
Abstract
Introduction:
Several studies have shown increased occurrence of migraine in ADHD patients. However, there is less evidence on whether migraine patients also have a higher ADHD frequency. The aim of this paper is determining whether the prevalence of ADHD symptoms or impulsivity is higher in patients with episodic migraine.
Methods:
An observational cohort study has been conducted. Patients with episodic migraine were included. The ADHD Rating scale, the Adult ADHD Self-Report Scale, and the scale of impulsiveness of Plutchik were used.
Results:
The mean value of inattention, hyperactivity and impulsivity scores on the ADHD scale was 5 ± 3.8 in cases and 2.7 ± 2.2 in controls (p < .00001), 4 ± 3.2 in cases and 2.5 ± 2.4 in controls (p = .000621) and 2 ± 1.5 in cases and 1.1 ± 1 in controls (p = .000407), respectively.
Conclusion:
Adults with migraine have a higher prevalence of ADHD symptoms. This should be considered when assessing these patients.
Introduction
Attention-deficit-hyperactivity disorder (ADHD) is a neuropsychiatric syndrome characterized by inappropriate levels of hyperactivity, impulsivity in motor, emotional and social responses, a general lack of inhibition, and pervasive inattention (Matthews et al., 2014). Symptoms usually emerge in childhood, with a current prevalence rate of 5% in 4 to 17-year-olds (Matthews et al., 2014), but ADHD is a lifelong condition often underdiagnosed in adults unless it has been diagnosed early in childhood. Several retrospective studies have shown a prevalence in adults of around 4% (Magnin & Maurs, 2017). In ADHD adults symptoms are still present with attentional predominance, but also observations of hyperactive or impulsive behavior (Ivanchak et al., 2012). Migraine is a common and potentially debilitating chronic neurologic disorder presenting significant and clinically important psychiatric comorbidities. Patients with episodic and chronic migraine usually report impulsive behavior and lack of attention and concentration during attacks and interictal phases (Bergman-Bock, 2018; Muñoz et al., 2016). Moreover, the prevalence of migraine could be higher in ADHD patients. The relation between migraine and ADHD has been extensively studied and research suggests that ADHD patients have a higher migraine frequency (Arruda et al., 2020; Hansen et al., 2018; Kutuk et al., 2018; Salem et al., 2018). Most studies have been carried out in children and adolescents and have studied migraine in ADHD patients. Hansen et al. assessed the prevalence of migraine and ADHD in participants from the Danish Blood Donor Study and found that migraine was strongly associated with ADHD (OR = 1.8, 95% CI [1.5, 2.1]), (238/6152 vs. 690/19,376) (Hansen et al., 2018). Fasmer et al. (2011) assessed migraine in patients using self-administered questionnaires in 572 ADHD adults and found that the prevalence of migraine was 28.3% in ADHD subjects compared to 19.2% in controls (p < .001), reporting an odds ratio of 1.67 (95% CI [1.28, 2.17]) for migraine in ADHD subjects as compared to the general population. However, there are fewer studies in adults and fewer studies assessing whether migraine patients have a higher prevalence of ADHD. Although the pathophysiology of both migraine and ADHD is not fully understood yet, there are several cortical and subcortical structures that participate in events underlying both disorders so that common mechanisms could explain a relation between both disorders.
Thus, understanding the relation between migraine and ADHD may be relevant in several respects. First, it might emphasize the need to consider ADHD symptoms in the treatment of migraine. Besides, it might advance an in-depth understanding of a possible common mechanism underlying both disorders.
As mentioned before, most studies to date have been conducted in children or adolescents and have been based on ADHD patients who have been assessed for migraine headache. Therefore, our work provides a different approach since it has been conducted in adults suffering migraine, whose ADHD symptoms may be unnoticed, and it analyses the prevalence of traits compatible with ADHD.
The main objective of this paper is determining whether the prevalence of ADHD symptoms or impulsivity is higher in patients with episodic migraine.
Methods
An observational cohort study has been conducted. The sample size was calculated using an estimation formula of the difference of two proportions to compare the frequency of occurrence of ADHD-related symptoms in migraine patients compared to healthy controls. Thus, for a level of confidence (95%), with a statistical power of 80%, estimating an a prioristic proportion of 5% of ADHD in the control group and 15% in migraine patients, a minimum required sample size of 100 cases was estimated, with a ratio of 1.5 controls per one case.
The subjects were selected from all consecutive patients treated in a headache clinic. The researcher explained to each participating subject the study, purpose, procedure, estimated duration, potential risks and benefits of participating in the study, as well as any inconvenience it could imply. Each participant was told participation was voluntary and that they could reject or abandon the study at any time, without affecting their subsequent medical treatment or their relationship with the treating physician. All subjects were given sufficient time to read and understand the patient information sheet before signing the consent form and received a copy of the document signed. The diagnosis of migraine was made by a neurologist specializing in headaches following the International Headache Society criteria. All patients that met criteria for episodic migraine and were older than 18 years old and had at least one attack/month, were included if the informed consent form was signed. Patients were excluded if they met criteria for chronic migraine or were taking preventive treatment for migraine or drugs that could influence attention and concentration.
To assess attention deficit, hyperactivity, and impulsivity, both the ADHD Rating scale (ADHD-RS) and the Adult ADHD Self-Report Scale (ASRS) were used. A final clinical diagnosis was not made, yet the frequency of symptoms suggestive of ADHD in both groups was analyzed. The ASRS is the World Health Organization’s (WHO) rating scale for adult ADHD to measure current ADHD symptoms. It consists of 18 items based on DSM IV symptoms/criteria for ADHD, which are measured on a 5-point scale (0 Never/Seldom and 4 Very often), yielding a possible score range from 0 to 72. Items 1 to 9 (Part-A) cover the symptoms of inattention; items 10 to 18 (Part-B) the symptoms of hyperactivity and impulsivity. This scale is useful for ADHD adult screening and diagnosis and should be used in conjunction with a clinical interview to provide additional information. ASRS has a high internal consistency (Cronbach’s alpha of .92). If the respondent scores often or very often in four or more items in Part-A, the individual symptom profile is considered highly consistent with ADHD diagnosis in adults.
However, the ADHD-RS is an 18-item scale reflecting the DSM-V criteria for ADHD. It consists of an inattention subscale with nine items and a hyperactivity/impulsivity subscale with other nine items. The beginning of sentences with “often” is omitted, and respondents are asked about the occurrence frequency of these symptoms in the last 6 months. Each item is scored from 0 to 3 points depending on the frequency (never, sometimes, frequently, constantly), and higher scores indicate the problem behavior. The final score of the ADHD-RS consists of the sum of the direct scores, independent of the rater. It was initially designed to be administered to child patients, but it has been adapted for adult subjects. The ADHD-RS has a high internal consistency (Cronbach’s alpha value of .8) and has been validated in Spanish, showing that it is a valid scale to differentiate ADHD adults from non-ADHD subjects (Richarte et al., 2017). For this work, if ≥6 items were met as frequent or constant on the inattention subscale, a diagnosis of ADHD inattentive subscale was considered; if ≥6 items were met as frequent or constant on the hyperactivity/impulsivity subscale a diagnosis of ADHD hyperactive subscale was considered; and if ≥6 items were met as frequent or constant on both subscales, a diagnosis of ADHD mixed subscale was considered.
Impulsiveness was measured using the scale of impulsiveness of Plutchik (PIS). It consists of a questionnaire of 15 Likert items with four possible answers (never, sometimes, often, almost always), scored respectively 0 to 3, with the exception of questions 4, 6, 11, and 15 that are scored in contrast. The final value is obtained by adding the score for each item, so it will be between 0 and 45. In the Spanish version, the authors propose a cut-off point of 20, with a sensitivity of 60% and a specificity of 74%. The internal consistency of the scale according to Cronbach’s alpha reliability coefficient was .9.
In all cases, demographic- and migraine-related variables were collected. The categorical variables were summarized in frequencies and percentages, while the numerical ones in averages and standard deviations (SD) or in medians and interquartile ranges (IQR), depending on whether the normality assumptions were given. The percentages were compared with the chi-square test; means, to the t-test, and medians with the Wilcoxon test and Mann-Whitney U test for independent data. Data analysis was performed using Microsoft Excel 2013 and the SPSS version 19 statistical package.
Results
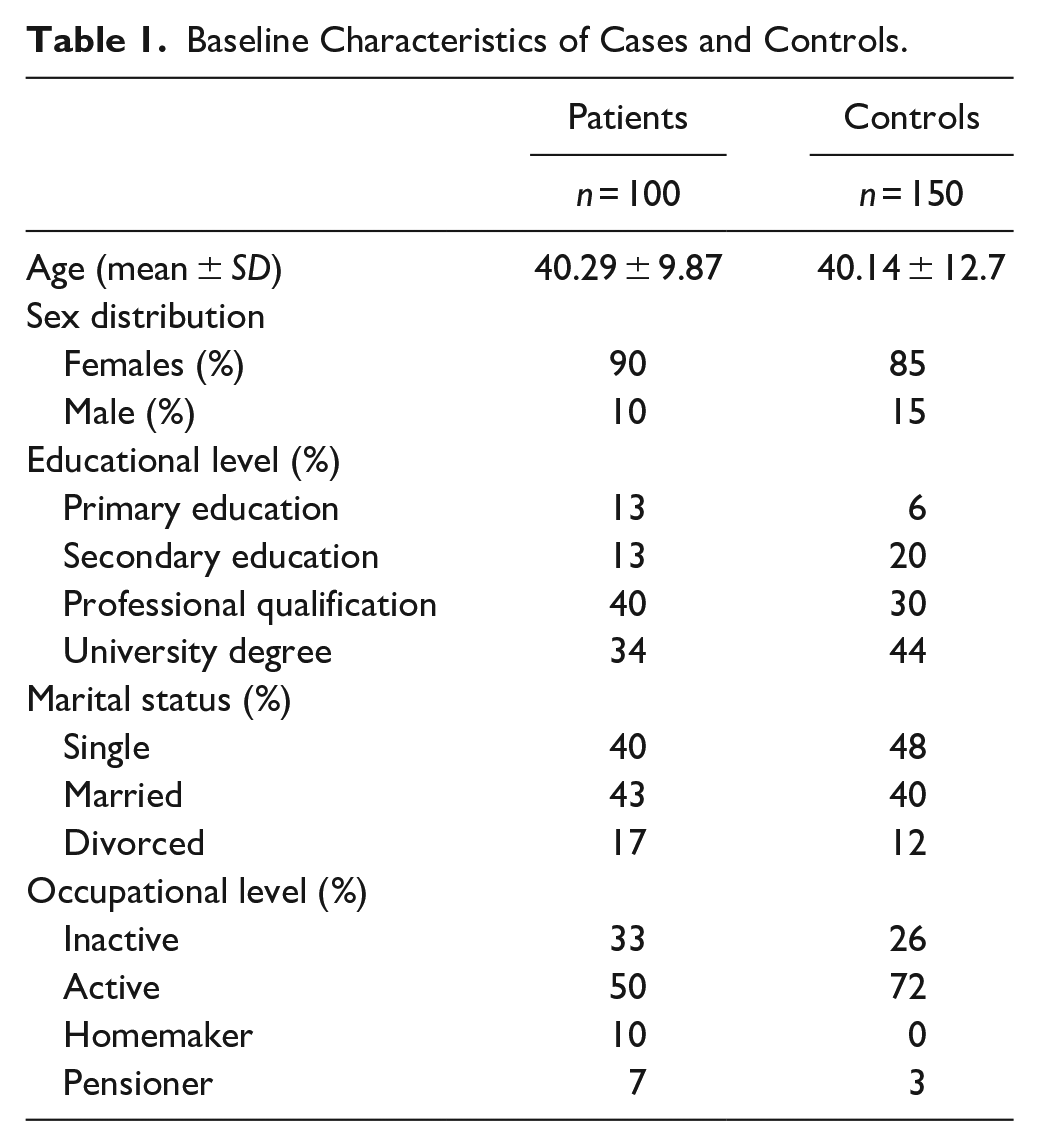
Two hundred fifty patients were included: 100 cases (90% female) and 150 controls (85% female). Median age was 40.29 ±9.87 years among cases and 40.14 ±12.17 years among controls. The social and demographic characteristics of cases and controls are listed in Table 1.
Baseline Characteristics of Cases and Controls.
Seventy cases suffered from migraine without aura, while 30 presented a migraine with aura. Ten cases (10%) had less than one attack per month, 64 (64%) had between two and four attacks per month, and 26 (26%) had more than four attacks per month.
The mean value of inattention, hyperactivity and impulsivity scores on the ADHD scale was 5 ± 3.8 in cases and 2.7 ± 2.2 in controls (p < .00001), 4 ± 3.2 in cases and 2.5 ± 2.4 in controls (p = .000621) and 2 ± 1.5 in cases and 1.1 ± 1 in controls (p = .000407), respectively. A 3.6% of migraine patients and a 0.6% in the control group scored often/very often in ≥6 items on the inattention scale (p = .28). A 5% of migraine patients scored often/very often in ≥6 items on the hyperactivity + impulsiveness subscale, compared to a 0.6% in the control group (p = .02). On the impulsiveness item, a 35.5% of migraine patients scored often/very often in ≥1 item, compared to 8.6% in the control group (p < .05); see Figure 1.
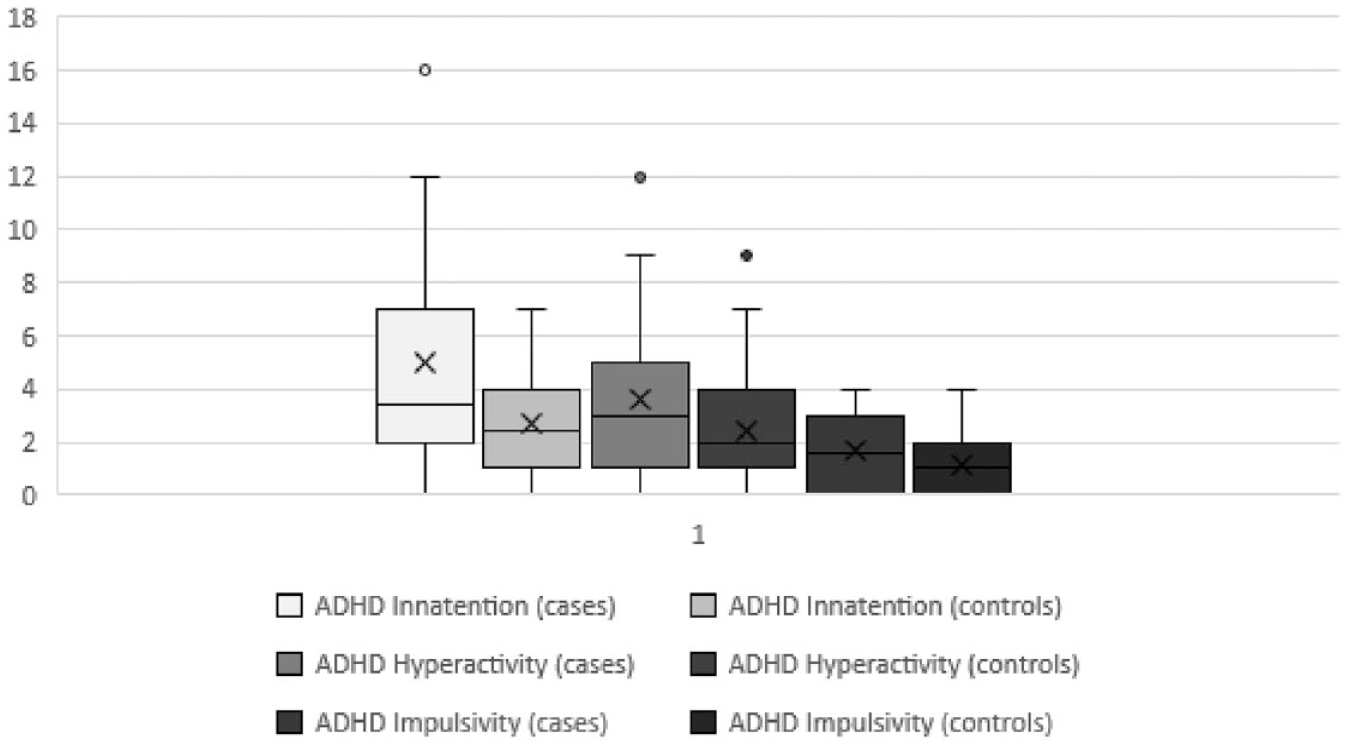
Scores on the ADHD-RS-IV scale in cases and controls.
The mean ARSR scale score was 15 ± 10.8 in cases and 12.3 ± 7.5 in controls (p = .024448). A 13.3% of migraine patients scored often or very often in four or more items in Part-A of the ASRS, compared to 2.8% of controls (p = .1).
No differences were obtained between migraine patients without aura and with aura in ADHD scores for inattention (5.3 ± 3.9 vs. 4.4 ± 3.7, respectively, p = .126226), hyperactivity (3.4 ± 3.2 vs. 3.9 ± 3, p = .207444) and impulsivity (1.7 ± 1.5 vs. 1.5 ± 1.4, p = .325564). There was also no difference between these two groups in the total score of the ASRS questionnaire (14.1 ± 10.6 in patients without aura vs. 15.8 ± 11.2 in patients with aura, p = .233089). No correlation was found between days per month with headache and ADHD scores for inattention, hyperactivity, and impulsivity, nor with ASRS total scores.
The median on the PIS scale was 15 ± 6.5 in the cases and 12 ± 5 in the controls (p < .05); see Figure 2. No differences in PIS scores were obtained between patients without and with aura (15.5 + 5.2 vs. 16.1 + 7.1, respectively, p = .32396).
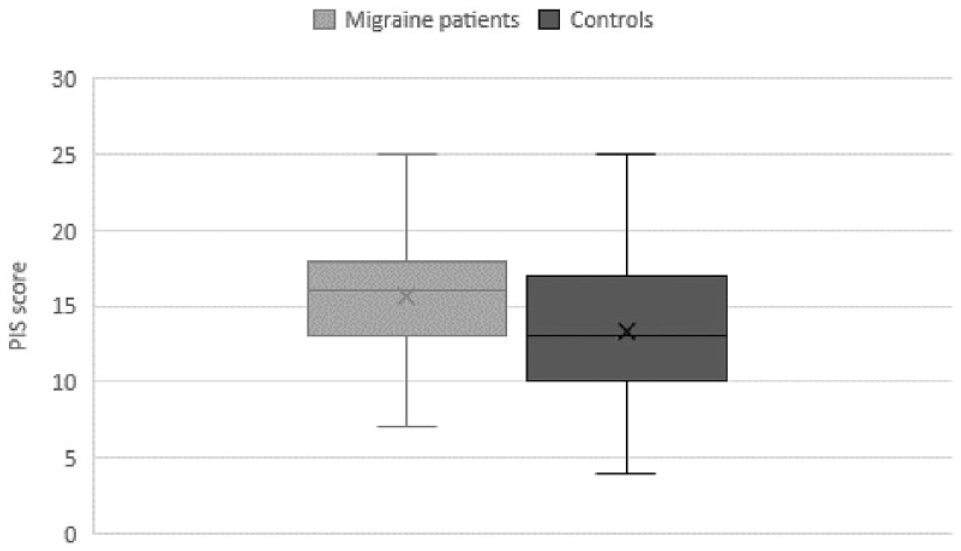
PIS score in cases and controls.
Discussion
In our study, we found higher scores on the inattention, hyperactivity, and impulsivity items of the ADHD scale, as well as a higher total score on the ASRS scale in migraine patients than in healthy controls. Despite we have not been able to demonstrate a statistically significant relationship between migraine and ADHD in adults, there seems to be a tendency toward some association as the analysis of the ASRS results suggest. The frequency of patients who scored four or more items as often or very often in Part-A of the test was five times higher in patients with migraine than in controls, although not statistically significant (p = .1). Considering the ADHD-RS results it could be suggested that this increase is fundamentally related to the hyperactive subtype, since the number of patients who scored ≥6 items as frequent/constant in the hyperactivity + impulsivity subscale was five times higher in migraine patients than in controls; in this case, the results obtained statistical significance. Furthermore, both the impulsivity subscale of the ADHD-RS and the PIS showed greater tendency toward impulsivity in migraine patients.
A previous study by Fasmer et al. (2011) already referred an association between ADHD and migraine. The authors used a methodology different from ours since patients with ADHD diagnosis (n = 572) were given a self-questionnaire to answer about several comorbidities and were compared with healthy controls (n = 675) filling in the same questionnaire. Fasmer et al. found out that the prevalence of migraine was significantly higher in the patient group compared to the controls (28.3% vs. 19.2%, p < .001, OR = 1.67, 95% CI [1.28, 2.17]). The difference from controls was particularly marked for men (22.5% vs. 10.7%, p < .001, OR = 2.43, 95% CI [1.51, 3.90]) but was also significant for women (34.4% vs. 24.9%, p = .008, OR = 1.58, 95% CI [1.13, 2.21]) (Fasmer et al., 2011). This same research group published a paper analyzing data from the Norwegian prescription database for 2006, including the total Norwegian population (N = 4,640,219), and reviewed the prescribing of anti-migraine drugs and ADHD treatments (Fasmer et al., 2012). In this study, a positive and significant association between prescription of anti-migraine and ADHD medication was found for all age groups between 20 and 50 years and for both genders, with odds ratios ranging from 1.8 to 2.8 (Fasmer et al., 2012). More recently, Hansen et al. (2018) studied 26,456 participants from the Danish Blood Donor Study. The presence of migraine was evaluated with two questions of the population screening questionnaire for migraine (SQM), and current self-reported ADHD symptoms were assessed implementing the current national recommendation for clinical assessment of adults by using the ASRS. In this study, 24.2% screened positive for migraine, 2.61% screened positive for ADHD, and 0.90% reported having both migraine and ADHD. Hansen et al. (2018) found an association between migraine and ADHD symptoms with OR = 1.81 (95% CI [1.53, 2.12], p = 1.4e−14). Carpenet et al. evaluated the association of self-perceived levels of attention deficit and hyperactivity symptoms with non-migraine and migraine headaches among 4,816 university students. Self-perceived attention deficit levels and self-perceived hyperactivity symptom levels were evaluated based on the ASRS (Carpenet et al., 2019). Compared with participants without headache, they found significant associations between global ADHD scores and migraine. Students in the highest quintile of global ASRS scores had an adjusted odds ratio (aOR) of 1.95 (95% CI [1.56, 2.45]) compared to the lowest (Carpenet et al., 2019). Recently, Hsu et al. (2022) evaluated the risk of migraine in children, adolescents, and young adults with ADHD and its association with ADHD medications. This longitudinal case-cohort study was conducted using data from the Taiwan National Health Insurance Database between 2001 and 2009. They enrolled 81,441 ADHD participants and a 1:1-matched control cohort for age, sex, and physical and psychiatric comorbidities. Patients with ADHD had a higher incidence of migraine than those in the control group (0.6% vs. 0.3%, p < .001). After adjusting for potential confounders, the hazard ratio (HR) was 1.92 (95% CI [1.64, 2.34]) for migraine in patients with ADHD versus controls. The subgroup analyses stratified by age showed that the HRs were 2.01 (95% CI [1.63, 2.49]), 1.94 (95% CI [1.35, 2.79]), and 1.31 (95% CI [0.58, 2.98]) for children (<12 years old), adolescents (12–17), and young adults (18–29), respectively, compared to controls (Hsu et al., 2022). Salem et al. (2018) evaluated the potential association between ADHD and headache in a meta-analysis that included 14 studies conducted mainly in children and found a positive association between ADHD and migraine (OR 1.322, 95% CI [1.018, 1717], p = .036). In our study, the group consisted of patients with diagnosed migraine, and not of patients with ADHD diagnosed or the general population who were given a headache or migraine questionnaire. We believe that our approach may influence the lower association we observed, as the questionnaires may overestimate the prevalence of migraine in patients with other types of headaches.
In our work there was no difference in ADHD and ASRS scores between patients without and with aura, not a correlation with the number of days with headache. Although these results may be influenced by the smaller sample size than in other published studies, it is possible that the association between ADHD symptoms and migraine is due to pathophysiological links between the two conditions, and not to the subtype of migraine or the number of days with pain.
Studies on impulsivity in migraine patients are limited. A study by Muñoz et al. (2016) involving 155 patients with chronic migraine or headache with analgesia abuse found no associations between Plutchik scale scores or the presence of impulsivity with either CM or MO. Tanik et al. (2020) enrolled 55 patients aged between 18 and 55, all diagnosed with episodic migraine, and 40 healthy controls in a prospective cross-sectional study and found no significant difference in terms of impulsivity (p = .711) using the Barratt impulsiveness scale-11. Santos et al. investigated impulsive behavior in migraine patients and with medication-overuse for migraine. They performed a cross-sectional study on 210 patients, using the Barratt impulsiveness scale-11. The group of migraine patients accounted for the highest impulsivity level, followed by the control group and, finally, by the medication-overuse group. However, these differences did not attain statistical significance (Santos et al., 2020).
Migraine has been associated with different psychiatric comorbidities, such as anxiety and depression. The pathophysiology of migraine is complex and not fully understood, although different structures and neurotransmitters involved in the genesis of migraine, such as serotonin and glutamate, have been described (Dodick, 2018). In migraine, a phase of neuronal hyperexcitability has been identified, as well as the hypersensitivity of patients to different stimuli. Additionally, a genetic susceptibility to migraine has been observed (Dodick, 2018). The etiology and pathophysiology of ADHD are incompletely understood. There is evidence of a genetic basis for ADHD, but it is likely to involve many genes with small individual effects. Differences in the dimensions of the frontal lobes, caudate nucleus, and cerebellar vermis have been demonstrated (Tripp & Wickens, 2009). Dysfunction in dopaminergic pathways may contribute to the clinical manifestations of ADHD (Sharma & Couture, 2014). There is evidence that low levels of serotonin neurotransmission are associated with increased impulsivity (Keele, 2005). Impulsive patients also show dysfunction in the pathways that mediate the generation and regulation of emotions (corticolimbic and corticostriatal) (Hazlett et al., 2005). Therefore, these disorders may share pathophysiological mechanisms that explain their association.
The limitations of our work include the cohort design, which does not allow for follow-up, as well as the diagnosis of ADHD based on self-administered questionnaires. Also, the sample size did not allow us to obtain deterministic results that could have been improved with a larger sample. However, we consider the inclusion of a group of cases with a well-defined diagnosis of migraine to be a strength, as well as the inclusion of a control group.
Therefore, in this work, we have shown that there is a tendency in migraine patients to a higher prevalence of ADHD symptoms, as well as a tendency to a higher impulsive personality trait. Although these results cannot be considered definitive, they can help delimit the psychiatric and personality comorbidities of patients with migraine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.