
Abstract
Experiencing the homicide of a loved one can lead to considerable posttraumatic stress disorder (PTSD) symptoms and impair life satisfaction. Beyond the loss itself, trial attendance and trial-related factors (perception of justice, distress during the trial, dissatisfaction with the verdict) can further influence the PTSD symptoms and life satisfaction of homicidally bereaved individuals (HBI). However, the relationship between trial attendance, trial-related factors and perceived social support (PSS) have not yet been examined. This study compared the PTSD symptoms and life satisfaction of HBI who attended a trial and those who did not. It also investigated whether trial attendance moderated the relationship between PSS, PTSD symptoms and life satisfaction. Finally, the study explored associations between trial-related factors, PTSD symptoms and life satisfaction among HBI who attended a trial. A total of 149 participants (including 63 HBI who attended a trial and 86 who did not) completed an online questionnaire. Results showed that trial attendance moderated the association between PSS and PTSD symptoms. Trial-related factors accounted for a significant portion of the variance of PTSD symptoms and life satisfaction, beyond the contribution of PSS and time since the homicide.
Introduction
Experiencing the homicide of a family member has severe psychological consequences. Indeed, studies have shown that homicidally bereaved individuals (HBI) often report elevated levels of posttraumatic stress disorder (PTSD) symptoms and reduced life satisfaction (Simmons et al., 2014; van Denderen et al., 2015). Regarding PTSD symptoms, Sharpe and Iwamoto (2022) found that 17.8% of HBI met the PTSD diagnostic threshold for PTSD, defined as a score of 30 or higher. For life satisfaction, in the study of Simmons et al. (2014), scores of HBI fell in the “slightly dissatisfied life” category (M = between 14.14 and 15.65; SD = not reported). Beyond PTSD symptoms and life satisfaction, HBI are also at risk of developing prolonged grief, depression, anxiety, and substance abuse (Bastomski & Duane, 2018; Miller, 2009; Rheingold et al., 2012; Rheingold & Williams, 2015; Zinzow et al., 2009). A qualitative study further suggests that when suddenly confronted with the homicide of a loved one, bereaved individuals can experience a profound loss of control, question their personal safety, and begin to avoid situations associated with the homicide (Mastrocinque et al., 2015).
Moreover, HBI are often exposed to specific stressors, such as attending a criminal trial (Alves-Costa et al., 2018; Connolly & Gordon, 2015) which is frequently experienced as distressing or even harmful (e.g., Pastia & Palys, 2016). However, to date, no quantitative study has specifically investigated the relationship between trial attendance, PTSD symptoms and life satisfaction among HBI. Qualitative studies suggest that attending a trial can exacerbate the PTSD symptoms in this population (e.g., Englebrecht et al., 2014; Metzger et al., 2015). Furthermore, studies investigating how trial-related factors (such as perception of justice, distress during the trial, and dissatisfaction with the verdict) are associated with PTSD symptoms and life satisfaction among HBI are scarce. Existing studies on the psychological impact of trial attendance and trial-related factors have focused on populations other than HBI, such as rape survivors (e.g., Campbell et al., 2001; Morissette & Wemmers, 2016; J. A. Wemmers, 2013). Nonetheless, their results suggest that such factors may also be relevant to the psychological adjustment of HBI.
In addition, prior research has yielded conflicting results regarding the association between perceived social support (PSS), a well-established protective factor, and PTSD symptoms among HBI. For instance, Rheingold and Williams (2015) showed that higher PSS is related to fewer PTSD symptoms, whereas Burke et al. (2010) reported no significant relationship between those variables. These disparities could reflect the influence of other contributors such as trial attendance and trial-related factors. However, to date, no study has examined the ways in which trial attendance and trial-related factors are related to PSS among HBI. In other populations, a study involving rape survivors found that a strong social support system is critical in helping individuals endure the significant psychological stress of legal proceedings (Feldthusen et al., 2000).
To address this gap, the present study compared the levels of PTSD symptoms and life satisfaction between HBI who attended a trial and those who did not. It also examined whether trial attendance moderates the relationship between PSS, PTSD symptoms and life satisfaction. Finally, among HBI who attended a trial, the study investigated whether trial-related factors influence PTSD symptoms and life satisfaction beyond the contribution of PSS. All analyses controlled for the time elapsed since the homicide.
This paper shed light on a specific stressor commonly experienced by HBI, which is trial attendance. In doing so, it identifies the challenges faced by bereaved individuals following the homicide of a loved one and offers a set of recommendations for mental health professionals and criminal justice workers to better address the needs of HBI.
PTSD Symptoms and Life Satisfaction of HBI
For each homicide, 7–10 individuals close to the deceased loved one are negatively affected in several aspects of their lives (Redmond, 1989; Rheingold et al., 2012). The violent and unexpected nature of this loss can lead to considerable PTSD symptoms including intrusive thoughts, avoidance of memories or situations associated with the homicide, negative alterations of thoughts, and emotions and hypervigilance (American Psychatric Association, 2013). The average PTSD score among HBI is considerably higher than that of individuals bereaved by accident and general populations, as assessed through undergraduate students (Ashbaugh et al., 2016; Burke et al., 2010; Djelantik et al., 2021). Additionally, the lifetime prevalence of PTSD among HBI significantly surpasses that found within the general population (19.1%–71% compared to 1.7%; Lake et al., 2020; van Denderen et al., 2015). In their systematic review, van Denderen et al. (2015) reported current PTSD prevalence rates among HBI ranging from 5.2%-6% across the studies reviewed.
Data indicates that the life satisfaction of HBI is also significantly impaired (Simmons et al., 2014). Life satisfaction is defined as the global evaluation of an individual’s life according to their chosen criteria such as goals and values (Diener et al., 1985; Shin & Johnson, 1978). Beyond the psychological consequences resulting from the loss, HBI must cope with very specific stressors such as attending a trial, which can impact their PTSD symptoms (e.g., Alves-Costa et al., 2018; Gekoski et al., 2013; van Denderen et al., 2016).
Impact of Trial Attendance
For both PTSD symptoms and life satisfaction, no study has specifically compared HBI who attended a trial and those who did not. In qualitative studies, navigating the legal system is challenging for HBI and exposure to the trial is often experienced as revictimizing and confusing (e.g., Metzger et al., 2015). Moreover, in the qualitative study of Englebrecht et al. (2014), findings suggest that although few HBI expressed positive views about their trial attendance, for others, this event exacerbated their grief and harmed them at a time of extreme vulnerability. Consequently, this study aimed to better understand the association between trial attendance, PTSD symptoms and life satisfaction among HBI.
Impact of Trial-Related Factors
Alongside trial attendance, researchers have studied the associations between trial-related factors and the PTSD symptoms and life satisfaction of HBI. These trial-related factors included perception of justice, distress during the trial and dissatisfaction with the verdict.
Perception of justice refers to the evaluation of the fairness of a situation (Van Den Bos & Lind, 2002) and is divided into four types according to the Organizational Justice Scale (OJS) developed by Colquitt (2001): (1) distributive (i.e., how the effort of the criminal justice workers reflects the outcome of the trial); (2) procedural (i.e., fairness of the legal procedures); (3) interpersonal (i.e., quality of interactions); and (4) informational (i.e., quality of information provided by criminal justice workers). One quantitative study using this construct indicated that being informed about the case (informational justice) was not significantly related to PTSD symptoms among HBI (Thompson et al., 1996). In qualitative studies, a global perception of justice was associated with less anger among HBI (e.g., Baliko & Tuck, 2008). Moreover, a lack of information regarding the CJS (informational justice) was associated with distress (e.g., Alves-Costa et al., 2021; Reed & Caraballo, 2022; Thiel, 2016).
The only available quantitative information regarding the association between perception of justice (other than informational) and PTSD symptoms relates to non-HBI populations. Among other crime victims (such as individuals affected by assault, robbery, threat, harassment of property crime), procedural, interpersonal and informational justice were significantly associated with fewer PTSD symptoms (Gray, 2006; Morissette & Wemmers, 2016; J. A. Wemmers, 2013).
Regarding life satisfaction, to our knowledge, no quantitative or qualitative study has examined the association between perception of justice (distributive, procedural, interpersonal or informational) and the life satisfaction of HBI. In other populations, a study conducted by Hu et al. (2024) showed that all four dimensions of perceptions of justice were positively associated with life satisfaction among workers from private-sector companies. The positive association between perception of justice and life satisfaction remains to be explored in traumatized populations such as HBI.
Distress during the trial refers to the emotions experienced during the trial. Regarding PTSD symptoms, to date, no quantitative study has examined how HBI’s distress during the trial is related to their PTSD symptoms. The qualitative study of Reed and Caraballo (2022) revealed that 15.8% of HBI reported experiencing negative flashbacks during court proceedings. In other populations, one quantitative study showed that rape survivors who perceived the trial process as hurtful reported higher levels of distress than those who did not have (Campbell et al., 2001). Regarding life satisfaction, to our knowledge, no quantitative or qualitative study has examined how HBI’s distress during the trial is related to their life satisfaction.
Satisfaction or dissatisfaction with the verdict constitutes the affective response to the positive or negative evaluation of the trial outcome (Kunst et al., 2015). Regarding PTSD symptoms, dissatisfaction with the verdict was not investigated quantitatively among HBI. The only available information relates to non-HBI populations. Indeed, several studies among victims of violent or property crime showed that satisfaction with the verdict was positively associated with self-esteem and faith in a just world (Orth, 2002) and was negatively associated with feelings of revenge toward the perpetrator (Orth, 2004), current distress (Tontodonato & Erez, 1994) and PTSD symptoms (Orth & Maercker, 2004). Therefore, it is possible that satisfaction with the verdict is also associated with PTSD symptoms among HBI. Regarding life satisfaction, to our knowledge, no quantitative or qualitative study has examined how HBI’s satisfaction or dissatisfaction with the verdict is related to their life satisfaction.
This state of scientific research indicates that studies looking at the relationship between trial-related factors, PTSD symptoms and life satisfaction among HBI are still very rare. However, studies among other populations (such as rape survivors) suggest that these factors could be associated with the PTSD symptoms and life satisfaction of HBI (e.g., Campbell et al., 2001; Hu et al., 2024; Orth & Maercker, 2004).
Impact of Perceived Social Support (PSS)
Perceived social support (PSS) refers to an individual’s perception of the quality of their social interactions. The Multidimensional Scale of Perceived Social Support (MSPSS), developed by Zimet et al. (1988), addresses this subjective assessment and identifies three specific sources of PSS: (1) family (e.g., I get the emotional help and support I need from my family); (2) friends (e.g., I can count on my friends when things go wrong), and (3) significant others (e.g., There is a special person who is around when I am in need). This instrument has frequently been used in the literature (e.g., Bailey et al., 2013; Burke et al., 2010) and was employed in the present study.
According to Lepore’s (2001) social-cognitive processing model, the psychological adaptation to a traumatic event is facilitated by PSS. Empirical studies have confirmed the positive role of PSS in numerous populations of trauma survivors (e.g., victims of natural disasters, emergency workers, individuals bereaved by suicide; Arnberg et al., 2012; Oexle & Sheehan, 2020; Setti et al., 2016).
Regarding PTSD symptoms, only two quantitative studies have examined the association with the PSS of HBI. One showed that PSS was significantly linked to fewer PTSD symptoms (Rheingold & Williams, 2015). However, Burke et al. (2010) did not find a significant relationship between these variables. The limited and inconsistent results indicate a need for further research, especially when HBI experience unique stressors such as trial attendance.
Regarding life satisfaction, in the study of Simmons et al. (2014), HBI who were talking with friends and family and were spending more time with family reported higher levels of life satisfaction. These results suggest a positive association between PSS and satisfaction with life which remains to be examined among HBI.
Association Between Trial Attendance and PSS
Regarding PTSD symptoms and life satisfaction, the interaction between trial attendance, trial-related factors, and PSS was not investigated quantitatively among HBI.
The qualitative research tends to focus on the social support received from criminal justice workers rather than the one received from loved ones. For example, the qualitative study of Englebrecht et al. (2014) revealed that many HBI perceived that the support provided by criminal justice workers lacked empathy and compassion, which was associated with feelings of anger and frustration. Moreover, Reed and Caraballo (2022) reported that 52.6% of HBI expressed concerns about the lack of respect or empathy shown to them by criminal justice workers.
Regarding social support received from loved ones, no qualitative study on the interplay between trial attendance, trial-related factors, and PSS received from loved ones has focused on HBI. However, in other populations, one qualitative study among adult rape survivors (Feldthusen et al., 2000) emphasized the need for a strong social support system, especially from family and friends, to endure the intense stress of the criminal process. Approximately half of the participants who attended a trial reported receiving support from friends and family during the process, while the other half described negative consequences on their personal relationships. This study, conducted among rape survivors, suggests a potential interaction between trial attendance, PSS received from loved ones and PTSD symptoms, which has not yet been explored among HBI.
To our knowledge, no quantitative or qualitative study on the interplay between trial attendance and PSS has focused on the life satisfaction of HBI. Additionally, the impact of trial-related factors (such as perception of justice, distress during the trial and dissatisfaction with the verdict) on the PTSD symptoms and life satisfaction of HBI, beyond the well-established role of PSS, remains to be examined.
Objectives of the Present Study
The first objective was to compare the levels of PTSD symptoms and life satisfaction between HBI who attended a trial and those who did not. In addition, we aimed to examine the associations between trial-related factors (perception of justice, distress during the trial, and dissatisfaction with the verdict), PSS, PTSD symptoms, and life satisfaction. The second objective was to examine whether trial attendance moderated the relationship between PSS, PTSD symptoms and life satisfaction, when controlling for time since the homicide. The third objective, focusing only on HBI who attended a trial, was to determine whether trial-related factors (block 3) influenced PTSD symptoms and life satisfaction beyond the contribution of PSS (block 2) and time since the homicide (block 1).
Method
Participants and Procedures
Participants were recruited via bereavement support organizations. Advertisements were also published on social media pages, in a newspaper, and on a university campus. All advertisements included a link to the Qualtrics web platform, where participants signed an informed consent form and completed the 30-min survey. The questionnaire was the same for all HBI, except for the evaluation of trial-related factors (perception of justice, distress during the trial and dissatisfaction with the verdict) which were only asked of HBI who attended a trial. When they signed the consent form, participants were given information on the support resources available (support groups, therapists, useful reading). They were also given the contact details of the principal investigator so that they could be contacted in the event of distress or mental health problems related to the questionnaire. Although participants did not receive direct financial compensation, they could enter a random drawing to win one of five 70$ gift cards. Ethical approval for the current study was obtained from the board of the University of Quebec in Montreal (#2021-3318). The data was collected between 2022 and 2023.
To participate, individuals had to be at least 18 years of age, reside in Canada, have experienced the loss of an immediate family member (i.e., romantic partner, child, parent, grandparent, sibling or grandchild) by homicide more than 6 months before and be fluent in French or English. If the homicide occurred less than 6 months before their participation, we offered the possibility of collecting their contact details and sending them an invitation when 6 months elapsed since the loss of their loved one. Of the 278 participants who opened the questionnaire, 129 did not meet the inclusion or exclusion criteria or completed less than 80% of all questionnaires, and therefore were excluded from the sample. Analyses show no significant differences between included and excluded participants in terms of their sociodemographic characteristics (e.g., age, gender, marital status, education) and their scores for the dependent and independent variables.
The final sample consisted of 149 HBI, who had a mean age of 55.28 years (range: 21–81; SD = 11.74). Most participants identified as women (85.5%) and were highly educated (75% had at least completed college, an undergraduate degree, or the equivalent). HBI identified as Quebecer, Canadian or American (87.2%), First Nations (2%), Latin American (0.7%), Caribbean or West Indian (3.4%), South Asian or Subcontinental Indian (0.7%), Western, Southern or Northern European (6%), Eastern European or Central Asian (3.4%), North African, Middle Eastern, and/or Sub-Saharan African (less than 1.5%). More than half (55%) of the sample reported being married, in a civil union, or cohabiting with their partner, 43% reported being single, divorced, separated, or widowed and 2% responded “other civil status.” Participants identified their deceased loved one as a child (40.9%), sibling (24.8%), parent (20.8%), romantic partner (12.1%), or grandchild (1.3%). For HBI who attended a trial (n = 63), the accused was found guilty (93.4%), not guilty (1.6%) or unknown status (4.9%). Eighty-six HBI did not attend a trial because the murderer was never identified (35.6%), the murderer died (22%), a murderer was suspected but not charged (16.9%), the evidence was insufficient (5.1%), the accused pleaded guilty (3.4%) or other reasons (17%).
To determine group membership, participants who reported attending at least 1 day of a trial were placed in the “attended a trial” group, while other participants were placed in the “did not attend a trial” group. No significant difference in terms of PTSD symptoms and life satisfaction were observed between the four categories of the “did not attend a trial” group. If the trial was currently taking place, we offered the possibility of collecting their contact details and sending them an invitation when the trial ended.
Measures
The evaluation of sociodemographic characteristics included questions about the age and gender of the participant, time since the homicide, quality of relationship with the deceased, and characteristics of the trial.
The OJS (Colquitt, 2001) is a 20-item self-report measure of perception of justice that uses a 5-point Likert scale (1 = not at all; 5 = very often). This measure assesses four types of perception of justice: distributive (4 items; e.g., “Does the outcome of the trial reflect the effort of the criminal justice workers?”), procedural (7 items; e.g., “Have you been able to express your views and feelings during those procedures?”), interpersonal (4 items; e.g., “Have the criminal justice workers treated you with respect?”), and informational (5 items; e.g., “Have the criminal justice workers communicated details in a timely manner?”). As Colquitt (2001) points out, although this scale was intended to measure organizational justice, it can be adapted to any decision-making situation. Therefore, five items were adapted to the context of the CJS. In this study, the total score (α = .94, possible range: 20–100) and the subscale scores (α = .81–.95; possible range: 4–35) were used. Higher scores indicate more perceived justice within the CJS. Distress during the trial was measured using this question: “To what extent was your experience difficult or painful during the trial?”. Dissatisfaction with the verdict was measured using a two-item composite score (i.e., “After the trial, to what extent were you dissatisfied with the verdict?” and “After the trial, to what extent were you dissatisfied with the sentence of conviction?”). Participants rated each of these two items using a scale from 0 to 100 (0 = not at all; 100 = extremely), with higher scores indicating greater distress during the trial or dissatisfaction with the verdict (α = .94). All 23 items were reviewed by a team of 10 psychologists specializing in trauma.
The MSPSS (Zimet et al., 1988) is a 12-item self-report measure using a 7-point Likert scale (1 = very strongly disagree; 7 = very strongly agree). Items from this scale assessed PSS either from their family (e.g., “My family really tries to help me”), from friends (e.g., “I have friends with whom I can share my joys and sorrows”) and from a significant other (e.g., “There is a special person who is around when I am in need”). Each subscale includes four items. A higher total score (α = .93; possible range: 12–84) indicates more positive PSS.
The PTSD Checklist for DSM-5 (PCL-5; Blevins et al., 2015) is a 20-item (e.g., “trouble remembering important parts of the stressful experience”) self-report measure of the intensity of PTSD symptoms over the past month, using a 5-point Likert scale (0 = not at all; 4 = extremely). The instructions clearly stated that the questions must be answered with the homicide in mind. A higher total score (α = .95; possible range: 0–80) is associated with more severe symptoms. A total score of 33 is considered the cut-off point for a clinical PTSD diagnosis (Blevins et al., 2015). The Satisfaction with Life Scale (SWLS; Diener et al., 1985) is a 5-item (e.g., “In most ways my life is close to my ideal”) self-report measure of life satisfaction, using a 7-point Likert scale (1 = strongly disagree; 7 = strongly disagree). The total score (α = .89; possible range: 5–35) indicates greater life satisfaction.
Data Analysis
Before running the main analyses, statistical power, missing data, and assumptions were examined. Separate a posteriori power analyses were conducted for the second objective with all HBI (including one independent variable, one dependent variable, one dichotomous moderator; n = 131) and the third one with only HBI who attended a trial (including three independent variables and one dependent variable; n = 52). Both analyses yielded estimates indicating medium to large effect sizes (f2 = 0.16 and 0.49) with a statistical power of 80% and using a risk of type I error (α) of 5%. Hence, the sample sizes for both objectives were adequately powered to detect medium to large effects. Power estimations were carried out using Monte Carlo simulations with the Mplus version 8 software (Muthén & Muthén, 2002) and G*power (Faul et al., 2007). To handle missing data, scores for each scale were computed to replace missing values only for participants who responded to at least 80% of the items. Regarding the assumption of normality (Tabachnick & Fidell, 2013), all variables demonstrated acceptable levels of skewness and kurtosis, except for time since the homicide, which required a logarithmic transformation. The sample included 161 participants related to 149 homicide victims, violating the assumption of data independence. As most deceased loved ones were related to only one participant, multilevel analyses were deemed inappropriate. To address this dependency, one participant per deceased loved one was randomly selected and kept in the sample, resulting in the exclusion of 12 participants.
For the first objective, independent sample t tests were performed to compare the levels of PTSD symptoms and life satisfaction between HBI who attended a trial and those who did not. Pearson correlations among study variables were also calculated. For the second objective, two moderation analyses were conducted to determine if the relationship between PSS, PTSD symptoms and life satisfaction differed between HBI who attended a trial and those who did not. For the third objective, focusing only on HBI who attended a trial, four hierarchical multiple linear (HML) regression analyses were performed, two for PTSD symptoms and two for life satisfaction, which were entered as dependent variables. Although the quality of the relationship with the deceased was measured, it exhibited a ceiling effect (nearly all the HBI reported that they had an excellent relationship with their deceased loved one), meaning this measure could not be used in subsequent analyses. Since three recent studies have indicated that time since the homicide is associated with fewer PTSD symptoms (McDevitt-Murphy et al., 2012; Soydas et al., 2020; van Denderen et al., 2016), this variable was controlled for the second and third objectives. The significance level was set at p < .05 for all statistical tests. All analyses were conducted with the SPSS 27.0 software.
Results
Descriptive statistics are presented in Table 1. Both groups were, on average, near the PCL-5 clinical cut-off score of 33 (M = 32.62; SD = 20.39) and 47% reported clinical PTSD in the total sample (according to the recommended cut-off; Blevins et al., 2015). The mean life satisfaction score for all participants was 20.63 (SD = 7.93), which represents the central point on the scale where the respondent is equally satisfied and dissatisfied (Pavot & Diener, 1993). The two groups (HBI who attended a trial and those who did not) did not differ significantly in terms of PSS, time since the homicide, PTSD symptoms, and life satisfaction (see Table 1). Among HBI who attended a trial (see Table 2), higher levels of global perception of justice, distributive justice and informational justice were significantly associated with higher levels of life satisfaction, but not with PTSD symptoms. Increased levels of distress during the trial and dissatisfaction with the verdict were both significantly associated with higher PTSD symptoms and lower levels of life satisfaction. High levels of PSS were significantly associated with fewer PTSD symptoms and higher levels of life satisfaction. Among all HBI (see Table 3), PSS and time since the homicide were significantly associated with fewer PTSD symptoms and higher levels of life satisfaction.
Descriptive Statistics and Group Comparisons.
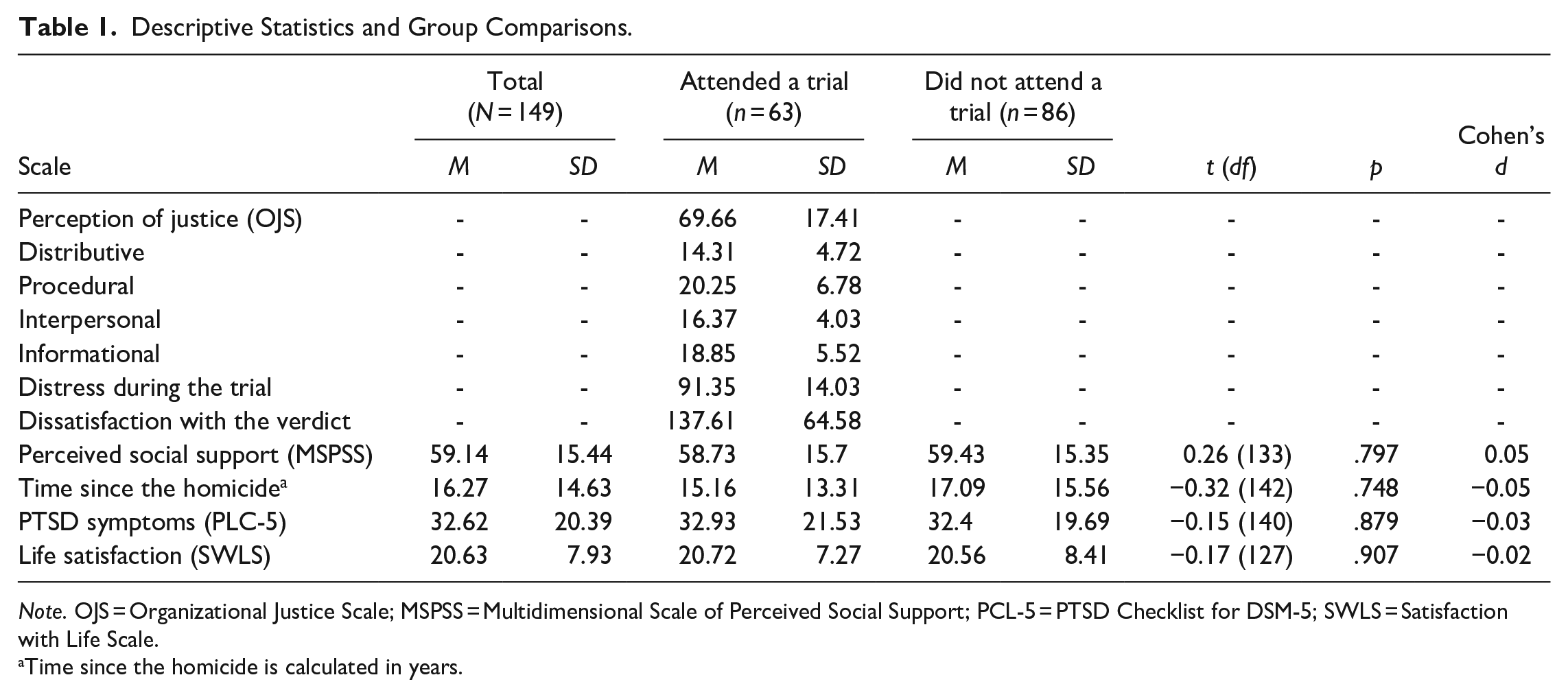
Note. OJS = Organizational Justice Scale; MSPSS = Multidimensional Scale of Perceived Social Support; PCL-5 = PTSD Checklist for DSM-5; SWLS = Satisfaction with Life Scale.
Time since the homicide is calculated in years.
Relationships Between Trial-Related Factors, Perceived Social Support, PTSD Symptoms, and Life Satisfaction Among HBI Who Attended a Trial (n = 63).
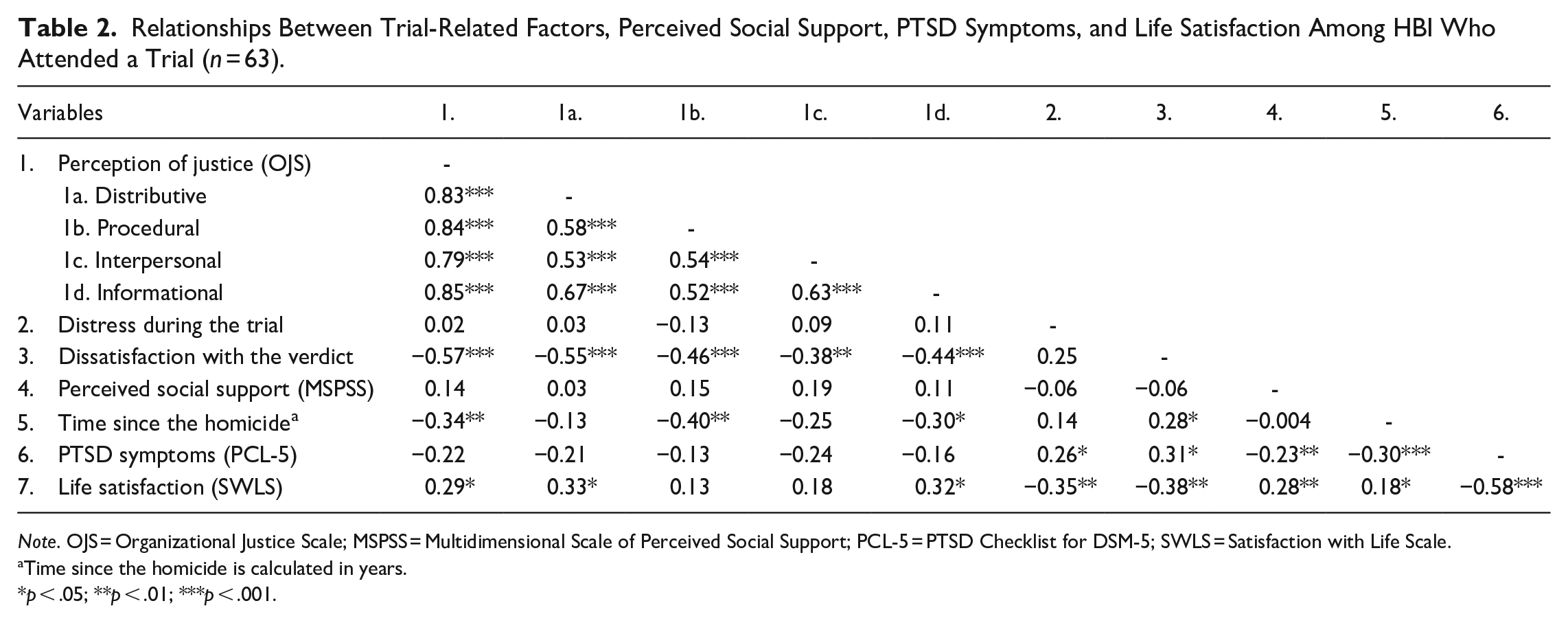
Note. OJS = Organizational Justice Scale; MSPSS = Multidimensional Scale of Perceived Social Support; PCL-5 = PTSD Checklist for DSM-5; SWLS = Satisfaction with Life Scale.
Time since the homicide is calculated in years.
p < .05; **p < .01; ***p < .001.
Relationships Between Perceived Social Support, Time Since the Homicide, PTSD Symptoms, and Life Satisfaction for the Total Sample of HBI (N = 149).
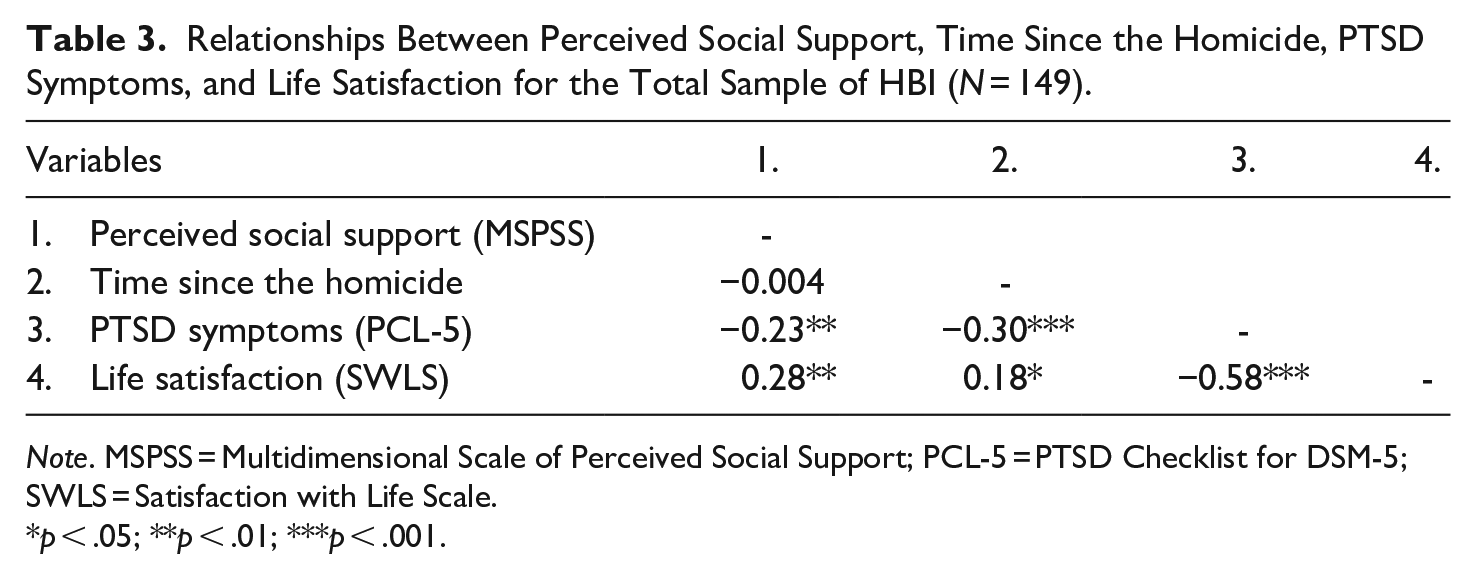
Note. MSPSS = Multidimensional Scale of Perceived Social Support; PCL-5 = PTSD Checklist for DSM-5; SWLS = Satisfaction with Life Scale.
p < .05; **p < .01; ***p < .001.
Moderation Analyses
To assess whether trial attendance moderated the relationship between PSS, PTSD symptoms and life satisfaction, two moderation analyses were conducted using Hayes’ PROCESS tool (Hayes, 2012, Model 1), while controlling for time since the homicide (see Figure 1). For PTSD symptoms, the interaction term was statistically significant (ΔR2 = 0.03; β = −.37, SE = 0.17, t = −2.19; p = .030), suggesting a moderating effect of attending a trial on the relationship between PSS and PTSD scores. This implies that the relationship between PSS and PTSD symptoms differed depending on whether the individual attended a trial or not. For individuals who did not attend a trial, PSS was not significantly related to PTSD symptoms (β = −.08, SE = 0.11, t = −0.78; p = .437). However, for HBI who attended a trial, there was a significant negative relationship between PSS and PTSD symptoms (β = −.45, SE = 0.13, t = −3.47; p < .001), suggesting that higher levels of PSS were significantly associated with fewer PTSD symptoms.
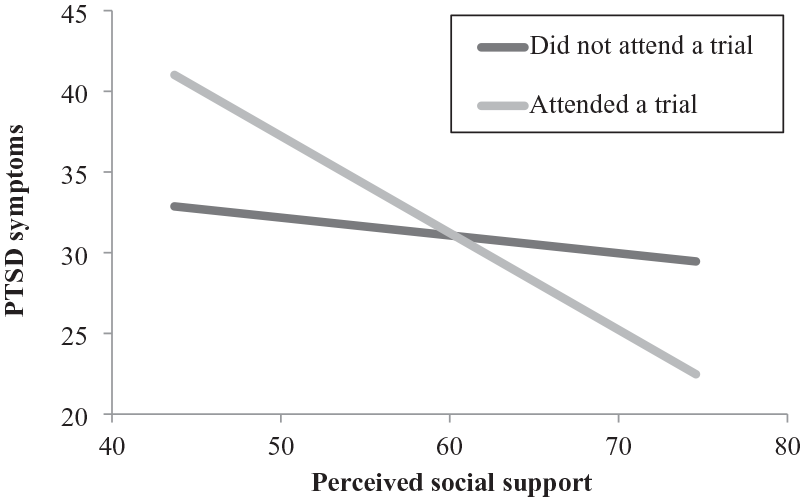
Changes in PTSD Symptoms as a Function of Perceived Social Support and Trial Attendance.
For life satisfaction, the interaction term was not statistically significant (ΔR2 = 0.01; β = .19, SE = 0.17, t = 1.09; p = .277), indicating that trial attendance did not moderate the relationship between PSS and life satisfaction. Indeed, PSS was positively associated with life satisfaction for HBI who attended a trial (β = .40, SE = 0.13, t = 3.02; p = .003) and for HBI who did not (β = .21, SE = 0.11, t = 1.92; p = .06).
Hierarchical Multiple Linear (HML) Regression Analyses
Four HML regression models were conducted with three blocks of variables. For the first pair (see Table 4), time since the homicide was entered in block 1, PSS in block 2, and perception of justice in block 3, with PTSD symptoms and life satisfaction as dependent variables. The final models accounted for 30% of the variance in PTSD symptoms and 23% of the variance in life satisfaction. After controlling for time since the homicide and PSS in blocks 1 and 2, perception of justice emerged as significantly and negatively associated with PTSD symptoms, and significantly and positively associated with life satisfaction among HBI who attended a trial. More specifically, perception of justice explained 7% of the additional variance in PTSD symptoms and life satisfaction.
HML Regression Analyses with Perception of Justice.
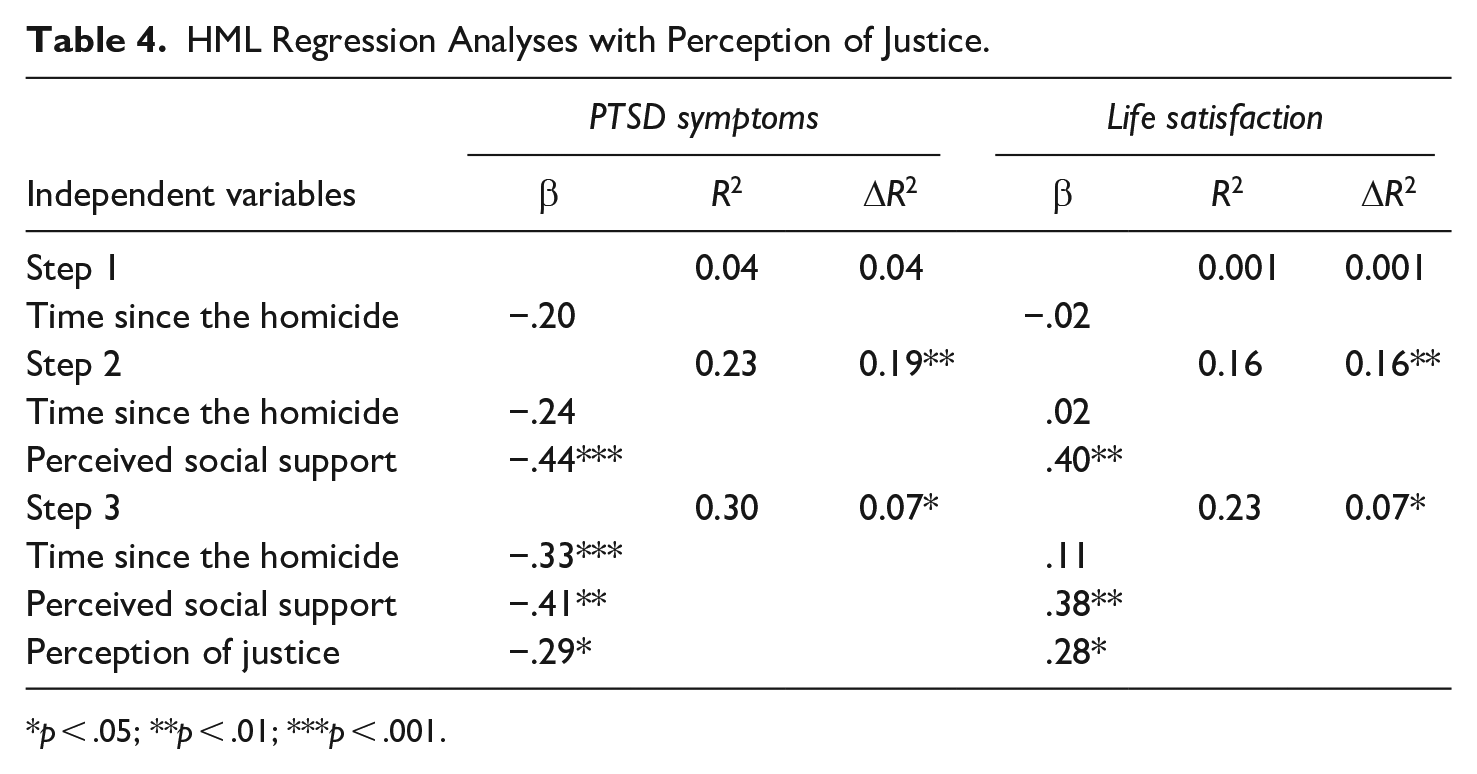
p < .05; **p < .01; ***p < .001.
For the second pair (see Table 5), time since the homicide was entered in block 1, PSS in block 2, and distress during the trial as well as dissatisfaction with the verdict in block 3, with PTSD symptoms and life satisfaction as dependent variables. The final models accounted for 48% of the variance in PTSD symptoms and 44% of the variance in life satisfaction. After controlling for time since the homicide and PSS in blocks 1 and 2, both distress during the trial and dissatisfaction with the verdict emerged as significantly and positively associated with PTSD symptoms, and significantly and negatively associated with life satisfaction among HBI who attended a trial. More specifically, distress during the trial and dissatisfaction with the verdict explained 22% of the additional variance in PTSD symptoms and 24% in life satisfaction.
HML Regression Analyses with Distress During the Trial and Dissatisfaction with the Verdict.
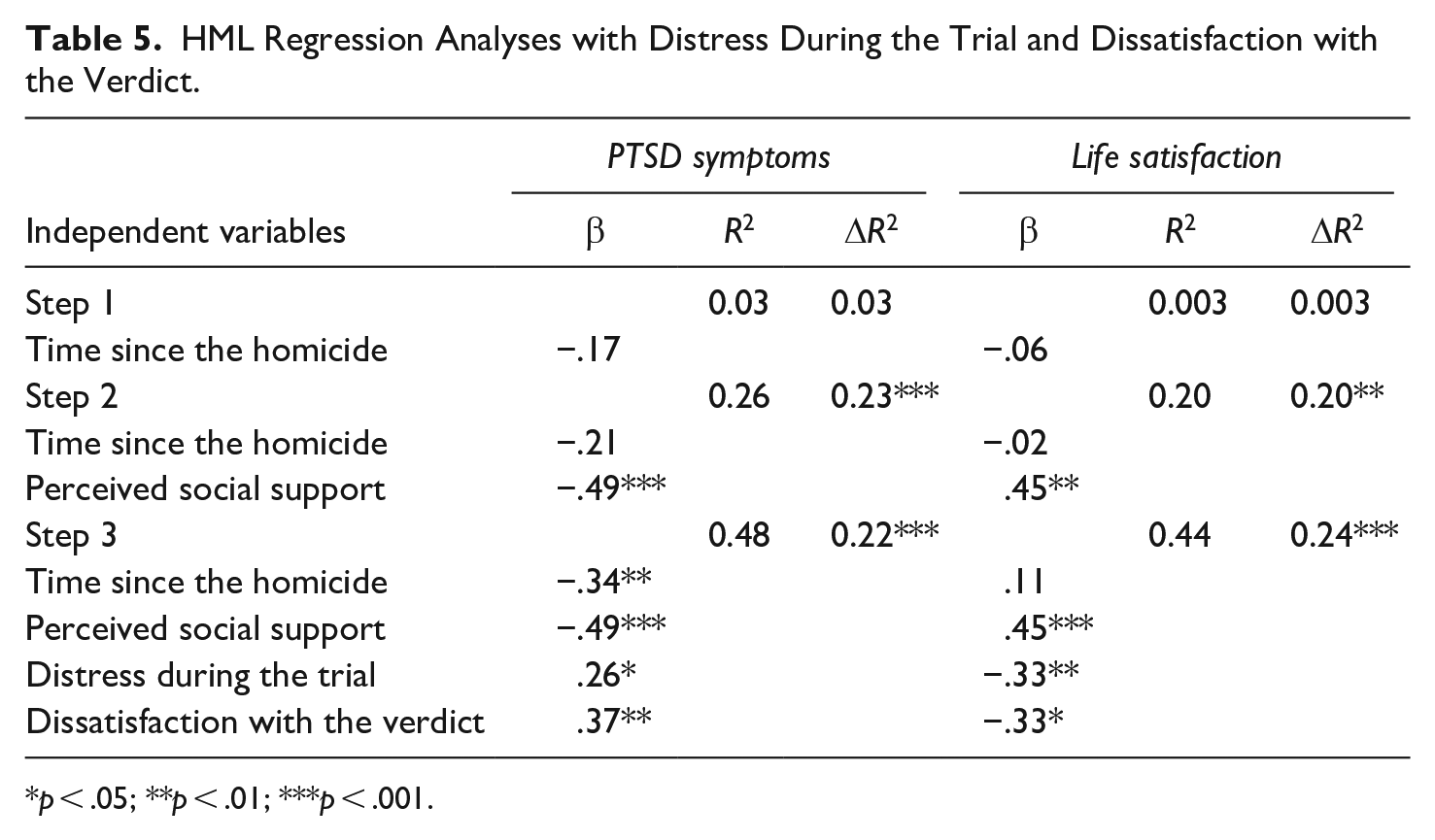
p < .05; **p < .01; ***p < .001.
Discussion
The first objective of the current study was to better understand the differences, in terms of PTSD symptoms and life satisfaction, between HBI who attended a trial, and those who did not. The second objective was to examine whether trial attendance moderated the relationship between PSS, PTSD symptoms and life satisfaction among all HBI when controlling for time since the homicide. Finally, the third objective, concerning only HBI who attended a trial, was to examine whether trial-related factors were significantly associated with PTSD symptoms and life satisfaction above the contribution of PSS and time since the homicide.
Main Findings
Comparisons (between HBI who attended a trial and those who did not) reveal similar means in terms of PSS, PTSD symptoms, life satisfaction, and time since the homicide. Previous qualitative research has indicated that attending a trial can exacerbate the PTSD symptoms of HBI (e.g., Englebrecht et al., 2014; Metzger et al., 2015). Therefore, trial-related factors, such as perception of justice, might better explain the variation observed in PTSD symptoms and life satisfaction, given conclusions drawn from qualitative studies.
Results from the correlation matrix provide notable findings. While a positive association emerges between perception of justice and life satisfaction, this factor is not significantly associated with PTSD symptoms. Evaluating the fairness of the criminal justice system (CJS) appears to have a significant role in life satisfaction but a more complex one in PTSD symptoms. Subscale analyses show that informational justice (e.g., criminal justice workers explained the procedures thoroughly) is the only subtype of perception of justice significantly associated with fewer PTSD symptoms. Meanwhile, distributive (e.g., the outcome of the trial reflects the work or the effort of the criminal justice workers) and informational justice are both significantly associated with greater life satisfaction. These results align with qualitative studies emphasizing the importance of informational and distributive justice for HBI’s mental health (e.g., Alves-Costa et al., 2018; Stretesky et al., 2010; Thiel, 2016). Therefore, perceiving the trial outcome as fair and receiving adequate information both seem to have a critical role in the PTSD symptoms and life satisfaction of HBI.
Regarding distress during the trial, results indicate a positive association with PTSD symptoms and a negative one with life satisfaction. These findings highlight the distressing nature of trial attendance for HBI, with lingering effects on mental health. Qualitative studies on this matter have shown that exposure to graphic details or images related to the homicide can be extremely triggering for HBI (Reed & Caraballo, 2022).
As expected, dissatisfaction with the verdict is positively associated with PTSD symptoms and negatively associated with life satisfaction. These findings are consistent with qualitative studies linking dissatisfaction with the CJS to anger (e.g., Baliko & Tuck, 2008). They are also similar to previous research conducted on other populations, such as victims of sexual or physical assault and property crimes (Orth, 2002; Orth & Maercker, 2004).
Perceived social support (PSS) is negatively associated with PTSD symptoms and positively associated with life satisfaction, corroborating previous research among HBI (Rheingold & Williams, 2015), other bereaved individuals (Scott et al., 2020) and victims of various types of traumas (e.g., war, violent crimes, road accidents; Andrews et al., 2003; Gros et al., 2016; Holeva et al., 2001). Qualitative studies among HBI (e.g., Hannays-King et al., 2015; Wellman, 2014) similarly revealed that insufficient support, particularly from family, can worsen grief, and stress symptoms.
For the second objective of this study, moderation analyses indicate, for the first time to our knowledge, that the protective role of PSS for PTSD symptoms varies depending on trial attendance. Perceived social support is associated with fewer PTSD symptoms among HBI who attended a trial, but not among those who did not. These findings underscore the crucial importance of social support for HBI participating in a trial, regardless of the time since the homicide. The trial experience may enhance the protective effect of social support, potentially by fostering opportunities for connection and emotional expression in the presence of validating support networks. Being surrounded by friends and family during the trial can offer HBI the opportunity to share, reflect and process their trauma, resulting in meaningful emotional support. Furthermore, these findings align with qualitative studies highlighting the value of support from victim advocates and support groups. For instance, Metzger et al. (2015) reported that HBI found support groups beneficial for expressing emotions and reducing isolation. HBI also expressed the desire for a victim advocate to accompany them throughout the criminal justice proceedings. The systematic review of Connolly and Gordon (2015) affirmed the significance of such resources in helping HBI cope with their loss. Shared experiences during a trial, whether with loved ones or support professionals, appear beneficial for the association between PSS, PTSD symptoms, and life satisfaction, even years after the homicide. The moderating effect of trial attendance on PTSD symptoms may help explain inconsistencies in the existing literature regarding the relationship between PSS and PTSD symptoms, as prior studies did not have accounted for trial attendance.
In examining the third objective (only on HBI who attended a trial), hierarchical multiple linear regression analyses reveal that trial-related factors (perception of justice, distress during the trial and dissatisfaction with the verdict) all explain a unique and important proportion of the variance in PTSD symptoms and life satisfaction, above and beyond the contribution of PSS and time since the homicide. These results add interesting data to a very limited field exploring the associations between trial-related factors, PTSD symptoms and life satisfaction in HBI. Specifically, a lack of perceived justice and the presence of distress during the trial and dissatisfaction with the verdict appear to exacerbate symptoms even when accounting for established predictors, such as PSS. Interestingly, while perception of justice is not significantly associated with PTSD symptoms in the correlation matrix, this variable is significant in the regression models, suggesting that PSS and time since the homicide obscure this relationship. Future studies should consider PSS and time since the homicide when investigating the contribution of perception of justice to the PTSD symptoms and life satisfaction of HBI.
Theoretical and Clinical Implications
This study highlights trial attendance as a specific and impactful stressor for HBI. The associations between trial attendance and PSS suggest that maximizing PSS is essential, particularly for HBI attending a trial. In the CJS, criminal justice workers could better assess the availability and quality of the social resources of HBI. They could also encourage trial attendance with supportive individuals who are able to provide positive support and validation. Socially, victim support organizations could also provide valuable sources of support during the trial. In clinical settings, it appears that assessing and strengthening PSS of HBI could be a key therapeutic target. Mental health professionals could also pay particular attention to HBI who do not attend trial, as they may lack situational opportunities to benefit from social support. This could include, for example, encouraging disclosure, and processing of the traumatic memories, even outside of legal contexts, to foster recovery.
This study also underscores the psychological burden of specific trial-related factors experienced by HBI. More specifically, it shows just how a lack of perception of justice, in particular distributive and informational justice, can be prejudicial for HBI who attend a trial. Allowing HBI to be informed about the process and to express their feelings and expectations of the court work and decision could be very beneficial. Therefore, criminal justice workers and victim advocates could be provided with training so they could explain the procedures thoroughly to HBI, communicate details in a timely manner, tailor communication to the specific needs of the bereaved and help them deal with the outcome of the trial. Support groups could also focus on the perception of justice of HBI and allow them to express their emotions and expectations toward the criminal process and the verdict. In a psychotherapeutic context, these results encourage mental health professionals to better assess the perception of justice of HBI, to verify the facts and interpretations at the source of these perceptions and to better measure the role of these perceptions in their PTSD symptoms and life satisfaction. For example, contextual strategies constitute an approach that recognizes the injustices that HBI have experienced after their loss and during the criminal justice process. Results have shown that these strategies have helped HBI find a balance between remembering the victim, reorganizing their family’s functioning and creating new long-term plans (Connolly & Gordon, 2015).
As distress during the trial is associated with the PTSD symptoms and life satisfaction of HBI years after the trial, it seems crucial to develop training for criminal justice workers to help them provide better support for HBI during this process. For example, preparing criminal justice workers to be mindful of the effects of the criminal evidence on HBI (e.g., informing HBI in advance of the evidence to be used, its purpose and when it will be presented, keeping graphic evidence out of sight, taking a break during the testimonial or while witnessing the evidence) could be very much appreciated and helpful (Gekoski et al., 2013). Indeed, it could help HBI prepare for and go through with the trial, and therefore reduce their distress during the trial and also for years after. In psychotherapeutic settings, mental health professionals should be very well informed about the specifics of a criminal trial and the technical procedures involved, so that they can better pass on valuable information to the HBI. They could also help HBI learn more effectively to regulate their emotions and maximize their adaptive resources when being exposed to disturbing details during the trial. Offering more psychological counseling during the trial could also be very helpful, as suggested by Orth (2002) regarding rape survivors and victims of nonsexual assault (such as robbery and bodily harm).
Dissatisfaction with the verdict is prevalent among HBI and is strongly associated with greater PTSD symptoms and reduced life satisfaction. Social measures could enhance satisfaction with the verdict. The results from the study of Regehr and Alaggia (2006), conducted with rape survivors, suggest that an increase in the criminal justice workers’ empathy could increase the satisfaction of HBI with the system and their willingness to accept the outcome of the trial. Moreover, Lens et al. (2015) revealed that delivering an impact statement in court would provide victims of violent crime with a chance to speak directly to the judge, the jury and the offender. However, this opportunity is not always associated with a positive therapeutic effect. Indeed, it can leave many HBI with painful feelings of frustration and disappointment (Englebrecht et al., 2014). In psychotherapeutic settings, mental health professionals could help HBI to better understand the verdict in the light of legal and social contingencies, to make sense of it, to more effectively manage their anger, hatred or despair resulting from it and to better manage their day-to-day lives to regain satisfaction with life despite their loss.
Limitations and Future Avenues of Research
The current study is not without limitations. Firstly, given that this is a sample composed mostly of educated, Western women, it may not be representative of all HBI. Also, our recruitment strategy (via organizations) might have led to a sample of HBI that is more distressed than those who are not seeking care. It could explain the higher prevalence rates of PTSD in our sample when compared to previous studies. To overcome this limitation and recruit more diversified and representative samples, future research could contact participants with the help of government departments. For example, J. A. Wemmers (2013) recruited their participants with the help of the Ministry of Justice in Quebec. Using this recruitment strategy, all individuals whose cases entered the criminal court and went further than the police could be invited to participate. Therefore, individuals who are not seeking care as well as individuals who are already connected to care would be considered, and the sample would therefore be more representative of the population of HBI. However, contact with certain government departments can be infrequent and difficult to establish.
Secondly, the cross-sectional design of this study also offers no information about the directionality and causal nature of the associations found. Therefore, the prospective relationships between trial attendance, trial-related factors, PSS, PTSD symptoms and life satisfaction could not be assessed. Future research could opt for a longitudinal design to overcome this limitation. For example, such studies could measure the distress of HBI at various phases of the trial to better understand the procedures most strongly associated with higher distress (e.g., exposure to graphic or disturbing details about the homicide).
Thirdly, although validated self-report measures are used, the absence of structured clinical interviews (e.g., CAPS; Blake et al., 1990) limits diagnostic precision. Indeed, self-reported measures of PTSD can overestimate prevalence, as suggested by prior research (Engelhard et al., 2007).
Fourthly, pre-homicide factors (e.g., prior traumas) and additional post-homicide factors (e.g., self-efficacy, resilience) are not assessed in the present study. These variables could influence PTSD symptoms and life satisfaction. According to Cieslak et al. (2008), low perceived coping ability can increase distress, while resilience could foster posttraumatic growth (Baliko & Tuck, 2008). Future research should explore these dimensions to refine our understanding of HBI recovery.
Conclusion
This study aims to clarify our understanding of a specific stressor experienced by HBI, that is, trial attendance, and how it influences their PTSD symptoms and life satisfaction. This was achieved by illustrating that, when controlling for time since the homicide, trial attendance moderates the relationship between perceived social support, and PTSD symptoms. Indeed, perceived social support is significantly associated with PTSD symptoms of HBI who attended a trial, but not for HBI who did not. The results also highlight the unique contribution of trial-related factors in shaping the PTSD symptoms and life satisfaction of HBI when accounting for well-known and established variables in the literature, that is, perceived social support. Indeed, this study shows how the inclusion of trial-related factors explains additional variance in the PTSD symptoms and life satisfaction of HBI.
Interventions in the criminal justice system that address trial-related factors and perceived social support appear to be essential for alleviating PTSD symptoms and enhancing life satisfaction among HBI. This population could also benefit from a distinct approach in psychotherapeutic settings. Future research should continue to investigate trial attendance and trial-related factors to further elucidate the nuances in the PTSD symptoms and life satisfaction of HBI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fonds de Recherche du Québec-Société et Culture under Grant 327830. This project was approved by the research ethics board of the University of Quebec in Montreal (#2021-3318), and an informed consent form was signed by all participants.