
Abstract
Background:
Attention Deficit Hyperactivity Disorder (ADHD) and Specific Learning Difficulties (SLD) are both associated with attentional and cognitive difficulties. This study examined the extent to which the cognitive impairments could be consequences of elevated levels of inattention and hyperactivity/impulsivity.
Method:
Secondary analysis was conducted on data from four groups selected from the Centre for Attention, Learning, and Memory, a neurodivergent cohort of children aged 5 to 18 years with a mean age of 9 years : children with ADHD only (n = 70), learning difficulties only (n = 406), ADHD with learning difficulties (n = 128), and a comparison group (n = 166). Covariance analyses examined whether any differences in basic cognitive skills and higher executive functions between the neurodivergent and comparison groups could result from variations in inattention and hyperactivity/impulsivity.
Results:
Irrespective of ADHD status, children with learning difficulties had low scores in short-term memory, working memory, sustained attention, processing speed, set sequencing, and set shifting. These cognitive deficits largely persisted when inattention and hyperactivity/impulsivity were covaried. In contrast, the ADHD only group performed at age-appropriate levels on measures of verbal short-term memory, verbal and visuospatial working memory, processing speed, and sustained attention. Their difficulties with set sequencing and visuospatial short-term memory were accounted for by inattention and hyperactivity/impulsivity, whereas their challenges with set shifting were independent of these attentional behaviors.
Conclusions:
The results point to distinct neurodevelopmental pathways to cognitive functioning for children with learning difficulties and those with ADHD. The independence of learning-related cognitive skills from levels of inattention and hyperactivity/impulsivity in children with learning difficulties either with or without ADHD suggests they represent the core deficits that underlie their learning difficulties. The limited cognitive challenges of children with ADHD without learning difficulties may be consequences of their elevated levels of attentional behaviors. Understanding the cognitive and learning profiles of children with ADHD and learning difficulties vital for identifying optimal intervention and support strategies that address their individual needs.
Introduction
Attention Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterized by high levels of inattentive and hyperactive/impulsive behavior (American Psychiatric Association Division of Research, 2013). Inattention involves difficulties in maintaining attention to tasks, distractibility, and forgetting task-related information. Hyperactivity and impulsivity are reflected in restless and distractible behaviors such as fidgeting, excessive physical and verbal activity, difficulty waiting one’s turn, and interrupting others. Specific Learning Difficulties (SLD) is a neurodevelopmental condition characterized by low levels of progress in reading and/or mathematics (American Psychiatric Association Division of Research, 2013). Between 19% to 44% of children with ADHD also meet the criteria for SLD (Carroll et al., 2005; Pastor & Reuben, 2008; Visser et al., 2020), and 28% to 42% of children with SLD have clinically significant levels of ADHD symptoms (Kibby et al., 2021; Operto et al., 2021; Parhiala et al., 2015; Willcutt & Petrill, 2023). Children with both ADHD and SLD typically have levels of inattention and hyperactivity/impulsivity similar to those observed in children with ADHD only, but which are greater than those of children with SLD only (Kibby et al., 2021; Willcutt & Petrill, 2023).
The attentional behaviors of inattention and hyperactivity/impulsivity are by no means limited to children with ADHD and learning difficulties. Higher levels of inattention are associated with lower levels of academic achievement in the general population (de Zeeuw et al., 2017; Salla et al., 2016; Tan et al., 2022). Levels of both hyperactivity and impulsivity are also elevated in Autism Spectrum Disorder, Conduct Disorder, and Oppositional Defiant Disorder (Rong et al., 2021; Rowe et al., 2010). This has led to proposals suggesting that attentional behaviors are best understood as functionally distinct transdiagnostic dimensions in neurodivergent populations (Astle et al., 2022; Michelini et al., 2024).
While extensive evidence has linked inattention to lower academic achievement, hyperactivity/impulsivity is more weakly associated with learning outcomes. Longitudinal studies of population cohorts show that increasing levels of inattention from childhood through adolescence predict lower performance in reading and mathematics, with academic impacts such as an increased likelihood of failing to obtain a high school diploma during adolescence (Breslau et al., 2010; Pingault et al., 2014; Sayal et al., 2015). Pingault et al. (2011) reported that changes in levels of hyperactivity/impulsivity across the early and middle childhood period did not predict educational achievement in adolescence once the developmental trajectories of inattention were taken into account. Studies examining the genetic pathways similarly distinguish the impacts of these two dimensions of attentional behaviors on academic outcomes. In a study of 5,000 twin pairs, Liu et al. (2019) found that genetic factors contributing to the developmental course of increased inattention symptoms from early to middle childhood are linked to lower academic performance in adolescence. Consistent with this, data from a large twin study by de Zeeuw et al. (2017) revealed both cross-sectional and longitudinal associations between ADHD symptoms and academic attainment from ages 7 to 12. Inattention but not hyperactivity/impulsivity significantly predicted educational achievement in both cross-sectional and longitudinal analyses. The relationship between inattention and learning was independent of shared genetic or environmental factors.
The cognitive challenges in children with ADHD and SLD overlap considerably (Lonergan et al., 2019; Loyer Carbonneau et al., 2021; Peng, Wang, et al., 2018; Peng et al., 2022; Pievsky & McGrath, 2018). Both groups experience difficulties with the processing of verbal and nonverbal information (Becker et al., 2021; Operto et al., 2021), as well as challenges in the executive functions of working memory, inhibitory control, and shifting between attentional sets (Crisci et al., 2021; Huang et al., 2016; Peng et al., 2013). Their abilities to sustain attention over extended periods under conditions of relatively low cognitive demands are also impaired (Slobodin et al., 2018; Tsal et al., 2005).
While elevated levels of inattention, hyperactivity/impulsivity, and cognitive difficulties are consistently observed in both ADHD and SLD, data from many studies remain limited in scope. Recent studies by Crisci et al. (2021), Faedda et al. (2019), and Operto et al. (2021), for example, each included fewer than 50 children per neurodivergent group (ADHD, learning difficulties, and co-occurring ADHD and learning difficulties). Cognitive assessments in other studies with larger neurodivergent samples often include executive function measures but lack more basic processing tasks needed to identify the specific sources of deficits in higher-level tasks (Huang et al., 2016; Kibby et al., 2021; Willcutt & Petrill, 2023).
The present study extends previous studies by drawing on a large sample of children who completed a broad range of assessments covering cognition, learning, and attentional behavior. Participants were selected from the Centre for Attention, Learning, and Memory (CALM; Holmes et al., 2019), a neurodivergent cohort that included a high proportion of children with ADHD and learning-related difficulties.
There were four groups: children with ADHD; children with learning difficulties (selected on the basis of low scores on standardized academic assessments of reading and/or mathematics); children with both ADHD and learning difficulties; and a comparison group of children with no known neurodevelopmental conditions.
Participants completed assessments of cognitive skills linked to educational attainment. Levels of inattentive and hyperactive/impulsive behaviors were rated by parents. The measures were drawn from psychometric test batteries widely used in clinical practice and research on ADHD and SLD. The cognitive assessments included measures of processing speed and two executive functions: working memory and set shifting, both of which are linked to academic achievement. Working memory is a multi-component, limited capacity system providing temporary storage and processing of information (Baddeley & Hitch, 1974; Cowan, 2022; Hitch et al., 2024). Working memory skills are closely associated with children’s attainment in both reading (Kasper et al., 2012; Peng & Fuchs, 2016) and mathematics (Allen et al., 2019; Friso-van Den Bos et al., 2013; Peng, Barnes, et al., 2018). Set shifting involves the volitional shifting of attention between different task content (Miyake et al., 2000) and is moderately associated with attainment levels in reading and mathematics (Peng et al., 2022; Peng, Wang, et al., 2018; Yeniad et al., 2013). It has also been reported to be impaired in children with ADHD and SLD (Huang et al., 2016; Kibby et al., 2021; Peng et al., 2022; Pievsky & McGrath, 2018)
Investigations of potential links between attentional behaviors and cognitive functioning have primarily focused on neurotypical children rather than individuals with ADHD or SLD. High levels of inattentive symptoms have been shown to be associated with lower performance on short-term memory, working memory, set shifting, processing speed, and phonological awareness tasks (Alloway et al., 2009; Gathercole et al., 2008; Plourde et al., 2018; Sørensen et al., 2012). Longitudinal studies have established links between early elevated levels of inattention and hyperactivity/impulsivity, and later difficulties in executive functions. For example, Friedman et al. (2007) found that inattentive and hyperactive/impulsive behaviors assessed repeatedly from ages 7 to 14 years were consistently associated with concurrent and later difficulties in working memory and set shifting at each timepoint across this developmental period. Similarly, Metcalfe et al. (2013) reported that higher levels of attentional behaviors at age 3 years predicted later cognitive difficulties, including impairments in working memory and processing speed assessed at age 6. These findings raise the possibility that high levels of attentional behaviors may interfere with children’s ability to engage with and benefit from structured learning situations (Willcutt, 2020). For example, high levels of distractibility may reduce attention to instructions or the ability to maintain attentional focus during learning activities, while impulsivity may lead to skipping essential steps in complex tasks or acting without thinking. Specific cognitive processes that could plausibly be disrupted by elevated attentional behaviors include phonological recoding during early stages of learning to read (Hulme & Snowling, 2013) and the storage of interim calculations in mental arithmetic (Friso-van Den Bos et al., 2013). It is possible that similar downstream consequences of elevated levels of inattentive, hyperactive, and impulsive behavior may also contribute to the cognitive challenges observed in children with ADHD and SLD.
This pre-registered study (https://osf.io/twe6r) involved secondary analysis of data from the CALM cohort (Holmes et al., 2019). The core cohort consisted of children identified by practitioners in education and health as having difficulties in attention, learning, and/or memory. The ADHD group was selected based on reported ADHD diagnoses at referral to the CALM. Although the cohort included a large proportion of children reported by practitioners as having learning difficulties, the majority did not have clinically confirmed diagnoses of SLD. This in part reflects variability in local systems for identifying and assessing children who may meet the diagnostic criteria in England, with a minority of children receiving in-school support for learning difficulties undergoing assessments by trained specialist assessors (largely privately funded by the family) that are required for diagnoses of dyslexia or dyscalculia.
Based on previous research (e.g., Crisci et al., 2021; Huang et al., 2016; Kibby et al., 2021; Trane & Willcutt, 2023), it was hypothesized that three neurodivergent groups—children with ADHD only, learning difficulties only, and co-occurring ADHD and learning difficulties—would show higher levels of cognitive difficulties, learning challenges, and attentional behaviors of ADHD than those in the comparison group. The study further explored the extent to which the known difficulties in cognitive functioning in each of the three neurodivergent groups could be accounted for by their co-occurring elevated levels of attentional behaviors. The central aim was not to isolate entirely “pure” cognitive skills from attentional difficulties, but rather to examine the extent to which group differences in cognitive performance between each neurodivergent group and the comparison group could be explained by elevated levels of attentional behaviors. This novel question was addressed by covarying levels of parent-rated inattention and hyperactivity/impulsivity in the comparison of cognitive performance across groups, which sought to statistically adjust for variability in these two attentional behaviors at a single time point. Group differences eliminated when these measures of attentional behavior were taken into account would provide evidence consistent with the speculation that reduced attentional focus and increased hyperactive/impulsive behavior interfere with the cognitive processes needed to complete these tasks in some or all of the neurodivergent groups.
Method
Participants
Data were collected from approximately 1,000 children aged 5 to 18 years attending the CALM research center between 2014 and 2021 (Holmes et al., 2019). Of these, 805 children with difficulties relating to attention, learning, and/or memory were identified via multiple referral pathways include specialist teachers, clinical psychologists, pediatricians, and speech and language therapists (the CALM 800). A second cohort of 178 children (the CALM 200 cohort), drawn from the same school population as the CALM 800 cohort, was recruited to serve as the comparison group. Children in the CALM 200 cohort had no reported difficulties in attention, learning, and/or memory. Parents or primary caregivers provided informed written consent and children provided verbal assent. Ethical approval was granted by the National Health Service (NHS) Health Research Authority NRES Committee East of England (REC approval reference 13/EE/0157).
Group Selection
Three neurodivergent groups were selected from the CALM 800 cohort—ADHD, learning difficulties, and ADHD and co-occurring learning difficulties. Children in the CALM cohort who were reported as having ADHD by their referring agents were selected for participation in the study. ADHD diagnosis in the UK is based on assessments conducted by specialist child and adult psychiatrists, pediatricians, and qualified healthcare professionals trained in diagnosing ADHD. These assessments follow standard diagnostic criteria, including clinical presentation, multi-informant observations, and direct assessments, in adherence to international diagnostic standards for ADHD (American Psychiatric Association Division of Research, 2013; World Health Organization, 1992). Diagnoses for children reported as having ADHD in the CALM clinic were made by trained assessors based in regional NHS ADHD clinics, consultant child psychologists or psychiatrists working in other NHS services, or suitably qualified professionals in private practice. CALM participants were recruited from multiple counties in the East of England through referrals from a wide range of professionals across multiple agencies, including education, child and adolescent mental health services, and speech and language therapy services (Holmes et al., 2019). UK data confidentiality laws precluded access to the original diagnostic records without separate ethical applications to the tens of ethics committees serving these regions. ADHD diagnoses were identified either directly by ADHD clinicians and assessors referring children to the CALM clinic or by practitioners in education and healthcare services who had been informed of the diagnosis by ADHD assessors. The ADHD status of each child was confirmed by the caregiver during the initial assessment session at the CALM clinic. Caregivers also reported whether the child was receiving stimulant medication for ADHD. However, further details regarding the prescribed medication, dosage, and frequency of dosing were not available.
To identify individuals with learning difficulties from the CALM cohort for the current study, children scoring at or below the 15th percentile (standard score ≤85) on either a reading or mathematics test (or both) were selected to form a learning difficulties group (see also, Galuschka & Schulte-Körne, 2016; Geary et al., 2007; von Wirth et al., 2021; Vukovic et al., 2010). This criterion corresponds to a less severe level of underperformance than the 1.5 standard deviation (SD) criterion (corresponding to a standard score of 77.5 or below) recommended for the clinical diagnosis of SLD in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; American Psychiatric Association Division of Research, 2013). The term “learning difficulties” is used in a diagnostically neutral sense as a functional description of low performance on standardized measures of reading and mathematics at the time of testing. Although it is distinct from a formal clinical diagnosis of learning difficulties, some of the children did have reported diagnoses of either dyslexia (n = 41) or dyscalculia (n = 1).
A total of 198 children with a reported ADHD diagnosis from the CALM 800 cohort were selected for this study. These children were divided into two subgroups based on their scores on subtests of the Wechsler Individual Achievement Test II (WIAT-II; Wechsler, 2005). The ADHD only group comprised 70 children (18 females, Mage = 10.48, SDage = 2.86, n = 37 currently receiving medication) with a reported ADHD diagnosis and age-standardized scores of 86 or higher on both the Single Word Reading and Numerical Operations subtests of the WIAT-II(Wechsler, 2005). No additional co-occurring diagnoses were reported for any participants.
The ADHD with learning difficulties group consisted of of 128 children (27 females, Mage = 10.06, SDage = 2.47, n = 70 currently receiving medication). Participants in this group had a reported diagnosis of ADHD and scored 85 or below on the Single Word Reading or Numerical Operations subtests of the WIAT-II (Wechsler, 2005). Among these, 16 children (0 female, Mage = 9.56, SDage = 2.92) scored below the cut-off on the reading subtest, 45 children (10 females, Mage = 10.13, SDage = 2.44) scored below the cut-off on the mathematical subtest, and 67 children (17 females, Mage = 9.31, SDage = 2.33) scored below the cut-off on both subtests. Four children were reported to have dyslexia (three females) and none with dyscalculia.
The learning difficulties only group consisted of 406 children (149 females, Mage = 9.27, SDage = 2.11) who scored at or below 85 on the Single Word Reading or Numerical Operations subtests of the WIAT-II (Wechsler, 2005). Among these, 74 children scored below the cut-off on the reading subtest (22 females, Mage = 8.31, SDage = 1.92), 112 children scored below the cut-off on the mathematical subtest (44 females, Mage = 9.29, SDage = 2.20), and 220 children scored below the cut-off on both tests (83 females, Mage = 8.70, SDage = 2.08). Thirty-seven children were reported to have a diagnosis of dyslexia (12 females), and one of dyscalculia (1 female).
The comparison group comprised 166 children drawn from the CALM 200 cohort (72 females, Mage = 9.99, SDage = 2.35). Participants were selected based on standard scores of 86 or above on the Single Word Reading and Numerical Operations subtests of WIAT-II (Wechsler, 2005). They had no reported difficulties in attention, learning, and/or memory, and had not received a neurodevelopmental diagnosis. The age distributions for each group are shown in Table 1.
Distribution of Participants by Age and Group.
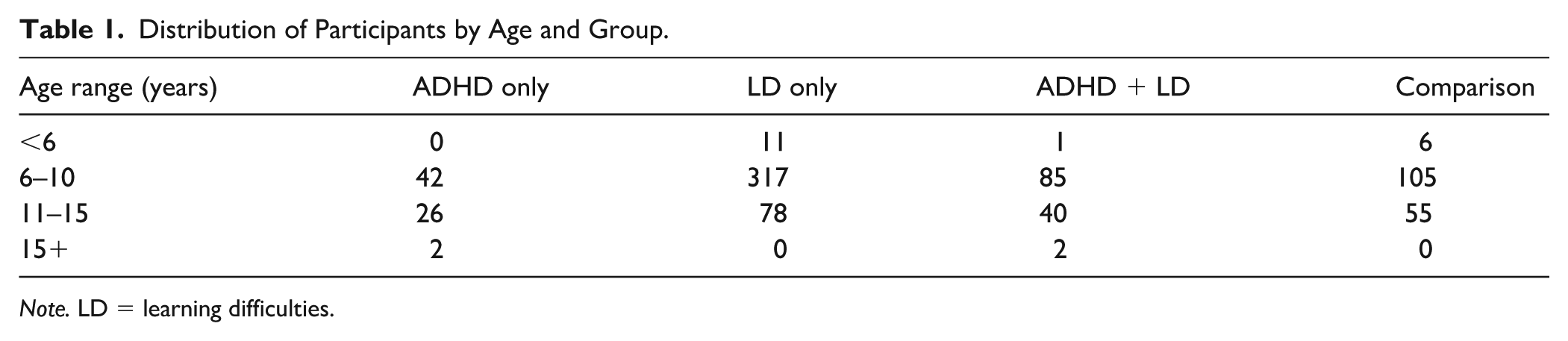
Note. LD = learning difficulties.
Socioeconomic status was evaluated by the Index of Multiple Deprivation (IMD). It is a relative measure that rank neighborhoods in England according to their level of deprivation relative to that of other areas, with 1 rank most deprived to 32,844th rank least deprived(Department for Communities and Local Government, 2015). The IMD ranks for the four groups were: ADHD only (M = 18,764, SD = 9,553); learning difficulties only (M = 20,328, SD = 7,811); ADHD with learning difficulties (M = 18,886, SD = 8,891); comparison (M = 20,203, SD = 8,239). An analysis of variance (ANOVA) comparing deprivation ranks of the four groups was nonsignificant, F(3, 766) = 1.52, p = .20.
All children completed assessments of cognition, learning, and attending behavior related to ADHD symptoms. Additional assessments of processing speed (Motor Speed and Visual Scanning) and set shifting were administered to participants aged 8 years and older: 54 children with reported ADHD only (16 females, Mage = 11.41, SDage = 2.55), 102 children with co-occurring ADHD and learning difficulties (23 females, Mage = 10.83, SDage = 2.22), 284 children with learning difficulties only (110 females, Mage = 10.25, SDage = 1.73), and 128 children from the comparison group (56 females, Mage = 10.94, SDage = 1.76).
Measures
Full details of testing materials and procedures are described by Holmes et al. (2019).
Short-Term and Working Memory
Participants completed four subtests of the standardized Automated Working Memory Assessment (AWMA; Alloway, 2007; Alloway et al., 2006; Nadler & Archibald, 2014): Digit Recall (verbal short-term memory), Dot Matrix (visuospatial short-term memory), Backward Digit Recall (verbal working memory), and Mr. X (visuospatial working memory). Test–retest reliability coefficients are .89 for Digit Recall, .84 for Dot Matrix, .86 for Backward Digit Recall, and .84 for Mr. X (Alloway, 2007; Alloway et al., 2008). The number of correct trials for each subtest was converted into age-standardized scores (M = 100, SD = 15), with higher scores indicating better performance.
Sustained Attention
Sustained attention was assessed by the Barking/Vigil Task, a subset of the Test of Everyday Attention for Children (TEA-Ch2; Manly et al., 2017). Children younger than 8 years completed the Barking task, while those aged 8 years and older completed the Vigil task. In the Barking task, participants were asked to count the number of repeated auditory dog-bark stimuli presented in each trial. In the Vigil task, participants counted the number of repeated auditory tone stimuli. Split-half reliability for this task is .55, and test–retest reliability coefficients range from .64 to .76 (Manly et al., 2001, 2017). The number of correct trials was converted to an age-scaled score and used for analysis (M = 10, SD = 3), with higher scores reflecting greater response accuracy.
Set Shifting
The Trail Making test from the Delis–Kaplan Executive Function System (D-KEFS; Delis et al., 2001) was completed by children aged 8 years and older. Measures of Number-Letter Sequencing, Letter sequencing, and Number sequencing were administered. The Number-Letter Sequencing task was the higher-order component that assessed set shifting under conditions of high executive demand. More basic processing skills were measured by Number sequencing and Letter sequencing tasks that did not require shifting between categories. Internal consistency for the Trail Making Test ranges from .57 to .79, and the test–retest reliability coefficient is .51 (Delis et al., 2001). Completion times were recorded, converted to scaled scores, and used in the analysis (M = 10, SD = 3). Higher scores on this task reflected faster task completion.
Processing Speed
Processing speed was assessed by the Visual Scanning and Motor Speed tests of the D-KEFS (Delis et al., 2001). Test–retest reliability is .50 for Visual Scanning and .82 for Motor Speed (Delis et al., 2001). Completion times converted to scaled scores (M = 10, SD = 3) were analyzed in the study. Higher scores denote faster task completion.
The Simple Reaction Time subtest of the TEA-Ch2 (Manly et al., 2017) provided a measure of processing speed. Split-half reliability for this task is .91 (Manly et al., 2017), and the test–retest reliability coefficient is .73 (Manly et al., 2001, 2017). Average response times were recorded and converted to scaled scores (M = 10, SD = 3). Higher scores reflect faster response times.
Behavior
The Inattention and Hyperactivity/Impulsivity subscales of the Conners 3-Parent Rating Scale Short Form (Conners, 2008) were used to assess attentional behaviors associated with ADHD. The internal consistency for the Conners 3–Parent Rating Scale Short Form ranges from .85 to .92, and its test–retest reliability ranges from .71 to .98 (Conners, 2008). Although test–retest reliability data for the subscales used in the present study were unavailable, previous research on the Revised Conners’ Parent Rating Scale has reported test–retest reliabilities of .78 for the Inattention subscale and .71 for the Hyperactivity/Impulsivity subscale (Conners et al., 1998). T-scores were computed for each subscale (M = 50, SD = 10) and used in the analysis. Higher scores indicated greater levels of attentional behaviors associated with ADHD.
Learning
The Single Word Reading and Numerical Operations subtests of the WIAT-II (Wechsler, 2005) assessed academic progress. For children aged 6 to 19 years, the test–retest reliability for the Single Word Reading subtest ranges from .95 to .98, and the split-half reliability ranges from .95 to .99. For the Numerical Operations subtest, the test–retest reliability ranges from .86 to .91, and the split-half reliability ranges from .85 to .95 (Wechsler, 2005). The number of correct responses was converted to standard scores (M = 100, SD = 15) and used in the analysis, with higher scores reflecting greater reading and mathematical abilities.
Analysis Plan
Primary Analyses
To maintain the variability of this neurodiverse sample, data were analyzed without excluding univariate or multivariate outliers, following the pre-registration plan (https://osf.io/twe6r). For completeness, a systematic check for univariate outliers was conducted across all outcome variables using the 1.5 × interquartile range. The large majority of variables had no univariate outliers and for those that did, the proportion was less than 5% (Table 1, Supplemental Material). Skewness and kurtosis statistics provide further distributional information for individual measures and potential deviations from normality. For the aggregated sample in this study (Table 1, Supplemental Material), most skewness values fell within the conventional range of −0.5 to 0.5, indicating approximately symmetric distributions consistent with normality (Bulmer, 1979). Backward Digit Recall, Barking/Vigil, and Numerical Operations showed moderate positive skewness, while Visual Scanning, Motor Speed, and Conners Inattention Subscale exhibited moderate to high negative skewness. Kurtosis values were below 3 (indicating a low likelihood of extreme outliers for all measures) for measures with the exception of Backward Digit Recall, Mr. X, Visual Scanning, and Motor Speed. Skewness and kurtosis values for each group were provided in Tables 2 to 5 (Supplemental Material).
The primary analyses were conducted in accordance with the study pre-registration. Parametric analyses were performed using R version 4.3.1. A series of ANOVAs compared cognitive functioning, learning, and attentional behaviors across groups, followed by specific pairwise group comparisons. The Bonferroni correction yielded a significance threshold of p < .008 for multiple group comparisons. To explore the potential role of attentional behaviors in disrupting cognitive functioning essential for learning, pairwise group differences for significant group effects on cognitive functioning were further examined using analyses of covariance (ANCOVA). For each pairwise comparison, scores of inattention and hyperactivity/impulsivity were first entered simultaneously as covariates to examine their combined effect on group differences in cognitive skills. Subsequently, each score was entered individually as a covariate to assess its independent effect on cognitive performance across groups. Significant group differences that were eliminated after accounting for variation in levels of inattention or hyperactivity/impulsivity would suggest that the observed differences in cognitive performance may be explained by elevated levels of these attentional behaviors.
Variance Inflation Factor (VIF) analyses were conducted using the car package in R to evaluate potential multicollinearity between the two covariates. All VIF values were below the commonly accepted threshold of 5, indicating acceptable levels of multicollinearity (Kutner et al., 2005). Values are shown in Table 6 of the Supplemental Material.
Further ANCOVAs investigated whether group differences on measures of higher-order cognitive abilities reflect differences in the lower-level basic processing components of the tasks (Peng et al., 2013; Trane & Willcutt, 2023). Measures of basic processing were included as covariates in group comparisons of higher-order cognitive tasks. For verbal and visuospatial working memory measures (Backward Digit Recall, Mr. X), the domain-specific verbal or visuospatial measure was used as the covariate for the respective basic processing task (Digit Recall or Dot Matrix). For the set shifting task (Number-Letter Sequencing), the composite score of the individual number sequencing and letter sequencing tasks (Number and Letter Sequencing Composite Score) was included as a covariate.
Additional ANOVAs evaluated the influence of ADHD medication on cognitive, learning, and behavioral outcomes across ADHD subgroups: ADHD only with medication, ADHD only without medication, ADHD with learning difficulties with medication, and ADHD with learning difficulties without medication. Significant group differences were followed up using two-sample t-tests comparing each ADHD subgroup to the comparison group, and one sample t-tests comparing each subgroup to the age-normed mean, to assess the degree of difficulty experienced by the neurodivergent groups.
Missing Values
The naniar package in R was used to summarise the proportion of missing data across the full analytic sample. Details of the proportion of missing data per variable are reported in Table 1 of the Supplemental Material. Levels of missing data ranged from 15% to 27% across variables. The underlying causes of missingness were not systematically recorded in the CALM dataset.
Missing data were imputed using predictive mean matching via the mice package in R (van Buuren & Groothuis-Oudshoorn, 2011). This method has been shown to yield reliable estimates under conditions of mild to moderate skewness with a sufficiently large sample size (N ≥ 500; Kleinke, 2017). Missing data were imputed for tasks administered to the three neurodivergent groups (n = 604, Mage = 9.67, SDage = 2.34): working memory (Backward Digit Recall, Mr. X) and short-term memory (Digit Recall, Dot Matrix), sustained attention (Barking/Vigil), one processing speed task (Simple Reaction Time), behaviors (Conners Inattention Subscale, Conners Hyperactivity/Impulsivity Subscale), and learning measures (Single Word Reading, Numerical Operations). A separate imputation was performed for tasks administered to children aged 8 years and above (n = 440, Mage = 10.61, SDage = 1.97), focusing on measures related to processing speed (Visual Scanning and Motor Speed) and two components of set shifting (Number and Letter Sequencing Composite Score, Number-Letter Sequencing). Imputations were separately carried out for each neurodivergent group. Two additional sets of multiple imputations were implemented to address missing data for children in the comparison group: one for tasks administered to all children (n = 166), and another for tasks administered to children aged 8 years and over (n = 128). For all groups, data were imputed if a participant had 20% or less missing value.
Results
Descriptive statistics for all measures are presented in Table 2. Significant group differences were observed for all measures in the ANOVAs. Detailed results of pairwise group comparisons using ANOVAs and ANCOVAs, with inattention and hyperactivity/impulsivity included as individual covariates, are provided in Tables 3 to 8. Additional results are presented in the Supplemental Material. The outcomes of the ANCOVAs, which include inattention and hyperactivity/impulsivity as covariates, are reported in Tables 7 and 8 (Supplemental Material).
Descriptive Statistics and Group Comparisons of Cognitive, Learning, and Attentional Behavior Measures.

Note. All values of p < .008 are shown in bold. All participants completed assessments of working memory, short-term memory, processing speed (Simple Reaction Time), and sustained attention. Only children aged 8 years and above completed measures of two additional processing speed tasks (Visual Scanning and Motor Speed) and set shifting.
Scores derived from basic number sequencing and basic letter sequencing scores.
Pairwise Group Comparisons (ADHD Only vs. Comparison) and Individual Covariate Analyses of Inattention and Hyperactivity/Impulsivity.

Note.All values of p < .008 are shown in bold.
Pairwise Group Comparisons (LD Only vs. Comparison) and Individual Covariate Analyses of Inattention and Hyperactivity/Impulsivity.

Note.All values of p < .008 are shown in bold.
Pairwise Group Comparisons (ADHD+LD vs. LD Only) and Individual Covariate Analyses of Inattention and Hyperactivity/Impulsivity.

Note.All values of p < .008 are shown in bold.
Pairwise Group Comparisons (ADHD+LD vs Comparison) and Individual Covariate Analyses of Inattention and Hyperactivity/Impulsivity.

Note.All values of p < .008 are shown in bold.
Pairwise Group Comparisons (ADHD Only vs. LD Only) and Individual Covariate Analyses of Inattention and Hyperactivity/Impulsivity.

Note.All values of p < .008 are shown in bold.
Pairwise Comparisons (ADHD Only vs. ADHD+LD) and Individual Covariate Analyses of Inattention and Hyperactivity/Impulsivity.

Note.All values of p < .008 are shown in bold.
The mean performance levels of the comparison group on cognitive and learning measures exceeded the age-expected levels defined by the age-normed mean from test standardization (Table 2). For instance, the comparison group scored approximately 0.5 standard deviations above the age-normed mean on Backward Digit Recall, Mr. X, Digit Recall, and Single Word Reading, and 1 standard deviation above the age-normed mean on Numerical Operations. Such overperformance is not uncommon in neurodevelopmental research (e.g., Operto et al., 2021; Trane & Willcutt, 2023; Willcutt & Petrill, 2023) and may reflect several contributing factors, including recruitment bias (e.g., lower rates of parental consent among children performing at the lower end of the cognitive spectrum) and outdated test norms (Elson et al., 2023; Trahan et al., 2014). To address this concern, additional one-sample t-tests were conducted to compare each group’s performance with the standardized mean on the cognitive and learning measures, in order to determine the extent to which each group significantly deviated from or scored above the age-normed level of these standardized tests (Section 2, Supplemental Material). The outcomes of these analyses were used to guide the interpretation of significant group differences reported in the group ANOVAs (Table 2) and the pairwise ANOVAs (Tables 3–8). The interpretive principle adopted was that when the comparison group scored significantly above both the neurodivergent group (as identified by the ANOVAs) and the age-normed mean (as indicated by the one-sample t-tests), but the neurodivergent group also scored at or above the age-normed mean, the neurodivergent group was not considered to exhibit genuine deficits relative to the comparison group. In the following section, we first present the results of the one-sample t-tests, indicating whether each group scored above, at, or below the age-normed mean of the standardized tests. We then describe significant group differences identified in the pairwise ANOVAs—whether between the neurodivergent and comparison groups, between neurodivergent groups, or both. Finally, ANCOVA results are reported to examine whether group differences remained after accounting separately for scores of inattention and hyperactivity/impulsivity.
Cognition
The comparison group performed significantly above the age-normed mean on all standardized cognitive and learning measures, except for the Barking/Vigil task, on which their scores fell below the age-normed mean. The ADHD only group exceeded the age-normed mean on Motor Speed and scored at the age-normed mean on Backward Digit Recall, Digit Recall, Mr. X, Simple Reaction Time, Barking/Vigil, and Visual Scanning. While significant differences were observed between the ADHD only and comparison groups on Digit Recall, Backward Digit Recall, and Mr. X, these differences are unlikely to reflect genuine difficulties in the ADHD only group, as their scores on these tasks did not differ significantly from the age-normed mean. The ADHD only group scored below the age-normed mean on Dot Matrix and on the set-shifting measures of the Number and Letter Sequencing Composite Score and Number–Letter Sequencing, with scores significantly lower than both the age-normed mean and those of the comparison group. Group differences between the ADHD only and comparison groups on the Number and Letter Sequencing Composite Score and Dot Matrix were eliminated when inattention or hyperactivity/impulsivity scores were included as covariates. Group differences on Number-Letter Sequencing remained significant when either inattention or hyperactivity/impulsivity scores were covaried.
The learning difficulties only group scored below the age-normed mean on all measures except for the Visual Scanning and Motor Speed tasks, on which performance levels were in line with the age-normed mean. The significant differences observed between the learning difficulties only group and the comparison group on these two tasks were therefore not interpreted as evidence of genuine impairments in the learning difficulties only group. On all other cognitive measures, the learning difficulties only group showed significantly lower performance than the comparison group. These group differences persisted even after controlling for either inattention or hyperactivity/impulsivity scores. The learning difficulties only group and the ADHD with learning difficulties group showed no differences from each other on all cognitive tasks, with the exception of Visual Scanning, on which faster performance was observed in the learning difficulties only group. This difference remained significant even when either inattention or hyperactivity/impulsivity were included as covariates.
The ADHD with learning difficulties group scored significantly below the age-normed mean on all cognitive assessments, with the exception of the Motor Speed measure, where performance was consistent with the age-normed mean. Thus, although a significant difference was observed between this group and the comparison group on that task, it was not interpreted as a genuine deficit. This group did however score significantly below the comparison group on all remaining assessed measures. Including inattention or hyperactivity/impulsivity scores as covariates only eliminated group differences on the Barking/Vigil task, while all other group differences remained significant.
The ADHD only group scored higher than both the learning difficulties only and ADHD with learning difficulties groups on measures of Digit Recall, Dot Matrix, Backward Digit Recall, Simple Reaction Time, Barking/Vigil, and Number-Letter Sequencing. The ADHD only group also had higher scores than the learning difficulties only group on the Number and Letter Sequencing Composite Score, but no differences were observed on this task between the ADHD only and ADHD with learning difficulties groups. When inattention scores were covaried, the ADHD with learning difficulties group performed significantly lower than the ADHD only group on the Visual Scanning task. All other group differences remained significant when either inattention or hyperactivity/impulsivity scores were covaried.
Learning
The comparison group performed significantly above the age-normed mean on both the Single Word Reading and Numerical Operations tasks. The ADHD only group performed at the age-normed mean on both learning measures. The learning difficulties only group and the ADHD with learning difficulties group scored significantly below the age-normed mean. All three neurodivergent groups scored at significantly lower levels on the learning measures than the comparison group. The ADHD only group had higher scores than both the learning difficulties only and ADHD with learning difficulties groups.
Behavior
Inattention and hyperactivity/impulsivity scores were significantly higher in the ADHD only, ADHD with learning difficulties, and learning difficulties only groups than the comparison group. Mean scores for inattention and hyperactivity/impulsivity in all three neurodivergent groups fell within the clinically significant range, with T-scores at or in excess of 70 (Conners, 2008). The ADHD with learning difficulties group had higher inattention scores than both the learning difficulties only and ADHD only groups, with no significant differences between the latter two. Hyperactivity/impulsivity scores were significantly higher in both the ADHD only and ADHD with learning difficulties groups compared to the learning difficulties only group. There were no significant differences in hyperactivity/impulsivity scores between the ADHD only and ADHD with learning difficulties groups.
Executive Function Covariance Analyses
A series of ANCOVAs examined group differences in executive function tasks, using scores on the relevant basic processing tasks as covariates for the executive function measures: Backward Digit Recall (covarying Digit Recall), Mr. X (covarying Dot Matrix), and Number-Letter Sequencing (covarying Number and Letter Sequencing Composite Score). In all cases, the differences between the comparison group and each neurodivergent group remained significant (Table 13, Supplemental Material).
Medication
Additional ANOVAs were conducted to evaluate the effect of medication by comparing performance across all measures among ADHD subgroups differentiated by medication status (Tables 14-16, Supplemental Material). Reaction times on the Simple Reaction Time task were significantly longer for the two subgroups receiving stimulant medication compared to those who were not. These significant group differences were followed up with t-tests against both the comparison group and the age-normed mean. The ADHD only group receiving medication did not differ significantly from either the comparison group or the age-normed mean on the Simple Reaction Time task. In contrast, the ADHD only group not receiving medication, as well as both ADHD with learning difficulties subgroups (with and without medication), showed significantly slower reaction times than both the comparison group and the age-normed mean. No other significant differences between medication subgroups were observed for cognition and learning measures. Inattention scores were significantly lower in the ADHD with learning difficulties group receiving medication compared to those not receiving medication; however, both subgroups still differed significantly from the comparison group.
Factor Analyses
Although executive functions are widely distinguished as separate constructs such as working memory and set shifting, it is widely recognized that they depend at least in part on common cognitive processes (Karr et al., 2018; Miyake et al., 2000). In order to establish whether the three neurodiverse groups in this study are distinguished by broad constellations of cognitive processes associated with measures of executive functions rather than the individual measures per se (see also, Kofler et al., 2024; Snyder et al., 2015), an exploratory Principal Components Analysis (PCA) was conducted on the measures completed by children 8 years and older (n = 568). Varimax rotation was applied to the PCA to enhance factor differentiation. Factors with Eigenvalues >1 were retained, and factor loadings of .45 or higher were used to interpret the factor structure (Tabachnick, 2018). Post-hoc pairwise comparisons of groups on individual factor scores were conducted, with p < .008 applied as the threshold for statistical significance in each comparison (Tables 17 and 18, Supplemental Material).
The PCA identified two factors accounting for 36% and 21% of the variance, respectively. The measures loading highly on Factor 1 represented the cognitively complex tasks of Backward Digit Recall and Mr. X (working memory), Number-Letter Sequencing (set shifting), Digit Recall and Dot Matrix (short-term memory), and Number and Letter Sequencing Composite Score (set sequencing). The measures loading highly on Factor 2 were less complex in their cognitive demands—the Barking/Vigil (sustained attention) and Simple Reaction Time (processing speed). An ANOVA performed on Factor 1 scores yielded a significant group effect, F(3, 564) = 110.64, p < .001. Post hoc pairwise comparisons established that the comparison group scored significantly more highly than the three neurodivergent groups. The ADHD only group had significantly higher scores than both the learning difficulties only and the ADHD with learning difficulties groups, which did not differ from one another. A significant group effect was observed on Factor 2 scores, F(3, 564) = 17.08, p < .001. Both the ADHD only and comparison groups scored higher than the learning difficulties only and ADHD with learning difficulties groups on this factor. No further significant group differences were observed.
Discussion
Drawing on data from a large neurodivergent cohort, the study compared cognition, learning abilities, and attentional behaviors of children with ADHD, learning difficulties, and ADHD with learning difficulties to a comparison group without neurodevelopmental conditions. A third of the children with ADHD showed no evidence of learning difficulties, a rate of co-occurrence similar to previous reports (Mayes & Calhoun, 2006). This group demonstrated age-appropriate performance on measures of simple processing tasks, sustained attention, verbal short-term memory, and working memory. In contrast, children with learning difficulties were impaired in multiple cognitive skills, including processing speed, set sequencing of numbers and letters, short-term memory, and executive functions of working memory and set shifting. The breadth of their cognitive impairments was similar for those children with co-occurring ADHD.
The study explored whether the observed deficits in the cognitive skills essential for learning in these populations could be a consequence of their elevated levels of inattention and hyperactivity/impulsivity. The limited deficits in measures of visuospatial short-term memory and basic sequencing of letters and digits in the group with ADHD only were eliminated when levels of inattention and hyperactivity/impulsivity were taken into account. In contrast, the more extensive and severe cognitive impairments of the children with learning difficulties could not be attributed to either of the two attentional behaviors, irrespective of whether they had co-occurring ADHD. All cognitive deficits other than in sustained attention persisted in the ADHD with learning difficulties group when inattention and hyperactivity/impulsivity scores were covaried.
The disparities in the associations between cognitive impairments and the attentional dimensions of inattention and hyperactivity/impulsivity across these neurodivergent groups are striking. There is some evidence that the unfocused, distracted, and fidgety behavior of children with ADHD in the absence of learning difficulties may have directly interfered with their ability to meet the attentional demands of two cognitive tasks: the Dot Matrix task measuring visuospatial short-term memory, and the Number and Letter Sequencing Composite Score task assessing rapid sequencing of sets of either numbers or letters. The finding that elevated levels of attentional behaviors disrupt the proper functioning of short-term memory is consistent with other evidence indicating that performance on the Dot Matrix task relies heavily on domain-general attentional resources (Alloway et al., 2006; Gathercole et al., 2008, 2019; Logie & Pearson, 1997; Morey & Bieler, 2013). Similarly, the task of rapidly generating sequences of numbers or letters relies on holding information in short-term memory and the speeded retrieval of learned verbal sequences from long-term memory, while simultaneously manipulating that information to produce the correct sequence. The present findings suggest that in the ADHD only group, the cognitive resources required for short-term memory and basic set sequencing tasks may be depleted, potentially due to elevated levels of attentional behaviors that form the basis of their diagnosis. It is less clear why performance on the rapid sequencing of single categories of either number or letter sets was selectively associated with attentional behaviors, whereas difficulties on the more complex alternating set tasks were also observed but appeared unrelated to high levels of inattention or hyperactivity/impulsivity.
In contrast, the more pervasive cognitive difficulties of the group with learning difficulties only showed no links with levels of inattention and hyperactivity/impulsivity. This group were impaired in measures of sustained attention, processing speed, set sequencing, short-term memory, working memory, and set shifting, reinforcing findings from previous studies (Crisci et al., 2021; Moura et al., 2014; Toffalini et al., 2017; Varvara et al., 2014; Willcutt & Petrill, 2023). Their very high levels of inattention accompanied by lower but still elevated levels of hyperactive/impulsive behavior are consistent with findings from past studies (Kibby et al., 2021; Parhiala et al., 2015; Willcutt & Petrill, 2023). The levels observed in the current study were generally higher than those reported in previous studies, with group means exceeding thresholds for clinical significance. However, the study provided no evidence that either inattentive or hyperactive/impulsive behavior underpins the cognitive deficits of children with learning difficulties only.
The cognitive impairments in the group with both ADHD and learning difficulties were similar to those previously observed in groups with learning difficulties or diagnosed SLD (see also Huang et al., 2016; Willcutt & Petrill, 2023). Levels of inattention were higher in the group with both learning difficulties and ADHD than the group with ADHD only, whereas levels of hyperactivity/impulsivity were comparable between the two groups. When both inattention and hyperactivity/impulsivity scores were taken into account, the cognitive deficits shared by both learning difficulties groups in processing speed, set sequencing, verbal and visuospatial short-term memory, working memory, and set shifting persisted. This outcome indicates that these cognitive difficulties were not a consequence of elevated levels of restlessness, distractibility, or fidgety behaviors. The exception was the sustained attention measure, on which inattention and hyperactivity/impulsivity contributed differently to group differences between the two groups with learning difficulties and the comparison group. This task required participants to count repeated auditory stimuli presented intermittently during a slow and monotonous sequence. Accounting for inattention or hyperactivity/impulsivity eliminated the group differences between the group with both ADHD and learning difficulties and the comparison group on this measure, but not between the learning difficulties only group and the comparison group. While this outcome was not anticipated, it may reflect differences in cognitive constraints across groups. The sustained attention difficulties in the group with co-occurring ADHD and learning difficulties may result from the disruptive effects of highly unfocused, distractible, and restless behaviors during a lengthy and unrewarding task. In contrast, difficulties on the same task in the learning difficulties only group could reflect more specific cognitive processing challenges that underpin their learning difficulties, rather than observable, parent-rated attentional behaviors.
Broadly speaking, pervasive cognitive deficits were found in the two groups with learning difficulties not in those with ADHD only. Although prior studies have found that individuals with co-occurring ADHD and learning difficulties experience greater cognitive challenges compared to those with learning difficulties only (Crisci et al., 2021; Kibby et al., 2021; Willcutt & Petrill, 2023), the current study finds that the cognitive profiles of these two groups are largely indistinguishable. This conclusion aligns with prevailing accounts that attribute learning difficulties in both reading and mathematics to core deficits in cognitive processes such as processing speed, phonological processing, and executive functions including working memory and set shifting (Allen et al., 2019; Peng et al., 2019, 2022; Snowling et al., 2022). The current findings indicate that the overt attentional behavioral problems associated with an ADHD diagnosis, which have reached clinically significant levels, have limited influence on academic progress. These effects are likely masked by the far greater impact of weak skills in multiple aspects of cognitive functioning.
Some aspects of the results reinforce Kibby et al.’s (2019) observation that although heightened levels of inattention and hyperactivity/impulsivity in ADHD do not disrupt the execution of relatively automatic tasks, reaction times slow down markedly when activities require more complex cognitive processing and rule shifts. While unimpaired on the Simple Reaction Time task of processing speed, the ADHD only group was slower to complete the set shifting task, which involved cognitively demanding rule shifts between response sets of numbers and letters. Children with ADHD also show high levels of variability in their reaction times (Karalunas & Huang-Pollock, 2013; Kofler et al., 2013; Salum et al., 2019), which is attributed to less efficient information processing. As reaction times for individual trials were not accessible in the D-KEFS (Delis et al., 2001), it was not possible to calculate measures of reaction time variability in this study.
The assessments employed in this study are labeled according to conventions in the broader research field and associated clinical practice. Thus, “verbal short-term memory” is used as the label for Digit Recall, “set shifting” for Number-Letter Sequencing, and so on. However, the labels and constructs are not homologous: neuropsychological tests do not provide pure assessments of single cognitive mechanisms, and the cognitive processes underpinning different tests can have substantial overlap. It has been widely acknowledged that this high level of construct impurity in psychological tests generates significant challenges for the coherent theoretical interpretation of test outcomes (Karr et al., 2018; Kofler et al., 2024; Snyder et al., 2015).
Given this high degree of construct impurity and substantial overlap across cognitive tasks, an exploratory factor analysis was conducted to identify underlying cognitive dimensions across the assessments analyzed in the study. This data-driven approach examined whether the neurodivergent groups could be distinguished from the comparison group, as well as from each other, based on latent cognitive dimensions identified through the test battery, offering a complementary perspective to independent analyses of individual measures. Exploratory factor analysis was conducted on the full set of assessments completed by children aged 8 years and older (Tables 17 and 18, Supplemental Material). Measures of verbal and visuospatial short-term memory, verbal and visuospatial working memory, set sequencing, and set shifting all loaded onto the first factor, whereas processing speed and sustained attention loaded onto the second factor.
The two extracted factors were relatively general in nature, consistent with previous findings indicating that individual tests within the battery do not necessarily measure the intended constructs exclusively, and that substantial overlap exists among measures that superficially appear to tap different cognitive processes (Karr et al., 2018; Kofler et al., 2024; Snyder et al., 2015). These two cognitive factors appear to be better distinguished by the complexity of the cognitive loads imposed by the tasks (Sweller, 2010) rather than by the overlap in specific cognitive processes involved. Specifically, the cognitive demands of responding to single stimuli in the processing speed and sustained attention measures, which loaded highly on the second factor, are considerably lower in complexity than the encoding and maintenance demands of the working memory and set-shifting tasks, which loaded on the first factor.
While this exploratory factor analysis provided a coarse-grained representation of cognitive dimensions in the sample, the two factors offered limited precision in distinguishing profiles of neurodivergent groups. Both the learning difficulties only group and the ADHD with learning difficulties group scored lower than the comparison group on both factors. On the first (high cognitive load) factor, the comparison group outperformed all three neurodivergent groups. In contrast, on the second (low cognitive load) factor, both the comparison group and the ADHD only group scored higher than the two learning difficulties groups. However, clear interpretation of these task differences is challenged by the generally high performance of the comparison group, who exceeded the test standardization means on all cognitive measures except for the sustained attention task. This makes it difficult to distinguish genuine deficits in the neurodivergent groups on the basis of these factor scores. Future studies involving these groups, incorporating carefully selected and broader sets of cognitive assessments with multiple tasks per construct, have the potential to yield valuable data-driven insights into their fundamental cognitive similarities and differences (Conway et al., 2005; Kofler et al., 2024; Willoughby et al., 2016).
Limitations
Due to the lack of a standardized and structured assessment process for SLD in England, it was not possible in this study to select children based on a formal diagnosis such as dyslexia or dyscalculia, as defined by the DSM-5 (American Psychiatric Association Division of Research, 2013). To compare the cognitive and behavioral profiles of children with learning difficulties to those with ADHD, this study used the Single Word Reading or Numerical Operations subtests of the WIAT-II (Wechsler, 2005) as a proxy for SLD. The selection criterion of scores at or below 1 SD from the population mean on these standardized tests was guided by other studies (Galuschka & Schulte-Körne, 2016; Geary et al., 2007; von Wirth et al., 2021; Vukovic et al., 2010). Applying this cutoff value includes all children in the lowest 15% for their age, whereas the 1.5 SD cutoff recommended by the DSM-5 captures the lowest 7%. Concerns regarding the relative leniency of these criteria as a proxy for clinical diagnosis were mitigated in two ways. First, even those children falling in the more lenient 7th to 15th centile range were making sufficiently weak academic progress to require additional support within school or clinic. Second, the cognitive profiles of these children closely align with findings from previous studies of children diagnosed with SLD (e.g., Menghini et al., 2011; Szucs et al., 2013; Varvara et al., 2014; Willcutt et al., 2013).
Both inattention and hyperactivity/impulsivity scores of the learning difficulties only group reached levels of clinical significance. A more typical profile for children with SLD is characterized by high levels of inattention and hyperactivity/impulsivity compared to the age-normed mean, although both remain below clinical thresholds (e.g., Crisci et al., 2021; Kibby et al., 2021). This may be a consequence of the referral process to the CALM clinic (Holmes et al., 2019). Education and healthcare practitioners referred children whom they had identified as experiencing difficulties in attention, learning, and/or memory. It is possible that there may have been disproportionately more children with learning difficulties who had moderately high levels of ADHD traits without a formal ADHD diagnosis than in a population sample. Given the near-equivalence of the cognitive profiles of the two learning difficulties groups and the independence of cognitive impairments from either inattention or hyperactivity/impulsivity scores, the potential overrepresentation of children with high but undiagnosed levels of ADHD characteristics is relatively unlikely to have distorted the empirical outcomes of the study.
The study reported data from children aged 5 to 18 years, covering the full age range of primary and secondary education. The statistical outcomes therefore represent a model aggregated across this broad developmental period of formal education. The strengths of this approach include the high statistical power of the study and the generality of the conclusions that can be drawn for these common neurodevelopmental populations across this wide developmental span 1 . However, as a consequence of the cross-sectional design, the findings do not capture the dynamic shifts in the processes that enable and disrupt formal academic learning and cognitive functioning between school entry and later adolescence (Ferguson et al., 2021; Pingault et al., 2011, 2014; Sayal et al., 2015).
The proportion of males was higher than females in both ADHD groups, with particularly high rates of 74% in the ADHD only group and 79% in the co-occurring ADHD and learning difficulties group, compared to 63% in the learning difficulties group and 58% in the comparison group. The over-representation of males with ADHD has been widely observed in both clinical and population-based samples (Cervin, 2023; Mayes et al., 2020; Mowlem et al., 2019; Trane & Willcutt, 2023), and clearly runs the risk of masking characteristics specific to females (Guy et al., 2022; Merrill et al., 2024).
The study relies on parental reports to assess attentional behavior. Parental ratings are commonly used in research in this field because parents frequently interact with clinicians, thus serving as important sources of information (Sims & Lonigan, 2012). Relying on single rather than multiple reporting sources, such as parents, teachers, and the children themselves, may limit the broad representativeness of reported symptoms across different settings and perspectives (Mulraney et al., 2022; Takeda et al., 2020). However, the study included direct assessments of sustained attention using the Barking/Vigil tests from the TEA-Ch2 (Manly et al., 2017). These tests were designed as accessible, child-appropriate analogues of the Continuous Performance Test (Conners et al., 2003), which is widely recognized for eliciting inaccurate responses in individuals with ADHD (Hall et al., 2016).
The comparison group scored above the age-normed mean on both cognitive and learning measures, which is commonly observed in other neurodevelopmental research (e.g., Operto et al., 2021; Trane & Willcutt, 2023; Willcutt & Petrill, 2023). To aid interpretation of the pairwise ANOVA results, additional one-sample t-tests were conducted to assess the extent to which each group exceeded or fell below age-normed expectations. A neurodivergent group was identified as showing difficulty on a cognitive or learning measure only if their performance was significantly below the age-normed mean in the one-sample t-test and also significantly lower than that of the comparison group or other neurodivergent groups in the pairwise ANOVAs. Significant pairwise group differences identified by ANOVAs should be interpreted with caution if the group scored at or above the age-normed mean in one-sample t-tests, as they may not represent genuine deficits for that group in the context of the study.
Finally, the CALM dataset lacks information regarding the type, dosage, and dosing frequency of medication taken by children with ADHD, and so does not extend previous research on the impacts of medication on cognitive performance in children with ADHD (Johnson et al., 2021; Swanson et al., 2011).
Conclusions
The study provides further evidence of cognitive heterogeneity in children diagnosed with ADHD in both their learning and specific cognitive skills (Coghill et al., 2014; Kofler et al., 2019). It demonstrates that the cognitive skills and academic attainments of many children with ADHD are largely intact. When impairments are found, they can often be attributed to the impacts of their inattentive and hyperactive/impulsive behavior on learning. In contrast, children with learning difficulties, either with or without ADHD, showed pervasive impairments across multiple cognitive and executive skills that were independent of their elevated levels of attentional difficulties. Their low academic attainments appear to reflect these core cognitive deficits (Allen et al., 2019; Peng et al., 2022; Peng, Wang, et al., 2018). These findings suggest that the largely distinct profiles of learning difficulties and ADHD reflect underlying differences in their neurodevelopmental pathways.
These findings align well with transdiagnostic approaches to neurodevelopmental conditions (Astle et al., 2022; Fletcher-Watson, 2022), demonstrating how discrete diagnostic categories alone offer only a limited understanding of the diverse challenges faced by children with ADHD and learning difficulties. The outcomes highlight the value of integrating assessments of learning and cognition into the periodic monitoring of children with ADHD and those with learning difficulties. Incorporating broader-based cognitive assessments into the periodic evaluation of neurodivergent children offers a means of identifying both cognitive strengths that can be built upon and weaknesses that can be addressed (Dvorsky & Langberg, 2016; Fletcher-Watson, 2022; Michelini et al., 2024). Understanding whether a child experiences learning-related cognitive deficits, ADHD, or both provides a valuable framework for prioritizing intervention and support strategies. These may include interventions targeting elevated levels of attentional behaviors (e.g., pharmacological treatment, classroom management, and family therapy) and educational support aimed at mitigating the impact of cognitive deficits on learning (Coghill et al., 2023; McDougal et al., 2023), or a combination of both approaches.
Supplemental Material
sj-docx-1-jad-10.1177_10870547251376776 – Supplemental material for Associations Between ADHD Symptom Dimensions and Cognition in Children With ADHD and Learning Difficulties
Supplemental material, sj-docx-1-jad-10.1177_10870547251376776 for Associations Between ADHD Symptom Dimensions and Cognition in Children With ADHD and Learning Difficulties by Yufei Cai, Joni Holmes and Susan E. Gathercole in Journal of Attention Disorders
Footnotes
Acknowledgements
The Centre for Attention, Learning, and Memory (CALM) research clinic is located at and receives support from the MRC Cognition and Brain Sciences Unit, University of Cambridge. The lead investigators are Duncan Astle, Kate Baker, Susan Gathercole, Joni Holmes, Rogier Kievit, and Tom Manly. Data collection process was supported by a large team of researchers and research students (![]() ). The authors express their gratitude to all the researchers involved in the project and to the professionals working in children’s services in the South-East and East of England for their valuable support, and to the children and their families for their participation.
). The authors express their gratitude to all the researchers involved in the project and to the professionals working in children’s services in the South-East and East of England for their valuable support, and to the children and their families for their participation.
Ethical Considerations
This study involves a secondary analysis of data from the Centre for Attention, Learning, and Memory (CALM) cohort. Ethical approval for the CALM study was granted by the National Health Service (NHS) Health Research Authority NRES Committee East of England, with the REC approval reference (13/EE/0157; Holmes et al., 2019). As the data used in this analysis are not personally identifiable, no additional ethical approval was required for the present study.
Author Contributions
Conceptualization: Cai and Gathercole. Data acquisition: Holmes, Gathercole, and the CALM Team. Formal analysis: Cai. Data Interpretation: Cai and Gathercole. Writing—original draft: Cai and Gathercole. Writing—reviewing & editing: Cai, Gathercole, and Holmes.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.