
Abstract
Objective:
Attention-Deficit/Hyperactivity Disorder (ADHD) is a common behavioral health condition that impacts 5% to 8% of children and 2.5% of adults worldwide. The symptoms of ADHD are effectively managed with medication, yet patients with ADHD may inconsistently take their medication. We assessed medication adherence among patients with ADHD and identified factors associated with medication adherence that may be utilized to optimize adherence.
Method:
This is a retrospective, observational study among patients aged 4 years and older with a diagnosis of ADHD at primary care and multispecialty outpatient clinics during May 2021 to May 2023. We assessed sociodemographic characteristics, stratified by medication adherence status (Percentage of Days Covered ≥ 80%) using simple proportion, Student’s t-test, and Chi-square test. We conducted univariable and multivariable logistic regression analyses to assess potential medication adherence factors, including sociodemographic characteristics, depressive symptoms, suicide risk, health service utilization, and social determinants of health (SDOH).
Results:
We found 7,661 patients diagnosed with ADHD, with a mean (SD) age of 21.8 (14.8) years. The ADHD prevalence was 5.5% for patients aged 4 to 12, 4.4% for 13 to 17, and 0.8% for 18+ years old. Most patients were male (56.9%), non-Hispanic White (37.6%), and privately insured (55.1%). Among these patients, only 4,242 (55.4%) were treated with medication. Among 4,011 patients with medication adherence information, the average adherence rate was 56%, and only 1,113 patients (27.5%) met our threshold for adherence to ADHD treatment (80%). Adherence was positively associated with being adults, having more BH and PCP visits, and negatively associated with racial and ethnic minorities and more severe depressive symptoms.
Conclusion:
Only half of patients with ADHD were treated with medication. Of those treated, less than a third adhered to medication. Age, race and ethnicity, depressive symptoms, and BH and PCP visits were statistically associated with medication adherence. Healthcare providers may need to address factors such as coexisting depressive symptoms, and unmet SDOH needs to improve medication adherence among patients with ADHD. Also, patients reaching adolescence may need enhanced medication management.
Background
Attention-Deficit/Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterized by persistent patterns of inattention, hyperactivity, and impulsivity. It is a common behavioral health condition, impacting 5% to 8% of youth and 2.5% of adults worldwide (Baweja et al., 2021; Biederman et al., 2019; Faraone et al., 2021; Polanczyk et al., 2014). It is usually first diagnosed in childhood and often lasts into adulthood. ADHD is associated with significant impairments across life domains, including mental health challenges like anxiety, depression, and substance use disorders, as well as educational, social, and occupational difficulties (French et al., 2024). Children and young adults with ADHD face increased risks of self-harm, delinquent behavior, academic underachievement, and health issues such as obesity and risky behaviors, which also impact their families’ well-being (French et al., 2024). In adulthood, ADHD is linked to poorer mental and physical health, lower quality of life, and elevated risks of accidents, suicide, and early mortality (French et al., 2024). With various associated adverse outcomes, ADHD imposes a substantial economic burden that is mostly driven by educational costs, direct healthcare costs, and caregiver costs on individual patients, families, and societies. The most recent study estimated the excess costs incurred by an individual with ADHD compared to an individual without ADHD in the US in 2018 at $19.4 billion among children ($6,799 per child) and $13.8 billion among adolescents ($8,349 per adolescent) (Doshi et al., 2012; Faraone et al., 2021; Polanczyk et al., 2014).
Medication is a cornerstone of ADHD multimodal treatment, reducing symptoms and improving daily functioning and long-term outcomes (Faraone et al., 2021). ADHD medication adherence was found to be associated with fewer adverse health outcomes among older adolescents transitioning to adulthood, especially among females (Rao et al., 2021). However, despite the proven efficacy of ADHD medications, adherence to these treatments remains a significant challenge (Baweja et al., 2021). Research consistently highlights suboptimal adherence rates that can be as low as 22% after 12 months among individuals with ADHD across different age groups (Ferrin et al., 2024). Less than half (46%) of children with ADHD were adherent to treatment with stimulants, and only 42% of adults with ADHD renewed their prescriptions on time (Biederman et al., 2019, 2020; Parkin et al., 2022). Challenges extend beyond individual-level factors, such as knowledge and self-efficacy, encompassing a broader spectrum of influences at various levels. The presence of comorbid conditions like depression and suicide risk, as well as the influence of socioeconomic factors and social determinants of health (SDOH), adds complexity to the landscape of ADHD medication adherence.
Among youth, many factors impact medication adherence. Parents’ or caregivers’ attitudinal barriers or lack of family support, cultural or social stigma, negative beliefs about ADHD medication, lack of parental/caregiver knowledge about ADHD, low income, low education level, and low self-efficacy may hinder medication adherence for children (Baweja et al., 2021; Boudreau & Mah, 2020; Ferrin et al., 2024; Khan & Aslani, 2020; Parkin et al., 2022). Additional factors related to poor ADHD medication adherence include comorbidities, lower intelligence quotient (IQ), family history or impaired family dynamics, multiple dosing, ineffectiveness or side effects from medication, less trustful physician-patient relationship and the use of short-acting medication (Ferrin et al., 2024). Racial/ethnic disparities are observed, with some minorities, such as African American and Hispanic children, exhibiting lower rates of ADHD medication persistence and adherence (Cummings et al., 2017; Ji et al., 2018). As adolescents gradually assume responsibility for their healthcare, unresolved challenges persist, and additional disparities emerge. Among adolescents, adherence declines with age and is worse for males and those with lower income (Rao et al., 2021).
Comorbid conditions, such as oppositional defiance disorder (ODD), depression, and suicidality, are other factors that may impact ADHD medication adherence (Jeun et al., 2024). From children to adults, those with ADHD are at a higher risk of an earlier age of depression onset, higher depression-associated impairment, a greater recurrence of depressive episodes, and increased persistence of subthreshold depression symptoms (Mochrie et al., 2020; Nigg et al., 2020; Powell et al., 2021). ADHD is associated with an elevated risk of suicide, however, medication treatment can mitigate this risk, underscoring the importance of consistent adherence (Liang et al., 2018; Shoval et al., 2021; Taipale et al., 2024).
Healthcare utilization patterns also impact medication adherence. Structural barriers to healthcare, including treatment availability, further reduce treatment engagement (Baweja et al., 2021). Patterns of healthcare utilization play a crucial role in the overall management of ADHD. A study conducted by Jeun et al. (2024) reveals that adherent patients exhibit a higher utilization of outpatient visits and prescription refills, highlighting the significance of these services in promoting treatment adherence.
Other factors that may impact general medication adherence are social determinants of health (SDOH), which are non-medical factors that impact a person’s health and well-being (Davis et al., 2021; Green et al., 2020; Mensah & Riley, 2021; Rao et al., 2021; Wilder et al., 2021). Food insecurity, discrimination, housing instability, poor health literacy, and costs negatively influenced adherence behaviors (Davis et al., 2021; Green et al., 2020; Mensah & Riley, 2021; Praska et al., 2005; Rao et al., 2021; Wilder et al., 2021). There is a very limited understanding of the relationship between SDOH and ADHD medication adherence specifically (Davis et al., 2021; Green et al., 2020; Rao et al., 2021; Wilder et al., 2021).
While numerous studies have investigated ADHD medication adherence (Biederman et al., 2019, 2020; Boudreau & Mah, 2020; Canfield et al., 2019; Charach & Fernandez, 2013; Cummings et al., 2017; Ferrin et al., 2024; Horne et al., 2005; Jeun et al., 2024; Ji et al., 2018; Lawson et al., 2012; Parkin et al., 2022; Praska et al., 2005; Rao et al., 2021; Wilder et al., 2021), notable gaps persist in the literature. Previous research has often focused on cross-sectional designs using specific age groups, such as only children up to age 18 or adults, limiting our understanding of ADHD medication adherence patterns across the lifespan (Biederman et al., 2019; Boudreau & Mah, 2020; Charach & Fernandez, 2013; Cummings et al., 2017; Ferrin et al., 2024; Horne et al., 2005; Jeun et al., 2024; Khan & Aslani, 2020; Parkin et al., 2022; Wilder et al., 2021). Existing studies have often been limited to hospital or mixed settings, overlooking the unique challenges present in outpatient settings alone (Biederman et al., 2019, 2020; Boudreau & Mah, 2020; Canfield et al., 2019; Charach & Fernandez, 2013; Wilder et al., 2021). Earlier studies have found barriers to adherence in traditional outpatient settings, such as accessibility, particularly among racial and ethnic minorities (Ferrin et al., 2024). Our study is among the first to examine if SDOH factors may have an association with ADHD medication adherence. Altogether, results on factors associated with ADHD medication adherence remain underexplored and inconsistent.
Therefore, this study assessed factors associated with medication adherence among patients with a diagnosis of ADHD who received primary care and multispecialty care services in an outpatient urban setting. We evaluated differences in multiple factors, including sociodemographic characteristics, depressive symptoms, suicide risk, health service utilization, and SDOH, between those who were adherent to ADHD treatment and those who were not.
Methods
Study Design and Population
This was a retrospective, observational study of patients aged 4 years and older who had an encounter at UT Physicians (UTP) primary care and multispecialty care clinics during May 2021 to May 2023 and a diagnosis of DSM-5 ADHD identified by ICD-10 codes F90.0-F90.9 from Epic, the electronic health record (EHR) system (Epic Systems Corporation, n.d.), during that period. UT Physicians is the practice plan of the UTHealth McGovern Medical School in the Greater Houston Metropolitan area, Texas.
Measures
We utilized the EHR data including sociodemographic information, diagnosis, medication prescriptions, screenings for depressive symptoms, suicide risk, SDOH, and behavioral health/primary care visits during May 2021 to May 2023. If the patient had more than one record for depressive symptoms, suicide risk, and SDOH, the most recent valid records were used for the analyses.
Medication Adherence
Broadly, adherence is defined as “the extent to which a person’s behavior (e.g., taking medication) corresponds with agreed recommendations from a health care provider” (Horne et al., 2005; Sabaté, 2003). Medication adherence from pharmacy databases is commonly measured by the proportion of days covered (PDC). It is calculated as the number of days with drug on hand divided by the number of days in the specified time interval (Canfield et al., 2019; Hess et al., 2006; Prieto-Merino et al., 2021). PDC is the preferred method to measure medication adherence for chronic drug therapies (Pharmacy Quality Alliance, 2019). The PDC can be used as a continuous measure or a dichotomous variable. The PDC threshold is the level above which the medication is reasonably likely to achieve the most clinical benefit. Clinical evidence has widely supported a threshold of 80% for adequate adherence to most medications (Baumgartner et al., 2018; Gellad et al., 2017; Sabaté, 2003). Previous studies have used PDC thresholds of 70% and 80% for ADHD medication adherence (Gajria et al., 2014). We used the stricter criteria of medication adherence (PDC ≥ 80%) in our study. The analysis of medication adherence was limited to medication(s) prescribed for the management of ADHD only. We used the most recent medication adherence rates, calculated as the PDC score for the medication group, obtained at the most recent visit. The system calculates PDC based on the patient’s most current outpatient medication list in Epic with the number of times a medication has been dispensed, also known as the length of time the current medication prescription has been active. The PDC accounts for times when the dispense history in the EHR may not be up to date. Hence, the lack of dispenses during that period does not negatively affect the PDC. The mean PDC for each patient was then calculated. Medication adherence rate, using patient mean PDC, was measured as a continuous and dichotomous variable (PDC ≥ 80%).
Sociodemographic Characteristics
Sociodemographic information was extracted from Epic. We used the following categories for each listed variable: age at the beginning of the study period (4–12 years, 13–17 years, and 18+ years), sex (male and female), race/ethnicity (Hispanic, non-Hispanic White, non-Hispanic Black, and Others (non-Hispanic American Indian or Alaska Native, Asian, Native Hawaiian or Pacific Islander or Other), and medical insurance (Private insurance, Medicaid, Medicare, Other government insurance, and Others).
Depressive Symptoms
Depressive symptoms were assessed by the self-reported Patient Health Questionnaire-9 (PHQ-9) and stored in Epic (Kroenke et al., 2001). Patients who are 12 years and older were screened for depressive symptoms and suicidality using the PHQ-9 annually. The revised version of PHQ-9 was used for younger ages. Severity was categorized as: none to minimal (score 0–4), mild (scores 5–9), moderate (scores 10–14), moderately severe (scores 15–19), and severe (scores 20–27).
Suicide Risk
We utilized question 9 of the PHQ-9 (“Thoughts that you would be better off dead or hurting yourself in some way”) to assess suicidal risk. Positive responses to question 9 of the PHQ-9 (Several days, More than half the days, and Nearly every day) were categorized as having suicide risk.
Health Service Utilization
We assessed the average number of behavioral health (BH) visits and primary care provider (PCP) visits per year. BH visits include an in-office or telehealth visit with BH professionals (psychiatrist, psychologist, neuropsychologist, clinical social worker, family nurse practitioner) in psychiatry or psychology departments. PCP visits included an in-office or telehealth visit with pediatricians, family medicine, or internal medicine. Only BH and PCP visits with an associated diagnosis of ADHD and visits after the earliest ADHD diagnosis during the study period were included in the analysis. We only included patients who have at least 1-year duration of diagnosis in the regression analyses. We adjusted the number of BH and PCP visits per year by the duration of the diagnosis (from the earliest ADHD diagnosis since May 2021 to the end of the study period of May 2023).
Social Determinants of Health
For the pediatric population, we screened for age-appropriate SDOH domains using the validated questionnaires during a well-child visit. Among the adult population, we screened for SDOH annually. We followed up as needed if patients screened positive for any domains. We assessed patients for financial resource strain, housing instability, health literacy, transportation, and food insecurity, which are the five domains commonly screened for across the pediatric and adult populations (Supplemental Appendix A). Only assessments prior to the latest medication prescriptions were included in the analysis. Answers for these SDOH domains were then recategorized into a dichotomous variable “At risk” when patients were screened positive for at least one of the domains (“At risk,” “High risk,” or “Medium Risk”) and “No risk” when patients had no positive responses to all of these domains during the valid study period.
Types of Prescribers
We assessed the types of prescribers for ADHD medication by using encounter information from the provider specialty and clinic departments. We categorized prescribers into five groups: (1) PCP only, (2) BH providers only, (3) both PCP and BH providers, (4) PCP and/or other specialists such as a neurologist, and (5) unknown prescriber.
Statistical Analyses
We assessed sociodemographic characteristics (age, sex, race/ethnicity, insurance) stratified by medication adherence status (adherence vs. non-adherence using an 80% cut-off) using simple proportion, Student’s t-test, and Chi-square test. Univariable and multivariable logistic regression analyses were conducted to evaluate potential factors related to medication adherence, adjusting for sociodemographic characteristics, depressive symptoms, suicide risk, type of prescriber, health service utilization, and SDOH. Multivariable linear regression analysis was also conducted to examine how these factors were associated with medication adherence when medication adherence was measured continuously. All analyses were conducted in Stata SE V.14 (StataCorp, 2015). Statistical significance was defined as a two-sided p-value < 0.05 for all comparisons. This study was approved by the Institutional Review Board at the University of Texas Health Science Center at Houston.
Results
Among 523,406 patients who received primary care or specialty care services at the outpatient clinics from May 2021 to May 2023, we identified 7,661 patients with ADHD, with a mean (SD) age of 21.8 (14.8) years and a median age of 16 years. The ADHD prevalence was 5.5% for patients aged 4 to 12, 4.4% for 13 to 17, and 0.8% for 18+ years old. Just over half the sample of patients with ADHD were male (56.9%) and privately insured (55.1%). The sample was racially and ethnically diverse, including 37.6% non-Hispanic White, 22.8% non-Hispanic black, and 18.7% Hispanic. Among these patients, only 4,242 (55.4%) were treated with medication, and 4,011 patients had non-missing medication adherence information. Among 4,011 patients with medication adherence information, the average adherence rate was 56%, and only 1,113 patients (27.5%) met our threshold for adherence to ADHD treatment (PDC ≥ 80%) There was a statistically significant difference in the patient’s mean adherence rate among different age groups (p < .005), with the 18+ years old having the highest mean adherence rate (58.4%), followed by the 4 to 12 years old (56.9%) and the 13 to 17 years old having the lowest mean rate of 49.4%. Figure 1 presents the distribution of the study population by treatment status, adherence status, and age group. Figure 2 displays the flow chart of the selection of the study analytical populations. In the analysis of factors associated with medication adherence, the analytical population consisted of 1,774 patients with ADHD who had ADHD diagnosis for at least 1 year, valid, non-missing medication adherence information and assessments. In the subgroup analysis that considered SDOH’s impact on medication adherence, the analytical population consisted of 510 patients with no missing data on relevant measures.
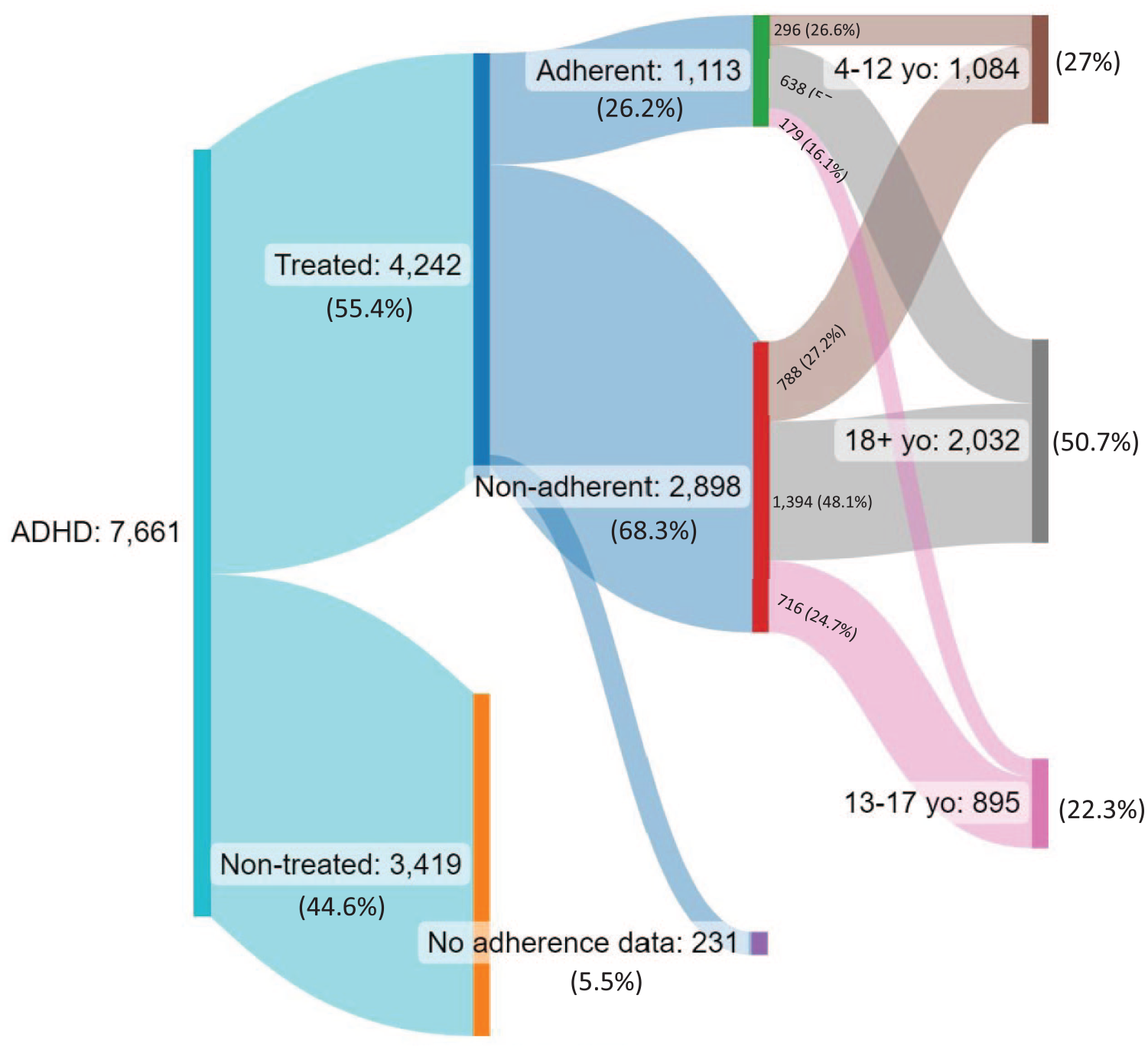
Sankey diagram of medication treatment and adherence to treatment (PDC ≥ 80%) in 7,661 outpatients with ADHD.
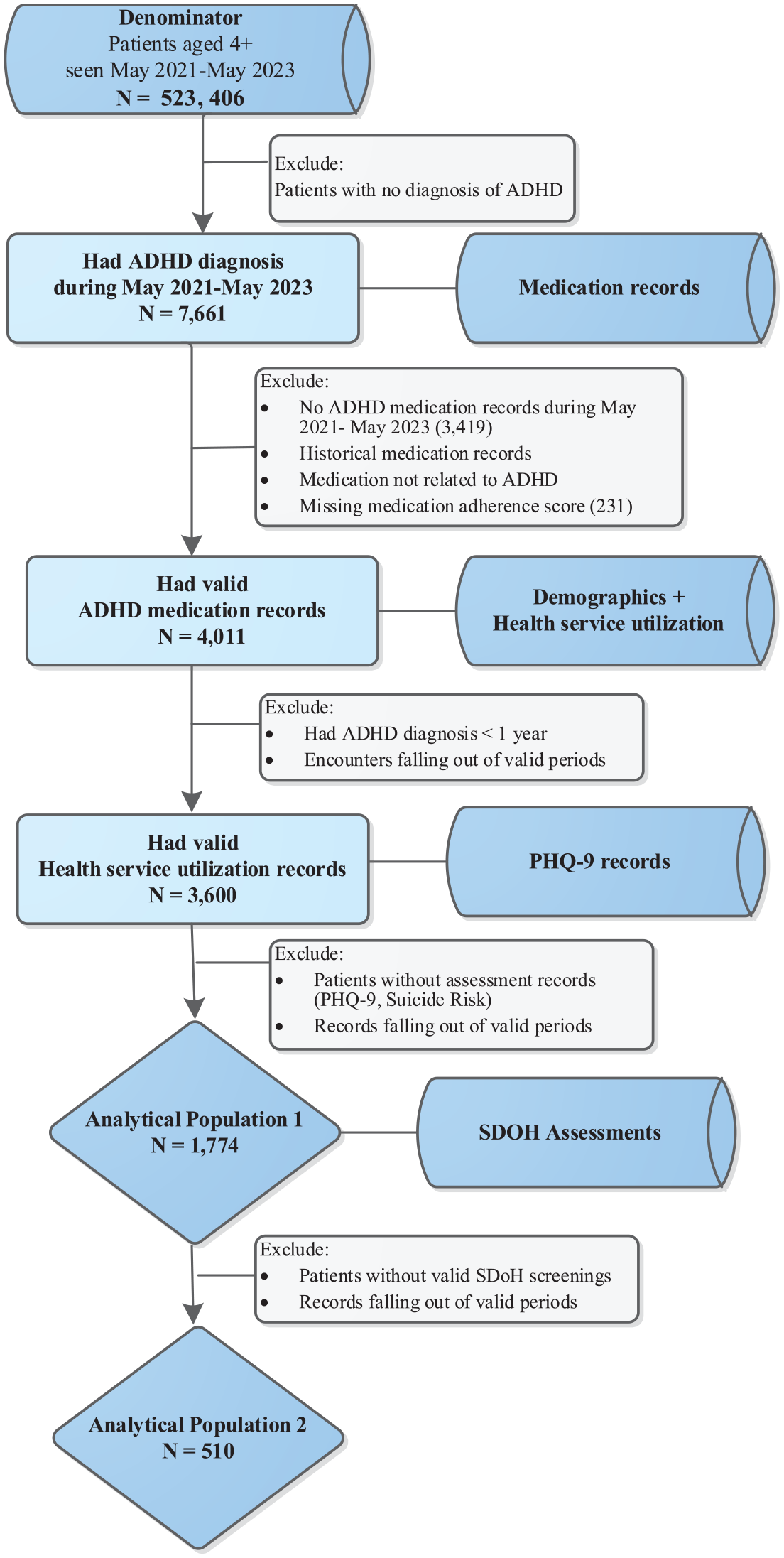
Study population flow chart.
Table 1 presents the patient’s demographic characteristics and health utilization by adherence status (adherence/non-adherence) among 3,600 patients with medication adherence information and ADHD diagnosis for at least 1 year. There was a significant difference in the distribution of age, race/ethnicity, insurance, and health utilization between patients who adhered to ADHD medication compared with those who did not. A higher proportion of adult (57.5% vs. 46.9%), non-Hispanic White (50.9% vs. 35.6%), and privately insured (63.9% vs. 54.1%) patients adhered to ADHD medication (p < .001). On average, patients who adhered to medication had significantly more BH visits per year (2.2 ± 2.8 vs. 1.9 ± 2.5 visits) and more PCP visits per year (1 ± 2.2 vs. 0.7 ± 1.6 visits; p < .001). There was no significant difference in the distribution of sex by adherence status.
Patient Demographic Characteristics, Prescriber Types, and Health Service Utilization by Medication Adherence Status (N = 3,600).
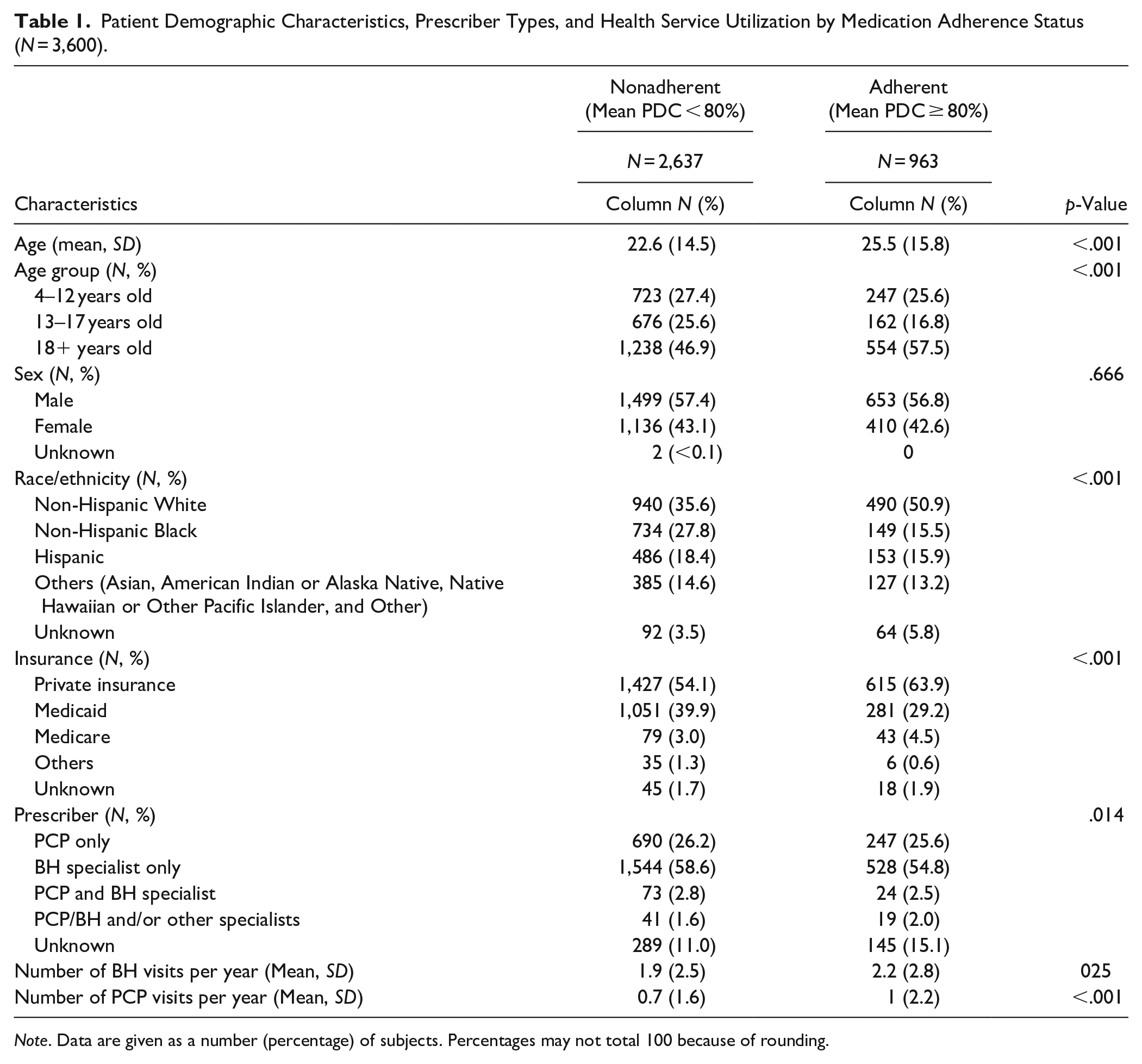
Note. Data are given as a number (percentage) of subjects. Percentages may not total 100 because of rounding.
The univariable and multivariable logistic regressions revealed associations between age, race/ethnicity, health service utilization, and the odds of adherence. Table 2 displays the relationships between demographic characteristics, clinical factors, health utilization, and the likelihood of being adherent to ADHD medication. Controlling for other factors, adult patients were almost 2.5 times as likely to adhere to medication (adjusted odds ratio [AOR]: 2.4, p < .05) than pediatric patients. Compared to non-Hispanic Whites, non-Hispanic Black patients had a 58%, and Hispanic patients had a 34% decrease in the odds of adherence (AOR: 0.42 and 0.66, p < .05, respectively). The severity of depressive symptoms was also found to be strongly associated with medication adherence. Compared with patients who had none or minimal depressive symptoms, those who reported mild or severe symptoms had a 30% and 54% decrease in the odds of being adherent, respectively (AOR: 0.70 and 0.46, p < .05). Patients who reported moderate or moderately severe symptoms had lower odds of adherence. However, it was not statistically significant. One additional BH visit and PCP visit per year increased the odds of adherence by 7% and 11%, respectively (AOR: 1.07 and 1.11, p < .05).
Factors Associated With Medication Adherence: Univariable and Multivariable Logistic Regression Analysis (N = 1,774).
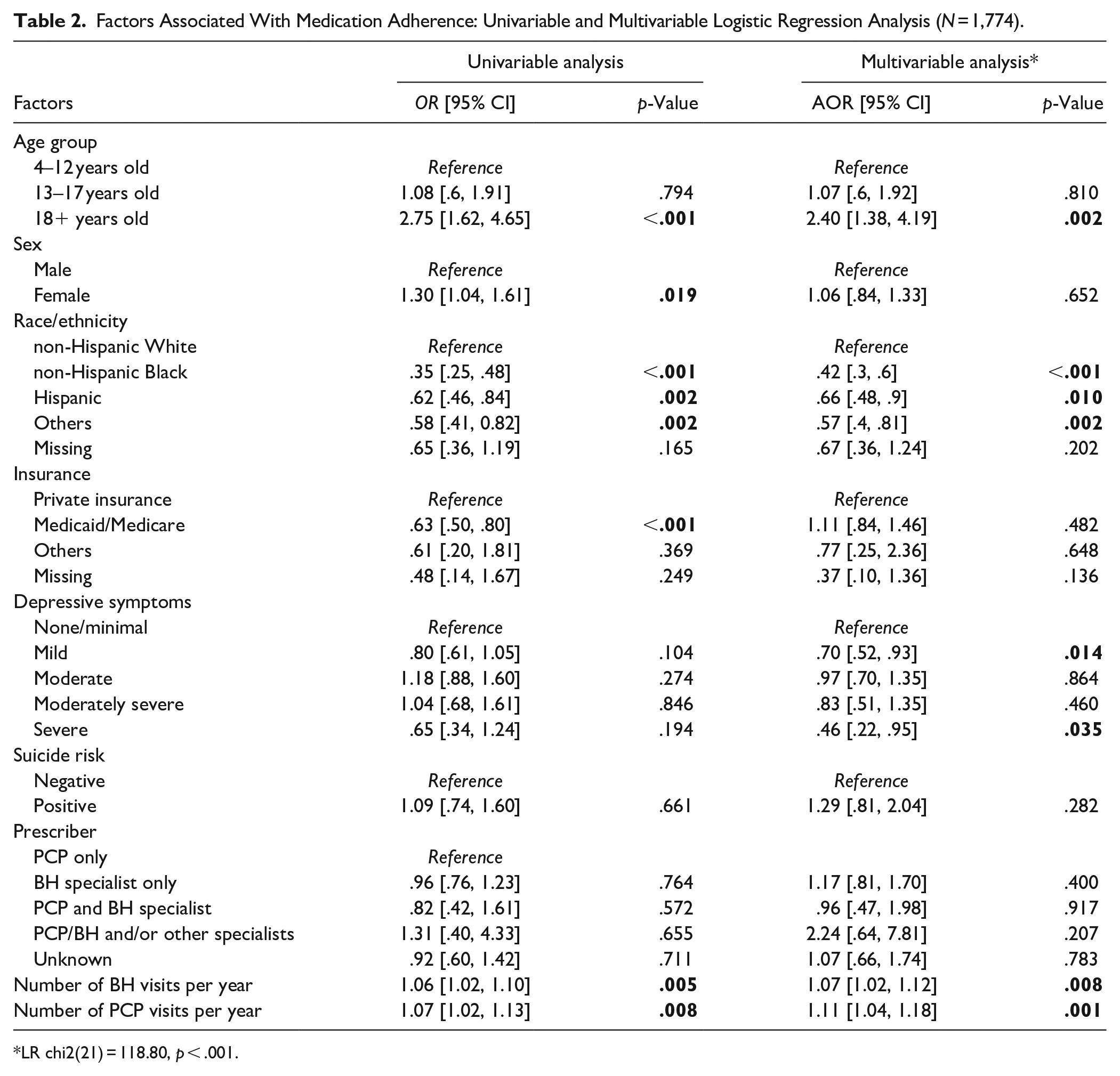
LR chi2(21) = 118.80, p < .001.
The secondary analysis (Supplemental Appendix B) assesses factors associated with medication adherence when medication adherence rate was measured continuously, and other variables were measured the same way. The characteristics that remained significantly associated with medication adherence were being adults, race/ethnicity, depressive symptoms, and health service utilization. Being White, being adults having less severe depressive symptoms, and having more BH and PCP visits per year were associated with better adherence rates.
Furthermore, when controlling for SDOH in the analysis of factors associated with medication adherence, we observed the same correlations between being adults, race/ethnicity, number of BH visits, and medication adherence as in the primary analysis (Table 3). We found that patients at risk for at least one SDOH domain had lower odds of adherence (AOR: 0.91). However, the association was not statistically significant.
Factors Associated With Medication Adherence: Multivariable Logistic Regression Analysis, Adjusting for SDOH (N = 510).
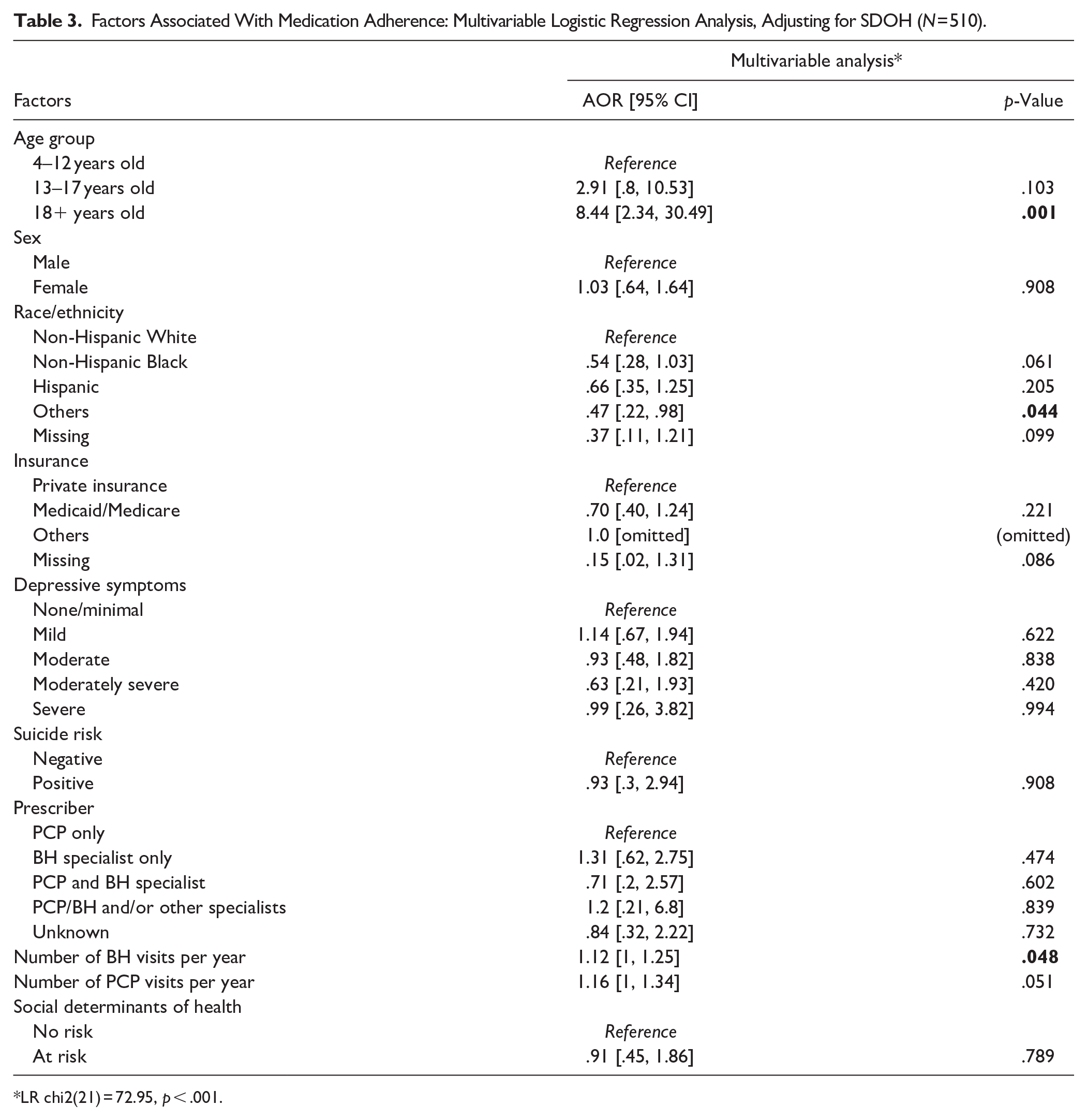
LR chi2(21) = 72.95, p < .001.
Discussion
The ADHD prevalence among our study population was 5.5% for those aged 4 to 12, 4.4% for 13 to 17, and 0.8% for 18+ years old, which is close to the expected prevalence in the general population. Our study found that only half of patients with ADHD were prescribed medication to manage their symptoms. Although patients were prescribed medication for management of their ADHD, the average adherence rate was low (55.3%). Factors positively associated with adherence were being 18 years of age or older, having more BH and PCP visits. Factors negatively associated with adherence were more severe levels of depressive symptoms and racial and ethnic minorities. Our findings are in line with previous studies exploring factors associated with ADHD medication adherence (Ahmed & Aslani, 2013; Biederman et al., 2019, 2020; Brikell et al., 2024; Charach & Fernandez, 2013; Ferrin et al., 2024; Parkin et al., 2022; Rao et al., 2021).
When comparing adherence rates by age group, patients aged 13 to 17 had the lowest adherence rate (49.4%), similar to previous studies (Biederman et al., 2019; Brikell et al., 2024). At this specific developmental stage, besides the experience of adverse effects, peers’ perception and anticipated stigma arising directly from taking medication may have a negative impact on the willingness to use medication among this youth population (Charach & Fernandez, 2013; Ferrin et al., 2024). In contrast, the odds of adherence almost doubled among our adult patients compared with patients aged 4 to 12. As individuals mature, they may develop coping skills to better manage their condition. Those with persistent ADHD in adulthood may also take on greater responsibility for their treatment and have sole autonomy in managing their medication and treatment plans. Therefore, medication use patterns may change as patients become adults. However, medication adherence in pediatric patients requires decision-making and acceptance among the patient, the parent/guardian, and the prescribing provider. Possible reasons were discussed earlier, including the child’s acceptance of medication, parents’ beliefs and attitudes toward ADHD, and treatment for ADHD that may impact their willingness to pursue long-term use. Higher child’s acceptance of medication and parent’s higher differential scores between needs and concerns were reported as the most important predictors of increased medication continuity among children (Brinkman et al., 2018; Ferrin et al., 2024). Parents’ concerns about adverse effects, medication safety and effectiveness, and social stigma associated with the medication were also reported as predictors of decreased adherence (Brinkman et al., 2018; Charach & Fernandez, 2013; Ferrin et al., 2024). Healthcare providers should improve communication by initiating a conversation with the parents and patients early enough in the treatment process to provide accurate information about ADHD, the directions regarding prescribed medications, and their expectations of the treatment, such as continuous treatment (Aremu et al., 2022; Ferrin et al., 2024; Jimmy & Jose, 2011). Providers should also address patients’ concerns in a timely manner to diminish misconceptions about the long-term consequences of medication use, enhance shared decision-making, and support medication continuity. Efforts to disseminate general knowledge about ADHD and improve mental health literacy, in general, may help alleviate barriers to medication adherence (Aremu et al., 2022).
Our study uncovered differences in medication adherence by race/ethnicity, with Whites having higher odds of adherence than other racial and ethnic groups. Despite limited research supporting differences among race/ethnicity, previous studies also indicated that children from minority groups (e.g., Hispanic, African-American) were more likely to discontinue treatment earlier and non-adhere to treatment compared to those from non-minority groups (Ji et al., 2018; Rao et al., 2021; Sleath et al., 2017). Given that individuals from minority groups are often diagnosed with ADHD later in life and individuals who are diagnosed with ADHD are less likely to take their prescribed ADHD medication consistently, developing culture-tailored interventions that focus on earlier diagnosis of ADHD and enhanced support for medication adherence among minority individuals is paramount (Ji et al., 2018; Rao et al., 2021; Sleath et al., 2017).
Depression has been identified as another risk factor for non-adherence with treatment (DiMatteo et al., 2000; Osborn & Egede, 2012). The association between co-occurring depressive symptoms and medication adherence has not been consistent in previous studies. Some found that comorbid conditions, such as depression, mediated poor ADHD medication adherence or even increased psychostimulant adherence (Atzori et al., 2009; Charach et al., 2004; Charach & Gajaria, 2008; Thiruchelvam et al., 2001). Potential explanations for this contradiction were that those with more comorbid disorders could need longer medication management, or having more comorbid conditions may increase the awareness of the importance of adherence. Our findings that patients with more severe depressive symptoms are less likely to consistently take their ADHD medications demonstrates the need for healthcare providers to identify and comprehensively manage additional behavioral health conditions that patients with ADHD may have. One key study finding is that one additional BH and PCP visit per year increased the odds of adherence by 9% and 6%, respectively, emphasizing the need to promote routine recurring visits with healthcare providers. Gardner et al. reported only 26% of patients with ADHD saw a mental health specialist, and patients had a median of one PCP visit over a period of 6 months (Gardner et al., 2004). Routine maintenance visits are necessary as providers can actively monitor side effects and coexisting conditions, provide anticipatory guidance about upcoming developmental hurdles, and strengthen the provider-patient relationship. The American Academy of Family Physicians (AAFP, 2024) recommends that all adults with a new ADHD diagnosis, uncontrolled symptoms, or any change in medication should be seen within 30 days and monthly thereafter until the symptoms and function improve and every 3 to 6 months when symptoms and function improve. The National Committee for Quality Assurance (NCQA, n.d.) established the quality metric for ADHD follow-up care for children aged 6 to 12 years old to recommend one follow-up appointment with a practitioner within 30 days of initiating treatment with ADHD medication (Initiation Phase) and at least two follow-up visits with a practitioner in the 9 months after the Initiation Phase to ensure close monitoring of children who are prescribed medication to manage ADHD symptoms. Both the AAFP and NCQA specify that the follow-up medication visits may be with a physician or a prescribing provider (NCQA, n.d.). Digital health interventions such as electronic follow-up visit reminders and telehealth services may also be effective in supporting treatment continuation (Vitija et al., 2022).
We did not find statistically significant associations between adherence and sex, suicide risk, and SDOH. In assessing for sex differences, findings from previous studies were somewhat mixed depending on the targeting population, age groups, and study settings (Biederman et al., 2019; Rao et al., 2021). For example, clinical trials found males to have worse adherence (Rao et al., 2021), but some studies have shown females to have worse adherence among children and youths (Biederman et al., 2019), while others found no influence of sex on adherence (Bhang et al., 2017; Safavi et al., 2019). Regarding SDOH, it is possible that some SDOH needs, such as transportation or financial resources, were addressed after our patients were screened positive, which may have helped improve their treatment continuation and medication adherence. Regarding suicide risk, the PHQ-9 suicide item that we used may have overidentified the risk of suicide and may not be as accurate a measure as the Columbia-suicide severity rating scale (C-SSRS; Chung et al., 2023). Therefore, we did not detect an association between suicide risk and medication adherence.
We also found no differences in medication adherence by type of prescriber, suggesting that ADHD may be effectively managed by primary care providers or behavioral health providers. Health systems experiencing a shortage of BH providers, access to care issues, and long waiting times may want to consider triaging patients with lower severity to be managed by their PCPs.
Our study has several strengths. First, as most ADHD patients are treated on an outpatient basis, our study population, which includes patients receiving primary care or behavioral health services, reflects “real world,” typical treatment settings. Second, our study included patients ages 4 years and older which allowed us to investigate differences in the prevalence and treatment pattern across pediatric, adolescent, and adult populations. Third, we evaluated various factors associated with medication adherence, including demographic characteristics, depressive symptoms, and healthcare utilization. Although some associated factors are not modifiable, depressive symptoms and healthcare utilization are modifiable factors that healthcare providers and healthcare systems can intervene upon. By exploring a large number of variables associated with medication adherence, our study identifies adherence influencers and pinpoints factors amenable to intervention for optimizing adherence.
Our study, nevertheless, has several limitations. First, due to the retrospective nature of this study and how ADHD was identified solely by ICD-10 codes, we could not control for baseline symptom severity, which may impact medication adherence or prescriber’s decisions to use medications (Charach & Fernandez, 2013). Additional data from structured interviews or standardized ADHD screening tools may assist with the diagnostic characterization of the patients (Kemper et al., 2018; Vallejo-Valdivielso et al., 2024). Second, due to limited data, we could not assess medication characteristics that may affect adherence, such as medication formulations and dose regimens (Charach & Fernandez, 2013). Third, although PDC has been one of the most frequently used measures for medication adherence based on pharmacy claims and provides insight into whether the medication was available for the person, PDC has some limitations and cannot confirm that the medication was taken as prescribed (Prieto-Merino et al., 2021). Other patient questionnaires, such as the Medication Adherence Questionnaire, the 8-item Morisky Medication Adherence Scale (MMAS), and the Brief Medication Questionnaire, can be useful measures for medication adherence. These measures assess important information regarding medication-taking behaviors, barriers to adherence, and beliefs associated with adherence and allow ranking the degree of adherence instead of using a cut-off. Fourth, information was limited to encounters with UTP providers, and patients may have had services at other locations that were not captured in the data. Finally, we were not able to assess primary language due to missing data, which could be a potential explanatory factor for medication adherence. However, our assessment of health literacy may have partially captured the language barrier.
In summary, our study identifies factors associated with ADHD medication adherence across the lifespan. Our findings support the strong association between age, race/ethnicity, depressive symptoms, health utilization and ADHD medication adherence. Several modifiable factors, when addressed, can potentially improve adherence and, thus, outcomes in ADHD. Interventions that may increase adherence should be considered when healthcare providers prescribe ADHD medication. They may include educating parents/patients on the expected time frame for improvement, consideration of the patient’s age, increased attention to patients with ADHD who are entering adolescence where adherence tends to be reduced, the presence of comorbidity and the level of education about the disorder in the family and including family support in medication management. Moreover, as other studies reported the negative impact of SDOH risk on medication adherence (Baweja et al., 2021; Wilder et al., 2021), we believe that implementing comprehensive support programs that address social determinants of health, such as SDOH screening and referrals to community resources, could reduce barriers to treatment and, in turn, improve medication adherence.
Conclusions
Our study suggests that the overall rate of treatment was low, and medication non-adherence was prevalent in ADHD treatment, especially among adolescents. The patient’s age, race/ethnicity, socioeconomic status, and healthcare utilization were associated with medication adherence. Healthcare providers may need to embrace a nuanced approach to optimizing ADHD treatment when prescribing ADHD medication. Efforts are needed to improve medication adherence, such as follow-up reminders, enhanced and culturally tailored provider-patient communication, patient and parent education, increased access to mental health services, and close monitoring of coexisting depressive symptoms. Additionally, comprehensive support programs that address BH utilization and social determinants of health can foster improved medication adherence, especially since ADHD medication is the most effective way to manage ADHD symptoms.
Supplemental Material
sj-docx-1-jad-10.1177_10870547251336852 – Supplemental material for Factors Associated With Medication Adherence Among Patients With Attention-Deficit/Hyperactivity Disorder (ADHD)
Supplemental material, sj-docx-1-jad-10.1177_10870547251336852 for Factors Associated With Medication Adherence Among Patients With Attention-Deficit/Hyperactivity Disorder (ADHD) by Linh Nguyen, Yen-Chi L. Le, Hannah Reygaerts, Todd R. Johnson and Cesar A. Soutullo in Journal of Attention Disorders
Footnotes
Acknowledgements
The authors would like to thank Heath Goodrum for his technological assistance with the data pull and Ingrid Castillo for overseeing the behavioral health initiatives at UT Physicians.
Consent to Participate
The requirement for informed consent to participate has been waived by the Committee for the Protection of Human Subjects at the University of Texas Health Science Center at Houston (HSC-MS-23-1141).
Consent for Publication
Not Applicable.
Data Availability
Not Applicable.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Cesar A. Soutullo, MD, PhD declares the following conflicts of interest: During the years of 2020 to 2024, Dr. Soutullo has received departmental research funds from the Texas Child Mental Health Care Consortium (Youth Depression & Suicide Network) SB11, Innosphere (Germany), John S. Dunn Foundation, Vivian L. Smith Foundation, and The Favrot Fund. Additionally, Dr. Soutullo has served as a consultant or on the advisory board for NeuroTech Solutions Ltd (Israel), Limbix/Big Health, and Medice (Germany). Dr. Soutullo has also participated in the Speaker’s Bureau or given non-product-related Continuous Medical Education talks for Bial (Portugal), Medice (Germany), Cuquerella Medical Consulting (Spain), and Tecnofarma (Perú). Lastly, Dr. Soutullo has received royalties from Editorial Médica Panamericana (Spain).
The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was approved by the Committee for the Protection of Human Subjects at the University of Texas Health Science Center at Houston (HSC-MS-23-1141).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.