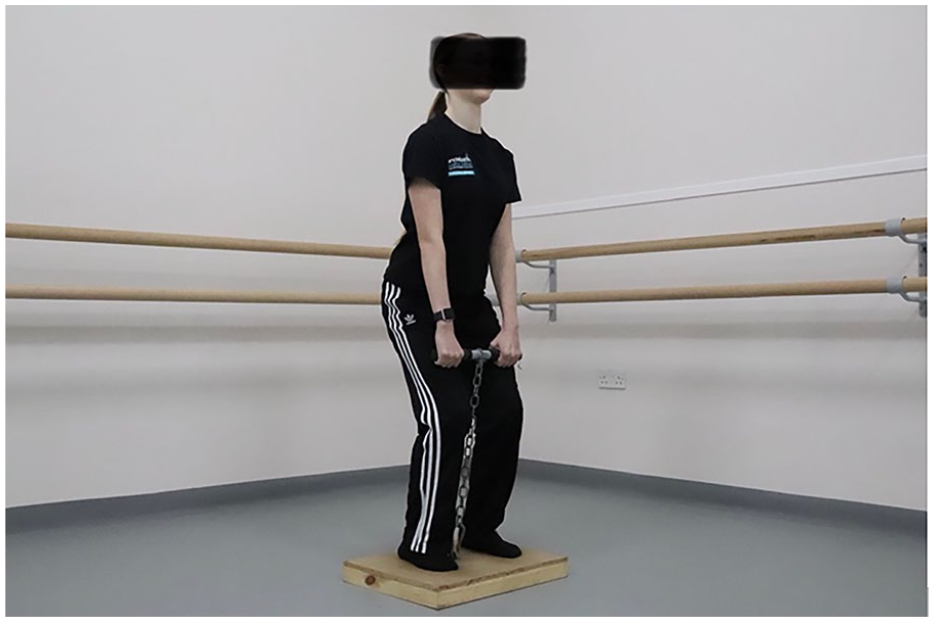
Isometric mid-thigh pull setup.
Each participant was provided 2 warm-up pulls, 1 at 50% and 1 at 75% of the participant’s perceived maximum effort, with 1 minute rest in between. 24 Once the warm-up pulls were completed the participants were given a countdown of “3, 2, 1, Pull.” The participants were instructed to relax before the command “Pull!” to avoid the precontraction. 8 They were then asked to pull the bar with their hands and push the platform away with your legs whilst maintaining their posture, with no backward leaning. The participants were instructed to refrain from a final moment jerk in their pull just before the completed 1 try. The pull lasted for 3 seconds, for 3 consecutive times with 60 seconds rest between the pulls. Strong verbal encouragement was given for each trial. The peak force (N) was then recorded and was used for the analysis.
Statistical Analyses
To evaluate the reliability of the within- and between-sessions we calculated the intraclass correlation coefficients (ICCwithin 2,1; ICCbetween2,k) and the 95% confidence intervals (CIs) 29 with a two-way mixed-effects model for absolute agreement. 34 ICC values less than .50 are indicative of poor reliability, values between .50 and .75 suggest moderate reliability, values between .75 and .90 indicate good reliability, and values greater than .90 suggest excellent reliability. 34 MDC was then calculated to assist practitioners understand the difference between noise and meaningful change in the data. 35 The mean and standard deviation (SD) of the peak force was calculated from the 3 trials from the 2 sessions. The assumption of normality was assessed with the Shapiro-Wilk test.
Standard error of the measurement (SEM) and MDC were also calculated to establish the between-sessions random-error scores.
36
SEM was calculated with the following equation
Two-way repeated measures analysis of variance (ANOVA) was conducted to assess the change of the within-session means. Paired-sample t-test was conducted to assess the difference of the between-sessions means. The relationship between the difference and the magnitude of the between-session measurements together with the potential systematic bias (the mean of the differences between the 2 measurements) were assessed by the Bland-Altman plot and the 95% Limits of Agreement (LOA). LOA was set as the mean difference between test and retest scores ±2 SD from the mean. 38
Data are presented as mean ± SD, whereas alpha level was set at P ≤ .05. The descriptive statistics, ICC, and SEM together with their 95% CIs were calculated with SPSS v28 statistical software (SPSS Inc., Chicago, IL, USA). The between-session intra-subject variability was established through the coefficient of variation (CV) which was calculated using the EnvStats R package. 39 All remaining analysis was conducted using the statistical software Jamovi version 1.6 (www.jamovi.org).
Results
Descriptive statistics for all the tries in the 2 sessions are presented in Table 1. Within-session the ICC indicated excellent reliability (ICC = .99, 95% CI: 0.98-0.99).
Descriptive Statistics for IMTP, Standard Deviation, Standard Error, and Minimum Detectable Change.
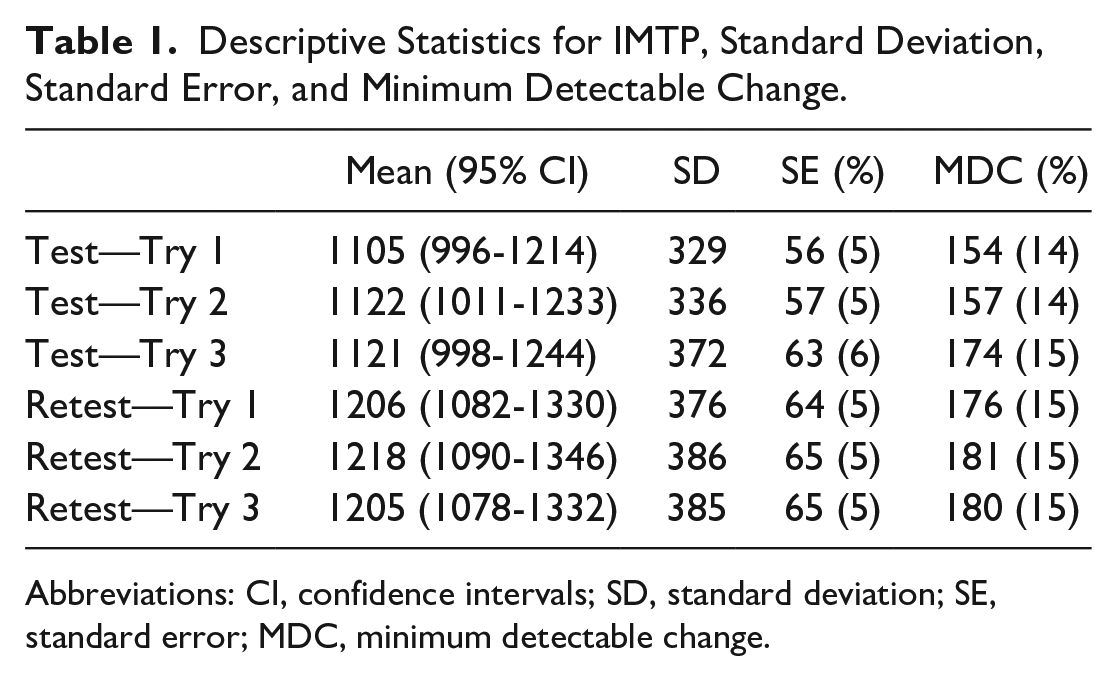
Abbreviations: CI, confidence intervals; SD, standard deviation; SE, standard error; MDC, minimum detectable change.
Between-session reliability was excellent (ICC = .98, 95% CI: 0.95-0.99). The standard error of measurement was 4% (48 N), the MDC was 12% (134 N) and the CV was 3%. There was no within-session statistically significant difference. The results from the morning (M = 1116 ± 342 N) and afternoon (M = 1209 ± 377 N) sessions indicate a statistically significant between-session difference (Mdiff = 93 N; t(34) = 5.04, P < .001; d = 0.85).
Limits of agreement ranged from −121 N (95% CI −186 to −56 N) to 307 N (95% CI 243-372 N). The Bland-Altman distribution plot demonstrated that, if a new individual from the studied population was assessed, the differences between any 2 tests would be expected to lie within the limits of agreement with an approximate 95% probability. 40 The estimated mean of the differences (bias) was 93 N (95% CI: 55-131 N) (Figure 2).
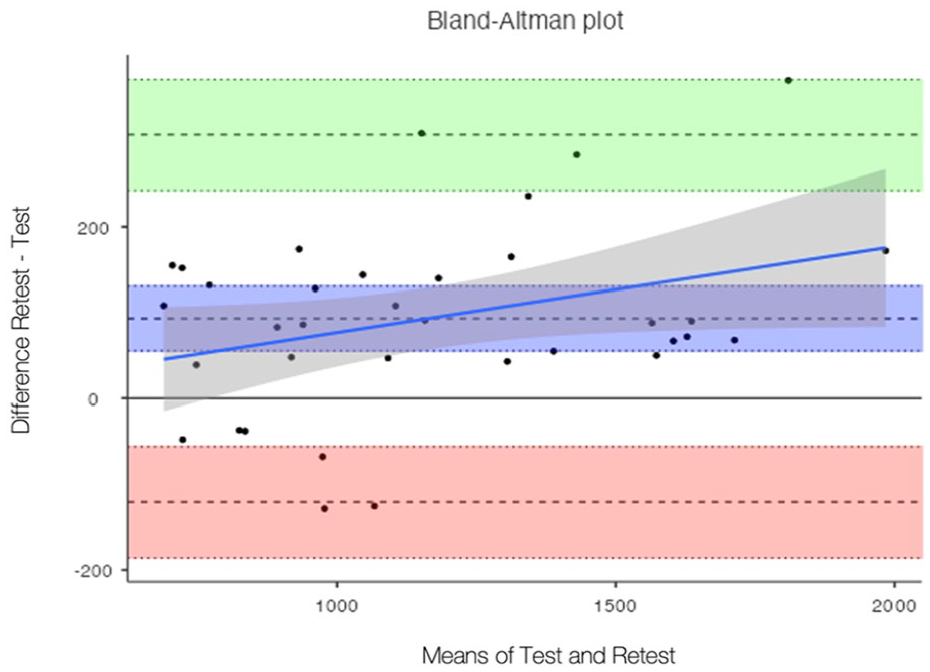
Bland-Altman distribution of the between-sessions IMTP agreement analysis (n = 35). Limits of Agreement are shown in dotted black lines with 95% confidence intervals in light green for upper limit and light red for lower limit. Bias (as dotted line) with 95% confidence interval (purple area), and regression fit of the differences on the means (as solid blue line) and 95% confidence interval (gray area).
Discussion
This is the first study to assess the reliability of the IMTP in adolescent dancers. The aim of this study was to assess the within- and between-session test-retest reliability, variability and MDC of this assessment tool. The findings indicate excellent levels of reliability as described by within-session ICC of .99 and between-session ICC of .98, with low variability (CV = 3%). The associated confidence intervals can provide more insight about the consistency of the measurements as for both the within and between-session ICC, the lower bound remains >90. The relationship between the difference and the magnitude of the between-session measurements that was assessed by the Bland-Altman plot and the 95% Limits of Agreement (LOA) suggest that the IMTP is a reliable method for assessing peak force in adolescent dancers. The potential systematic bias (93 N) between the sessions cannot be associated with a potential learning effect as the participants were all experienced with this test. The bias may be suggesting that the time of the day is a factor to consider, as the afternoon scores were higher than the morning scores.
Our results indicate similar within- and between-session reliability scores to De Witt et al
27
(
We observed no within-session statistically significant difference in both sessions. This further supports the findings of a study with adolescent gymnasts. 31 Moeskops et al suggest that providing young athletes enough familiarization time with the IMTP test, peak force measurement can be obtained from a single trial. This makes the IMPT easier to administer and more time efficient, when practitioners are dealing with large population (ie, school setting) and there is limited time availability for screening.
There was between-session statistically significant difference in the scores (P < .001). This may be associated with the time of the day that the pre (11am) and post (3pm) testing took place. A study with 10 to 11 years old boys indicates a time-of-day effect, with performance in strength and power improving from morning (8am) to afternoon (2pm). 42 Also, it has been previously suggested that personal best performance of athletes is affected by the time of the day in swimmers,43,44 judo athletes, 45 and young soccer players. 46 Facer-Childs and Brandstaetter 47 however, suggest that time since entrained awakening is a strong predictor of peak performance, and not just the time of the day. Although we did not check the time our participants had woken up, the first assessment was performed closer to their wake-up time, approximately 2 to 3 hours after breakfast. Whilst the IMTP indicates excellent reliability, practitioners should consider the time of the day when they conduct the assessment. More than 3 hours from the time the adolescents wake-up or simply conducting the assessment in the afternoon may be advisable if they want to obtain peak force scores closer to the individual’s personal best.
Test-retest reliability sessions are customary conducted with minimum 24-hour rest in between.24,27,31 The current study’s test-retest assessments were conducted on the same day with 4 hours break between, with no signs of fatigue in the pre-post measurements. It has been previously suggested that the IMTP induces minimal fatigue and is time efficient. 30 For these reasons, practitioners in similar environment of high training load and lack of availability time for the participants may consider utilizing the IMTP as an assessment tool for maximal muscular strength.
This study is characterized by several limitations. Maturation status was not taken into consideration. Moeskops et al 31 have indicated the pre-peak height velocity athletes showed greater variability in absolute and relative peak force than post-peak height velocity athletes. The authors further suggest that there is systematic bias within the less mature group, therefore, further familiarization may be necessary. 31 Due to the age range of our cohort, there may have been individuals at a different maturation status. All our participants, however, had a minimum of 1 year experience with the test (minimum 24 isometric pulls) and therefore any potential learning effect bias may have been eliminated. We did not investigate the rate of force development, therefore, further research is needed for more detailed force-time curve variables in adolescent dancers with biological maturation taken into consideration.
Practical Applications
There are many different test protocols to assess muscular strength capacity in adolescent dancers, however, these protocols require some level of technical competency for adolescents to safely perform them. The IMTP is validated against 1RM squat performance, 23 therefore it is a reliable alternative for maximal strength capacity assessment in young individuals with low training age or experience. Providing that the participants are given enough time to familiarize with the protocol, the IMTP is a safe assessment for adolescent dancers, especially if the training age is low and the participant has little or no experience in resistance training. In addition, the test is self-regulated, therefore familiarization is easier and safer. The lack of vertical load may also potentially make the IMTP easier to implement in the traditional setting. Health practitioner and strength and conditioning coaches can use the current findings to monitor and establish real changes in IMTP performance and should look for changes in peak force greater than 12% to identify meaningful changes in response to training in adolescent dancers. The time of the day of the assessment together with the time since entrained awakening should be taken into consideration for practitioners to obtain closer to personal best peak force performance in adolescent dancers. Lastly, it may not be feasible for non-boarding schools to have a 24-hour break between the assessment day and the last training day. Further research should focus on testing peak force on a dance day to assess the magnitude of the dance schedule on the scores.
Conclusion
This is the first study to investigate the within- and between-session reliability, variability, and MDC of peak force in the IMTP. The results demonstrated excellent within- and between-session reliability, low variability, and an MDC of 12%. The consistency observed in the scores for all the tries suggest that peak force data may be obtained with single try efforts, once the participants are familiar with the testing protocol. Higher scores were observed in the afternoon retest session; therefore, practitioners should consider the potential time-of-day effect when conducting the IMTP test. The findings of this study make the isometric mid-thigh pull a reliable assessment tool for maximal muscular strength in adolescent dancers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.