
Abstract
Human rights statements on intersex characteristics distinguish legitimate “medically necessary” interventions from illegitimate normalizing ones. Ironically, this binary classification seems partially grounded in knowledge of anatomy and medical interventions; the very expertise that human rights statements challenge. Here, 23 European health professionals from specialist “disorder of sex development” (DSD) multidisciplinary teams located medical interventions on a continuum ranging from “medically essential” to nonessential poles. They explained their answers. Participants mostly described interventions on penile/scrotal, clitoral/labial, vaginal, and gonadal anatomy whose essential character was only partially grounded in anatomical variation and diagnoses. To explain what was medically necessary, health care professionals drew on lay understandings of child development, parental distress, collective opposition to medicalization, patients “coping” abilities, and patients’ own choices. Concepts of “medical necessity” were grounded in a hybrid ontology of patients with intersex traits as both physical bodies and as phenomenological subjects. Challenges to medical expertise on human rights grounds are well warranted but presume a bounded and well-grounded category of “medically necessary” intervention that is discursively flexible. Psychologists’ long-standing neglect of people with intersex characteristics, and the marginalization of clinical psychologists in DSD teams, may contribute to the construction of some controversial interventions as medically necessary.
Intersex is one of several contested umbrella terms used to describe physical characteristics that render a person’s embodiment different from normative or typical definitions of male and female bodies. Other terms used in this arena include “Variations in Sex Characteristics” (or VSC, Government Equalities Office, England and Wales, 2019), disorders of sex development (or DSDs, Lee et al., 2006), and differences of sex development (see Delimata et al., 2018 on experts’ current disagreements, and Lundberg et al. (2018) on laypeople’s understandings of such “umbrella terms”). Since the 19th century, clinical medicine has been the dominant discipline which has adjudicated questions about what constitutes intersex and how intersex people should be treated in society (Dreger, 2000; Reis, 2009). Psychological rationales for the medical “normalization” of intersex characteristics, particularly surgeries in infancy, were pressed with greater urgency in the middle of the 20th century. In that context, by drawing on the cybernetics and animal psychology of his time, the psychologist John Money prescribed infant genital surgeries to enhance both infants’ identification with assigned genders, and to enable parent–child bonding (Gill-Peterson, 2018; Morland, 2015). These interventions became more common as advances in pediatric endocrinology allowed cortisol injections to save the lives of infants born with congenital adrenal hyperplasia (CAH). Infants with XX genotype and CAH were the largest, and best researched, diagnostic group who experienced the kinds of “normalizing” infant surgeries promoted by John Money’s protocols, which went uncontested in clinical medicine into the 1980s (Kessler, 1990).
In the 1990s, diverse challenges from the social sciences (Kessler, 1998), patient advocacy (Chase, 1998), medical ethics (Dreger, 1998), and revelations of fraud in Money’s research and ethical abuse in his clinical practices (see Colapinto, 2001) all cast considerable doubt on the legitimacy of long-dominant protocols in this otherwise isolated medical specialism (see also Davis, 2015). Skepticism regarding Money’s hypothesis that any child could adopt any gender identity to which they are assigned in infancy led many to call for a blanket ban on early surgical interventions (Diamond & Sigmundson, 1997). With their legitimacy challenged, medical interventions on intersex became subject to sharper thinking about which were genuinely vital, or had well-evidenced health benefits, and which had been—problematically—conducted only to “normalize” physical appearance with dubious rationales, and often without clear informed consent (see e.g., Frader et al., 2004, p. 427). The Intersex Society of North American (ISNA) pushed for a patient-centered approach to replace paternalistic medicine, focused on open communication, consent, the avoidance of unnecessary interventions, and the acknowledgment of psychosocial need and risk.
The growth of intersex advocacy groups in the 1990s not only led to a critique of existing protocols by giving voice to the harms they had caused, it also allowed “intersex” to become a social identity category with which some people began to identify in some situations (Preves, 2003). However, social psychological understanding of how people with intersex characteristics navigate social contexts marked by stigma was, and remains, limited. Instead, in a long history of dehumanizing and instrumentalizing research, women and girls with CAH, were positioned as “natural experiments” to satisfy scientific curiosity about nature/nurture issues (See Ellis, 1945; Money & Ehrhardt, 1972, for early arguments). Even into the 21st century, psychologists studied women and girls with CAH for few reasons other than to discover their adult sexual identities and gender role behaviors, with little regard for the impact of life events or individuals’ responses to such events (Stout et al., 2010). Ignorance of psychosocial and psychosexual impact of medicalization was so profound that it was only in the 21st century that studies empirically demonstrated that “normalizing” clitoral surgery in infancy impacted adult psychosexual functioning (Crouch et al., 2008; Minto et al., 2003).
In pediatrics, the field defining “Chicago Consensus Statement” responded to these epistemological and moral controversies (Lee et al., 2006). This consensus statement grounded diagnostic concepts in genetics in ways that would have been unimaginable by John Money in the 1950s, when many phenotypic variations were known, but genotypic understanding was limited (Gill-Peterson, 2018; Griffiths, 2018b). Georgiann Davis (2015) describes the “chicago consensus statement” as a move to reground intersex within the terms of medical authority. It projected an ideal of certainty and of good medical practice that might address some evident concerns, but subsequent research has suggested that it did not end controversy on several important points (Liao & Roen, 2014).
First, the Chicago consensus recommended that the term “disorders of sex development” be used in preference to “intersex” or other terms on the grounds that the term DSD was clearer and less pejorative. However, these claim are troubled by continuing controversies between medical specialists as to whether DSD refers primarily to genetic or anatomical variation (see Griffiths, 2018b), social research showing that affected young people and their carers use a range of language terms in everyday contexts, other than DSD (e.g., Lundberg et al., 2019), and a 10-year update to the consensus statement which found continuing expert disagreement about why the DSD might be problematic (Delimata et al., 2018). This lack of coherence may result from the fact that “DSD” is often understood to be an Aristotelean category with clear biological referents, but is often deployed as a goal-directed category, describing a range of ways that medical interventions and diverse bodies can, with some optimism, be brought together (Thorne & Hegarty, 2019).
Second, while the consensus described the goal of medical intervention in patient-centered terms, medical practice has not changed substantively in some areas. While the Chicago consensus acknowledged the harms of infant clitoral surgeries, only some teams self-reported a reduction in rates of these surgeries in its wake (Pasterski et al., 2010) and national statistics in some countries show no clear reductions over the long run (Creighton et al., 2014, see also Mouriquand et al., 2016; Wolffenbuttel & Crouch, 2014). Chicago also acknowledged a lack of evidence for Money’s assumption that surgical interventions would enhance parent–child bonds, and endowed parents with greater authority in medical decision making. Several qualitative studies have shown that the obligations of decision making remains profoundly distressing for parents, and are often rushed in medical practice (Roen, 2019). Even when health care professionals seem to advocate delaying interventions, their arguments for delay can be unclear (Liao et al., 2019) and their presentation of medical interventions in positive terms can sway parents’ decisions (Timmermans et al., 2018). Davis’ (2015) claim that Chicago was an attempt to reimpose medical authority seems borne out by the increased funding for biomedical research on DSD following Chicago (Sandberg et al., 2015).
These diverse and partial effects of the Chicago consensus statement explain why advocates have adopted diverse goals and strategies in different organizations and movements since its publication. One broadening counter-consensus describes how current medical management, prototypically infant surgeries, places human rights in jeopardy, particularly children’s rights to bodily autonomy and self-determination (Carpenter, 2016; Office of the High Commissioner for Human Rights, 2019). Informed by advocacy groups who remained critical of Chicago after 2006, such as Organization Intersex International, global human rights bodies have increasingly researched ongoing medical practice and added their voices to challenging its ongoing legitimacy. A second strategy of medical activism operated by placing activists on decision-making bodies to change guidelines and to bring about change to democratize decision making about both clinical care and research directions (see Davis, 2015; Sudai, 2019). The present article aims to inform general psychologists about what their medical colleagues might be doing in this contested space. We aim to draw psychology closer to the question of what people with intersex characteristics, and those who support their flourishing, might hope to gain from current human rights movements, and their statements about which medical practices particularly need to be prohibited to protect infants’ human rights. While legal scholar Tanya Ni Mhuirthile’s (2010) notes that people with intersex characteristics might hope for less from the exercise of prohibitive law, than appears to be the case, Sudai (2019) argues law can both reground questions on fundamental principles of justice and value and that law remains critical to challenging professional norms in this area of medicine.
Human rights documents do not position all possible medical interventions on intersex characteristics as infringing human rights. Rather they construct two classes of interventions whose differing necessity undergirds their different legitimacy as practices that need to continue and practices that the law must prohibit. An agreed-upon limit of the exercise of legal prohibition in this area is the category of legitimate “medically necessary” interventions on intersex characteristics that might, or even should, be performed to protect human rights. This category is conceptualized somewhat differently in different documents. For example, a 2015 United Nations factsheet declared that states should recognize the risk of abuse engendered by “unnecessary surgery and treatment on intersex children” that is performed without consent (emphasis added). Similarly, Parliamentary Assembly of the Council of Europe Resolution 1952 (2013) calls on member states to guarantee bodily integrity by forbidding treatments that are “cosmetic rather than vital for health during infancy or childhood” (emphasis added). In 2015, the EU Fundamental Rights Agency described irreversible interventions that impose sex on babies and toddlers as “cosmetic rather than medically essential” (emphasis added). Also in 2015, Malta prohibited “any sex assignment treatment and/or surgical intervention on the sex characteristics of a minor” and is often described as the first country to ban surgical interventions (Malta, 2015). However, even the Maltese law allowed parents to consent to interventions in “exceptional circumstances” as long as they are not “driven by social factors.” Similar dichotomies can be found in Amnesty International’s (2017, p. 26) report on medical practices in Germany and Denmark which exemplified the category of the “clear medical necessity for surgery” using the example of a urogenital sinus. Research by Human Rights Watch (2017, p. 95) in the United States pointed to “the removal of cancerous gonads” to exemplify “intersex conditions that do, indisputably, require surgical intervention.”
A detailed description of this category is in Bill 201 of the California Senate (2019) which defines necessity as reasonable, necessary to protect life, prevent significant illness or disability, or alleviate severe pain, to address a risk of cancer significantly greater than that in the population, cannot be safely deferred until informed consent is possible, cannot be based on “psychological factors,” follows from consent that does not discuss risks and alternatives. The United Nations (2015, p. 10) has also reasserted the distinction between nonurgent interventions that are “invasive or irreversible” which bring “high potential for, and evidence of, harm” from those “essential for physical health, such as when an infant is unable to urinate, or unable to retain salt.” The Yogyakarta + 10 principles assert, in relation to sex characteristics, that “No one shall be subjected to invasive or irreversible medical procedures that modify sex characteristics without their free, prior and informed consent, unless necessary to avoid serious, urgent and irreparable harm to the concerned person” (Yogyakarta Principles, 2017).
In sum, human rights bodies do not call for complete cessation of all interventions but include grounds for conceptualizing interventions as necessary if they are vital, essential, exceptional, reversible, noninvasive, unlikely to harm, and are nonessential if they are cosmetic, appearance-based, normalizing, or driven by social factors. There are variable ways of constructing line between allowable necessary and immoral practices in human rights documents, and those lines can rest on current medical expertise to a variable degree. Who else, other than a medical professional, can be trusted to judge when an infant’s body does or does not put that infant’s own life at risk? As such, human rights documents adopt an ambivalent stance toward medical professionals in DSD teams. On one hand, those teams are guilty of human rights abuses and, on the other hand, they possessing unique expertise that sets the limits of the human rights critique of their practices. In the United States, DSD health care professionals have been observed to use this conceptual ambiguity to exercise their clinical judgment when they advise parents of infants with intersex traits in practice (Timmermans et al., 2018).
To better understand how expert health care professionals in DSD teams might respond to this complex positioning of their expertise, we examined empirically here how they demarcate medical interventions that are essential from those which are not. Both cognitive and discursive psychologists have good reason to anticipate that the morally laden dichotomy in human rights documents and in emerging law might be simpler than health care professionals’ reasoning about interventions that their teams can enact. Humans think with categories that have fuzzy boundaries, internal structures that vary depending on the goals they are constructed to pursue, and which are represented by characteristics or exemplars in different contexts (see e.g., Barsalou, 1983; Medin, 1989; Rosch & Mervis, 1975). Categorization is also social, and humans rarely categorize other humans just for the sake of it, but quite often do so to impose culturally specific, morally laden forms of social orders on more messy forms of reality (Douglas, 1966). In practice, this often requires switching between different modes of categorization, as when diagnostic reasoning involves both reasoning with exemplars (cases) and formal definitions (Bowker & Starr, 1999; Croskerry, 2009). Human rights documents exemplify this flexibility in categorical construction, drawing on both characteristics (such as necessity), exemplars (such as a urogenital sinus), and background norms (against which extremity is conceptualized) in their discourse. Such thinking may be characterized by “the illusion of explanatory depth”; people reason as if their categories had clear ontological grounding, which emerges as illusionary when those categories require explicit explanation (Hampton, 2010).
We examined whether DSD professionals found themselves challenged by unexpected dilemmas when called upon to “draw the line” regarding essential medical interventions. Qualitative studies have often described health care professionals as voicing rationales for medical intervention that go beyond the interests of people with intersex characteristics themselves (Karkazis, 2008; Kessler, 1990). Interventions can be understood by health care professionals as benevolent, sometimes because they are grounded in an understanding of normative embodiment as providing a shelter from stigma and shame or merely in avoiding parental distress (e.g., Binet et al., 2016). The bioethicist Ellen Feder (2014) has argued that human rights can not only be conceptualized as lying within bounded individual subjects, but may exist in relationships, between parents and children for example. Peck and Feder (2017) have also urged consideration of how health care professionals in DSD teams may commit institutional evils—not out of conscious intent—but rather out of the failure to consider and challenge institutional norms which may reasonably be foreseen to bring about intolerable harms. Parents often chose interventions for their children in medical practice, when those interventions are made available to them (Ellens et al., 2017; Timmermans et al., 2018). Vulnerability to human rights abuse emerges at the intersection of familial and organizational socialities.
Human rights statements make health care professionals vulnerable to charges that they are enacting torture, or other cruel, inhumane and degrading treatment or punishment against which appeals to benevolent intent do not offer a sustained defense. The best wishes in the world for children to escape stigma, and for their parents’ distress to be eased, are not grounds for medical interventions by contemporary human rights standards. Responding to their own context of contested authority, health care professionals, like others in argumentative contexts, may be expected to draw on different ontological grounds for particularizing and generalizing from instances to position the line between medical necessity and non-necessity (Billig, 1987). Again, cognitive research would suggest that they might do so by more clearly articulating how patients are vulnerable because they differ from social norms for embodiment, development, and identity, such that it is easiest to imagine mutation in the direction of normativity (Kahneman & Miller, 1986). To the extent that reasoning does draw upon such “blind spots” regarding what is assumed as normative, health care professionals’ understandings of the medically necessary, may be linked to structural oppression regarding sex and gender (Peck & Feder, 2017, p. 214).
When Mendez (2013) clarified, in his role as the U.N. Special rapporteur on Torture, that the United Nations understood that torture did not require harmful intent, he did so at a time when the American Psychological Association (APA) Code of Ethics called on psychologists to end torture in all of its manifestations (APA, 2002). Clinical psychologists’ inclusion in DSD multidisciplinary teams is described by the 2006 Chicago consensus statement as material to ethical decision making and patient and parent well-being. The 2015 Hoffman report on collusion of the APA with torture carried out by the U.S. Department of Defense in Guantanamo has made clear that the 2002 APA Code of Ethics was written to allow psychologists who experienced conflict between professional ethical obligation and a law or order to ethically follow the law or order. Hoffman et al. (2015) concluded that the writing of this ethical standard into the 2002 APA Code was a consequence of collusion between actors in the APA and the U.S. Department of Defense. Torture had been defined restrictively by the U.S. Department of Defense after the September 11th attacks in 2001. However, Hoffman et al. (2015) also included that there had been no deliberate intention to afford psychologists’ active involvement in interrogations involving torture techniques in Guantanamo in the writing of the 2002 Ethics Code.
The relationship between the definition of torture in psychologists’ professional ethics and the more recent attribution of torture to the medical interventions conducted in multidisciplinary DSD teams has not been addressed before. In various public statements prior to the Hoffman et al. Report (2015), the APA reaffirmed its commitment to principles of opposing torture under international human rights law and to the authority of the office on the U.N. Special Rapporteur on Torture in deciding what is and what is not “torture” (APA, n.d.). Consequently, one understanding of the current landscape would be that clinical psychologists, who are often made peripheral in multidisciplinary DSD teams (See Liao & Roen, 2019), may collude with torture in medicalized environments, while acting in good faith for patient benefit. Clarifying how health care professionals ground the medical necessity of their practices may thus be of broad ethical concern for general psychologists.
The Present Study
Here, we analyzed how health care professionals might, when pressed to do so, “draw the line” between different interventions that vary in their necessity. We draw on interviews that were conducted as part of the SENS project, which includes the in-depth and systematic investigation of how young people, parents, and carers, DSD health care professionals, and laypeople make sense of differences of sex development and their medicalization. SENS data was collected in four European countries; Scotland, England, Norway and Sweden. Three previous publications, drawing on these interviews with health care professionals in this corpus have examined how these DSD health care providers make sense of continuing interventions on the vagina (Roen et al., 2018), the penis (Roen & Hegarty, 2018), and the clitoris (Liao et al., 2019). Consistent themes emerged from these analyses. DSD health care professionals (a) wrestle with dilemmas between historical warrants and recent challenges to particular medical interventions, (b) are often unaware of the performative effects of their discourse in framing available interventions as necessary ones, and (c) do very little to challenge patients and parents’ received norms about what “normal” bodies are or can do. The present analysis focuses on how medical necessity is conceptualized and talked up across all possible interventions and draws on a conceptual task that we introduced early on in these interviews.
Methodology
Data Collection
The U.K. National Health Service and a U.K. University Ethics Committee approved this study. The last author used snowball sampling recruitment methods, supported by the fourth and fifth authors’ networks, to interview 32 U.K. and Swedish health professionals working with or in multidisciplinary DSD teams. Early in those interviews, she presented a 3,500 mm horizontal line with ends marked as “medically necessary” and “cosmetic.” Her interview protocol read as follows: The distinction between interventions that are medically essential, and interventions that are helpful for improving appearance (i.e., cosmetic interventions) may be seen differently by different people. Can you tell me about what kinds of interventions you would describe as medically essential interventions or interventions that are helpful for improving appearance? If these are the endpoints on a continuum, what kinds of interventions would you describe as lying along the continuum?
This paper-based task was not carried out in six telephone interviews. Two further interviewees choose not to mark the paper but talked about the idea of the continuum presented. Another replaced the diagram with a three-pronged radial diagram labeled “necessary,” “appearance,” and “family.” These three responses evidence that a binary distinction, or even a continuum, between essential versus cosmetic interventions is not the natural or immediate way for these health care professionals to conceptualize what their teams do. The analysis here draws on the responses of the remaining 23 interviewees who responded to our challenge to place their team’s interventions on this line; six urologists, four endocrinologists, three psychologists, three geneticists, three gynecologists, two pediatric surgeons, and two nurse specialists. Even within this sample, a further two strongly suggested alternative diagrams to better represent multidimensional spaces that included “family” “reconstructive,” “functional,” or “psychosocial” interventions more explicitly. Diagrams were retained and interviews were audio-recorded and transcribed.
Placing Interventions Along the Line
We interpreted the 3,500 mm line as a 101-point scale ranging from 0 (nonessential) to 100 (medically essential). Interviewees made 2 to 15 legible marks each (M = 6.82), to a total of 157 such responses. Responses were widely distributed around the scale’s midpoint, M = 53.3, SD = 32.5. One response positioned beyond the “nonessential” end was scored as 0. The first author read and reread the sections of interview transcripts where participants explained their responses. A two-tier system for categorizing the interventions emerged. Interventions were framed in discourse primarily by reference to the site, the goal, or the targeted group of the interventions. Second, responses were subdivided by the distinct sites, goals, or groups addressed. Table 1 displays the number and proportion of interviewees making responses in each subtype and their range on the continuum. As it shows, participants most commonly conceptualized these interventions in terms of the site that they targeted, consistent with a grounding of interventions primarily in the natural facts of bodily variation with goals and diagnoses being secondary.
Number, Mean, and Range of Locations of Medical Interventions on 100-Point Scale and Number and Percentage of Health Professionals who Mentioned Them by Site, Function, and Group (0 = Not Essential, 100 = Medically Essential).
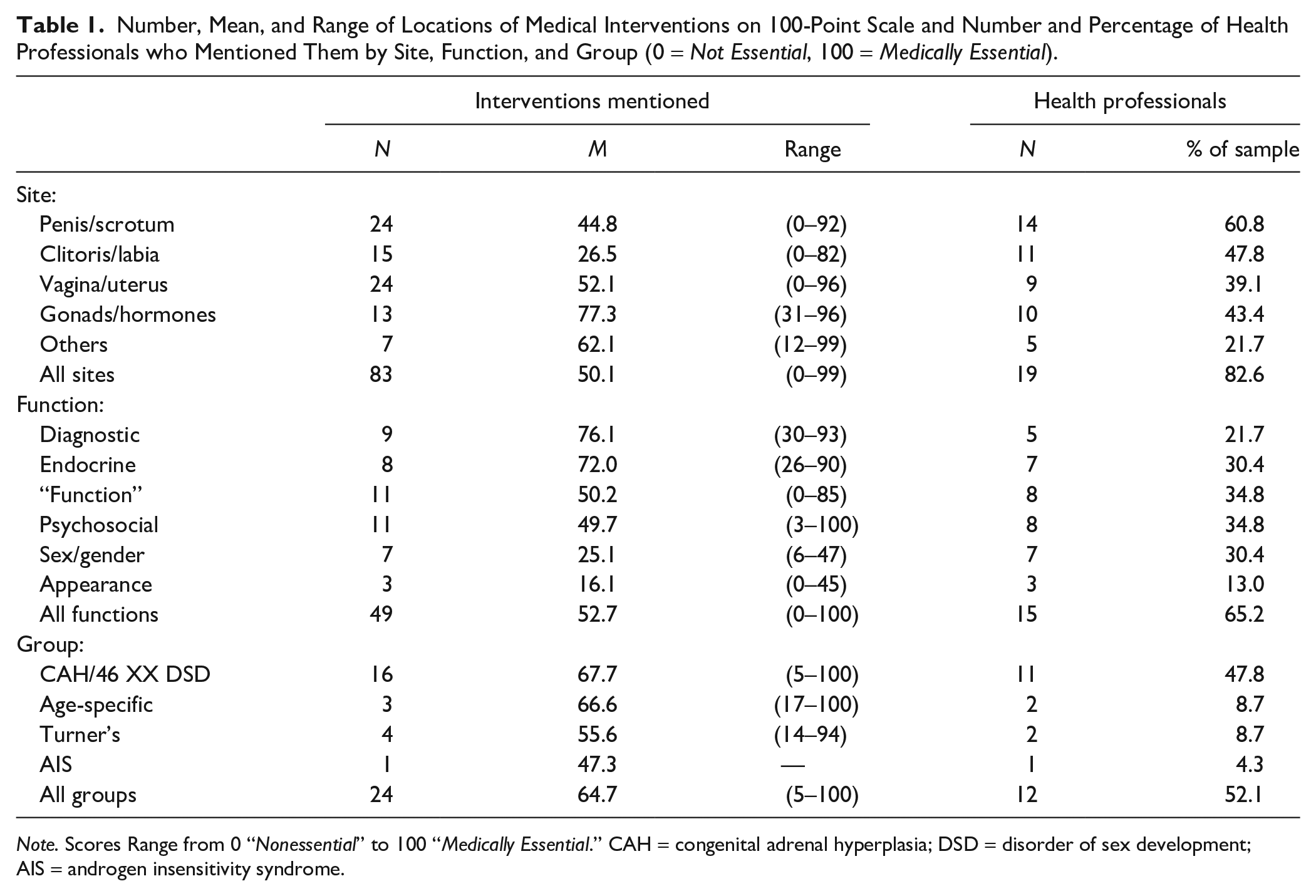
Note. Scores Range from 0 “Nonessential” to 100 “Medically Essential.” CAH = congenital adrenal hyperplasia; DSD = disorder of sex development; AIS = androgen insensitivity syndrome.
The first author extracted the talk about each subtype as the first step in the thematic analysis (Braun & Clarke, 2006). Systematic overlap in the contents of subtheme led to the decision to conduct the present analysis which is oriented around the sites of intervention. Published analysis of clinician’s talk from the entire interviews about the intervention on the first three of these sites have been published as noted above. We reference those papers in the analysis below so that we can examine how the category of “medical necessity” emerges across interventions rather than only in regard to interventions targeting a particular anatomical characteristic.
Four preliminary observations preface this analysis and frame the forms of categorization that health care professionals attempted here. First, cognitive psychologists have long known that the most prototypical instances of any category are called to mind quickly and with greatest frequency (Rosch & Mervis, 1975). The clearest example of the “prototype” of a medically necessary intervention here, being mentioned first and by many participants was the life-saving steroid interventions used to address salt-wasting CAH in infancy. Second, the continuum was not symmetrical but marked (Horn, 2001), as the nonessential pole had no equivalently common or readily accessible anchor, and its meaning was sometimes reconstructed; “. . . it may be a functional choice,” or relabeled (as “interventions that are helpful for the overall management of the family” for example). The definition of what medical necessity is seems far clearer and more coherent than the definition of what it is not. Third, while expert medical consensus favors clear and precise referential language in this domain (Lee et al., 2006), interviewees had clear preferences for vagueness in some areas. It was particularly difficult to specify what cognates of the word “function” mean, as they sometimes seemed to be discrete ways of talking about physical excretion or sexual practices, and sometimes seemed to refer to psychosocial experiences more loosely attached to those physical processes. Finally, interventions targeting the breast, cloaca, or urethra were mentioned too rarely to allow detailed analysis.
Analysis
Is Hypospadias Repair Necessary on a Desert Island?
The urethral opening of a hypospadic penis is located along the underside and not at the tip, and hypospadias are routinely “repaired” by surgery to “normalize” appearance and allow boys to control urinary stream (Lee et al., 2006). Hypospadias surgeries were mentioned by over 60% of interviewees (see Table 1), reflecting Karkazis (2008, p. 144) description of them as the “bread and butter” work of DSD surgical teams. As described elsewhere, interviewees were aware that hypospadias surgeries were somewhat controversial, and pointed to a lack of personal experience with their own patients’ postsurgical regret (Roen & Hegarty, 2018). Variance in locating these interventions on the continuum was large, partially as a function of a commonly evoked distinction between “mild” or “distal” hypospadias occurring closer to the tip of a penis and “severe” or “proximal” hypospadias occurring closer to or at the scrotum. Interventions on the latter were always deemed more essential.
In addition, health care professionals’ constructions of the essential or nonessential character of these interventions prompted several of them to project forward what the social environment of young boys with untreated hypospadias might be. One urologist voiced the traditional view that hypospadias surgery was necessary to give the young person an opportunity to, you know, particularly as a boy to, you know, be continent to not least stand up at the urinal with his pals and pee in the pot at the same time.
The idea that hypospadias surgery is particularly necessary for psychologically healthy boyhood because all boys must be able to urinate standing up, is long-standing in pediatric urology (Griffiths, 2018a). Informed by the possibility of such stigmatization in childhood, contemporary bioethical opinion describes hypospadias intervention as an intervention that might particularly pit the benefits of a stigma-free childhood against risks to sexual sensation for adults (Wiesemann et al., 2010). While these risks to children have been mentioned in the medical literature since the 1920s (Reis, 2009), no developmental psychological studies evidence the risk of stigma from untreated hypospadias. Risks to adult men from iatrogenic effects of surgery were not mentioned; participants called to mind sexual behavior only in regard to “where the semen has to go” and never in regard to risks to sexually sensate tissue. Some health care providers clearly rejected the inherited view in pediatric urology regarding the risk of teasing in the toilet: the reality is that doesn’t happen, because children these days do not look at other people’s, other children’s penises, they just don’t do that. So, I’m not sure whether it’s medically essential.
Finally, empathy with parents’ anxiety and distress about the risks of stigma, even in the absence of any evidence of its likelihood, can impact clinicians. As another urologist put it: “in some cases the boy is not all that concerned, but the father is.” Elsewhere in the interviews, some health care professionals, notably clinical psychologists, reported responding to these parents’ concerns by framing the refusal of surgery as actively “waiting” rather than “doing nothing” (Roen & Hegarty, 2018). This urologist described the non-necessity of this intervention as follows: If you lived on a desert island um, hypospadias would be perfectly compatible with normal survival. So um, I, I think one would have to start with the idea that all hypospadias surgery is cosmetic.
Desert islands have anchored western people’s imagination of stories of individuals living in cultural isolation for centuries (see e.g., Defoe, 1719). Here, the image supports the logical conclusion that since hypospadias repair is “only cultural” that intervention on it is not essential. This framing is consistent with a human rights perspective that hypospadias surgery is conducted for such socially normalizing reasons. Such rationales were variously endorsed and rejected by health care professionals and used in combination with descriptions of variation in penile anatomy to draw the line around what might be “medically essential” here.
Clitoral Surgery: “I Can Hear Some of What They Are Saying.”
46 XX karyotype children with CAH are more often born with fused labia and/or a larger than typical clitoris (Lee et al., 2006). Talk about these anatomical sites and talk about these diagnostic groups overlapped considerably. About half of the participants mentioned interventions that targeted the labia and the clitoris and they were located more toward the nonessential pole of the continuum than interventions targeting all other anatomical sites (M = 26.5, see Table 1). Health care professionals voiced more explicit awareness of the controversial nature of surgical interventions when discussing interventions that targeted the labia and the clitoris than when discussing hypospadias surgery. One participant mentioned an advocacy group and said, “I can hear some of what they are saying.” At times, opposition to these medical interventions led some health care professionals to name harmful effects and to attribute them to parents: I’ve been to some meetings where girls are talking about having a clitoris that’s been mutilated. To think that it’s mums (or dad’s) poor compliance [with medication intended to curb clitoral growth] that’s sending us into that. I think there is a role here for child protection.
In other parts of the interviews, clinicians described the need to remain flexible to manage dilemmas between historically inherited norms for intervention and challenges to those interventions (Liao et al., 2019). When these interventions were placed closer to the medically necessary pole, their location was justified on similar grounds to arguments for hypospadias surgery; concern that the child would not cope in school, particularly if anatomic variation was deemed to be “severe,” and parental concern about such possibilities. Health care professionals also drew inferences about children and parents’ variable capacity for “coping” to infer when clitoral reduction, however undesirable, remained worth doing: clitoral reduction in child is purely for cosmetic reasons and to keep parents happy really. Actually. But also it’s you know how does that child cope with school and all that sort of stuff?
One participant who opposed such surgeries described them as not on my planet. This was accompanied by an appeal to health economics, and prioritizing demands within a socialized health care system according to principles of distributive justice.
In conclusion, health care professionals were far more aware of the controversial nature of clitoral and labial interventions than others, but still used personal experience with particular patients to argue why such interventions might approach necessity, for well-intentioned reasons, in some “severe” cases. In the larger interview contexts, discussions of these interventions suggested the possibility of pluralistic ignorance (Prentice & Miller, 1996), as all health care professionals suggested that their own DSD teams had become more conservative in regard to these surgeries than was the norm in medical practice (Liao et al., 2019, p. 3). As the next themes show, participants’ understandings of where the professional norm lies for any given intervention could be very debatable.
Sexuality, Identity, and Fertility: “Do You Need a Vagina for Medical Reasons?”
Vaginal agenesis is associated with complete androgen insensitivity syndrome (CAIS) and Mayer–Rokitansky–Küster–Hauser (MRKH) syndrome. Common vaginal construction interventions include irreversible surgery and dilation regimes, with the latter being preferred as the first approach in many European countries. Surgery on adolescents and adults carries risks, and dilation can be painful, effortful, and prolonged (Liao et al., 2011). These interventions are not life-saving but aim to support identity, sexuality, and fertility in adults (Lee et al., 2006). In our analysis of the larger interviews, we found health care professionals to be aware of pressure on women to “normalize” their vaginas, and the distress that normative ideas of womanhood can bring about for women with androgen insensitivity syndrome (AIS) have long been known to qualitative psychologists (Alderson et al., 2004). Also, and in contrast to the last two themes, health care professionals voiced far more explicit awareness that the interventions that they might offer in regard to vaginal agenesis would place an additional demand on patients’ ability to “cope.” Accordingly, health care professionals discussed how some psychological preparedness would be required before the demanding dilation regimes could begin.
Health care professionals were more discriminating between specific vaginal interventions than in all other areas when drawing the line; the nine who described vaginal construction made, on average 2.67 distinct marks on the line, in contrast to 1.71 marks for interventions on the penis and scrotum, and 1.36 marks for interventions on the clitoris and labia (see Table 1). Discriminating more finely between interventions did not lead to simple stable conclusions about where to draw the line. Rather, speech disfluencies, such as “uhs” and “ums,” were particularly common in explaining where vaginal interventions might fall along the continuum. Health care professionals also more often commented on their difficulty of explaining their answers here. They voiced awareness that medicalization of the body was an intentional act, that the extent of valid medicalization was in doubt, and that the resulting understanding of medical necessity fell out from the construction of medicalization that was chosen. One gynecologist marked distinct interventions for vaginal agenesis at six points on the continuum, but still wondered out loud “Do you need a vagina for medical reasons”? They expanded: That is the question really isn’t it? Most people would argue yes t- in ord-
1
you know that you know you want to be sexually active in order to maintain your general health and things like that so I suppose you could then stick vaginal dilators up here [locating “vaginal dilators” at point 62 on the continuum] and a vaginoplasty if necessary comes somewhere in the middle but you would actually you don’t need that . . . not required until an adult . . . until sexually active [locating “vaginoplasty—not required until sexually active” at point 61 on the continuum].
One clinical psychologist made the contingency between the “medicalizing” and the consequent “essential” nature of intervention explicit by distinguishing between understandings of patients as mechanical bodies that might need repair, or as bodies with which people may wish to function sexually: it depends whether you want to medicalise the body and say that they are medically essential because you need to repair the body but then they would probably say more they’re for sexual functioning.
It was around these interventions where it became most apparent that health care professionals needed to choose between two different ontologies of their patients’ embodiment to complete the task. In one ontology, which provided certainty and stable ground, patients’ embodiment could be understood in mechanistic terms. In the other, patients’ bodies were understood as situational and phenomenological, such that sex development was more like a process of “embodied becoming” in which physical, psychological, and social were mutually interacting and constitutive of each other (Roen, 2009). Health care professionals seemed most keenly aware that the first ontology could not ground their concept of medical necessity, on its own, in regard to vaginal interventions. The disparity between these two was lessened if patients who requested interventions in a manner consistent with health care professionals’ own opinions were called to mind. But even then, other matters might trouble the attribution of adult consent to a patient, leaving the dilemma of defining medical necessity in play. Such troubling factors included patients’ age: if it’s interventions like dilatation, for example, I guess if it’s something that the young person wishes to happen, um, and they want to be a sex-, have a sexual life, then I guess, oh it’s really difficult.
Or the desire for intervention for psychological reasons rather than for heterosexual intercourse: The, the whole concept of cosmetic then changes once people can give informed consent um and um there are people I’ve come across who do not want to have a vagina um, there are some, there’ve been a few who’ve said, “I never intend to use my vagina for intercourse, but I still want to have one because it will make me feel more normal.” Um, i-, it may be as simple as being able to refer to “my vagina” um.
As the next theme makes clear, when describing interventions on aspects of the body that can be imagined as having a causal effect on psychology, different grounds for constructing medical necessity emerge.
Managing Risk: Hormones, Gonads, and the Category of the “Essential”
In some conditions, a 46, XY child’s gonads may be testicular, may be undescended, and may co-occur with a female gender identity (Lee et al., 2006). In recent decades, the “brain gender” hypothesis that fetal androgens organize both brain development and external genital anatomy has gained influence (Jordan-Young, 2010), and more children with intersex traits have been assigned male in recent decades (Kolesinka et al., 2014). Gonadectomy without explicit consent occurred commonly prior to the 2006 Consensus Statement (Preves, 2003). Endocrine interventions and interventions on gonads were considered, on average, the most essential of the interventions described by participants (see Table 1). Here, health professionals commonly voiced the traditional justification of gonadectomy by cancer risk, rarely qualifying their judgments of that risk by condition, or referencing human rights concerns. Beyond the very prototypical “medically essential” cortisol interventions to save the lives of infants with CAH, interventions on hormones and gonads were described as medically essential on grounds other than being life-saving. Describing hormone blockers for a girl with CAH going through some virilization, one geneticist said: Well, it’s not going to be life threatening but for some people it might be essential because it might be absolutely vital that they . . . don’t virilize or they have a choice but for other people it is down here [further from the medically essential pole], it is an intervention that is helping cosmetic appearances . . . so you know it is dependent on the disorder that is the problem, a lot of these things are dependent on the disorder.
Here, an intervention is described as essential and vital, even though it is not going to be life-saving, and what is vital is that the body does not virilize. This response makes very clear how endocrinology might ground a category of seemingly essential interventions that are categorically not life-saving, and are common in this area of clinical medicine. Feder (2014) has argued that when intersex characteristics are conceptualized primarily in terms of their inconsistency with gender binary norms, then they may not be understood as human tissues with value and integrity. As Dreger (2000, p. 1) notes, citing Canguilhem, the phenomenology of normativity is such that the exception appears to consciousness long before the norm from which it deviates comes into view. In this study, less normative embodiment seems to call for a “vital” intervention, while the norm of embodiment to which intervention orients goes without saying. Although the proposed intervention has clear benevolent intent, the grounding of that benevolent intent in normative understandings is less explicit.
This understanding can be bolstered by appeal to an understanding of the patient either as a body or as a person. This geneticist qualified their judgment with appeal to medical classification; it is dependent on the disorder that is the problem. In contrast, a psychologist resolved the dilemma via an understanding of medical necessity that recognized the psychological impact of intervention on the individual: So I think things like pubertal induction I think I would generally say, yes, they’re around cosmetic and appearance related issues and should we really be, um, intervening with that? But at the same time I kind of feel in terms of psychologically, um, the impact, kind of feel like I would fall more on this side ever so slightly.
After 2006, some clinics delayed some gonadectomies to allow spontaneous pubertal development and to avoid the need for hormonal replacement (Allen, 2009). As with vaginal surgery, adult patients’ own wishes informed health care professionals’ judgments about when gonadectomy was medically necessary. But while they often oriented to patients who wanted interventions more than was medically normative, here they described dilemmas and discomfort arising from patients refusing interventions that were medically possible: Now increasingly I understand, that more and more of these ladies are choosing not to have their gonads removed, which is putting health professionals now in a difficult dilemma. Because they feel they want to re-, they need to be removed, they’re leaving them to let the individual decide and then the individuals have decided to do something opposite of what they feel should be done. Well then you’ve given them that choice and you need to respect their decision.
We next draw together these findings to reach conclusions for general psychology.
Conclusions
Like the human rights documents that critique them, the DSD professionals interviewed here can call to mind clear-cut examples of particularly essential interventions, understand that cosmetic, appearance-based interventions conducted only for socially normalizing reasons are not legitimate, and remain vexed by ambiguous cases where it seems less clear whether people with intersex characteristics should be conceptualized primarily as bodies, psychological subjects or rational choice-makers. Health care professionals sometimes draw lines between interventions on grounds of anatomical variation alone. But they also often find it necessary to draw on a more phenomenological ontology in which bodies are situations that human subjects experience. These participants were sometime aware that they did not operate on a “desert island” but in a context sometimes characterized by a dubious received wisdom about interventions, collective opposition to medicalization, parental anxiety, health care economics, the state’s role in child protection, and patients’ powers to make choices to demand or refuse particular interventions.
Our demand to “draw the line” around medical necessity presented these DSD health care professionals with “a difficult dilemma” (Billig et al., 1988). However, drawing the continuous line for this task allowed them more room for ambiguity than does the binary classification of interventions emerging in human rights and legal documents. A useful conceptual distinction between human rights framings and the clinical expertise described here is offered in a recent statement on bodily integrity in regard to infant genital surgeries. The Brussels Collaboration on Bodily Integrity (2019) distinguishes what is “medically beneficial” on the balance of harms and benefits from what is “medically necessary” on the grounds of being life-saving. This study has shown how DSD health care professionals have flexible, consistent, and practiced ways of stretching the latter category of interventions to address the former, by grounding their understandings of benevolent action in psychosocial concerns. Medical expertise might be characterized by an illusion of explanatory depth (Hampton, 2010) that relies on norms to an extent that is not always clear to those who voice the expertise. As a result, current practices can be explained as if they refer to clear categorical differences when that is not really the case.
This observation, that DSD professionals may not explicitly understand what they are doing in regard to social norms or human rights, is not new (see also Kessler, 1990; Karkazis, 2008; Human Rights Watch, 2017). Nor is it surprising, considering that surgeries on infants’ intersex characteristics, have, from John Money’s work onward, been warranted by humanistic concerns grounded in untested optimism about what medical interventions can achieve (Morland, 2015). Current human rights movements force health care professionals to argue for medical practices that once seemed reasonable to presume. In this more contested context, arguments may seem grounded in “personal opinion” (as with hypospadias here), harms blamed on parents (as with clitoral surgeries here), of unclear value (as with vaginal interventions here) or grounded in a not-yet refuted medical specialism such as endocrinology. To convince, such arguments often project narratives in which psychology may figure as centrally as anatomy. As Timmermans et al. (2018) put it, such arguments about the future life of a patient rather than their current status may be person-focused without being infant-focused. In the context of such narratives, human rights demands to retreat medicine to the strictly “medically necessary” or to that which adult patients freely choose may seem like flawed attempts to withdraw social support offered by the only professionals entrusted with responsibility to support the care and flourishing of people with intersex characteristics and their families.
It would seem then that people with intersex characteristics might be offered more diverse forms of social support, which legal prohibitions on some interventions will not provide on their own (Ni Mhuirthile, 2010). Recognizing that human rights and children’s rights particularly depend upon how we imagine nurturing relationships with adults points to the question of what psychologists can do, in the most general sense, that might support people with intersex characteristics, their families and the over-reaching health care providers whose interactions are such a cause for concern. The under-application of psychology is matched only by the overreach of medicine to psychological matters in these interviews. Since 2006, a plethora of smaller qualitative psychology studies have contributed clear answers about how the social organization of health care can be made more humane and less shaming, in this area (Roen, 2019). These studies are but one sign of how—since John Money’s pivotal writings of the mid-20th century—psychological science has vastly expanded its understandings in ways that might be conducive to demedicalizing intersex. For example, psychologists have developed understandings of the bounded rationality achieved by multidisciplinary medical teams (Meehl, 1973), children’s ecological contexts (Bronfenbrenner, 1979), how people cope actively in response to threats of social stigma (Crocker & Major, 1989), how to conceptualize the difference between professional and lay understandings of concepts (Kelley, 1992), the resolution of ideological dilemmas, including health care dilemmas through common sense reasoning (Billig et al., 1988), how projections of social norms onto children inform the concept of “development” (Burman, 1994), and how heteronormative and cisgenderist assumptions operate in psychological science (Hegarty, 2018).
Aspects of epistemological violence such as the denial of a voice in shaping research questions, and instrumentalizing research about nature/nurture issues that tends to “other” may be material to this late application of psychology’s usual enthusiasm for humanistic projects grounded in science (Teo, 2010). Rather than blaming bad medicine that over-reaches, we psychologists might reflect on our own positions and the historic neglect of people with intersex characteristics, qua people, in our own field, which has been material to medicine’s over-reaching. It is not adequate to delegate this responsibility to clinical psychologists within DSD teams, such as those sampled here, who inhabit an ambiguous and treacherous institutional context. Clinical psychologists may face dilemmas between their professional understanding of psychosocial needs and the organization of health care in which they find themselves. Elsewhere in the SENS interviews, DSD medical professionals showed an understanding of psychology as most relevant to patient care when patients or parents were already in distress, and sometimes in distress that was a consequence of interactions with other DSD team members (Liao & Roen, 2019). In other studies based on the SENS data set, clinical psychologists reframe medical necessity by creatively reframing waiting on making decisions as a way of “doing something” (Roen & Hegarty, 2018; c.f, Roen, 2008). In the face of highly variable personal opinions among clinical colleagues, the dynamic of culpability and complicity with medical intervention is likely to characterize clinical psychology in this area (see Peck & Feder, 2017). The urge to “do something” in the clinic may, in part, be a result of other psychologists doing very little, for a long time, in any other respect to impact this medicalized population. Psychologists have not yet conceptualized clearly enough the flourishing of people with intersex characteristics and their family members, nor have we adequately understood the dynamics among communities, societies, and legal and health care frameworks upon which that flourishing might rely.
Footnotes
Acknowledgements
The authors thank David Griffiths and Iain Morland for comments on an earlier draft, and Faisal Ahmed, Naomi Crouch, and Julie Alderson for invitations to present these results to European medical professionals who work in DSD multidisciplinary teams.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.