
Abstract
Purpose:
Avoidant automatic thoughts (AAT) are thoughts that precede or accompany a delay in the starting or ending of a task. In a prior study of college students using Ecological Momentary Assessment (EMA), AATs were frequent daily occurrences and participants with more severe ADHD symptoms at baseline reported more frequent AAT. Importantly, momentary presence of AAT was associated with greater task avoidance and inattentive symptoms. In the current study, we replicated and extended this study in a community sample of adults.
Method:
We measured AAT in the daily lives of 106 adults using EMA. Data were collected at baseline and up to five times per day for 6 days.
Results:
Using multilevel modeling, we found that baseline ADHD symptoms predicted more frequent AAT and more severe task avoidance and negative emotion in daily life. Recent presence of AAT was associated with inattention, task avoidance, and slightly elevated negative emotion in the moment. More severe baseline ADHD strengthened the relationship between AAT and both inattention and task avoidance. In exploratory analyses, we found that work tasks and household chores were the most avoided activities and that, instead, people were most likely to be doing other work tasks or engaging in screen time or self-care, respectively.
Conclusions:
This study replicates and extends our prior findings regarding AAT in daily life and their relationship to ADHD and supports continued research on this construct, which may have clinical utility for intervening in problematic avoidance behaviors.
Keywords
The study of maladaptive thoughts from a cognitive-behavioral perspective has focused almost entirely on the problematic impact of thoughts that are negative in content and emotional valence (Beck, 2011; Ehring & Watkins, 2008; Glass & Arnkoff, 1997; Wahl et al., 2019). If positive thoughts are measured in research studies, they are often assumed to be adaptive “opposites” of maladaptive negative automatic thoughts (NAT; Ingram et al., 1995). This juxtaposition is fitting for the thoughts most relevant to emotional disorders—the anxiety disorders and major depressive disorder—which are characterized by maladaptive, uncontrollable negative emotions and lower levels of positive emotion. However, the historical origins of the negative-bad, positive-good dichotomy may have restricted the field’s view of what a maladaptive thought can “look like” and, therefore, which automatic thoughts might be clinically relevant in certain contexts.
In a recent study (Knouse et al., 2023), we introduced the concept of Avoidant Automatic Thoughts to describe thoughts that may precede avoidant behavior—specifically, delaying the starting or ending of a task or activity (e.g., “I don’t have to get started on that yet.”). Importantly, AAT may often be non-negative or even overly optimistic in content (e.g., “I work best under pressure.”). In reviewing the literature on automatic thoughts, we proposed the following definition: Automatic thoughts are thoughts that, (1) arise spontaneously (without deliberation), (2) are about a current experience (external or internal), and, (3) tend to be believed by the thinker, especially in the absence of reflection. Thus, we define avoidant automatic thoughts as spontaneously arising thoughts about delaying the starting or ending of an activity that tend to be believed by the person thinking them.
The origins of the AAT concept are rooted in the application of cognitive-behavioral therapy to ADHD in adults. Most CBT approaches for adult ADHD do include skills that target the deleterious impact of negative automatic thoughts, as adults with ADHD report elevated levels of negative automatic thoughts and dysfunctional beliefs (Mitchell et al., 2013; Ramsay, 2020; Torrente et al., 2014) that may contribute to the development of depression (Knouse et al., 2013). But clinical observation and subsequent research have revealed that some clients with ADHD struggle with the effects of overly optimistic thoughts that precede a failure to engage with an important task or self-regulation strategy (see Knouse & Mitchell, 2015 for a review). For example, a client might think, “I can do this for just a few minutes longer,” and leave too late for an appointment, or a client might think, “I have plenty of time to do that tomorrow,” and engage in a preferred task instead of a task with an impending deadline. Our prior study (Knouse et al., 2023), described in further detail below, demonstrated that, while ADHD symptoms are associated with higher rates of AAT in daily life, AAT and associated task avoidance were by no means confined to people with high levels of ADHD symptoms. This result supported our notion that AAT, like NAT, are a useful concept for understanding both typical and atypical cognitive-behavioral processes and that they are a potentially useful tool for understanding avoidance processes across diagnostic categories.
Prior Findings and Goals of the Current Study
In our prior work, we defined, described, and measured Avoidant Automatic Thoughts in the daily lives of undergraduate students (n = 101) using Ecological Momentary Assessment (EMA). EMA and other thought-sampling methods have been used previously and productively to study clinically relevant thoughts and their correlates (Hurlburt, 1997; Wenze & Miller, 2010; Wenze et al., 2018). We found that AAT were frequently reported by these students at 53.48% of the moments sampled. Recent presence of AAT was associated with increased task avoidance and inattention, but not with negative emotion. ADHD symptoms predicted higher rates of AAT and task avoidance, but ADHD symptoms did not moderate (strengthen) the relationship between AAT and avoidance. Limitations of this study, however, included the undergraduate-only sample, the fact that data collection took place while the COVID-19 pandemic was very much affecting daily life (Spring 2021), and the first-time use of the AAT items to measure this construct using EMA.
In the current study, we sought to replicate our prior work in a community sample with a broader age range than the prior study (n = 106; age = 18–75 years) and at a time further removed from the acute effects of COVID-19 (Summer of 2022). In addition, we increased our EMA sampling frequency from three times per day to five times per day. Finally, we sought to gather more information about the context of AATs and task avoidance in daily life—specifically, when participants indicated that they were engaging in task avoidance, we asked them what they were avoiding and what behaviors they were engaging in instead of those avoided tasks.
Hypotheses (Pre-registered)
ADHD Symptoms and Momentary Experiences
Self-reported ADHD symptoms will be positively related to momentary experiences of AAT, task avoidance, and inattention. ADHD symptoms will also be positively related to momentary negative automatic thoughts and negative affect.
Momentary AAT and Momentary Experiences
Momentary AAT (within person) will be positively associated with momentary task avoidance and inattention at the same time point. Mean AAT levels (between person) will also be positively associated with momentary avoidance and inattention. Baseline ADHD symptoms will moderate these relationships such that people with more ADHD symptoms will show stronger positive relationships. Momentary AAT will be negatively associated with negative affect at the same time point, as will mean AAT levels.
Exploratory Analyses
We report the frequency with which participants said they were avoiding different categories of tasks and frequencies for what they endorsed doing instead. We also conducted exploratory lagged analyses testing the relationship between momentary negative affect and likelihood of AAT at the next time point and between momentary AAT and degree of task avoidance at the next time point.
Method
Please note that, because this study is a replication of Knouse et al. (2023), some descriptions of the Measures, Procedure, Plan of Analysis, and language used in the reporting of Results are similar to that paper.
Participants
Data were collected from 106 smartphone-owning adults (age = 18–75 years; M = 38.69, SD = 14.66) from the United States during June and July 2022. Seventy-eight participants (74%) self-identified as women, 26 (25%) identified as men, and 2 (2%) identified with a gender identity other than woman or man. Fourteen participants (13.21%) identified as Black or African-American, 12 (11.32%) identified as Asian, 2 (1.89%) identified as North African or Middle Eastern, 75 (70.75%) identified as White, 1 (0.94%) identified as Native American, 4 (3.77%) selected “Other,” and 3 participants (2.83%) preferred not to answer this question. (Note that categories sum to more than 100% because participants could select more than one.) Six (5.66%) participants identified as Hispanic or Latinx. For highest level of education, 4 participants (3.8%) had completed some college but no degree, 21 (19.8%) were currently enrolled in college, 2 participants (1.9%) had an Associate’s or technical degree, 36 (34%) had earned a Bachelor’s degree, 39 (36.8%) had earned a Master’s degree, and 4 (3.8%) had received a doctoral, medical, or law degree. Forty-seven participants (44.3%) were single, 37 (34.9%) were married, 6 (5.7%) were living with a partner long-term, 15 (14.2%) were divorced, and 1 participant (0.9%) had been widowed. Forty-three participants (40.6%) had children. Eleven participants (10.4%) reported having a diagnosis of ADHD and seven of these participants reported taking medication for ADHD.
Measures
Baseline Self-report
At baseline, participants completed a series of self-report measures. In this report, we only describe the scales used in the current analyses. Information on measures administered can be found on project Open Science Framework (OSF) page at https://osf.io/e56gx/.
The Barkley Adult ADHD Rating Scale (BAARS-IV; Barkley, 2011) asks participants to self-report on the ADHD symptoms they experienced within the last 6 months on a 4-point Likert scale (1 = never or rarely and 4 = very often.) The scale includes the 18 DSM-IV ADHD items and asks participants to detail the age during which they started to exhibit these symptoms. The normative study used to develop the scale (n = 1,249 adults; Barkley, 2011) provides evidence of reliability and validity (test-retest reliability = .75 at 2 to 3 weeks; internal consistency = .91). Mean scores for the 18 DSM-IV ADHD items were used in this study and internal consistency in this sample was good (α = .89). The mean ADHD symptom score in this sample was 1.75 (SD = 0.49).
EMA Measures
The following measures were collected in the order below at each EMA assessment time point. We measured affect first to avoid participants’ report of their thoughts and task avoidance potentially contaminating this measure. Reliability for EMA measures was estimated using a Generalizability Theory framework (Shrout & Lane, 2011), allowing for separate consideration of between-subject reliability (RKR) and within-subject reliability (RCN). For these analyses, time was considered a random variable nested within people. Reliability analyses were conducted using the “psych” package in R, version 2.4.3 (Revelle, 2024).
Affect
Items were drawn from the Positive and Negative Affect Schedule-Expanded form (PANAS-X; Clark & Watson, 1994) to assess the affect of each participant at each separate momentary assessment. Participants were asked to specify the extent (1 = not at all, 5 = extremely) to which they were currently feeling the following emotions: sad (sad, lonely), fear (jittery, nervous), angry (angry, hostile), guilt (guilty, ashamed), and positive moods—specifically from the joviality scale (happy, excited). The term anxious was also included to reflect the frequent use of this term by members of the study population in everyday life. Ratings for the nine negative emotion items were averaged to yield one score reflecting negative affect. The between-subjects reliability for negative affect was substantial (RKR = .98), and the within-subjects reliability was fair (RCN = .57). Ratings for the two positive mood items were also averaged together to yield an overall measure of positive affect. The between-subjects reliability for positive affect was also substantial (RKR = .97). However, these two items were not reliable markers of within-subject change (RCN = .09).
Avoidant Automatic Thoughts (AAT)
To assess presence of avoidant thoughts at each momentary assessment, participants were asked to report whether or not they had each of 10 avoidant thoughts in the last few minutes before receiving the survey. Seven items were drawn from the ADHD Cognitions Scale (ACS-7; Knouse et al., 2019) developed to measure ADHD-related avoidant thoughts and modeled on the Automatic Thoughts Questionnaire (Hollon & Kendall, 1980). Examples of scale items include: “I do better waiting until the last minute” and “I’ll just do this one thing first.” In developing measures for our prior EMA study (Knouse et al., 2023) we noted that the ACS-7 included more thoughts about difficulty disengaging from a current activity (e.g., “I have plenty of time; I’ll just do one more thing before I go.”) but did not have comparable representation of thoughts about delaying engagement in a task. As such, we included three additional items: “I have time to do this later,” “I don’t have to do this right now,” and “I’ll feel like doing this later.” In a prior analysis of single-time-point self-report data using a 5-point Likert response scale (Knouse et al., 2022), we found that these 10 items showed adequate internal consistency (α = .83) and split-half reliability (.74). In this study, participants were asked to check off any thoughts they had in the few minutes preceding receipt of the text. They were first presented with the difficulty disengaging items in a group along with an option reading “another thought like this” with a text box to enter content. Next, they were presented with the delaying engagement items followed by a similar open-ended option. We used endorsement of any of the 10 avoidant thought items (yes/no) in the analyses for the current study. Responses to the “another thought like this” prompt were not included.
Negative Automatic Thoughts (NAT)
To assess NAT, participants were asked to report whether or not they had each of four negative thoughts in the last few minutes before receiving the survey. As for avoidant thoughts, we also included an option to endorse “another thought like this” and fill in the specific content. Items were drawn from the Automatic Thoughts Questionnaire, which measures negative automatic thoughts that are related to depression (Hollon & Kendall, 1980). Items included “What’s the matter with me?” “My life is not going the way I wanted it to,” “I’m worthless,” and “It’s just not worth it.” Again, we used endorsement of any negative thought (yes/no) in our analyses.
Task Avoidance
At each momentary assessment, in response to the prompt: “Right now, to what extent are you putting off doing something you need to accomplish?” participants responded on a 5-point scale (1 = not at all, 5 = a great deal). If they gave a response other than “not at all,” they were also asked to choose the best answer for what it was they were putting off. (See supplement on Open Science Framework for more information at https://osf.io/e56gx/) Participants were then asked to specify the urgency of the avoided task (1 = not urgent, 5 = very urgent) and its importance (1 = not important, 5 = very important). Participants were also asked to specify the extent to which they were aware of their own avoidance prior to being asked about it in the survey (1 = not at all aware, 3 = very aware). Finally, they were asked what task they had been doing instead of the avoided task.
Inattention
Four items were drawn from the BAARS to assess inattention at each separate momentary assessment. Participants answered each question using a 5-point scale ranging from 1 = not at all to 5 = a great deal. The between-subjects reliability of these four items was substantial (RKR = .98), and the within-subjects reliability was moderate (RCN = .69).
Procedure
The study was advertised via flyers, social media (e.g., Facebook ads and posts), to staff of the University at which the research took place via the institution’s daily email of events, and through word of mouth. Participants first completed a short online screening questionnaire to determine eligibility for the study. To participate, volunteers had to endorse generally being awake from 9 am to 10 pm, using a smartphone daily, being over the age of 18 years, and endorsing that they would be located in the same time zone for the duration of the study. We structured our recruitment to obtain a broad age range. Specifically, once 25 participants in the 18 to 25 years range were recruited, we screened out additional participants in this age range for the remainder of the recruitment period. Participants who screened into the study were directed to a scheduling page where they could self-schedule a time for a baseline visit via Zoom video conferencing.
During the videoconferencing baseline visit, which lasted up to 1 hour, participants were given information about the study procedures by a study research assistant and completed the informed consent process. Participants were then assigned a study ID that would link their data across the baseline and EMA surveys. Next, the research assistant guided the participant in enrolling with the SurveySignal online platform in order to receive text messages for the EMA portion of the study. Once SurveySignal enrollment was confirmed, the participant completed online baseline questionnaires in Qualtrics to assess a variety of psychological and behavioral variables (see Measures Section).
During each of the 6 days of the EMA portion of the study, participants received five text messages with unique links to Qualtrics surveys per day. The first text was sent on the day following the baseline session. Texts were sent within five specified time blocks between 9 am to 10 pm, with randomized delivery times within blocks allowing for a minimum of 60 minutes between surveys. The participant had up to 1 hour to complete each survey after which the link was inactive. A reminder text was sent if a given survey was not completed within 20 minutes At the conclusion of participation, participants were sent, via email, compensation of $20 for the baseline visit and $0.50 for each completed EMA survey in the form of an Amazon gift code for maximum compensation of $35.00. Participants who completed 75% or more of the EMA surveys were also entered into a raffle for one of two $100 Amazon gift codes. The payment email also contained study debriefing information.
Plan of Analysis
See https://osf.io/xdy4f for study pre-registration. We used multilevel modeling (MLM) to test the key hypotheses. Analyses were conducted in R using the lmer package using full information maximum likelihood estimation for continuous outcomes and the glmer package with a binomial link function for dichotomous outcomes. Data were structured within three levels: Occasion (Level 1), Day (Level 2), and Participant (Level 3). We centered ADHD symptoms (Level 3) at the grand mean and we centered AAT (Level 1) within-person (centering within cluster) by subtracting each person’s mean from each momentary value (Yaremych et al., 2023). When testing the effects of AAT, we included both the within-person centered variable and each participant’s mean in order to parse within vs. between person variance.
For each dependent variable, we first calculated a null model to estimate the proportion of variance at each level. Although none of our key variables of interest are Level 2 (Day), we included Level 2 because null models indicated substantial variance at this level in our data (see Table 1). We also included the Level 2 variable of Weekend (YES/NO; weekend defined as Saturday and Sunday) and the random effects of weekend our models when possible computationally. Level 1 predictors were included with random effects. If models fail to converge we systematically fixed effects in each model based on degree of theoretical interest until convergence was obtained (Barr et al., 2013). Specifically, we first fixed the slopes for weekend and, if the model still did not converge, we fixed the slopes of other variables based on theoretical importance such that the most important fixed effects also had corresponding random slopes when possible. Finally, if required for convergence, we removed Level 2 from the model. The specific models estimated for each analysis are indicated in the Table captions.
Intraclass Correlations for Momentary Variables.
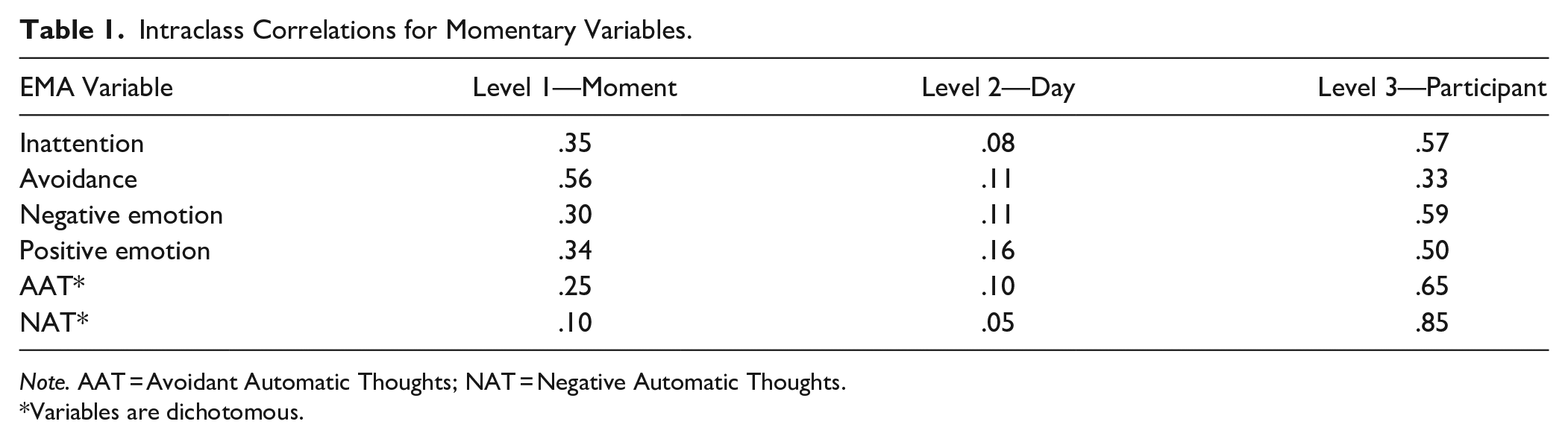
Note. AAT = Avoidant Automatic Thoughts; NAT = Negative Automatic Thoughts.
Variables are dichotomous.
We first tested whether ADHD symptom scores (Level 3) predicted momentary inattention, task avoidance, AATs, NATs, and negative emotion. We then tested whether AAT (Level 1—both within person variance as measured by person centered AAT and between person as measured by each person’s mean AAT) predicted task avoidance, inattention, and negative emotion and whether ADHD symptoms increased the strength of the relationship between the within person centered AAT variable and both task avoidance and inattention–that is, whether there was a cross-level interaction for these variables and whether simple effects supported the pattern described above.
We then proceeded with exploratory analyses including a descriptive analysis of what participants reported as their avoided task and the tasks they were doing instead as well as exploratory lagged analyses of the relationship between negative emotion at Time 1 and AAT at Time 2 and the relationship between AAT at Time 1 and avoidance at Time 2.
Departures From Pre-registration
As described in our pre-registered data collection plan, we planned to discontinue participant recruitment when we had collected EMA data from 100 participants. In practice, during the final week of data collection, we scheduled a number of participants that we estimated would meet this threshold based on the observed no-show rate during the previous weeks. As such, as indicated in our pre-registered plan, this effort to account for non-completers resulted in slight oversampling of 106 participants.
Our pre-registration erroneously indicated that, in scoring the EMA responses for AAT and NAT, we would score these variables as “present” if participants checked the “other thought like this” item (two such options for AAT and one option for NAT). We did not include these items in order to replicate the procedure of our prior study (Knouse et al., 2023). Importantly, this scoring adjustment was made prior to any data analyses.
Finally, some of the pre-registered hypotheses used incorrect level labels for the key variables (i.e., Level 1 vs. Level 3). This has been corrected in the statement of hypotheses made here.
Results
Preliminary Analyses
We identified 36 duplicate surveys in the dataset (1.5%) and deleted them, keeping the survey that was earlier and therefore closer in time to the original survey prompt. This resulted in a total of 2,439 EMA data points from 106 participants, where the number of surveys completed ranged from 5 to 30 per participant with a mean of 23.01 (SD = 6.57). It should be noted that some surveys were missing due to two instances in which the system sending the text messages was temporarily offline. Importantly, self-reported ADHD symptoms at baseline were not significantly correlated with the number of surveys completed (r = −.09, p = .34). In response to a suggestion from an anonymous reviewer, we also examined whether data missingness was related to age and to the proportion of AAT reported across moments for each participant. Results showed that younger participants returned fewer surveys (r = .20, p = .04), and participants who reported AATs on a greater proportion of the surveys they did complete also returned fewer surveys (r = −.31, p = .001).
AAT were endorsed at 44.9% of the moments sampled during the study and the median participant reported AAT at 48% of sampled moments. Ninety-seven percent of participants endorsed AAT for at least one sampled moment and 7.5% reported AAT at every sampled moment.
The intraclass correlation coefficients for all momentary variables (Table 1), reflecting the proportion of total variance at each level, indicated sufficient variance to justify the multilevel modeling approach and the three-level modeling structure, given that Level 2 (Day) accounted for between 5% and 16% of the variance in the momentary variables.
ADHD as a Predictor of Daily Experience
As shown in Table 2, as predicted, self-reported ADHD symptoms at baseline were associated with greater momentary inattention, task avoidance, negative emotions, avoidant thoughts, and negative thoughts. ADHD symptoms at baseline also predicted lower levels of momentary positive emotion. Thus, this self-report measure of ADHD symptoms at a single time point predicted thoughts, feelings, and behaviors in daily life in this community sample.
Baseline Mean ADHD Symptoms (Level 3) Predicting Daily Experiences.
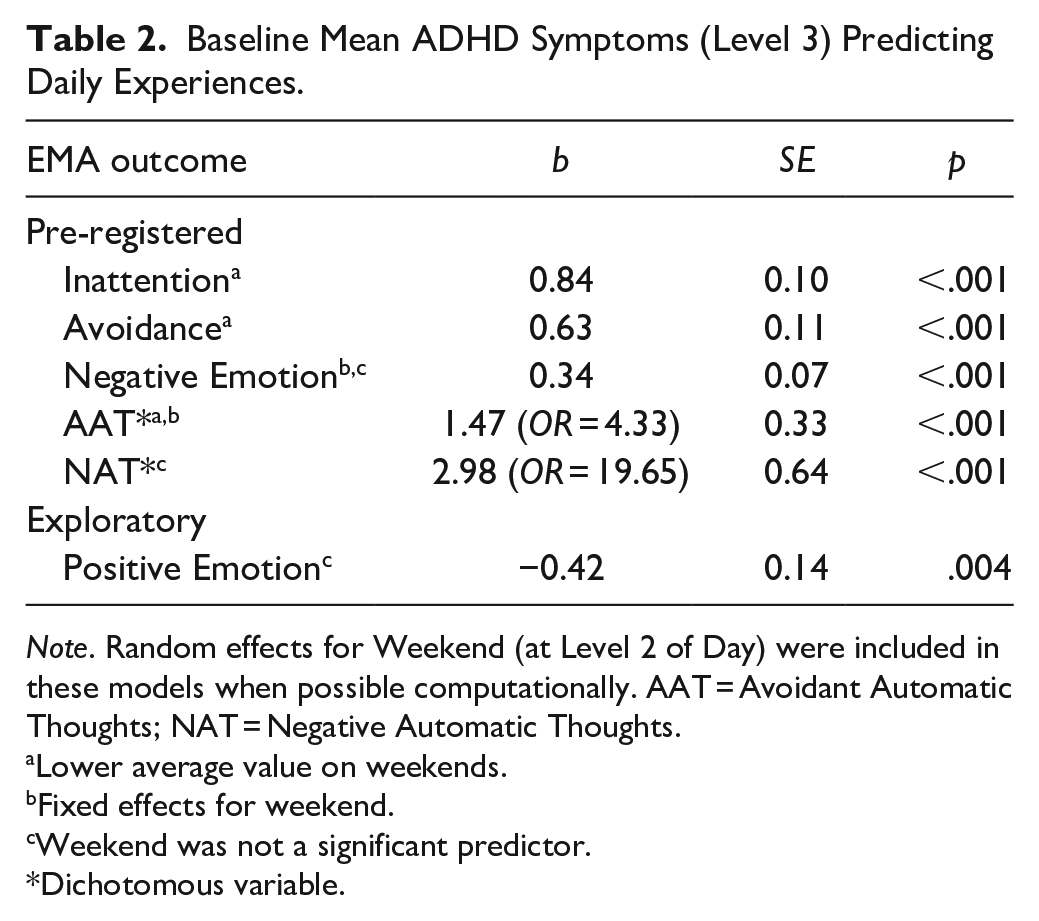
Note. Random effects for Weekend (at Level 2 of Day) were included in these models when possible computationally. AAT = Avoidant Automatic Thoughts; NAT = Negative Automatic Thoughts.
Lower average value on weekends.
Fixed effects for weekend.
Weekend was not a significant predictor.
Dichotomous variable.
Momentary Relationships Between AAT and Key Variables
Main Effects
As shown in Table 3, as predicted, the presence of AAT was positively associated with both momentary task avoidance and inattention. This relationship was significant for both the momentary level (person mean centered variable) and the person level (each person’s grand mean). In other words, while people who report more frequent AAT in general were also more likely to report greater inattention and task avoidance at a given moment, the presence of AAT at a given moment also predicted greater task avoidance and inattention soon after.
Main Effect of AAT Predicting Momentary Experience (Same Assessment Point).
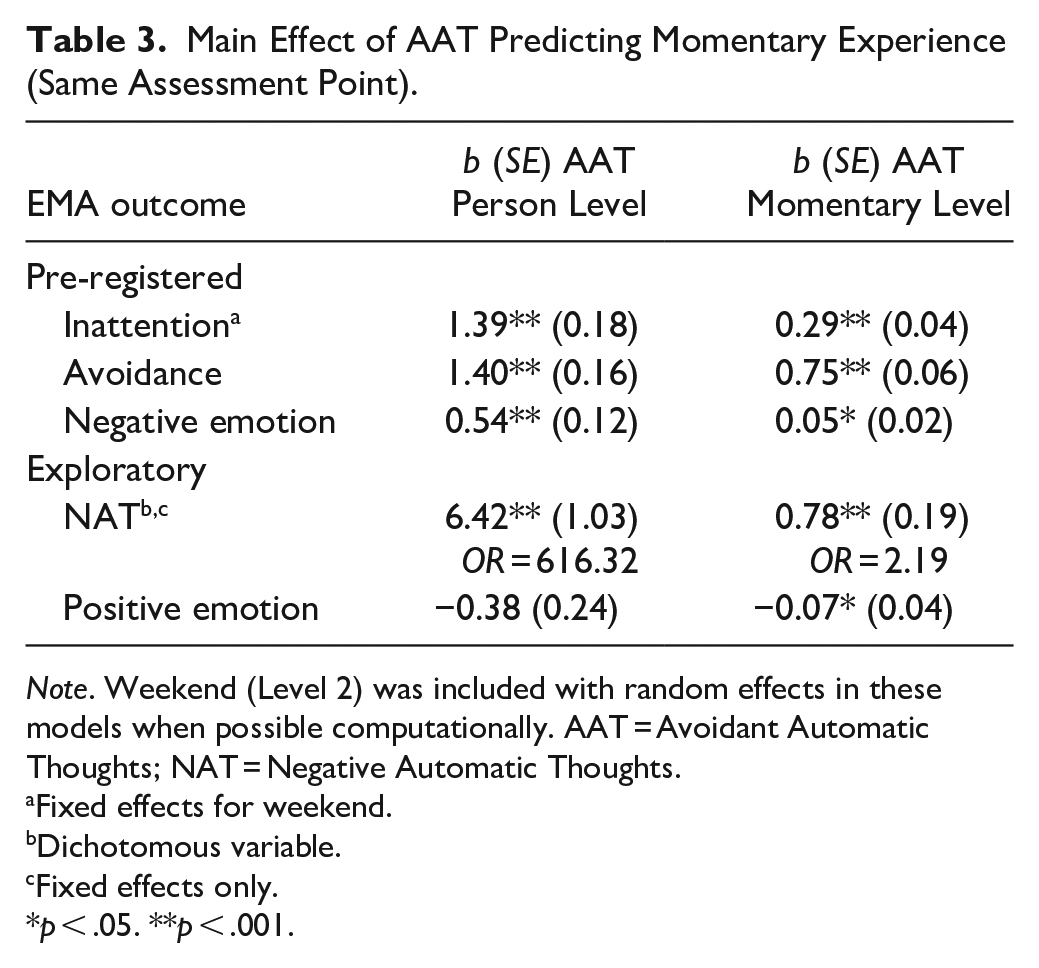
Note. Weekend (Level 2) was included with random effects in these models when possible computationally. AAT = Avoidant Automatic Thoughts; NAT = Negative Automatic Thoughts.
Fixed effects for weekend.
Dichotomous variable.
Fixed effects only.
p < .05. **p < .001.
We had predicted that the presence of AAT would be associated with lower levels of negative emotion. However, the momentary relationship, although small, was in the opposite direction, such that the presence of AAT was associated with slightly elevated negative emotion. There was also a significant positive person-level relationship between AAT and negative emotion. In other words, people who generally experience AAT more frequently in daily life are also more likely to report negative emotion in a given moment.
In exploring the relationship between AAT and NAT, we found a positive association between these avoidant thoughts and negative thoughts at both the person and the momentary level. For AAT and positive emotion, we did not observe a relationship at the person level and found a weak negative relationship between AAT and positive emotion at the momentary level. In other words, when people report AAT in a given moment, they tend to report slightly less positive emotion.
Moderation by ADHD Symptoms
We predicted that ADHD symptoms would strengthen the relationship between AAT and task avoidance and inattention. As shown in Table 4, in contrast to findings in our prior study (Knouse et al., 2023), both of these predictions were fully supported, such that the relationships between momentary AAT and both inattention and task avoidance were stronger for participants with more severe ADHD symptoms. Simple slopes showed that the momentary level AAT-inattention effect was 0.20 (SE = 0.06, p < .001) at 1 standard deviation below the mean for ADHD symptoms, 0.28 (SE = 0.04, p < .001) at the mean, and 0.37 (SE = 0.05, p < .001) at 1 standard deviation above the mean. In other words, the mean difference in inattention between a moment without and with an AAT increases from .20 for people with low ADHD symptoms to .28 for people with average ADHD symptoms, to .37 for people with high ADHD symptoms. For the AAT-avoidance effect, simple slopes showed 0.59 (SE = 0.08, p < .001) at 1 standard deviation below the mean for ADHD symptoms, 0.73 (SE = 0.05, p < .001) at the mean, and 0.88 (SE = 0.07, p < .001) at 1 standard deviation above the mean. In other words, the mean difference in avoidance between a moment without an AAT and with an AAT increases from .59 for people with lower ADHD symptoms to .73 for people with average ADHD symptoms, to .88 for people with high ADHD symptoms.
Testing Interaction Effect of AAT and ADHD Symptoms on Momentary Experience (Same Assessment Point).
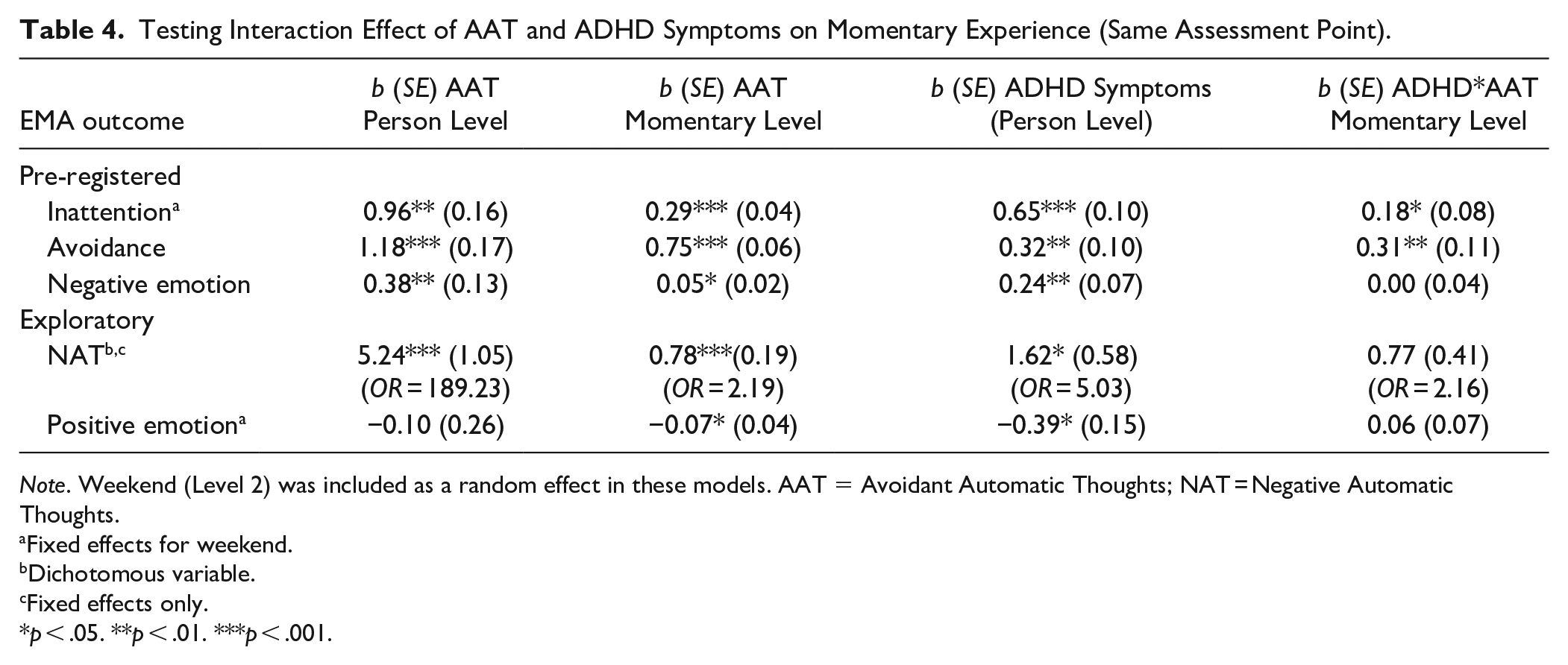
Note. Weekend (Level 2) was included as a random effect in these models. AAT = Avoidant Automatic Thoughts; NAT = Negative Automatic Thoughts.
Fixed effects for weekend.
Dichotomous variable.
Fixed effects only.
p < .05. **p < .01. ***p < .001.
Exploratory analyses did not detect significant moderation effects of ADHD symptoms on the relationship between AAT and negative emotion, NAT, or positive emotions.
Exploratory Analyses
What Are People Avoiding, and What Are They Doing Instead?
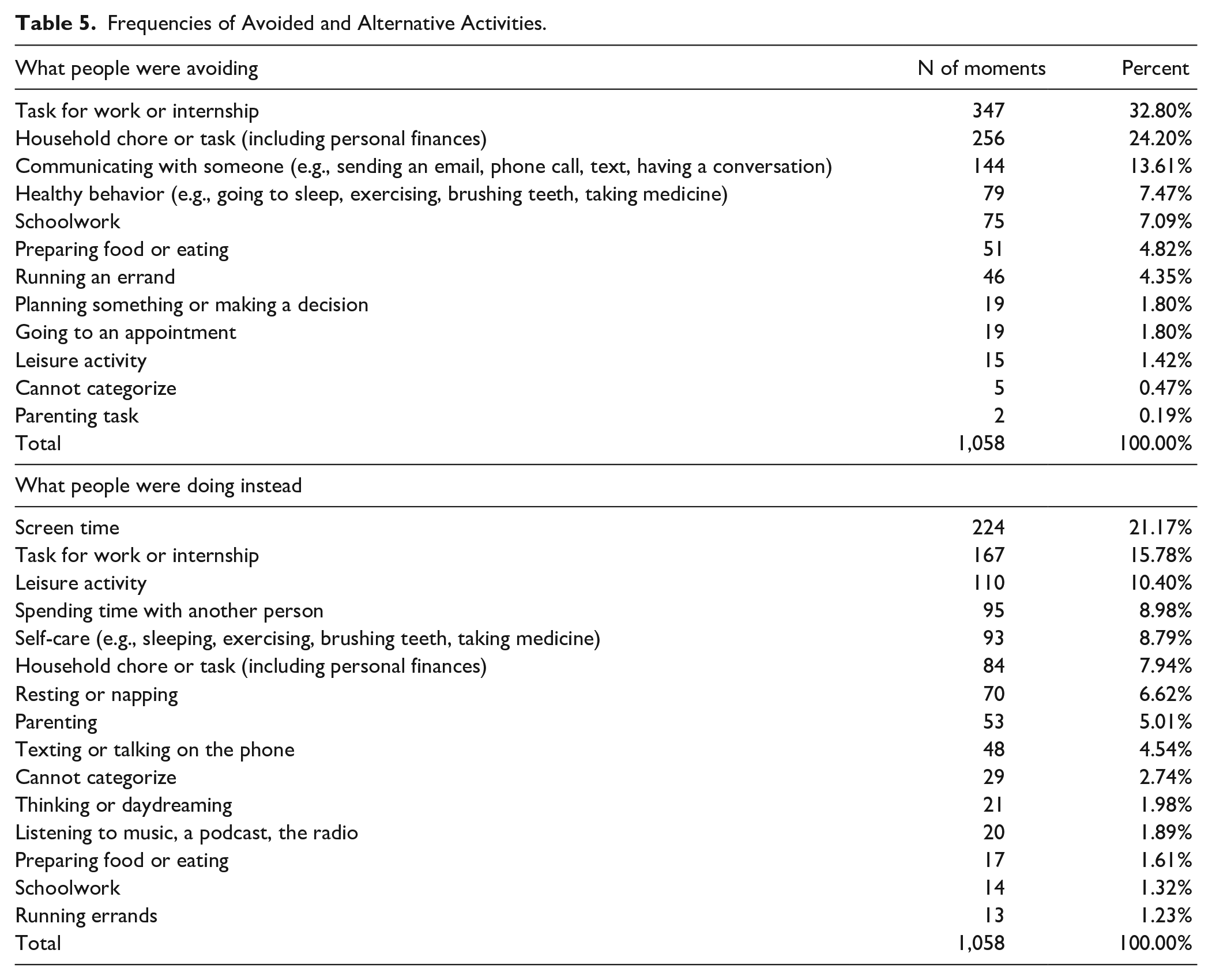
We were also interested in describing what kinds of tasks people were putting off and also what alternative activities people were engaging in when they reported putting off doing something they needed to accomplish. A detailed description of these analyses appears in the Online Supplement on Open Science Framework at https://osf.io/e56gx/. Table 5 provides a description of what people avoided and what they reported they were doing instead. The most frequently reported avoided activities were work tasks (32.80%), household chores (24.20%), and communicating with others (13.61%). The most commonly reported alternative activities were screen time (21.17%) and work tasks (15.78%). We further explored these data and found that certain avoided activities were differentially associated with certain alternative activities, χ2(153) = 282.97, p < .001. Here, we focus on the two most commonly avoided tasks—work tasks and household chores. When avoiding work tasks, people were more likely than would be expected to be engaging in other work tasks, but were less likely than would be expected to be engaging in screen time, leisure activities, self-care, and parenting. When avoiding household chores, people were more likely than would be expected to be engaged in self-care activities and screen time and less likely than would be expected to be doing tasks for work.
Frequencies of Avoided and Alternative Activities.
What Happens in the Hours Before and After AATs?
We explored whether moment-level negative emotion at Time 1 would predict AAT at the next time point (at least 1 hr later) and whether moment-level AAT at Time 1 would predict subsequent task avoidance. Negative emotion at the moment level was not a significant predictor of AAT at the next time point (p = .48). Moment-level AAT did significantly predict avoidance at the next time point (0.19, SE = 0.05, p < .001); however, when Time 1 avoidance was added to the model, Time 1 AAT was no longer significant (−.02, SE = 0.05, p = .63) suggesting that ATT was not associated with avoidance at later time points above and beyond avoidance at the prior timepoint. See Supplement on OSF for full results of these analyses.
Discussion
The current study replicates and extends our prior findings regarding AAT in daily life. In this sample of community adults, we found that AAT were frequently reported; specifically, at nearly 45% of the moments sampled. This rate is slightly lower than the 53% reported by college students in the previous study (Knouse et al., 2023), but still represents a substantial proportion of participants’ daily experience. Replicating the prior study, recent presence of AAT was associated with increased task avoidance and inattention, but not with reduced negative emotion. In fact, in this study, recent presence of AAT was associated with a slight but significant elevation in negative affect. We later return to a discussion of these emotion-related findings with respect to an escape-avoidance theory of AAT later in the Discussion.
As in our prior study, more severe ADHD symptoms at baseline predicted higher rates of AAT, task avoidance, and inattention in daily life. In contrast to the prior study, more severe ADHD symptoms at baseline significantly moderated (strengthened) the relationship between AAT and avoidance. This difference in findings across studies may be due to the increased power afforded by five-times-per-day sampling in the current study compared to only three times daily in the prior study since, notably, the size of the moderation effect was comparable across studies. This significant moderation effect means that people with more severe ADHD symptoms not only reported experiencing AAT more often in daily life but, when those thoughts were present, they were also even more likely than people with less severe ADHD symptoms to report task avoidance. This finding suggests that, metaphorically, AAT may be “stickier” for people with greater ADHD symptoms in the sense that, when they occur, AAT are more likely to link to avoidance.
In this study, we explored what kinds of tasks people were avoiding and also what they did in lieu of the avoided task. We observed the somewhat counterintuitive result that work tasks are among both the most frequently avoided activities and the most frequent alternative activities. Looking further into the data, we discovered that work tasks were much more likely than would be expected by chance to be an alternative activity to other avoided work tasks—perhaps reflecting the idea of “productive procrastination” or “procrastivity” that is prominent in popular culture and investigated in some recent academic research (Westgate et al., 2017). 1 Screen time was, overall, the most common alternative activity, but it was much more commonly associated with avoidance of household chores and tasks than with avoidance of work tasks. If we assume that at least some of the avoided tasks reported by our participants were meaningful to them or that accomplishing them would improve quality of life, these results suggest that people might benefit from even small incremental shifts of engagement in lower priority (possibly easy) to higher priority (possibly harder) work tasks and from screen time to household tasks.
Our work raises the question of whether AAT are always and inherently maladaptive and, if not, how to identify adaptive instances of AAT. Our answer to the first question is a resounding “no”—AAT are probably often neutral in their association with maladaptive behavior and outcomes and sometimes are adaptive. 2 The most obvious reason for this is that avoidance of aversive stimuli is not inherently maladaptive. Organisms evolved the capacity for avoidance learning precisely because it is often adaptive. Likewise, there are many instances in which avoiding certain tasks at a given time might be efficient or strategically advisable.
In our view, the only definitive answer to the second question—how to distinguish an adaptive instance of AAT from a maladaptive one—is to examine the functional outcome of a given instance and judge whether that outcome is consistent with a person’s goals and values. This conceptualization of AAT is consistent with contextual behavioral science in that a given instance of thought-behavior cannot be understood or evaluated outside of its context (Hayes et al., 2012). In other words, we believe it is not possible to identify a maladaptive AAT simply by its content. While this position might seem to be at odds with our approach in the current study, the coping literature demonstrates that, in the aggregate, when people’s responses to stress are dominated by automatic and inflexible coping responses, including escape and avoidance, functional outcomes tend to be worse (Skinner & Zimmer-Gembeck, 2016). As such, examining a person’s patterns of thoughts, behaviors, and outcomes that taking into account context as much as possible (using, e.g., EMA) can identify instances in which AAT are more likely to lead to functional outcomes. As such, future research on AAT should examine their relationship with additional contextual factors (e.g., type of task avoided; types of situations) as well as continue to link AAT and avoidance to functional outcomes (e.g., life satisfaction; comorbidity; see Knouse et al., 2019).
Using the concept of negative reinforcement, Knouse and Mitchell (2015) proposed an escape-avoidance account of AAT-like thoughts—specifically, that such thoughts occur in people’s private behavioral repertoires because they are frequently immediately reinforced by a reduction in aversive internal experiences (i.e., distressing emotions). For example, when an aversive task comes to mind and unpleasant emotions arise, thoughts such as, “I have plenty of time to do that tomorrow!” have as their consequence an immediate reduction in unpleasant emotions. Thus, in our prior study, we predicted that recent presence of AAT would be associated with lower levels of negative emotion and argued that such a result was consistent with the escape-avoidance account. In that prior study and in the current study, however, when AAT had been recently present, people’s levels of negative emotion were slightly higher than their average. Such a result could be interpreted as inconsistent with the escape-avoidance account of AAT.
On the other hand, two methodological limitations prevent these results from providing a definitive test of the escape-avoidance account. First, as noted in our prior paper, the fleeting nature of reductions in negative emotion following AAT onset may not be captured by the EMA method. In that paper, we suggested that methodologies such as psychophysiology or event-related potentials (ERP) might be needed to capture the temporal dynamics of avoidant automatic thought and emotion (Kam et al., 2021; Raugh et al., 2019). Second and as important, we do not know what participants’ level of negative emotion was before the onset of each AAT. Negative reinforcement is defined by a reduction of an event as a consequence of behavior that results in an increased occurrence of that behavior (Hineline & Rosales-Ruiz, 2013). As such, a reduction in the relative intensity of aversive emotion could negatively reinforce AAT, even if the absolute intensity of negative emotion remains above a certain threshold. Taken together, these facts limit the extent to which the escape-avoidance account of AAT can be rigorously evaluated using our current EMA methods.
Despite the difficulties in assessing the scientific veracity of the escape-avoidance explanation of AAT, we argue that this conceptualization offers a clinically useful framework for understanding and intervening with problematic AAT in daily life. Clinicians using skills-based approaches can readily incorporate AAT work into their practice in at least two ways: (1) Conduct assessment and psychoeducation with clients regarding AATs, and, (2) Incorporate AATs into standard cognitive therapy strategies. During initial assessment, clinicians can provide a brief explanation and examples of AATs and ask clients whether they experience these thoughts and whether they seem to be associated with avoidance or other problematic responses. The ADHD Cognitions Scale, a short self-report scale freely available in the published report, might be a useful tool (Knouse et al., 2019). When providing psychoeducation on the emotion-thought-behavior interplay inherent to the CBT model, clinicians can incorporate specific examples of AAT provided by the client.
With respect to cognitive therapy strategies, we have found that AAT can be easily incorporated into the typical strategies that CBT clinicians use to help clients become aware of potentially problematic thoughts and change their responses to these thoughts–for example, self-monitoring and skills practice using a daily thought record (DTR). Clinicians do, of course, have to expand the prompts they use to help clients identify relevant instances to self-monitor. For example, a typical prompt might be that the client should complete the DTR when they notice a significant negative shift in emotion. Since AAT may not result in such a shift, instructions to the client could also include a prompt to complete the DTR when they notice they have gotten off track in terms of their goals in a given instance. Increased awareness of the emotion-thought-behavior relationship can then be followed by the application of a variety of other CBT skills to increase engagement in valued action and reduce avoidance (Canu et al., 2023; Knouse & Mitchell, 2015; Knouse et al., 2023). In the future, EMA might be a useful tool to these clinical ends as well.
This study’s limitations should be noted. First, the nature of our sample and therefore the generalizability of our results should be considered. Our sample was a mostly White and relatively highly educated sample of mostly women in the United States and therefore the results of this study are limited to samples with these characteristics. Second, although we investigated the association of AAT with ADHD symptoms, we did not specifically recruit people diagnosed with ADHD so we cannot draw conclusions about clinical levels of ADHD and AAT. Third, some of our EMA measures lacked adequate within-person reliability—particularly our measure of positive emotion in the moment. This limits our ability to detect within-person effects and cross-level interactions for these variables. In the future, we intend to develop more reliable versions of these measures for use with EMA. Finally, we captured fewer moments from younger participants and from participants who, when they did respond, were more likely to report AAT. This latter result raises the possibility that EMA surveys are missing not at random (MNAR) and, although this issue is a common one that is recognized as a pressing in the field, few robust solutions exist in multilevel modeling when data are MNAR (Stone et al., 2023). As such, readers should interpret our results with some caution and consider that results may be biased by survey missingness.
The results of this study suggest several future research directions. First, as noted above, we need to further investigate the function of AAT in people actually diagnosed with ADHD as well as whether particular tasks are more avoided by this population. Second, we intend to investigate the transdiagnostic nature of AAT by extending our investigations to other disorders, symptom dimensions, and areas of functional relevance. Third, to facilitate future research endeavors, we intend to develop an improved, more comprehensive measure of avoidant and other varieties of automatic thought. In the past, automatic thought measures have been closely tied to the clinical populations they were developed to study (mostly, the emotional disorders; Glass & Arnkoff, 1997), limiting their potential utility for study of automatic thoughts across diagnostic categories. Indeed, most of the items in our measure of AAT were drawn from a scale designed to measure automatic thoughts reported by people with ADHD (Knouse et al., 2019), and so there is room for a measure that is more diagnosis-neutral. The development of better measures of AAT is also consistent with the experimental medicine approach advocated by the National Institutes of Health Science of Behavior Change program (Nielsen et al., 2018), as improved measurement will allow us to continue to evaluate the target validity of AAT—that is, the extent to which changes in AAT frequency or “stickiness” lead to changes in avoidance behaviors. Additional research should then focus on target engagement by investigating what kinds of interventions can most strongly alter AAT frequency or impact. For example, we are interested in testing whether EMA could be used as a clinical tool in this regard.
Conclusion
The current study demonstrates that AAT are a frequent daily occurrence in the lives of the adults we sampled and that they potentiate task avoidance and inattention in the moment. Frequent AAT that are more powerfully associated with task avoidance may be one mechanism by which adults with more severe ADHD symptoms experience impairment in daily life. In a world with increasingly complex choice landscapes, helping people develop strategies to respond to AAT by acting in line with their values and goals might improve quality of life and mental health.
Footnotes
Acknowledgements
The authors would like to thank Sampson Valdez for his assistance in data collection for this project.
Author’s Note
Yueyi Fan is also affiliated to University of Pennsylvania, PA, USA.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L. Knouse is a member of the Professional Advisory Board of Children and Adults with ADHD (CHADD), receives book royalties from Routledge Publishers, and is a clinical and research consultant for Get Inflow, LTD. The other authors have no competing interests to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: L. Knouse was funded by a School of Arts and Sciences Faculty Summer Fellowship and by a Provost’s Faculty Fellowship from the University of Richmond during the completion of this work and the University of Richmond provided funding for the project. Y. Fan and A. Narayanan were supported by the School of Arts and Sciences Undergraduate Summer Research Fellowships.