
Abstract
Objectives:
Although ADHD has its roots in childhood, significant symptoms persist into adulthood for more than half of individuals. Adults with ADHD are heterogeneous in terms of symptom presentations, impairment domains, and relative strengths. Consequently, it is essential to better understand the diverse self-perceptions and experiences of adults with ADHD; qualitative methods are a valuable complement to quantitative work in this area. Our aim is to provide a scoping review of qualitative studies on adults with ADHD to articulate the current status of the field and establish future research directions.
Method:
We review 41 studies, separating findings into four subpopulations: (1) adults with childhood ADHD, (2) college students with ADHD, (3) adults diagnosed with ADHD in adulthood, and (4) other studies (unspecified age of diagnosis).
Results:
Qualitative research on all four subgroups identifies recurring themes: substance use, decisions about medication for ADHD, perceived domains of impairment, factors that promote or hinder success, and concerns about identity and stigma. Notably, the relative emphasis of each theme varies as a function of sample type. Specifically, qualitative research among adults with a childhood ADHD diagnosis focuses principally on substance use and treatment desistance, whereas studies of individuals diagnosed with ADHD as adults often examine emotional responses to receiving the diagnosis. For college students with ADHD, themes frequently relate to struggles with the increased independence demanded by post-secondary educational environments and the adoption of accommodations or coping strategies. For future studies of adult ADHD, we highlight key domains for which mixed-methods strategies will be critical: (a) similarities and differences between multiple reporters of functioning, (b) willingness to receive treatment, (c) women, (d) participants from diverse racial and ethnic groups, and (e) middle age and older adults.
Conclusion:
In all, we highlight the value of qualitative and mixed-methods approaches to ensure that research captures the beliefs, intentions, experiences, emotions, and self-perspectives of people with ADHD.
Keywords
Introduction
ADHD is a neurodevelopmental condition characterized by developmentally atypical levels of inattention and/or hyperactivity-impulsivity contributing to limitations and impairments in multiple settings (American Psychiatric Association, 2013). Although ADHD begins in childhood, (a) many girls and women are not recognized and diagnosed until later in development (e.g., Hinshaw et al., 2022) and (b) the majority of affected individuals continue to experience elevated and impairing levels of symptoms into adulthood (Sibley et al., 2022). Many do not continue treatment as adults (Swanson et al., 2017) and experience poorer educational, occupational, emotional, and substance-use outcomes than those without the disorder (Hechtman et al., 2016). Adult interpersonal and romantic relationships are also often areas of challenge for those with ADHD (Moyá et al., 2014; Safren et al., 2010; Wymbs et al., 2021).
This knowledge has emanated largely from quantitative research. Indeed, quantitative research into the cognitive, academic, and social functioning of individuals with ADHD has been foundational to the field. At the same time, complementary methods utilizing a qualitative approach, which features analysis of open-ended responses to provide contextual understanding of respondents’ experiences, may allow for new insights into salient areas not identified or expanded upon by existing quantitative measures. Qualitative and quantitative methods each have unique limitations and strengths (Weisner, 2005, 2016), and both can enrich our understanding of ADHD in adulthood. For instance, in addition to the potential under-reporting of “stigmatized” behaviors, such as substance use, in quantitative relative to qualitative reports (e.g., Weisner et al., 2018), qualitative methods can capture and expand upon the phenomenological experience of living with ADHD. Idiographic narrative accounts provided by participants in qualitative interviews can provide a personal story that can aid understanding of their behaviors and thoughts. A qualitative approach to understanding such experiences can inform theoretical frameworks surrounding adults with ADHD that can then be tested using quantitative methods, ensuring that findings are more clinically meaningful than if either approach is used in isolation (Weisner, 2016).
The social model of disability argues that impairment is related to a mismatch between individual differences (e.g., developmentally atypical levels of ADHD symptoms) and the sociocultural or environmental contexts in which individuals reside (Dwyer, 2022). As such, a purely deficit-focused approach to ADHD is incomplete: the contexts and situations in which the individual functions must also be appreciated, as well as how these individuals understand and perceive these environments. Indeed, a symptom that is problematic in one context may be innocuous in another (e.g., Nielsen, 2019). For instance, some individuals with ADHD report that symptoms are not impairing if they are in environments that “fit with” their proclivities or interests (e.g., Lasky et al., 2016). For related perspectives, the growing neurodiversity movement has provided important insights (Grinker, 2021; Ingstad & Whyte, 1995; Silberman, 2015).
For adults with a childhood diagnosis of ADHD, conceptualization of the diagnosis and descriptions of the disorder as part of who they are may change over time. For example, some adults may report that they no longer have ADHD; others may report that it is just part of their personality or is still there but manageable. For these and other reasons, many adults with childhood-diagnosed ADHD do not persist in seeking out services, at least in early adulthood (Swanson et al., 2017). Although adoption of qualitative or mixed-methods approaches has occurred for questions related to self-perceptions of symptoms, impairment, and treatment in youth with ADHD and their parents (see Ringer, 2020 for a review), such research approaches among adults with ADHD are underutilized, and a critical review of the extant literature is needed to highlight important areas for future inquiry.
A rapid review by Ginapp et al. (2022) summarized existing qualitative literature on adults with ADHD and highlighted recurrent themes, including being diagnosed as an adult, ADHD symptoms and adaptations to such symptoms, substance use, interactions with society, and perceptions of the self and one’s diagnosis (Ginapp et al., 2022). Extending this work, we aim to discuss the current state of qualitative literature on adults with ADHD, focusing on the diverse and heterogeneous lived experiences of adults with ADHD (e.g., adults diagnosed with ADHD in childhood, college students with ADHD, and adults first diagnosed in adulthood) and with an eye toward important directions for future research. Regarding the former, ADHD in adults is characterized by extreme heterogeneity in symptom presentation and associated impairment (e.g., Luo et al., 2019; Sibley et al., 2022). For example, the strengths, coping strategies, and experiences of college-enrolled young adults with ADHD may not be representative of those with ADHD not enrolled in post-secondary school (e.g., Howard et al., 2016). Although it is crucial to understand why individuals with ADHD who attend college often perform more poorly than their peers academically (Rabiner et al., 2008), such information may not translate well to individuals with ADHD who are struggling in the workforce. Additionally, adult symptom severity/impairment, self-construals, and coping strategies may differ considerably between those first diagnosed in childhood versus adulthood. For instance, those with childhood-diagnosed ADHD may no longer have clinically significant symptoms as adults—or may continue to struggle with ADHD-related impairment (Sibley et al., 2022). In contrast, those recently diagnosed with ADHD as adults are highly likely to endorse clinically significant symptoms. Unfortunately, previous reviews of the qualitative literature on ADHD do not parse the unique perspectives and experiences of these distinct subsets of adults with ADHD (e.g., Ginapp et al., 2022).
In sum, to better understand and contextualize the unique phenomenological and lived experiences of diverse adults with ADHD, we separately review qualitative findings from four subgroups: (1) adults with a childhood diagnosis of ADHD, (2) college students with ADHD (some but not all of whom were diagnosed in childhood or adolescence), (3) adults diagnosed with ADHD in adulthood, and (4) other samples for which age of diagnosis is not specified. We argue that heightened understanding of adult ADHD requires pluralistic methods and diverse samples to reflect the heterogeneity of the disorder.
Methods
PsycInfo, Google Scholar, Web of Science, and AnthroSource were searched to identify relevant qualitative articles. Abstracts were searched for the following terms: (ADHD OR attention deficit* OR hyperactiv* OR inattent*) AND (Qualitative* OR elicitation OR entification* OR phenomenography OR discourse* OR grounded theory* OR identity OR theme* OR thematic* OR focus group* OR Dedoose OR invivo OR LIWC OR atlas). Results were refined to include only articles that were human studies, peer-reviewed, and available in English. Titles were scanned for relevance; subsequently, we scanned abstracts. Excluded were articles on children or adolescents (age < 18 years), those that focused on ADHD symptoms (but not a diagnosis), those that did not focus on ADHD, those on perspectives other than adults with ADHD (e.g., only parents or teachers), those focusing the impact of a specific pharmacological or nonpharmacological intervention, case studies, reviews, and studies without qualitative components. References cited by relevant empirical and review articles of qualitative research on adults with ADHD were also considered to ensure a comprehensive representation of the literature.
Ultimately, we identified 41 relevant empirical articles. Five discussed qualitative findings from adults with ADHD who were diagnosed in childhood, 9 had samples of college students with ADHD, 11 explored perspectives of adults who were diagnosed with ADHD in adulthood, and 16 articles either did not specify or had mixed ages of diagnosis. Thirteen used some degree of mixed qualitative and quantitative methods. Twenty-seven studies based findings upon information gathered during individual semi-structured interviews. Among the remainder, nine had other or unspecified types of interviews, three utilized focus groups, one utilized both focus groups and individual semi-structured interviews, and two used some other method to obtain qualitative perspectives (see Table 1).
Characteristics of Qualitative Studies of Adults With ADHD Included in the Review.
Note. If the sample consisted of individuals with and without ADHD, demographics and results reflect only the subset of individuals with ADHD. Papers were considered mixed methods if they incorporated both qualitative and quantitative components into analyses, such as discussing the percentage of people who endorsed each theme, responses on questionnaires in comparison to qualitative responses, etc.
SU = substance use; SUD = substance use disorder; ACDS = Adult ADHD Clinical Diagnostic Scale; ADHS-SB = Attention-Deficit/Hyperactivity Self-Report Scale (German); ASRS = Adult ADHD Self-Report Scale; BAARS-IV = Barkley Adult ADHD Rating Scale IV; CAARS = Conners’ Adult ADHD Rating Scale; CGI-P = Conners’ Global Index-Parent Scale; DISC = Diagnostic Interview Schedule for Children; DIVA = Diagnostic Interview for ADHD in Adults; DBDRS = Disruptive Behavior Disorder Rating Scale; ICD-10 = 10th revision of the International Classification of Diseases; IRS = Impairment Rating Scale; SCL-90-R = Symptom Checklist 90-Revised (German); WRI = Wender-Reimherr Interview (German); WURS-k = Wender Utah Rating Scale (German).
—indicates that this information was not reported in the text.
Jensen et al. (2018), Lasky et al. (2016), Mitchell et al. (2018), Swanson et al. (2018), and Weisner et al. (2018) all use data from the qualitative follow-up of the Multimodal Treatment of ADHD Study.
Results
Upon review, several recurrent themes emerged across multiple studies, including substance use; ADHD medications; areas of impairment; factors that promote success/coping strategies; identity, stigma, and disclosure; and perceived positives of ADHD. Some of these themes were repeatedly highlighted during semi-structured interviews, whereas others emerged from open-ended interviews, depending on the study. Key findings organized by adult ADHD subsample (childhood diagnosis, college students, adult diagnosis, other) are included in Tables 2 to 5.
Themes/Insights From Qualitative Studies of Adults With ADHD Diagnosed in Childhood.
Themes/Insights From Qualitative Articles of College Students With ADHD.
Themes/Insights From Qualitative Articles of Adults Diagnosed With ADHD in Adulthood.
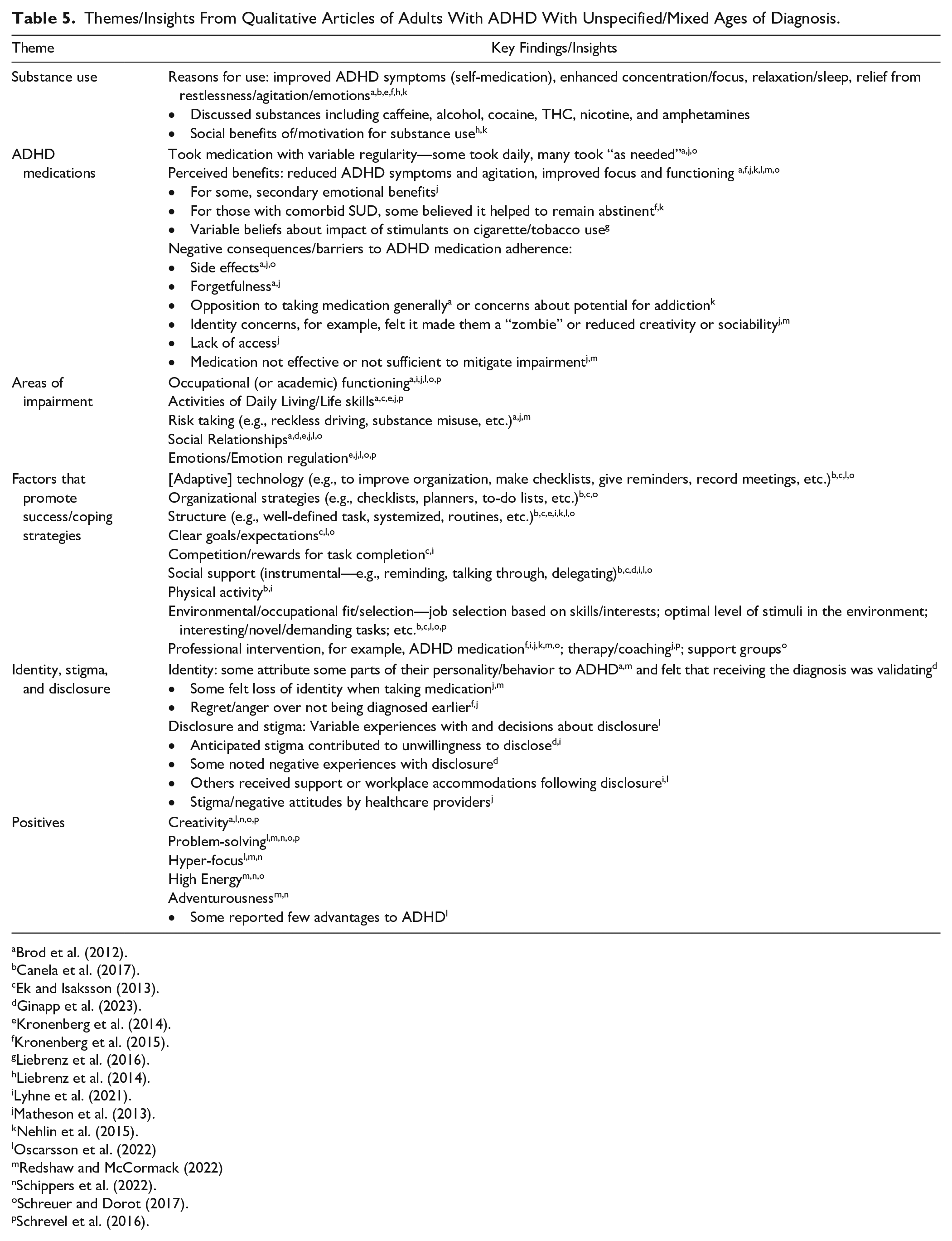
Themes/Insights From Qualitative Articles of Adults With ADHD With Unspecified/Mixed Ages of Diagnosis.
Adults With Childhood ADHD
Five studies discussed qualitative and mixed methods outcomes among adults diagnosed with ADHD in childhood. All used the same dataset—a qualitative follow up to the Multimodal Treatment Study of Children with ADHD (MTA; The MTA Cooperative Group, 1999). In childhood, 579 youth with the combined type of ADHD were assigned to treatment with either medication, behavioral therapy, their combination, or treatment-as-usual in the community for 14 months. Along with a normative sample without ADHD, these youth were followed into adulthood as part of an observational, longitudinal assessment phase. As young adults, a subset (n = 125 with ADHD, n = 58 without ADHD) participated in extensive semi-structured qualitative interviews about their life experiences. Researchers oversampled for individuals with a history of ADHD and a history of persistent substance use, in order to fill a 2 × 2 design (ADHD diagnosis × persistent substance use). The interviews touched on a number of domains: views about their life, family, work, educational, and relationship experiences; self-perceptions of ADHD; and a number of questions about substance use (Jensen et al., 2018; Lasky et al., 2016; Mitchell et al., 2018; Swanson et al., 2018; Weisner et al., 2018). For some participants, additional data were collected from their parents (in separate interviews) about perceptions of their child’s life, whether they think they still have ADHD, relationships, medication use, and perceived need for and use of ADHD treatment (these latter variables have not yet been published).
In these articles, some findings differed as a function of ADHD diagnosis. For example, relative to the comparison sample, young adults with ADHD reported fewer positive and more negative role models in their lives. They also expressed fewer reasons not to use substances (Jensen et al., 2018). Individuals with ADHD who persistently used substances were more likely than those without ADHD to report using marijuana to achieve “stability” (e.g., reduced stress, self-medication, etc.), although the two subgroups did not significantly differ on other motivations for use (Swanson et al., 2018). Individuals with ADHD who persistently used substances often used cannabis to reduce negative mood; the majority of those individuals believed that cannabis improved their ADHD symptoms (Mitchell et al., 2018). Additionally, Weisner et al. (2018) explored beliefs about links between ADHD symptoms, substance use, and ADHD medication use, finding that most of the individuals with ADHD who persistently used substances did not believe that ADHD medication was related to later substance use (Weisner et al., 2018).
Both qualitative and quantitative data analyses revealed that young adults with and without ADHD often reported similar reasons for their decisions to use or abstain from substances (Weisner et al., 2018). For individuals with and without ADHD, those who abstained (i.e., those with no drug or heavy alcohol use) reported higher self-efficacy and a greater number of supportive people in their lives than did those who persistently used substances (Jensen et al., 2018). Furthermore, relative to those who had desisted from substance use, those who used substances reported more consequences (both positive and negative) associated with substance use, plus more social motivations for using substances (Jensen et al., 2018). Regardless of ADHD diagnosis, those who used substances persistently believed that cannabis enhanced positive mood, with this positive impact outweighing any perceived negative consequences (Mitchell et al., 2018).
An additional paper from the same dataset examined occupational outcomes in young adults with ADHD, particularly the perceived relation between work contexts and ADHD symptoms (Lasky et al., 2016). Young adults with ADHD reported fewer symptoms when engaged in stimulating work environments, described as busy, fast-paced, stressful, challenging, physically demanding, novel, and/or intrinsically interesting. In contrast, work environments lacking these features were often perceived to exacerbate symptoms. Some young adults with ADHD reported intentionally selecting jobs with stimulating work environments or found that they fit well in such settings once employed (“niche-picking”). Young adults also varied in how they viewed ADHD as part of who they are: Some described it as part of their character/personality; some used trait descriptions; and others described it as an external and past diagnosis (e.g., “I used to have it”) or something in between (e.g., “I still have ADHD but manage it when I need to”).
As summarized in Table 2, young adults with ADHD (diagnosed in childhood) often use substances in an effort to improve their mood or their ADHD symptoms (Jensen et al., 2018; Mitchell et al., 2018; Swanson et al., 2018) and report that the degree of their occupational impairment varies as a function of the suitability of or “fit” with their environment (Lasky et al., 2016). These narratives provide insight into adults’ understanding and self-construals of their ADHD and how they place such perceptions into contemporary contexts in their lives.
Preliminary analyses in a subsample of women with ADHD from the same dataset suggest that most young adult women have relatively positive outlooks on their lives (satisfaction, productivity) although many also report continued ADHD symptoms and few coping strategies for dealing with stress or ADHD (Rosenthal et al., 2024).
College Students With ADHD
Approximately 5.6% to 7.4% of college freshmen in the US have ADHD (Hotez et al., 2022; Stolzenberg et al., 2019). Understanding how these individuals navigate college is essential to helping parents, instructors, and universities best support them and promote academic and social success. Nine studies provided insight into the qualitative experiences of college students with ADHD, with sample sizes ranging from 10 to 36 (M = 18). Five such studies used semi-structured interviews, one used focus groups, and the remaining used other or unspecified interviews. In the only dual-informant qualitative study of its kind (with the exception of preliminary analyses using MTA data (with the exception of preliminary analyses using MTA data, Rosenthal et al., 2024), Sibley and Yeguez (2018) interviewed a diverse sample (21% Non-Hispanic White, 64% Hispanic, and 14% Mixed/Other) of both college students with ADHD (n = 13) and their parents to better understand factors that promoted and impaired success with the transition to college. Intrinsic and extrinsic motivation, self-efficacy, personal values, goals, and natural consequences served as powerful motivators for academic/vocational achievement. Viewed as particularly helpful were environments that fit the young adult, defined as “minimizing the impact of deficits and drawing on protective strengths such as high IQ, agreeable personality traits, or talents”—and those conveying reasonable demands (Sibley & Yeguez, 2018). Also perceived as helpful were educational resources, social support, and a balance of autonomy and support from families. Of the subsample taking stimulant medications, all found the medications helpful yet many also held reservations (see elaboration below). Both parents and young adults identified difficulties with organization, time management, self-awareness, and self/emotional control as salient. Young adults and parents reported that life stressors, change, excessive leisure activities, and comorbid anxiety/mood disorders exacerbated ADHD symptoms (Sibley & Yeguez, 2018).
More broadly, college students with ADHD discussed widespread challenges, including life skills (e.g., financial management, organization, eating habits, sleep, time management; Goffer et al., 2022; Lefler et al., 2016; Waite & Tran, 2010) and academic skills/achievement (Goffer et al., 2022; Lefler et al., 2016), as well as occupational, social, and emotional difficulties (Sibley & Yeguez, 2018; Waite & Tran, 2010). The independence required upon college entry, regarding both time and medication management, is often a considerable departure from pre-college expectations (Schaefer et al., 2017; Stevens et al., 2024). Factors thought to exacerbate challenges during the college transition included persistent ADHD symptoms, addictive behaviors, lack of social support (Meaux et al., 2009), time management difficulties (Schaefer et al., 2017), stress (Meaux et al., 2009; Sibley & Yeguez, 2018), parental over-involvement (Stevens et al., 2024), and co-occurring mental health challenges (Sibley & Yeguez, 2018). Participants also noted resources facilitating their success. In addition to formal psychosocial/organizational/academic interventions/groups for ADHD (Lefler et al., 2016), specific strategies included alarm setting (Goffer et al., 2022; Meaux et al., 2009), positive self-talk (Meaux et al., 2009), studying with friends (Goffer et al., 2022), academic accommodations, and ADHD medication (Goffer et al., 2022; Meaux et al., 2006, 2009; Sibley & Yeguez, 2018). Support from friends and parents was also viewed as critical (Meaux et al., 2009; Sibley & Yeguez, 2018; Stevens et al., 2024).
Across samples, participants reported that ADHD medication was often taken inconsistently or “as needed” but was also seen as helpful or necessary in achieving academic success (Loe & Cuttino, 2008; Meaux et al., 2006, 2009; Schaefer et al., 2017; Sibley & Yeguez, 2018; Waite & Tran, 2010). Concerns about stimulants included side effects (appetite loss, sleep problems, fatigue, social relations, etc.), lack of medication efficacy, feeling guilt/powerlessness for relying on medication to manage symptoms (Goffer et al., 2022), and feeling a loss of one’s usual personality when on medication (Loe & Cuttino, 2008; Meaux et al., 2006). A belief that one can outgrow ADHD also contributed to non-adherence among young adults (Schaefer et al., 2017). In a number of cases, college students with ADHD resumed taking medication after off-medication periods because of the high demands of college (Meaux et al., 2006). Despite impairment related to ADHD symptoms, use of academic accommodations was low (Waite & Tran, 2010). In fact, some participants reported that accommodations and support were critical for success, whereas others were unaware of their eligibility or feared stigma (Lefler et al., 2016; Meaux et al., 2009; Sibley & Yeguez, 2018).
In terms of perspectives on the diagnosis, most participants viewed the etiology of ADHD as largely biological (Waite & Tran, 2010). Lefler et al. (2016) found that some saw benefits to having the diagnostic label, whereas others felt stigmatized and embarrassed about the diagnosis. Many were reluctant to tell other people about their ADHD because of the fear of being perceived as “wanting drugs” (Meaux et al., 2006). Crucially, college students often felt pressured to share stimulants with others (Schaefer et al., 2017).
In summary, qualitative and mixed-methods studies reveal that college students with ADHD report a wide range of experiences, many different adaptations to manage the disorder, and diverse beliefs about what ADHD means for their college life (Table 3). Other themes involve struggles with independence along with core life and academic skills (Goffer et al., 2022; Lefler et al., 2016; Loe & Cuttino, 2008; Meaux et al., 2009; Schaefer et al., 2017). Sampled individuals often noted inconsistent usage of ADHD medications as well as complex feelings regarding both academic benefits and side effects (Goffer et al., 2022; Lefler et al., 2016; Loe & Cuttino, 2008; Meaux et al., 2006, 2009; Schaefer et al., 2017; Sibley & Yeguez, 2018; Waite & Tran, 2010). Academic accommodations appeared to be underutilized (Lefler et al., 2016; Meaux et al., 2009; Sibley & Yeguez, 2018; Waite & Tran, 2010).
ADHD Diagnosis in Adulthood
Eleven studies examined the qualitative experience of receiving an ADHD diagnosis in adulthood, with samples ranging from 5 to 40 participants (M = 13.6). Five obtained data using semi-structured interviews, five used other unspecified or open-ended interviews, and one utilized online narratives.
Participants commonly wished for an earlier diagnosis and felt anger, regret, or sadness about the time prior to their diagnosis (Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Stenner et al., 2019; Toner et al., 2006; Young et al., 2008). Many felt “different” from others while growing up without knowing why (Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Nielsen, 2017; Stenner et al., 2019; Toner et al., 2006; Young et al., 2008). Following diagnosis, many sought additional information about ADHD (e.g., Aoki et al., 2020; Toner et al., 2006) and believed the disorder was linked to biological causes (Nielsen, 2017).
An adult diagnosis of ADHD may well be met with conflicting emotions (Holthe & Langvik, 2017; Young et al., 2008). Many participants accepted the diagnostic label and thought it fostered help-seeking, experiencing relief and reduced self-blame post-diagnosis (Holthe & Langvik, 2017). Some now viewed ADHD as a part of their identity and believed the disorder was associated with both positive and negative traits (Aoki et al., 2020; Hansson Halleröd et al., 2015; Nielsen, 2017; Stenner et al., 2019; Young et al., 2008). For some, ADHD was described as a distinct part of themselves but not one that was “broken” (Nielsen, 2017). Perceived strengths associated with ADHD included creativity, hyper-focus, energy, and adventurousness (Fleischmann & Miller, 2013; Holthe & Langvik, 2017; Nyström et al., 2020; Sedgwick et al., 2019). In contrast, others reacted to their new diagnosis with hopelessness, expressed fears about ADHD limiting their future possibilities, or found the label itself confusing or difficult to accept (Aoki et al., 2020; Fleischmann & Miller, 2013; Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Holthe & Langvik, 2017; Nielsen, 2017; Toner et al., 2006; Young et al., 2008). In some cases, it forced individuals to grapple with their identity (Stenner et al., 2019) and with what was their “personality” versus their “ADHD” (Aoki et al., 2020). Self-stigma was common (Aoki et al., 2020; Holthe & Langvik, 2017). In addition, stigmatizing messages in the media and by close others discouraged disclosure (Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Toner et al., 2006; Young et al., 2008). Still, some felt confident disclosing their diagnosis to close friends/family (Aoki et al., 2020; Toner et al., 2006; Young et al., 2008).
Among those diagnosed with ADHD in adulthood, participants believed that ADHD contributed to impairment in many domains, including life skills (e.g., financial management, disorganization; Nystrom et al., 2020), emotion regulation (Fleischmann & Miller, 2013; Holthe & Langvik, 2017), and relationships (Fleischmann & Miller, 2013; Henry & Hill Jones, 2011; Nystrom et al., 2020; Toner et al., 2006). In an all-female sample, concerns about parenting and passing ADHD onto one’s children were raised (Holthe & Langvik, 2017). Factors believed to exacerbate difficulties included ADHD symptoms, comorbidities, academic underachievement, lack of fit in the workplace, and poor self-esteem (Toner et al., 2006). To manage ADHD, helpful strategies noted by participants included acquiring coping skills (e.g., setting alarms and writing things down, Aoki et al., 2020), creating structure/routines (Holthe & Langvik, 2017), receiving detailed instructions (Nystrom et al., 2020), workplace accommodations following disclosure (Aoki et al., 2020), physical activity/outdoor activities (Nystrom et al., 2020; Toner et al., 2006), and social support (emotional and instrumental, Holthe & Langvik, 2017; Nystrom et al., 2020). Work environments that were creative, challenging, and required changing locations were perceived to diminish symptoms or their impact (Nystrom et al., 2020). Medication to manage ADHD was believed to reduce symptoms and improve functioning, and in some cases were perceived to have secondary benefits for increasing one’s coping and decreasing one’s anxiety (Aoki et al., 2020; Holthe & Langvik, 2017; Nystrom et al., 2020; Toner et al., 2006; Young et al., 2008).
In summary, for many, receiving an ADHD diagnosis as an adult may have a distinct impact on self-perceptions and require identity re-negotiation. As might be expected in samples characterized by healthcare-seeking adults, individuals diagnosed with ADHD in adulthood often wished they had been diagnosed sooner (Fleischmann & Miller, 2013; Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Holthe & Langvik, 2017; Nielsen, 2017; Stenner et al., 2019; Toner et al., 2006; Young et al., 2008) and reacted to the diagnostic label with a wide range of emotions (Aoki et al., 2020; Fleischmann & Miller, 2013; Hansson Halleröd et al., 2015; Henry & Hill Jones, 2011; Holthe & Langvik, 2017; Nielsen, 2017; Stenner et al., 2019; Toner et al., 2006; Young et al., 2008). Irrespective of the integration of ADHD into one’s identity, those with adult-diagnosed ADHD reported considerable functional impairment (e.g., Henry & Hill Jones, 2011; Holthe & Langvik, 2017; Nystrom et al., 2020; Toner et al., 2006) and adopted a variety of coping strategies, including medication (Aoki et al., 2020; Hansson Halleröd et al., 2015; Holthe & Langvik, 2017; Nielsen, 2017; Nystrom et al., 2020; Toner et al., 2006; Young et al., 2008).
Other Studies
Finally, 16 studies, which appear to comprise 14 unique samples, did not differentiate between those diagnosed with ADHD as children and those diagnosed as adults. These studies had sample sizes ranging from 8 to 206 (Mean = 37; Median = 17). Eleven used semi-structured interviews, two used focus groups, one used both semi-structured interviews and focus groups, one used an online questionnaire, and another used an unspecified form of interview.
In one of the largest samples of its kind, Brod et al. (2012) conducted focus groups with 108 participants across seven countries to explore the experience of ADHD and its impact on various life domains. Only 27% of such participants were diagnosed with ADHD in childhood. Adult symptoms were believed to influence many domains of life, including work, financial management, and social relationships, which contributed to low self-esteem (Brod et al., 2012). Risky behaviors (e.g., risky driving, substance misuse, eating disorders) were also commonly observed. Most participants had a history of trying ADHD medications, though many stopped due to perceived side effects or lack of efficacy (Brod et al., 2012). Some self-medicated with alcohol or drugs for ADHD symptoms. Many viewed ADHD as “part of who they are.”
Individuals with comorbid substance use disorder (SUD) and ADHD reported that “jumbled” thoughts and emotions contributed to substance use (Kronenberg et al., 2014, 2015). Similarly, many viewed nicotine or other substances as “self-medication” to reduce restlessness and promote concentration/relaxation (Liebrenz et al., 2014; Nehlin et al., 2015). Interestingly, many reported that smoking cessation worsened ADHD symptoms after physical symptoms of withdrawal stopped (Liebrenz et al., 2016). Individuals diagnosed with both SUD and ADHD often believed that ADHD medication helped them to remain abstinent (Kronenberg et al., 2015); those addicted to nicotine had more varied beliefs about the impact of stimulants on the risk of later nicotine use (Liebrenz et al., 2014).
In the literature more broadly, individuals with ADHD believed that the disorder contributed to interpersonal challenges (conflict, inconsistent communication, etc.; Ginapp et al., 2023; Matheson et al., 2013; Oscarsson et al., 2022), stress (e.g., Oscarsson et al., 2022), sleep problems (Matheson et al., 2013), and emotion dysregulation (Matheson et al., 2013; Oscarsson et al., 2022). A number of studies reported that individuals with ADHD find it difficult to manage job demands (Ek & Isaksson, 2013; Lyhne et al., 2021; Matheson et al., 2013; Oscarsson et al., 2022; Schreuer & Dorot, 2017), especially jobs with repetitive and boring tasks as well as those lacking in structure, organization, and managerial support (Oscarsson et al., 2022).
Adults with ADHD endorsed a variety of strategies to cope with disorder-related challenges, including technology, creating routines and structure, physical activity, and selecting environments without distractions (Canela et al., 2017; Ek & Isaksson, 2013; Ginapp et al., 2023; Kronenberg et al., 2014; Lyhne et al., 2021; Oscarsson et al., 2022; Schreuer & Dorot, 2017; Schrevel et al., 2016). Social compensatory strategies and the use of prescribed (e.g., stimulants) and other substances (e.g., alcohol, cocaine, etc.) were also discussed (Canela et al., 2017). Within the workplace, in addition to medication, adapted environments or expectations (Ek & Isaksson, 2013; Oscarsson et al., 2022; Schreuer & Dorot, 2017), clear and well-defined goals, structure, breaks, assistive technology (Ek & Isaksson, 2013), and social support/motivation (Ek & Isaksson, 2013; Lyhne et al., 2021; Oscarsson et al., 2022; Schreuer & Dorot, 2017) were perceived as promotive of success.
Medication was viewed as valuable for managing symptoms (Oscarsson et al., 2022; Redshaw & McCormack, 2022; Schreuer & Dorot, 2017). For some, it was necessary but not sufficient to reduce impairment (Matheson et al., 2013). Barriers to adherence included forgetfulness, side effects, uncertainty about effectiveness, and fears of/inner conflict about loss of identity/authenticity on medication (Matheson et al., 2013; Redshaw & McCormack, 2022). Externally, difficulty accessing medical services for diagnosis or treatment contributed to nonadherence for some (Matheson et al., 2013).
Self-acceptance for adults with ADHD was facilitated by increasing self-knowledge, effective communication, and gaining an understanding of their positive characteristics (Schrevel et al., 2016). However, experiences regarding acceptance from others varied—some participants chose not to disclose their diagnosis because loved ones did not understand or take the disorder seriously (Ginapp et al., 2023) or because of prior negative experiences with workplace disclosure (Oscarsson et al., 2022). Although some individuals reported few if any advantages to ADHD (Oscarsson et al., 2022), in other samples, most adults with ADHD noted at least one positive feature of the disorder (Schippers et al., 2022). 1 These strengths included problem-solving (Oscarsson et al., 2022; Redshaw & McCormack, 2022; Schippers et al., 2022; Schreuer & Dorot, 2017; Schrevel et al., 2016), creativity (Brod et al., 2012; Oscarsson et al., 2022; Schippers et al., 2022; Schreuer & Dorot, 2017; Schrevel et al., 2016), high energy (Redshaw & McCormack, 2022; Schippers et al., 2022; Schreuer & Dorot, 2017), adventurousness/spontaneity (Redshaw & McCormack, 2022; Schippers et al., 2022), and hyper-focus (Oscarsson et al., 2022; Redshaw & McCormack, 2022; Schippers et al., 2022).
In summary, many studies either did not specify the age of diagnosis or had mixed samples with some recently diagnosed as adults and others diagnosed in childhood (often weighted toward the former; see Table 5). Persistent symptoms were perceived as contributing to continued impairment in many domains, including work (Brod et al., 2012; Canela et al., 2017; Lyhne et al., 2021; Oscarsson et al., 2022; Schrevel et al., 2016). Finally, those with ADHD and substance use challenges often viewed ADHD symptoms as contributing to substance use (Brod et al., 2012; Canela et al., 2017; Kronenberg et al., 2014, 2015; Liebrenz et al., 2014; Nehlin et al., 2015).
Discussion
We review the qualitative literature on ADHD in adulthood among four different subgroups: those with a childhood ADHD diagnosis; college students with ADHD; those diagnosed with ADHD in adulthood; and mixed/other. Some themes were noted across some subgroups, including substance use (perceptions of and reasons for use); use of stimulant medication to manage ADHD symptoms (perceptions of and frequency of use); life domains negatively affected by symptoms; strategies and accommodations used to manage symptoms, including selecting conducive environments; perceptions of ADHD as an identity and beliefs about/experiences with stigma and disclosure; and perceived positive aspects of ADHD. Tables 2 to 5 present summaries of qualitative findings related to these major themes for each subgroup.
All qualitative studies of adults with childhood-diagnosed ADHD were from the MTA and many emphasized reasons for substance use (often stability and abating ADHD symptoms or negative mood; Jensen et al., 2018; Mitchell et al., 2018; Swanson et al., 2018). Other studies highlighted reduced levels of self-reported impairment in conducive environments (Lasky et al., 2016). Future research on this subpopulation should explore (a) why many of those diagnosed with ADHD in childhood no longer pursue treatment as adults; (b) why some individuals continue to identify with the ADHD diagnosis whereas others do not, and the relation between this identification (or lack thereof) and well-being; and (c) the types of interventions, discussions, or psychoeducation that may contribute to continued, effective, and independent management of ADHD into young adulthood and beyond.
Next, qualitative research highlights that college students with ADHD experience impairment in many domains (Goffer et al., 2022; Lefler et al., 2016; Sibley & Yeguez, 2018; Waite & Tran, 2010) and that both specific strategies—particularly social support plus environmental “fit”—are believed to facilitate success (Goffer et al., 2022; Meaux et al., 2009; Sibley & Yeguez, 2018). Although ADHD medication was viewed as crucial for some students, medication was taken with variable regularity and yielded mixed emotions (Goffer et al., 2022; Lefler et al., 2016; Meaux et al., 2006, 2009; Sibley & Yeguez, 2018; Waite & Tran, 2010). Similarly, academic accommodations were viewed as necessary by some students but were unused by many others (Lefler et al., 2016; Meaux et al., 2009; Schaefer et al., 2017; Sibley & Yeguez, 2018; Waite & Tran, 2010). Outside of qualitative research, the efficacy of many ADHD-related accommodations has received decidedly inconsistent support (Lovett & Nelson, 2021). Further investigation is required regarding (a) the qualitative and quantitative factors earlier in development that predict college enrollment, retention, and success among individuals with ADHD—with emphasis on contextual or motivational factors that can be targets of future interventions; (b) contributors to the lack of uptake in academic accommodations among college students with ADHD, as well as potentially modifiable factors that cause difficulty in navigating college life; (c) motivations, attitudes, and beliefs about the benefits of medication (and psychological) treatments; and (d) ways in which colleges and universities can leverage supports/motivations that are salient for individuals with ADHD (for instance, those discussed by Sibley and Yeguez, 2018).
Third, for those diagnosed with ADHD in adulthood, qualitative studies often focused on how the diagnostic label was viewed and incorporated into one’s identity, sometimes leading to re-negotiation of identity, re-interpretation of past behaviors, and mixed emotions (but often relief; Aoki et al., 2020; Holthe & Langvik, 2017; Stenner et al., 2019; Young et al., 2008). Similar to ADHD detected earlier in life, ADHD diagnosed in adulthood contributed to challenges in emotional and social functioning, among other domains (Henry & Hill Jones, 2011; Nystrom et al., 2020; Oscarsson et al., 2022; Redshaw & McCormack, 2022). It is notable that in these studies, some or all participants actively sought out this ADHD diagnosis as an adult, implying significant adult impairment, knowledge of ADHD, and access to healthcare resources. Thus, these individuals’ attitudes, feelings, and treatment-seeking behaviors may diverge from those who received the diagnosis as children. For individuals diagnosed with ADHD as adults, future qualitative research should explore (a) the presenting problem(s) motivating individuals to seek out the psychological/psychiatric services that result in diagnosis (e.g., ADHD symptoms? Co-occurring mental health conditions? Was a child of theirs diagnosed with ADHD?); (b) how and why strategies, conceptions, and treatment decisions related to ADHD (and co-occurring symptoms) are similar to or different from those with ADHD who were diagnosed earlier in life.
Gaps and Areas for Future Research
We highlight underexplored areas where we believe it is important for future research to incorporate a qualitative approach. These areas are crucial to better understand the experience of adults with ADHD and inform treatment of ADHD.
Multiple Reporters
Past quantitative research on ADHD suggests that, both in childhood and beyond, those with ADHD may underestimate the degree of their symptoms and impairment relative to close others (e.g., parents, teachers, or spouses; Barkley et al., 2011; Bourchtein et al., 2017; Sibley et al., 2012). Indeed, diagnostic best practices highlight the importance of obtaining reports of symptoms from multiple raters/informants to ensure the diagnosis is accurate, particularly in adulthood (e.g., Sibley et al., 2017). Only one study obtained qualitative accounts from multiple reporters in adults with ADHD (Sibley & Yeguez, 2018). This study compared a group of post-secondary students with ADHD and a group of their parents but did not explore potential (dis)agreement within each dyadic parent/child pair (Sibley & Yeguez, 2018). Obtaining and comparing interviews from multiple perspectives may be crucial to understanding daily functioning and well-being in adults with ADHD, as well as the extent or efficacy of coping strategies. These alternate reporters need to be individuals who see the participant regularly—and in settings where symptoms may be evident. Such additional perspectives may provide a more comprehensive understanding of the experiences of adults with ADHD and additional insight into the nature of and the factors contributing to inter-reporter discrepancies in adulthood.
Children With ADHD as Adults
Only 5 of the 41 studies reviewed (12.2%) focus on adults who had received a childhood ADHD diagnosis, and all of these used qualitative data from the MTA study. This unique subpopulation is not fully captured by qualitative investigations into college students with ADHD or adults who receive an ADHD diagnosis in adulthood. College students with ADHD may have levels of academic achievement or support that are not representative of all adults who grew up with ADHD. As such, their perceptions may not generalize to those with ADHD who did not pursue a four-year degree. Furthermore, many studies emphasize how receiving a new ADHD diagnosis as an adult leads to redefining past experiences and reconsidering future expectations, suggesting that this experience is phenomenologically distinct. Qualitative research on college students may benefit from distinguishing among those who were diagnosed in childhood versus during college or young adulthood, as these subgroups may reflect quite different experiences navigating college life, healthcare systems, and educational accommodations.
Topics related to identity and self-understanding were sparse in qualitative studies of adults with ADHD who were diagnosed as children. Identity and self-perceptions change across life and have an immense impact on how individuals set expectations for the future and derive meaning from their experiences (Eccles, 2009). It is important for future work to elucidate (a) how individuals who grew up with an ADHD diagnosis and associated symptoms and stigma navigate adulthood, (b) how this process may relate to decisions about why and whether to (dis)engage with treatment, and (c) what interventions or supports during adolescence would encourage empowerment, self-management, and treatment engagement in adulthood for those who have grown up with ADHD.
Experiences of Women With ADHD
As reviewed by Hinshaw et al. (2022), girls and women have been and continue to be underrepresented in the ADHD literature both qualitatively and quantitatively. Concerns about birth control, parenting, and pregnancy may be important to women with ADHD, and decisions about whether and when to take medication may reflect considerations of reproductive and parenting intentions. Although both parents must be responsible for caring for and raising a child, disproportionate levels of household work are often placed on women in romantic or marital relationships (Coltrane, 2004). Tackling these important life tasks and challenges may be particularly salient and difficult for women with ADHD. Besides female-specific concerns, recent work in science generally and ADHD specifically has emphasized that the experiences of males/men cannot be considered the default, and those who identify as women have unique and valuable experiences that must be represented in research (see also Hinshaw et al., 2022; Young et al., 2020). As well, the lived experiences of gender diverse and transgender individuals with ADHD are completely understudied (Goetz & Adams, 2024), even though these individuals have unique perspectives shaped by their intersecting identities and resulting experiences. Navigation of life cycle transitions, treatment decisions, and overall daily functioning for women, nonbinary, gender fluid, and transgender individuals with ADHD are nuanced and complex, with the potential to be uniquely captured by qualitative approaches.
Diverse Demographic Groups
People who identify as members of historically marginalized racial or ethnic groups may have unique experiences with ADHD and its treatment, although these perspectives have not been well-captured in either qualitative or quantitative research. Only 39.0% of reviewed studies reported the racial/ethnic breakdown of their samples (16); among these, only 2 (12.5%) analyzed samples that were not ≥70% non-Hispanic White. In the United States, white youth are disproportionately likely to receive an ADHD diagnosis and treatment, which is thought to reflect unmet needs rather than true underlying racial differences in the rate of ADHD (Shi et al., 2021).
Structural barriers combined with intersecting marginalized identities are likely to affect the meaning-making process related to ADHD, including attitudes about oneself and the disorder, treatment/accommodation-seeking behavior, and willingness to disclose one’s diagnosis (Bailey et al., 2014; Fadus et al., 2020; Hervey-Jumper et al., 2008). They may also influence how healthcare systems and close others perceive, interpret, and respond to one’s ADHD symptoms and efforts to cope (Bailey et al., 2014; Fadus et al., 2020; Hervey-Jumper et al., 2008).
Cross-cultural and international studies of how ADHD is clinically and culturally defined can highlight differences in how ADHD is identified, understood, described, and treated by international medical systems/communities. These should include qualitative and ethnographic research methods. In sum, understanding the experiences, attitudes, and strengths of diverse adults with ADHD both in the US and abroad is a crucial gap for future qualitative and mixed-methods work to fill.
Wider Age Range of Adults With ADHD
Although ADHD was once thought of as a childhood-limited disorder, in recent decades, the disorder’s continued impact into adulthood has been increasingly acknowledged (e.g., Sibley et al., 2022). Prior quantitative work has highlighted the continuity of ADHD symptoms into older adulthood (Semeijn et al., 2016) as well as continued ADHD-related impairment, which may interact with normative age-related challenges (for a review, see Fischer & Nilsen, 2024). However, on the whole, older adults (50+) with ADHD have been understudied in both the qualitative and quantitative literature. Although two of the reviewed studies specifically highlighted the experiences of older adults with ADHD (Henry & Hill Jones, 2011; Nystrom et al., 2020; all diagnosed age 40+), continued qualitative research can and should explore how individuals with ADHD navigate the disorder across the lifespan and into old age. It will be important to understand how older adults with ADHD deal with age-related changes in physical and cognitive abilities; decisions about retirement; (for some) roles as parents or grandparents; and an ever-changing landscape of government benefits and health insurance. This work may highlight areas where additional support and services can be provided to promote health-related quality of life among older adults with ADHD and their families.
Conclusions and Implications
Qualitative and mixed-methods research on ADHD has contributed greatly to our understanding of the impact, coping strategies, treatment decisions, and complex identities of adults with ADHD in ways that complement and extend existing quantitative research. Identity, decisions about disclosure, and perceived symptoms/domains of impairment show both important similarities as well as differences with respect to the timing of diagnosis (e.g., childhood vs. adulthood diagnosis) and sample composition (e.g., college students vs. general adults). Clinically, it is important to consider and explore how and whether individuals identify with the disorder and the degree to which they believe symptoms are present and impairing, as such perceptions have marked implications for willing-ness to seek out and engage with treatment. Highlighting developmentally specific ADHD-related concerns, for instance, while navigating college, parenting, retirement, menopause, and the menstrual cycle, will be critical for future qualitative and quantitative research to further individualize therapeutic treatment.
Future research incorporating qualitative methods should extend current work by emphasizing (1) multiple reporters; (2) individuals who were diagnosed with ADHD as children, and their perspectives and healthcare needs as adults; (3) experiences of women and gender-diverse individuals; and (4) demographically diverse samples (in terms of culture, race/ethnicity, and age). These foci will be essential to increasing the field’s knowledge of the impact of ADHD on adults in ways that can inform the implementation of treatments, coping strategies, and accommodations that are more accessible, evidence-based, and helpful for adults with ADHD, most of whom continue to struggle with the disorder despite positive aspects and strengths.
Footnotes
Author Contributions
EAR, PSJ, JTM, and TW conceived of the project. JTM, TW, and PSJ provided feedback on searches and project scope, as did LTH and LGA. EAR developed the search strategy, conducted searches, wrote the manuscript, edited the manuscript, and supervised CY and NS. NS conducted searches, extracted information, and provided feedback on the manuscript. CY extracted data from papers and produced tables. JTM, TW, PSJ, LTH, LGA, and SPH reviewed and provided feedback on the manuscript as well as supervision. All authors reviewed the manuscript.
Data Availability Statement
This review paper relied on published papers, which are available via their journal websites.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SPH receives grant support from the National Institute of Mental Health as well as book royalties from Oxford University Press, St. Martin’s Press, Wiley, Guilford, and Ballantine. JTM acknowledges research support, consulting, and/or royalties from Guilford Press, Lumos Labs, MindFit, and Keller Postman LLC over the past 2 years. No other authors have competing interests to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations and Consent to Participate Statements
As this is a review and synthesis of existing publications, this project did not require ethical approval.
Consent for Publication
Not applicable.