
Abstract
The field of traumatic stress is often referred to as being in a state of controversy and lack of continuity. Throughout history, disputes repeatedly centered on defining the psychological consequences of severe adverse events and on their causes. Even to this day this is current. To understand these controversies, an extensive historical literature review is presented of how mental consequences of trauma have been described in history, of the circumstances in which this took place, and of the disputes that have influenced the conceptualization of these mental responses. We found psychotrauma always being surrounded by controversy. Significant heterogeneity in symptom expression has been described over the centuries to this day. Some symptoms appeared steadily over many decades, but often each time period showed its own core symptoms. At syndrome level, we found an acute condition, one with longer duration, and a complex condition. Also here, definitions varied over the decades. Finally, causes have always been debated, such as biological, psychological, socio-economic, cultural, political, or legal. To better reflect the described ongoing variation in symptomatology, a more flexible diagnostic approach is proposed with a combination of both staging and subtyping that offers room for a more flexible, symptom-oriented, and personalized perspective.
It is hard to find a province of psychiatry in which there is less discipline than this one. There is practically no continuity to be found anywhere, and the literature can only be characterized as anarchic. (Kardiner, 1959, p. 245)
Throughout history, descriptions of the psychological aftermath of severe shocking or traumatic experiences have been reported. A common thread has been a constant dispute about the consequences of these events in terms of terminology, cause, and description of psychic posttraumatic symptoms and syndromes. The inclusion of the diagnostic category Post Traumatic Stress Disorder (PTSD) in DSM-III (Diagnostic and Statistical Manual, third edition; APA, 1980) was an attempt to unify the psychotrauma field and has been described as a paradigm shift in the conceptualization of psychological trauma (Jones & Wessely, 2007). Nevertheless, also after 1980, the field of traumatic stress was described as in a state of anarchy (Boulanger, 1990), while others described the field as shredded or truncated, where central insights of earlier findings of trauma scholars were lost (Ehrenreich, 2003; Gersons & Carlier, 1992). Up to the present day, even the official diagnostic manuals show mixed opinions. While the PTSD definition in DSM-5 became very extensive (APA, 2013), the ICD-11 (International Classification of Diseases, eleventh edition; WHO, 2018) defined PTSD on the basis of only limited symptoms. So, in the coming years, patients, clinicians, and researchers are faced with two official PTSD concepts which do not convey much unity in the trauma field.
To understand this lack of unity, it is imperative to look back into the history of psychotrauma (Ben-Ezra, 2011). A historical review provides important clues that shed more light on the genesis, developments, and manifestations of psychological concepts over the centuries, allowing a better understanding of influencing factors, discussions, recurrent dilemmas, and pitfalls about these changing concepts. This will not only lead to a better recognition and understanding of current discussions, but will also allow for better ways to define posttraumatic psychopathology and the dilemmas involved. Several questions are important here. For instance, why are scientists and clinicians repeatedly confronted with different concepts of trauma-related disorders and why are they still unable to reach agreement on what exactly posttraumatic psychopathology entails?
Accordingly, in the present article, we aimed to investigate the ways posttraumatic symptoms and syndromes evolved and changed over time, and under what conditions and influences this occurred. To this end, we employed a historical literature review. The broad scope of such a review is irreplaceable to track and examine the origins, progress, and changes of clinical concepts in time (Ferrari, 2015). This provides an opportunity to examine the literature on psychotrauma through the ages, starting with the first time concepts emerged in the scientific literature, then following their evolution in chronological order, and summarizing clear trends. From there, we discussed the findings from a broader historical perspective and described a direction from which desirable new developments in posttraumatic psychopathology can be better defined.
For this review, we first collected influential review articles published in scientific journals in the last 30 years. From there on, we collected other pivotal reviews, and subsequently we retrieved original papers. Per era, a selection of the articles was made. The articles should include the description of specific traumatic or serious adverse life events. In addition, the psychological consequences associated with these events should be described. We limited our search to articles published in scientific journals in the English language, involving adults only. We made exceptions in case significant contributions were only described in book chapters or in non-English publications.
Psychotrauma Before the Introduction of PTSD
Although already in ancient times reports were made about psychological trauma and its consequences, the first to introduce the term “psychic trauma” was, to our best knowledge, the German professor in neurology Eulenburg in 1878. He regarded “psychic trauma” as a sudden action of tremendous emotions that could cause a molecular concussion of the brain, which he compared with the concussion of the brain after physical trauma (Van der Hart & Brown, 1990).
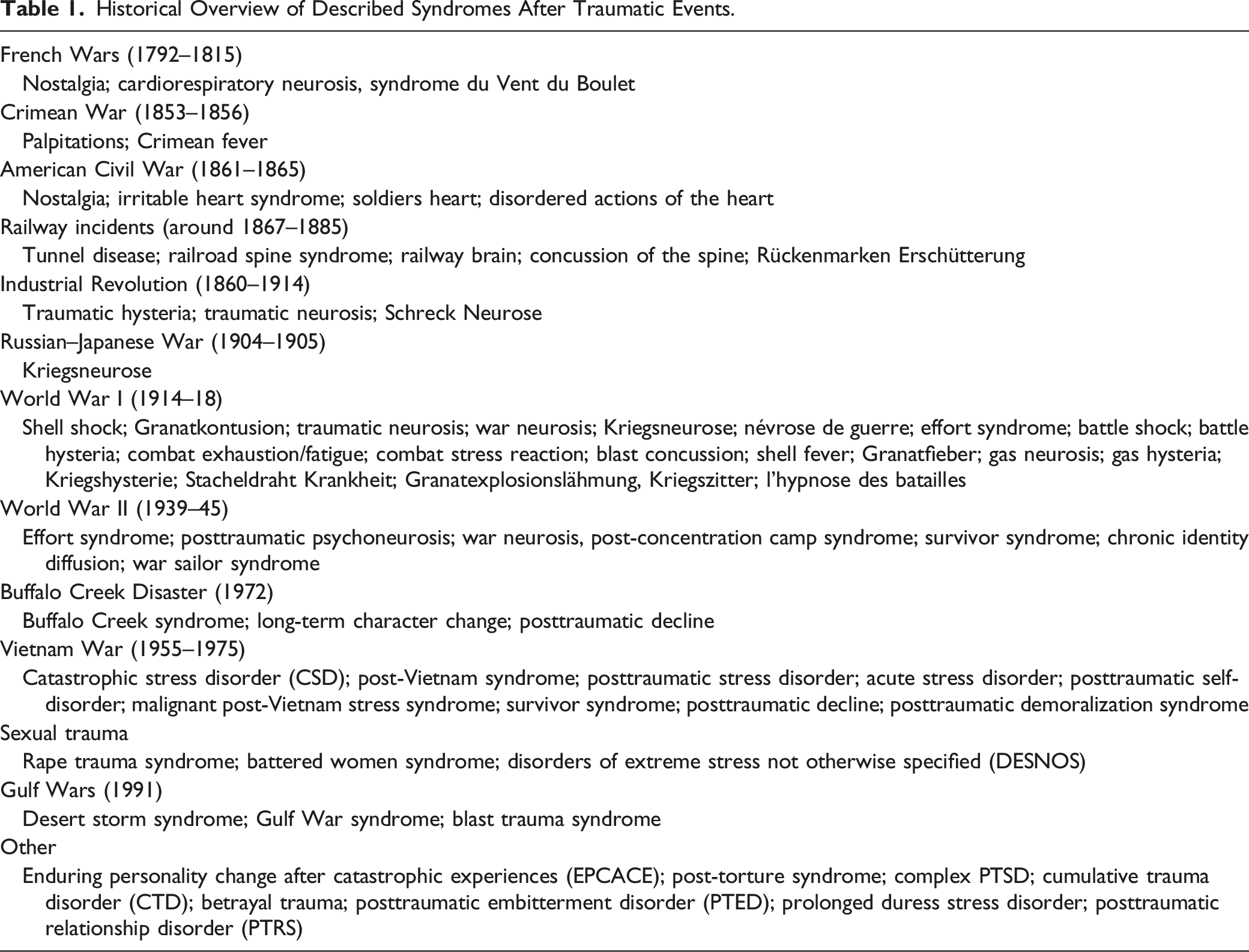
Historical Overview of Described Syndromes After Traumatic Events.
Industrial Revolution
During the second half of the 19th century, clinicians were confronted with patients who, next to physical casualties, exhibited psychological complaints after accidents and calamities. Victims were mainly working class men, who worked in construction sites and factories, as well as victims of accidents because of the rapidly increasing use of trains (Weisaeth, 2002). In several European countries, accident insurances were introduced providing financial compensation for injured victims. The combination of societal, clinical, and legal contexts in this episode had a significant impact on the diagnostic developments of the consequences of these serious events.
The often serious railway-accidents with many casualties led to significant societal concern, especially in Great Britain. In 1866, the physician Erichsen described the “railroad spine syndrome,” which consisted of a variety of symptoms including anxiety, distressing dreams, disturbed sleep, irritability, startle response, memory problems, and multiple somatic symptoms. Whereas Erichsen believed in an organic damage of the spinal cord, the London surgeon Page argued in 1885 that not physical injuries but fright, fear, and alarm caused the disorder he called “nervous shock.” From that moment on, an important shift in thinking about the consequences of trauma started (DiMauro et al., 2014; Kinzie & Goetz, 1996).
In the 1880s, the famous Parisian professor in neurology Charcot investigated patients with hysteria. Remarkably, he did not associate hysterical symptoms with traumatic events in his female patients, while he did in his male patients with serious accidents at work. These men were suffering from what he called “traumatic hysteria,” which encompassed a great variety of symptoms. First, there were aberrations of sensibility, especially anesthesia and hyperesthesia, and visual disturbances like double vision or even blindness. Second, patients exhibited neurological motor symptoms, like paralyses and spasms. Third, Charcot described a wide range of other symptoms, like chest palpitations, chest pain, dizziness, and language disorders such as stuttering and mutism (Ellis, 1984; Micale, 1990).
In Berlin, one of the leading German neurologists Oppenheim also worked with work-related psychic complaints and he was the first to formulate the notion of a syndrome called “traumatic neurosis” in 1888. Since Oppenheim wanted to equate somatic and mental disorders after major accidents in the context of German insurance procedures, he emphasized, much more than Charcot, that the traumatic experiences are the “real cause” of the disorder. To his opinion, the magnitude of the fear during the traumatic event resulted in microscopic brain damage with symptoms developing from an often initial paralysis to a more long-lasting change in mental functions. Oppenheim located the disorder somewhat between hysteria and neurasthenia, with next to shaking, paralyses, and disturbances in sight, also melancholic mood, fear, irritability, palpitations, pressure on the breast, and insomnia (Holdorff, 2011; Schmiedebach, 1999).
In short, this period was characterized by profound social and industrial changes, with many casualties of accidents, resulting in loss of labor and increasing financial support legislation for the injured. These societal developments urged clinicians to develop clear definitions of medical consequences of traumatic events. In this way, partly under societal pressure, clinicians increasingly worked in a complex medical, social, political, legal, and moral context that fueled heated academic disputes over symptoms, diagnoses, and causes (Gersons & Carlier, 1992; Weisaeth, 2002). In particular, in Germany, several prominent neuropsychiatrists heavily disputed Oppenheim’s “traumatic neurosis,” and proposed to abolish the concept. In 1890, at an international meeting in Berlin, they stressed the role of simulation and social causes such as civilization and the German accident insurance legislation. In addition to simulation, the diagnosis of hysteria was brought to the fore, which would not be specifically caused by the (external) traumatic experiences themselves, but rather by (internal) imaginative desires and constitutional dispositions (Holdorff, 2011; Lerner, 2003).
In 1891, also The Lancet seriously questioned the concept of “traumatic neurosis” because it tended to contain far too many symptoms and causes, including signs of simulation, malingering, organic nerve injury, hysteria, shock of the cerebrospinal system, neurasthenia, and psychosis (Rollin, 1990).
Psychotrauma in War and Combat
Before World War I
Already in ancient times, reports were made about psychic symptoms following combat. Descriptions were made of grief, guilt, numbness, anger, intrusions, nightmares, dissociation, and somatic symptoms (see, e.g., Ben-Ezra, 2011; Birmes et al., 2003, 2010; Ellis, 1984).
Until well into the 19th century, the relationship between traumatic combat experiences and psychological complaints was rarely recognized in scientific literature (Kinzie & Goetz, 1996; Kloocke et al., 2005): if a soldier had a mental breakdown, this was interpreted as a suffering from circumstances like heat, homesickness, heavy packs, or pinching belts (Jones & Wessely, 2001; Rosen, 1975). An exception was Pinel, a French physician and pioneer of early psychiatry, who around 1798 was one of the first to specifically associate mental symptoms with terrifying wartime experiences and coined the term “cardiorespiratory neurosis” (Crocq & Crocq, 2000).
In the Crimean War (1854–1856), Handfield Jones described “Crimean fever” which was characterized by pains in the limbs, irritable heart, agitation, and exhaustion. Shortly thereafter, in the American Civil War (1861–1865), cardiac disorders became the most prominent sign among soldiers, described by military physicians like Hawthorne, Maclean, Myers, and Da Costa. The disease was named “soldiers heart” or “irritable heart syndrome,” and encompassed rapid and feeble pulse, palpitations, chest pain, shortness of breath, and extreme fatigue. Other symptoms were disturbed sleep with unpleasant dreams, melancholy, and gastrointestinal symptoms (Jones & Wessely, 2001; Kinzie & Goetz, 1996; Ray, 2008). Some years later, during and after the Russian–Japanese war (1904–1905), the German physician Honigmann was in 1907 probably the first to coin the term “Kriegsneurose” (“war neurosis”) and depicted the similarities between traumatized soldiers and Oppenheim’s traumatized civilians (Crocq & Crocq, 2000).
Concluding, from ancient days on, several war-related symptoms were described. Especially, in the 19th century, clinical emphasis became more and more on physical symptoms like heart disease, general weakness, gastrointestinal symptoms, and exhaustion. This probably was due to a major paradigm shift: around 1869, the new concept of “neurasthenia” (described as enfeeblement of the nervous system without organic lesion) obtained a dominant position in psychiatry. This meant an important change in psychiatric nosology resulting in a time-bound mechanical view on stress and psychopathology. The term “war neurasthenia” became popular as a catch-all for unexplained symptoms in soldiers with no apparent physical injuries (Bogacz, 1989; DiMauro et al., 2014).
World War I: Not Just Shell Shock
During World War I (WWI; 1914–1918) the “irritable heart syndrome” remained widespread, together with other concepts like “war neurasthenia” and “traumatic hysteria.” However, WWI was above all the war of “shell shock,” a term introduced by Myers (1915). “Shell shock” was originally seen as a form of commotio cerebri that was a result of powerful compressive forces but soon it also became related to frightening experiences like horrible sights and the fright of being buried alive (Wiltshire, 1916). Soldiers, often coming directly from the battle fields and trenches, were described as suffering from neurological symptoms like tremors and paralyses, neurasthenic symptoms, and symptoms of anxiety. When it became clear that enormous numbers of soldiers were suffering from “shell shock,” and hence were being discharged from service, authorities tried to restrict and discourage the use of the term, or even tried to abolish it. This lead to remarkable new alternative diagnoses, like “malingering,” “pension wish neurosis,” and “not yet diagnosed—nervous.” And even very cruel treatment methods were used by army doctors, such as painful electrical treatments as an aversive therapy that caused the men to return to the front (Freud, 1955; Jones et al., 2007; Mosse, 2000; Weisaeth, 2002).
While in Germany Oppenheim again began to defend the concept of “traumatic neurosis” at the start of WWI, again important scholars especially the influential German psychiatrist Bonhoeffer vehemently opposed his view. Ultimately, Oppenheim’s concept was rejected for the second time, at the 1916 War Conference in Munich. Central theme in the dispute was whether the cause of the disorder was psychological or physical. The leading opinion among a significant part of the experts was that without physical lesions, weakness, a deficiency of will-power, and simulation were the principal reasons for patients to present this “social disease” (Bonhoeffer, 1926; Lerner, 2003). Interestingly, in the period after the war, a new generation of German psychiatrists embraced the concept again, in order to better understand their traumatized patients (Holdorff, 2011; Kloocke et al., 2005; Schmiedebach, 1999). And also, the Viennese psychoanalyst Freud wrote about war neurosis after the war, as early as 1919. He believed that simulation was rare, and he observed how traumatized patients acted as if they were in the traumatic situation again (Freud, 1955). Many decades after WWI, the complaints of many traumatized veterans continued, as American psychiatrist and psychoanalyst Kardiner described in his important book “The Traumatic Neuroses of War” (Kardiner, 1941). He described long-lasting symptoms, which later influenced the definition of trauma-related disorders in the 1952 and 1980 DSM editions.
In sum, in many countries, causes, symptoms, and even the existence of psychological consequences of war were discussed heavily. Just as was the case in the context of the industrial revolution, also here the enormous societal pressure influenced the professional debates. In both cases there was fear of costs for financial compensation and fear for lack of manpower. Holdorff (2011, p. 472) described the problematic aspects of these dynamics: “Under the pressure of political, military and conceptual circumstances, physicians bent medical ethics and departed from their traditional individual focus in favour of new social ethics and political commitments.”
World War II: Combat-Related Trauma
To avoid another epidemic of “shell shock” once World War II (WWII; 1939–1945) started, British authorities again tried to ban the term as a preventive measure. Still, already at the beginning of the war, discussions about post-combat syndromes came ahead. The general opinion was that only those with a pre-combat constitutional vulnerability would not recover naturally once removed from danger (DiMauro et al., 2014; Jones & Wessely, 2007). This opinion grew problematic since many soldiers of both sides of the war developed long-lasting symptoms similar to those described in WWI: physical symptoms like tremor, fatigue, gastrointestinal problems, poor memory, and also psychological symptoms like anxiety, nightmares, irritability, and startle reactions (Engelbrecht et al., 2018; Jones et al., 2007; Kloocke et al., 2005).
Studies conducted directly in and after WWII are scarce. Grinker and Spiegel (1945) identified anxiety as a core symptom next to several other mental complaints in soldiers in Northern Africa in 1943. Swank (1949) distinguished four groups of symptoms in a sample of WWII soldiers: emotional, cognitive, physical, and hysterical symptoms. Also, research on the long-term consequences of WWII combat is sparse. Prominent exceptions are the two studies of veterans in the 1960s, reporting many symptoms later defined in PTSD (Archibald et al., 1962; Archibald & Tuddenham, 1965).
Despite the limited research, these studies significantly influenced the definition of later PTSD, with findings of the chronic nature of post-combat symptoms and that even soldiers without a pre-war vulnerability could develop chronic symptoms (Archibald & Tuddenham, 1965; Swank, 1949).
World War II: The Consequences of the Concentration Camps
After WWII, the deeply intrusive and far-reaching psychological consequences in victims of the Nazi concentration camps were studied. Especially in the Netherlands, several physicians and camp survivors themselves, like Tas, De Wind, and Cohen (see De Wind, 1972; Cohen, 1981) but also Thygesen from Denmark, published their experiences and observations shortly after the war. Friedman (1949) was probably the first to publish a scientific paper about camp survivors. But on the whole, not until many years later, several important clinicians and researchers in the field followed. Those were among others, Hermann and Thygesen (1954) in Danmark, Bastiaans (1957) in the Netherlands, Eitinger (1961) in Norway, Von Baeyer et al. (1964), Venzlaff, and Lederer (mid 1960s) in Germany, and Krystal and Niederland (1968) in the US. Early research was hampered by societal influences such as an emphasis on civilian reconstruction and a lack of understanding of the camp survivors’ extreme experiences. And here too controversies arose about the origins of complaints. Next to psychological theories, several authors pointed out a relation between complaints and brain damage caused by injury, illness, and extreme starvation in the camps (e.g., Eitinger, 1961; Venzlaff, 1964).
Even though most of the mentioned authors described case observations, the degree of agreement on symptoms was remarkably high. They defined the “post concentration camp syndrome” or “survivor syndrome” as a different syndrome compared to the classical “traumatic neurosis.” For instance, Bastiaans (1957) described the syndrome as more complex, with chronic over-activity, aggression, despair, psychosomatic complaints, and a permanent blockage of human relations. Niederland (1968, p. 313) stated: “The concept of traumatic neuroses does not appear to cover the multitude and severity of clinical manifestations of the survivor syndrome.” Therefore, Niederland wanted to sharpen the distinction between the two disorders to indicate that this type of traumatization is of such magnitude, severity, and duration that a recognizable clinical entity must be defined. Based on clinical observations of close to 2000 survivors of Nazi concentration camps, he described the “survivor syndrome” in seven symptom clusters, namely, symptoms regarding anxiety, cognition and memory, depression, psychosis/dissociation, personal identity, psychosomatic conditions, and apathy (Niederland, 1968, 1981).
Concluding, in case of the extreme and long-lasting, dehumanizing traumatization of victims of the Nazi concentration camps, there was the need to define a syndrome with a more extensive and complex symptom constellation next to the already existing “traumatic neurosis.” This was a completely new development in trauma diagnostics: a split was made in which not one but two trauma syndromes were found necessary.
Disaster-Related Trauma
Already in the ancient world there were reports of emotional reactions due to suffering (Birmes et al., 2010; Kinzie & Goetz, 1996). Much later are the well documented descriptions concerning the “Great Fire of London” in 1666 by the two famous diarists Evelyn and Pepys. Evelyn observed an acute reaction, described as a state of shocked inertia and passivity (Parry-Jones & Parry-Jones, 1994), whereas Pepys reported about complaints until 5 months after the fire, especially symptoms of re-experiencing and sleeping difficulties (Daly, 1983). In 1765, Ignazio Somis reported extensively about victims of a large snow avalanche disaster in the Italian Alps. He also described an acute, transient stress response for some days with immediate loss of senses, fright, and faint and besides a longer lasting reaction which pursued for years, with nightmares, daily intrusions, avoidance behavior, and autonomic hyperarousal (Parry-Jones & Parry-Jones, 1994).
From the beginning of the twentieth century onwards, several disaster-related studies were conducted (see, e.g., Norris et al., 2002; Weisaeth, 2002). The Swiss physician Stierlin (1911) systematically studied the reactions of survivors after the Courrières mine (1906) and the Messina earthquake (1908) disasters. Remarkably, he again described the two different mental reactions: an acute and transient reaction usually lasting for some days with clouded consciousness, disorientation, and fearful affect and another of longer duration that included loss of energy, sleep disturbances, and nightmares. Important other studies were on victims of the 1906 earthquake in San Francisco by James (1911) and victims of ship explosions by Hesnard (1914). Adler (1943) described the disastrous fire of the Coconut Grove nightclub in Boston, with a variety of symptoms like irritability, fatigue, insomnia, fears and nightmares, hostility, avoidance, and physical symptoms.
In the 1970s, various studies on the effects of the 1972 Buffalo Creek flood disaster gave increased attention to disaster research. Importantly, in these studies, next to the previously described “acute and transient reaction” and the “reaction of longer duration,” a third kind of post-disaster syndrome was mentioned. This “Buffalo Creek syndrome,” described as “long-term character changes” or “post-traumatic decline,” encompassed symptoms of over-control and rigidity, social isolation, hostility, feelings of helplessness, and demoralization (Lindy & Titchener, 1983; Titchener & Kapp, 1976).
In sum, disaster researchers delivered thought-provoking findings. Even three types of post-disaster psychological disorders emerged. First, an acute and transient reaction to the sudden threat was described, second, a condition of a longer duration, and third, a more far-reaching and severe syndrome with even characterological changes. The latest observations in particular showed important similarities with findings from the field of concentration camp survivors, although it is remarkable that the disaster studies hardly made any reference to this.
Domestic and Sexual Trauma
While Charcot had no regard for traumatic events as an origin of hysteria in women, in later years, the relation between hysteria and adverse, often sexual, life events in childhood became more recognized. It was Janet who introduced a new way of looking at this relationship. From 1886 onwards, he explored and described extensively the role that dissociation played in unresolved traumatic memories (Birmes et al., 2003; Van der Hart & Horst, 1989). In the same period, Freud wrote in “About the aetiology of hysteria” (1896) that sexual experiences in early childhood were the basis for the development of many psychic symptoms in later life. But while Janet stuck to his vision of sexual trauma, Freud soon left his theory about the importance of early childhood sexual experiences (Van der Kolk & Van der Hart, 1989).
Gradually, the attention on sexual trauma decreased. One reason for this was the dominant position within psychology and psychiatry of Freud’s psychoanalysis, which had strayed from sexual trauma. Furthermore, in contrast to events such as wars or natural disasters that disrupt society, domestic violence could more easily remain invisible and hidden for long periods of time (DiMauro et al., 2014). Around the 1970s, a revival arose, largely because of the influence of the female rights movement. Several influential papers dealing with domestic and sexual violence were published. Burgess and Holmstrom (1974) paved the way for the later PTSD in DSM-III by describing the “rape trauma syndrome,” with re-experiencing symptoms, avoidance, high startle responses, triggers related to the events, but also a damaged sense of safety, suicidality, and severe problems in relationships. In another syndrome, the so-called “battered women syndrome,” particular attention was paid to the mechanism of learned helplessness (Gayford, 1975; Walker, 1977).
So after an initial focus on, and then a long pause in thinking about sexual and domestic violence, a new important development came to the fore from the 1970s onwards. Again, driven by an influential citizen movement and prominent clinical advocates, severe symptom constellations emerged, some of which were not covered by existing diagnostic categories. The influence of these researchers had a significant impact: eventually their findings led to new, highly influential complex trauma concepts.
Psychotrauma and the DSM and ICD Classifications
DSM-I, DSM-II, and the Prelude to PTSD
The Run-Up to the DSM
After mid-19th century, German was the international language in psychiatry and German-speaking physicians dominated the classification of mental disorders. The most influential of them was Kraepelin, professor of psychiatry in Heidelberg. In the highly influential eighth edition of his textbook (published between 1909 and 1915), he described a classification of psychiatric syndromes based on observed clinical and not biological grounds. Several developments made an end to the rich German diagnostic traditions. First, World War II ended German influence as the international language of science, including psychiatry. The initiative shifted to the US, where there was practically no tradition in psychiatric classification. Second, because of their wartime experiences, many American physicians especially had experience with patient groups that differed greatly from those of their German colleagues, namely, non-institutionalized and non-psychotic patients. And third, psychoanalysis was on the rise in post-war psychiatry, partly because of the need to focus on this relatively new patient group. This too was an important development, because psychoanalysis, in general, was not very concerned with classification (Grob, 1991; Shorter, 2022).
The Road to PTSD in DSM-III
In October 1945, a committee under the supervision of the US psychiatrist Menninger, who was a general in WWII, launched the “Medical 203 Bulletin,” which consisted of a nosology largely based on psychodynamic principles and can be considered the predecessor of the DSM-I. In 1952, the American Psychiatric Association (APA) took the initiative and launched the first edition of the DSM. This DSM-I introduced a new stress and trauma-related syndrome called “gross stress reaction” (GSR), based on the work of among others Grinker, Spiegel, and Kardiner who also worked in the military during WWII. The disorder represented a transient overwhelming fear response to an extreme external stressor in a person without previous mental problems. The reaction should disappear after the person no longer was exposed to the stressful situation. This definition was in line with older theories and suggested that long-lasting conditions could only occur in the presence of predisposing mental disorders. In the DSM-II (1968), GSR was replaced by “transient situational disturbances” which was not a specific trauma-related category at all. As a result, DSM-II missed a specific trauma-related disorder. It has been suggested that the lack of such a disorder was due to the fact that none of the APA committee members had experience with combat-related disorders (Scott, 1990).
At that time, the Vietnam War had already started for the US but the most serious consequences of this war became more visible to American society in the 1970s, including with the marches of the “Vietnam Veterans against the War,” immense numbers of veterans that were in need for psychosocial help, a shifting public opinion about the war, and influential psychiatrists such as Lifton and Shatan vehemently opposed to the war. These developments led to what Shatan (1973) and later Friedman (1981) defined as the “post-Vietnam syndrome”: a delayed and long-lasting trauma syndrome, with grief and guilt-related symptoms, rage, numbing, alienation, intrusive nightmares, drug dependence, depression, and anxiety.
Remarkably, in the early development of the DSM-III around 1974 again no trauma-related diagnosis was planned. Some US-research groups argued heavily that existing diagnoses covered the symptoms of traumatized Vietnam veterans adequately. But Shatan, Lifton, and others had set up a working group to vigorously oppose this view. WWII experts Niederland and Krystal joined, as well as among others the stress-expert Horowitz and the US professors in psychiatry and DSM-III task force members Andreasen and Spitzer. The merger of these specialists broadened the scope to all kinds of traumatic events. Together they formed a strong and successful lobby and eventually defined a new syndrome which they termed “catastrophic stress disorder” or “CSD” (Scott, 1990).
The development of this new disorder had noteworthy similarities with the mechanisms earlier clinicians were faced with in trying to describe the mental consequences of catastrophic events: social pressure and unrest, lobbying by (politically) engaged clinicians and patients, and a need to acknowledge the overwhelming suffering after horrific experiences ensured that a new diagnosis appropriate for the time was created. And here too, opposing forces emerged that saw no benefit in the newly made diagnosis. It looked like a repeat of earlier described motions: the oscillation between the denial of the existence of a psychotrauma syndrome and the strong forces to name and define such a syndrome.
A New Syndrome: PTSD
In 1978, it was decided that the symptom profile of “CSD” would be included in the DSM-III (APA, 1980), under the name of “PTSD.” The new syndrome was supposed to give more clarity for clinicians, researchers, as well as patients. In addition to the experimental research of Horowitz (1976) in particular, research into the diagnostic criteria of PTSD was largely based on only a limited number of studies. Besides, the diagnosis was strongly promoted by a community-driven group of psychiatrists and veterans who worked together to place the diagnosis in the DSM-III. The latter two points have led some scholars to argue that the introduction of PTSD was largely the result of strong lobbying efforts, particularly motivated by societal forces (Jones & Wessely, 2007; Scott, 1990; Turnbull, 1998). In general, however, it can be said that both medical, psychological, and societal influences converged at a time when there was an urgency to understand (and treat) the suffering of individuals. However, these developments have made PTSD an objectively created reality for many professionals, rather than being seen as a construct from a diversity of time-bound perspectives (Frueh et al., 2010).
The definitions of PTSD from DSM-III to DSM-IV (APA, 1994) were largely the same. In essence, the criteria were grouped in symptom clusters of, respectively, re-experiencing, avoidance, and hyperarousal. As a whole, the grouping of criteria in these three symptom clusters narrowed the definition of PTSD in a significant way: PTSD lost several symptoms seen in earlier literature, like interpersonal problems, personality features, and especially physical symptoms. In particular, the somatic symptoms were subsumed under non-trauma-related disorders, such as somatization disorders and conversion disorder.
In the DSM-IV, a new diagnosis was introduced, the “acute stress disorder” (“ASD”): an acute and temporary condition with dissociative symptoms, and symptoms of re-experiencing, fright, and hyperarousal (APA, 1994). Whereas acute mental reactions after psychotrauma are described throughout history, especially after sudden, overwhelming events like disasters, shortly after its introduction the disorder was already criticized because it might medicalize a normal transient reaction, and because of the limited value to predict PTSD (Marshall et al., 1999).
The World Health Organization (WHO) introduced a section of mental disorders for the first time in the ICD-6 (1948), with a trauma-related disorder called “Acute situational maladjustment” including a “combat fatigue” subtype. The ICD-8 (1967) and ICD-9 (1978) of the World Health Organization were very similar to the DSM-II of the American Psychiatric Association. But when DSM-III was launched in 1980, a radically new classification was created which had little connection with the ICD-system anymore. Within ICD-9, a coding scheme was developed for DSM-III categories, but ICD-10, published in 1993, had its very own section for mental disorders (WHO, 1993). Although this section still was more or less compatible with the DSM, it was not the same, and as a result, from this point on, an important development was set in motion where the two major diagnostic classification systems went their separate ways (Peters et al., 1999).
Thanks to all these developments, after the introduction of PTSD in 1980, the field of psychotrauma has flourished. The number of scientific publications on PTSD has increased considerably over the years, several journals have emerged that focus purely on trauma, and various associations have been founded, such as the International Society for Traumatic Stress Studies (ISTSS) in 1985 and the Division56 of the American Psychological Association (APA) in 2006.
After PTSD: Heterogeneity and Complexity Revisited
Despite the desire to unify the psychotrauma field, fundamental criticism persisted after the introduction of PTSD in 1980. Among others, the overlap and similarities with other diagnoses was in debate, but also the way PTSD was defined. In particular, several authors again missed numerous symptoms especially in complex traumatized patients and made several suggestions to overcome the identified shortcomings. For instance, it was suggested to look beyond classification and better define PTSD as a spectrum disorder, defined with core PTSD-symptoms like re-experiencing, and besides numerous heterogeneous symptoms that especially could be identified in severely traumatized patients (Ciccone et al., 1988; Kolb, 1989; Lerer, 1988). Nevertheless, strict diagnostic categorization continued to be preferred, as many authors attempted to re-formulate novel syndromes after prolonged and severe suffering like, for example, “Posttraumatic Character Disorder” (Horowitz, 1986), “Post-Traumatic Self-Disorder” (Brende, 1983; Parson, 1984), “Malignant Post-Vietnam Stress Syndrome” (Rosenheck, 1985), “Post-Combat Survivor Syndrome” (Goderez, 1987), and “Post-Traumatic Demoralization Syndrome” (Parson, 1990) (Table 1). Most of these syndromes were based on observations in Vietnam veterans and included symptoms like pronounced identity and personality changes, social isolation, self-destructive and violent behavior, affective instability, guilt, shame, suicidality, and use of drugs and alcohol.
A similar development was visible in another psychotrauma field. The attention for especially early childhood sexual abuse grew in the 1980s. Several authors reported high incidences of physical and sexual violence among psychiatric patients and described trauma-related symptoms like depression, anxiety, self-destructive behavior, poor self-esteem, substance abuse, and a tendency towards revictimization (e.g., Bryer et al., 1987; Herman et al., 1986; Terr, 1991). Soon thereafter, Herman (1992) introduced a new syndrome named “Disorders of extreme stress, not otherwise specified” (“DESNOS”), also called “complex PTSD.” “DESNOS” was supposed to be associated with severe and repeated interpersonal abuse and consisted of a wide variety of symptoms, classified into clusters such as alterations in regulation of affect and impulses, consciousness, self-perception, relations with others, somatic symptoms, and systems of meaning (Herman, 1992; Luxenberg et al., 2001).
The new syndrome was investigated in field trails (Van der Kolk et al., 2005) and, for instance, in studies with patients with repeated interpersonal traumatization (Roth et al., 1997; Zlotnick et al., 1996) and in combat veterans (Jongedijk et al., 1996; Newman et al., 1995). Despite research efforts and, also here, lobbying by dedicated clinicians, “DESNOS” was not officially adopted as a distinct disorder in DSM-IV. This was mainly due to the limited amount of research available at the time, concerns about the clinical utility of the very broad and mixed symptom profile, and its problematic distinction from other disorders, especially the Borderline Personality Disorder (Luxenberg et al., 2001). Despite this, “complex PTSD” gained widespread following among clinicians as well as patients (Veissière, 2021). Both felt recognized that the consequences of severe, long-term events went beyond what they believed to be limiting symptoms of PTSD.
Unlike DSM-IV, the ICD-10 did included a trauma category associated with the concept of “DESNOS.” The disorder was called “Enduring personality change after catastrophic experiences” or “EPCACE” (WHO, 1993). The first drafts of “EPCACE” were already made around 1985 by the Norwegian WWII expert Eitinger (Malt et al., 1996). Symptoms of “EPCACE” included pervasive hostility, mistrust, social withdrawal, feelings of emptiness, chronically vigilance, and estrangement. In a review of expert’s opinions, the features “hostility” and “mistrust” were ranked as most important symptoms (Beltran et al., 2008). The precipitating stress should be of an extreme nature in order to plausibly account for the observed personality change, irrespective of the person’s prior level of adaptation (WHO, 1993). “EPCACE” was not supported by robust research, resulting in a weak empirical basis. Moreover, some experts pointed at the lack of specificity of its criteria and the potential overlap with other mental disorders (Beltran & Silove, 1999). These concerns parallel the concerns about “DESNOS.”
In short, as described in previous periods, a diagnostic gap in trauma diagnosis was also found here: heterogeneous symptoms after especially enduring, far-reaching traumatic experiences were not covered by the existing disorder PTSD. Whereas most of the described syndrome names did not caught hold, the urge to fill the gap more sustainably became more and more prominent and influenced the development of recent concepts radically.
Most Recent Developments: DSM-5 and ICD-11
In the run-up to the DSM-5, there was again discussion about the PTSD concept. Challenging paper titles like “PTSD: a problematic category” (McHugh & Treisman, 2007) or “Saving PTSD from itself in DSM-V” (Spitzer et al., 2007) showed the dispute with regard to core assumptions, hypothesized mechanisms, validity, and clinical utility of PTSD.
Finally, PTSD entered the DSM-5 with rigorous changes (APA, 2013). Called as “the changed face of PTSD” (Schnurr, 2013), the disorder no longer was classified as an anxiety disorder but was included in a new chapter of disorders related to stressful events. This change was supposed to reflect the recognition that not all traumatizing events are threat-based and posttraumatic stress not always includes fear as the hallmark emotion (Friedman, 2013). Furthermore, the symptom clusters were extended from 3 to 4, and included 20 separate symptoms (17 in DSM-IV). In a new cluster termed “negative cognitions and mood,” existing PTSD symptoms were accommodated but also new symptoms were added like, for example, persistent distorted blame of self or others, horror, guilt, shame, and self-destructive behavior. Furthermore, a dissociative subtype for PTSD was distinguished, with depersonalization and derealization symptoms. Accordingly, the DSM-5 characterized a broad scope of post-traumatic responses, with many heterogeneous symptoms besides anxiety-related responses.
The broadened PTSD concept was criticized by several authors. PTSD underwent more changes than any other mental disorder (Hoge et al., 2016) and was the disorder with the most extensive number of criteria in DSM-5, with 636.120 ways to have PTSD (Galatzer-Levy & Bryant, 2013). Whereas at the time it was decided not to include DESNOS or complex PTSD in DSM-IV, critics argued that in DSM-5 PTSD became rather “DESNOSish” because of the breadth and variety of symptoms (Maercker & Perkonigg, 2013). On the other hand, it was claimed that adding relevant symptoms would encourage clinicians and researchers to assess them, treat them, and include them in research (Kilpatrick, 2013).
In contrast, the ICD-11 went the reverse way, defining PTSD in ICD-11 by a much smaller set of symptoms (WHO, 2018). PTSD requires the presence of three symptom clusters: re-experiencing, avoidance, and perceptions of heightened current threat. The members of the ICD-11 working group wanted to express the essential features of PTSD and agreed that re-experiencing trauma together with active avoidance and heightened sense of threat appeared to be the distinct factors of the disorder (Brewin, 2013). In addition, they emphasized the need for accessibility and thus easy applicability in non-English speaking countries with minimal resources, so that identification of people at risk will lead to more effective use of health services (WHO, 2018).
Interestingly, in the ICD-11, the definition of the trauma criterion was defined more globally and less strictly, which certainly has its advantages. After all, this decision equates PTSD with the other diagnostic categories in the DSM, most of which have no etiological factor in their criteria (Jongedijk et al., 2022). In addition, research showed that individuals who have experienced stressors that do not meet the trauma criterion according to the DSM may also develop PTSD (Robinson & Larson, 2010). However, the decision of the ICD-11 may have far-reaching conceptual consequences. By easing the trauma criterion, the legitimacy of PTSD as a unique diagnosis after traumatic experiences is undermined. After all, there are many similarities between PTSD symptoms and symptoms of other disorders (Spitzer et al., 2007).
Because the narrow PTSD definition in ICD-11 was considered not to cover the full range of clinical symptoms in patients with a history of long-term interpersonal traumatization, the ICD-11 introduced a new “complex PTSD” category. In addition to the PTSD criteria, individuals with “complex PTSD” must meet three additional symptom clusters: pervasive affective dysregulation, persistent negative self-concept, and persistent difficulties in sustaining relationships and in feeling close to others (WHO, 2018). “Complex PTSD” defined in this way is less elaborate than “DESNOS,” more precisely defined compared to “EPCACE,” and with better distinction compared to personality disorders (Cloitre et al., 2014).
All in all, this means that there are significant differences between the two leading diagnostic classification systems: there are two definitions of PTSD and furthermore “complex PTSD” is not included in DSM-5 while it is in ICD-11. Besides, “ASD” is included in DSM-5 but not in ICD-11. But above all, the confusion of the two different definitions of PTSD is quite problematic due to possible differences in prevalence rates in studies and the fact that the two diagnostic systems tend to identify different individuals (Bryant, 2019). This situation may have disadvantageous effects in, for example, comparing research findings across studies, or in comparing the burden of trauma between countries that use different diagnostic systems (Schnurr, 2013). For patients and clinicians, it may have the confusing consequence that choosing one system or another will have different impact on thresholds for treatment or for specific treatment options, but also on the assignment of pensions and insurance coverage (Carvajal, 2018; Hoge et al., 2016). Despite these negative consequences, it also offers scientific opportunities to search for new questions about defining the condition more precisely and to stimulate better diagnostic constructs (Carvajal, 2018; Schnurr, 2013).
Discussion and Challenges for the Future
Common Threads Throughout History
In this extensive historical literature review, we pointed out recurring dilemmas and pitfalls in the field of psychotrauma. Our central questions were how did posttraumatic symptoms and syndromes evolve and change over time, what are the causes of these changes, and why are scientists and clinicians still unable to create unity?
Posttraumatic Symptoms and Syndromes Classified.
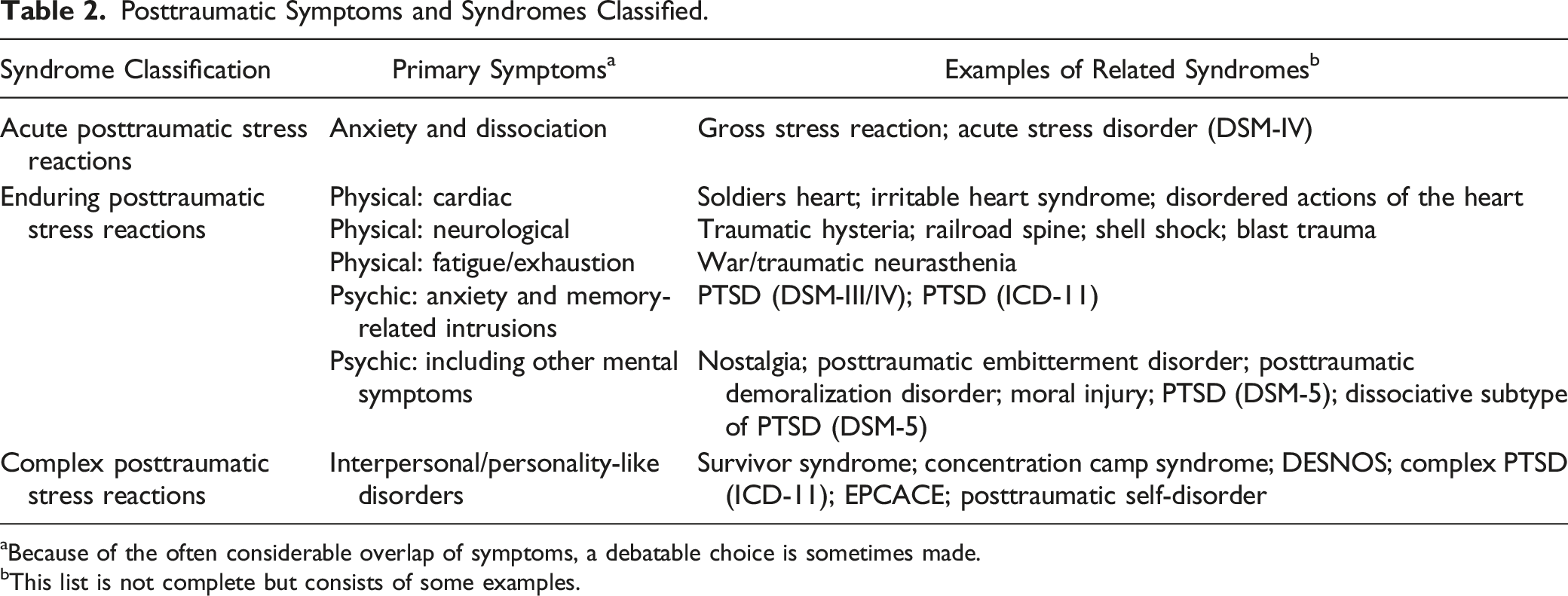
aBecause of the often considerable overlap of symptoms, a debatable choice is sometimes made.
bThis list is not complete but consists of some examples.
Symptoms and Syndromes: They Come and Go
Over time, the described symptoms have changed significantly, and there was a great variation in the descriptions of trauma-related reactions. An important observation in this review is that a wide range of physical symptoms was described in great detail in almost every era, with symptoms of fatigue or heart diseases in some eras, and neurological signs or gastrointestinal complaints in others (Table 2). It is remarkable that most of these symptoms were not included in the original PTSD-criteria and got little attention thereafter.
Related to this, there has been much discussion in recent decades about whether psychological or physical factors play a role in psychotrauma complaints. These discussions took place, for example, with the train accidents and certainly with Oppenheim’s traumatic neurosis. But also after the Second World War, when psychosomatic theories emerged and connections were made between living conditions, stress, and physical illnesses (Bastiaans, 1957; Weiss & English, 1943). The discussion between soma and psyche continues to this day, for example, with the concepts of “blast trauma” and brain injury (Greer et al., 2018) resembling the earlier “shell shock” discussions or with the recently re-cited old concept of the “soldier’s heart” and cardiological phenomena (Borges et al., 2020).
Whereas symptoms such as reliving the traumatic event were certainly reported throughout history, after the introduction of PTSD, memory-based theories dominated the psychotrauma literature. Symptoms that did not fit in here disappeared into the background, but later found a place again, albeit less prominently in, for example, DSM-5s PTSD and ICDs complex PTSD. Looking at a syndrome level, many syndrome names have been put forth as listed in Table 1. However, we did find a reasonable agreement in history about three syndromes to be classified. First, there is an acute syndrome of short duration, with intense fear, horror, and dissociative symptoms. Second, a syndrome with symptoms enduring for months until years, including various somatic symptoms, anxiety, reliving, hyperarousal, but also dissociation, and grief and mood symptoms. And third, a more complex symptom constellation was delineated, with features resembling personality changes. In essence, this classification into three forms of disorders is to some extent similar to current diagnostic entities called “ASD,” “PTSD,” and “complex PTSD,” respectively. However, it is important to note that there are significant differences in the various reported symptom constellations. In other words, despite the global similarities at syndrome level, the symptoms associated with the three distinct syndrome types varied considerably throughout history and were always subject to change over time. This means that concepts as “soldiers heart,” “shell shock,” “traumatic neurosis,” DSM-5s PTSD, or ICD-11s PTSD are defined differently and are not the same disorders (Table 2).
PTSD: A Time-Bound Disorder?
In the controversy about PTSD as a validated diagnostic concept, contrasting points of view can be distinguished. These opposing views may explain many of the depicted disagreements about PTSD. One view is that PTSD is a clearly scientifically proven universal and timeless psychobiological response to overwhelming traumatic stress. This is a frequent point of view in modern, especially western psychotraumatology (as described in, for example, Bracken, 2001; Figueira et al., 2007; McNally, 2004). In contrast, others criticized the PTSD concept, and question the scientific basis and even the raison d'être of PTSD (e.g., McHugh & Treisman, 2007; Rosen & Frueh, 2007; Rosen & Lilienfeld, 2008). In order to explain these differing viewpoints, important thoughts and analyses have been presented, especially from a historical perspective, on how PTSD is defined. These stem from, for instance, historians themselves (e.g., Shepard, 2004), anthropologists (e.g., Young, 1995), philosophers (e.g., Hacking, 1994; Leys, 2010), sociologists (e.g., Horwitz, 2018), and psychologists and psychiatrists (e.g., Bracken, 2001; McNally, 2004; Summerfield, 2001). In this section, we will limit ourselves to some key mechanisms that could explain the recurring diagnostic problems in trauma-related concepts.
In addition to the opposing views of PTSD as a universal, psychobiological, and timeless disorder versus a culture-bound, socially constructed one, a third option has been described: time-bound social contexts have a decisive influence on the manifestations of PTSD in an interactive way. In other words, reported symptoms are influenced by the classification process itself. In this way, symptoms become part of reality as both clinicians and patients shape them accordingly, as an interaction between psychobiology and socio-cultural contexts (Hacking, 1999; McNally, 2004).
Any particular period will have a predominant idea of what is considered a real disease. Presentations of especially mental illness vary during various time periods and draw on what Shorter (1993) called the “symptom pool.” This term refers to how symptoms are represented in the culture’s collective memory as belonging to a real illness. Symptoms of the symptom pool have been known throughout the ages, but their appearance fluctuates in frequency at different times. In some periods of history, certain symptoms are drawn from the pool, while in other periods, they are barely visible. How these fluctuations come about has to do with what is considered legitimate symptoms for disease at any given time. Subsequently, experts and doctors will shape manifestations of diseases according to current medical knowledge and under the influence of the existing socio-cultural paradigm. Patients follow, as they will present legitimate symptoms associated with an expert-diagnosed disease. This mechanism of culturally shaped symptom pools could explain the changes in posttraumatic symptoms over time (Horwitz, 2018).
For instance, in the century of the industrial revolution, a widely accepted mechanistic mindset caused scientists, clinicians, as well as patients to form symptoms that fit into the prevailing frame of reference. At that time, for example, symptoms of the heart were widely accepted (“irritable heart syndrome”). A little later, the same applied to fatigue complaints and exhaustion of the nerves (“neurasthenia”). From a mechanistic paradigm prevailing at the time, the pathogenic mechanism of “neurasthenia” was believed to stem from a failing defence barrier of the brain to excessive external stimuli. The origins of the current PTSD-concept, however, are related to the emerging psychologization and individualization of western 20th century societies. Compassionate humanity towards those affected received more attention than before and subsequently received a prominent place in the PTSD concept: there was an explicit cause without personal weakness. But above all, psychological theories reflecting internal mental processes were applied to the PTSD concept, with symptoms explicitly connected to the “traumatic event” (the etiology) and the “traumatic memory” (the pathogenic mechanism) (Bracken, 2001; Frankel, 1994; Young, 2004, 2016).
The principles of the “symptom pool” can be further substantiated when one considers that they apply not only to a historical point of view, but also to current global paradigms: studies in non-western traumatized patients report crucial differences from western populations in PTSD symptoms, including relative salience of avoidance and especially somatic symptoms (Hinton & Lewis-Fernández, 2011).
Even in recent decades, there have been shifts in the symptom pool of PTSD. The changes in the criteria from PTSD according to DSM-III/DSM-IV to those according to DSM-5 demonstrate this. PTSD was no longer categorized as a threat-based anxiety disorder, and to further underline this, a new cluster of symptoms called “negative alterations in cognitions and mood” was introduced. While re-experiencing symptoms still dominate the PTSD criteria, the DSM-5 added many other key symptoms, vastly expanding the variety of PTSD symptoms from the diverse historical “symptom pool.” Perhaps a trend has started here, where the focus will shift from “reliving” and the concept of “traumatic memory” to yet others, for example, depression, shame, and guilt. Interesting is the recent focus on moral aspects of traumatic situations, termed “moral injury” (Griffin et al., 2019). Moral aspects have always played a role in traumatic situations, but perhaps they come to the fore especially in these days because, more than in the past, humanity is seen as an important value.
In short, regardless of whether trauma-related disorders have an universal psychobiological basis, history shows that they have an interpretive superstructure that allows for ever-changing symptom manifestations (Horwitz, 2018). Consequently, this could explain the non-existence of a stable set of posttraumatic symptoms throughout history. Therefore, the current PTSD formulation can be seen as the next stage in an ever-changing pattern of responses to life-threatening situations (Jones & Wessely, 2007).
For the Future: Towards More Flexible Symptom Profiles
One of the main findings from this historical review is the large heterogeneity in symptom and syndrome expressions described in posttraumatic stress syndromes, which has fluctuated over the centuries. These findings are not surprising: in our opinion, there is a substantial bias in thinking about serious adverse experiences leading to a specific symptom profile. Throughout history, there was a search for a universal, timeless, single way to describe the mental response to an enormous range of adverse events, from single traumatic events like motor vehicle accidents to torture, concentration camps, or long-lasting abuse. This is likely impossible: the consequences of traumatic events depend on a broad range of factors like, for example, characteristics of the events itself, characteristics of those affected, the circumstances before, during, and after the events, and certainly time-bound social, cultural, and professional developments and paradigms. This knowledge should lead to the insight that the mental consequences of traumatic experiences will never be unambiguous and will always remain varied in expression. This creates a challenge to look for diagnostic models that are more flexible in defining the variety of changing symptom profiles.
Several diagnostic approaches have been put forth in recent decades, some of which represent a whole new diagnostic angle. In these approaches, diagnostic classifications are being supplemented or replaced by specific symptom dimensions within or outside these diagnostic classes. Examples are the “Hierarchical Taxonomy of Psychopathology” (HiTOP; Kotov et al., 2017), the “Quadripartite Model” (Watson, 2009), or the “Research Domain Criteria” (RDoC; Cuthbert, 2015). An upcoming and challenging way of diagnostics is being worked out in the network approach. In this approach, symptoms are not reflective of an underlying latent construct but are related to and cause each other (Borsboom, 2017) and has also been studied in PTSD (Birkeland et al., 2020).
While these diagnostic models offer challenging, entirely new perspectives, research has not progressed far enough to provide these models with a sufficiently solid foundation. Therefore, here we formulate a proposal that is closer to the existing, categorical way of thinking. This means that, in our opinion, posttraumatic phenomena can be better described in a hybrid form, with dimensional information in addition to categorical information: a diagnostic model with both subtyping and staging.
The model of “subtyping” of PTSD means that in addition to the core symptoms of PTSD, subtypes can be added to reflect the variation in symptomatology (Dalenberg et al., 2012). Subtypes give a more personalized representation of the diversity of posttraumatic symptoms and will allow more specific treatment targets. Due to the presumed dimensional nature of PTSD (Broman-Fulks et al., 2006), subtyping can add useful information. Although DSM-5 contains non-dimensional delayed and dissociative subtypes, several studies indicated important other subtypes such as on the dimension of internalizing versus externalizing symptomatology (Forbes et al., 2010), somatic comorbidity (McFarlane et al., 2017), subthreshold versus full PTSD (Morgan-López et al., 2020), symptom complexity (Cloitre, 2015), or symptom severity (Jongedijk et al., 2019). Severity in particular is an important dimension, as Broman-Fulks et al. (2006, p. 377) state: “At a minimum, researchers should supplement the categorical diagnosis with dimensional measures of PTSD severity.”
A variant of subtyping is the approach of “staging,” a diagnostic model derived from diagnostic models in somatic diseases such as cancer and diabetes. Some authors argue that PTSD is viewed too much as a unitary entity without considering a longitudinal perspective that encompasses a series of stages in the progression of the disorder (McFarlane et al., 2017; Nijdam et al., 2022). They propose a model with, in short, four stages defined as: (0): Asymptomatic but at risk; (1a): Undifferentiated symptoms of mild anxiety and distress; (1b): Subsyndromal distress with some behavioral and functional decline; (2): First episode of full-threshold symptoms; (3): Persistent symptoms with ongoing impairment; and ultimately (4): Severe unremitting illness of increasing chronicity with substantial disability. The last two stages in particular are characterized by a high degree of comorbidity, often blurring the boundaries between the different diagnostic DSM-classifications (Jongedijk et al., 2019).
While subtyping provides current information about the variety of posttraumatic symptomatology, staging provides a longitudinal perspective. We propose to combine both approaches to get a thorough and realistic picture of the patient’s psychopathology. This would yield a more personalized diagnostic point of view. In addition, it offers scope for a more targeted treatment approach aimed at specific symptoms that are most burdensome for the individual patient (McFarlane et al., 2017; Schmidt, 2015).
In conclusion, our review of the phenomenological descriptions of posttraumatic disorders along the lines of history provides an important clinical message: clinicians have to consider a broadening view on the posttraumatic symptomatology they are faced with. In other words, diagnostic classification has not to be based on “top-down” diagnostics, but be drawn by diagnostic formulations from a thorough “bottom-up” assessment that reviews all diagnostic possibilities (McHugh & Treisman, 2007). A description of posttraumatic symptomatology according to a model of both “staging” and “subtyping” will help patients to find recognition of their mental conditions, to understand and rebuild their life histories, and to find more personalized treatment approaches. Ultimately, a more flexible diagnostic system may replace the unproductive search for a universal trauma reaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.