
Abstract
Objective:
This study investigated the psychometric properties of the Arabic version of the Adult Self-Report Scale-5 (the ASRS-5-AR) within a large sample of adults residing in Saudi Arabia.
Methods:
This cross-sectional study applied the ASRS-5-AR to a random sample of 4,299 Saudi and non-Saudi adults, aged 19 to 66 years (31.16 ± 9.26 years), living in the regions of Riyadh, Makkah, and the Eastern Province in Saudi Arabia. Collected data were analyzed using IBM SPSS Statistics 26, JASP 0.18.3.0 software, and MedCalc 22.030 statistical software.
Results:
The ASRS-5-AR demonstrated strong internal consistency, with all six items showing significant positive correlation with the total score (.675–.735). Results of confirmatory factor analysis revealed a goodness-of-fit coefficient of 0.983 for the one-factor model and McDonald’s omega, Cronbach’s α, and Spearman-Brown coefficients of 0.786, 0.788, and 0.724, respectively. In addition, the findings revealed statistically significant differences in self-reported ADHD symptoms based on age (F = 18.68; p < .001), level of education (F = 2.61; p < .05), and marital status (F = 22.30; p < .001). However, there were no significant differences in self-reported ADHD symptoms between males and females (t = 0.625; p > .05) or Saudi and non-Saudi participants (t = 0.409; p > .05) or based on region of residence (t = 2.19; p > .05).
Conclusions:
This study provides valuable insights into the psychometric properties of the ASRS-5-AR within a large sample of adults in Saudi Arabia. The findings demonstrate acceptable reliability of the ASRS-5-AR within this population. While these findings suggest the ASRS-5-AR may be a useful tool for initial assessment, further research is crucial. Future studies should focus on establishing accurate cutoff scores by comparing a general population sample with a clinically diagnosed sample of adults with ADHD in Saudi Arabia. This will allow for a more accurate evaluation of the scale’s utility in identifying individuals who may require further clinical assessment.
Introduction
Attention-deficit/hyperactivity disorder (ADHD), a prevalent neurodevelopmental disorder typically diagnosed during childhood years, can manifest with symptoms that persist into adulthood. Over the past 10 years, the prevalence of ADHD among adults has increased by 123% (Chung et al., 2019). There has also been a rise in the awareness of ADHD in adults and an increase in the numbers of adults seeking diagnosis. Those two factors alongside the evolving diagnostic criteria of the DSM-5 have driven the demand for reliable, evidence-based assessment methods for this underdiagnosed population (Kooij et al., 2019).
Data on the prevalence of ADHD have been conflicting. In one meta-analysis, Willcutt (2012) reported that the prevalence of ADHD among adults according to studies conducted in the United States, Iran, Colombia, and Australia was 5%, which was 1.5- to 2.3-times higher than rates reported by European studies. Prevalence among older adults was reported by Dobrosavljevic et al. (2020) to be 2.18%. According to another meta-analysis, reviewing 2346 global studies, persistent ADHD (that is, ADHD manifesting in childhood and continuing to adulthood) was found to be prevalent among 2.58% of adults, while the prevalence of symptomatic ADHD reached 6.67%, indicating that there were approximately 139.84 million and 366.33 million adults, respectively, with ADHD globally (Song et al., 2021). Recent reports for ADHD prevalence in the Middle East and North Africa show ranges from 1.3% to 22.2%, and the rate is higher in adults (13.5%) than in children and adolescents (10.10%) (Al-Wardat et al., 2024).
Studies also indicate that the disorder is more prevalent among men than women, young adults compared with older adults, divorced individuals compared with people who are unmarried, and people who have high income compared with those of low income (Hargitai et al., 2023). Other reports, however, show no differences in prevalence between countries of low, middle, and high income (Cortese et al., 2023).
Symptoms of ADHD in adults include impulsivity, restlessness, disorganization, problems concentrating, poor time management skills, problems focusing on a specific task, poor listening skills, and difficulty relaxing. Compared with children who have ADHD, adults are less likely to be hyperactive, and, thus, symptoms may be less noticeable in adults (American Psychiatric Association, 2013; Faraone et al., 2003). In addition, ADHD symptoms can make everyday tasks more difficult and contribute to problems like missing meetings or social plans and difficulty setting priorities, focusing, and completing tasks (Canu et al., 2020; Chung et al., 2019; Hargitai et al., 2023; Lutfi, 2022). ADHD is also associated with greater mortality by unnatural causes (Cortese et al., 2023).
Kessler et al. (2005) noted that developing measures to assess ADHD in children, adolescents, and adults is challenging, because symptoms continuously change throughout development. According to Niina et al. (2022), symptoms of ADHD differ at ages 7, 17, and 25 years. At age 7, fidgeting, talking excessively, and being easily distracted are most common. At age 15, common symptoms include being easily distracted, having difficulty organizing, and avoiding task that require concentration; while at age 25, difficulty calming down, feeling frustrated, difficulty organizing, and being easily distracted are the most common symptoms. Consequently, Haavik et al. (2010) pointed out that the diagnostic evaluation of adults with ADHD should include symptoms other than those typically seen in children, including mood instability, frustration intolerance, anxiety, personality disorders, and symptoms of comorbid psychological disorders. They also emphasized that it is important the evaluation be based on a combination of assessments including clinical interviews, rating scales for previous and current symptoms, and additional information from multiple raters for those symptoms to develop appropriate therapeutic interventions according to the diagnostic features.
There are various scales to assess ADHD in adults, based on the individual’s current ADHD symptoms, functional impairment, quality of life, and the DSM-5 diagnostic criteria. The most widely accepted tools that allow for retrospective assessment of childhood ADHD symptoms are the Wender Utah Rating Scale and Barkley and Murphy’s Childhood Symptoms Scale. Widely used self-reported rating scales include the Conners’ Adult ADHD Rating Scale (1997), the Current Symptoms Scale by Barkley and Murphy (1998), the Adult ADHD Self-Report Scale (ASRS) by Kessler et al. (2005), and the Attention Deficit Hyperactivity Disorder-Self Report Scale (ADHD-SR) by Rösler et al. (2004). All of these scales assess ADHD based on DSM criteria, while the Wender-Reimherr Interview uses a different diagnostic algorithm (Rösler et al., 2006).
It is crucial to identify ADHD in individuals because of the significant personal, familial, and social costs involved; however, diagnosing the condition remains a challenge, typically relying on the DSM for the general population (Perera et al., 2020). To address the need for a tool to screen for ADHD in adults in the general population, the World Health Organization (WHO) developed the Adult ADHD Self-Report Scale-version 1.1 (ASRS-v1.1) in collaboration with the WHO International Composite Diagnostic Interview. The tool is available in two versions: a full version, with 18 questions, and a shortened version, with six questions (Kessler et al., 2005). The ASRS-v1.1 was developed based on the 18 diagnostic criteria in the DSM-IV-TR, such as trouble wrapping up, difficulty organizing, problems with remembering, fidgeting, and being overly active, organized in two parts. Part A consists of six questions that are more predictive of ADHD symptoms, and Part B contains 12 questions (Adler et al., 2019).
The ASRS is a valuable tool used to identify adults who require a more comprehensive assessment for ADHD. Its credibility and reliability for use with the general population have been confirmed in various studies (Anbarasan et al., 2020). According to reports, the short, six-item, version has shown greater sensitivity (68.7%), specificity (99.50%), and symptom concordance (0.08) compared with the full version (Garland, 2006), and it should be preferred in community studies or clinical outreach programs for raising awareness and detecting cases (Kessler et al., 2005). Therefore, Garland recommended using the short version to diagnose ADHD among adults for both community and clinical purposes.
There are two commonly used versions of the ASRS: the previously mentioned ASRS-v1.1 and the ASRS-5. The ASRS-v1.1 was developed in 2005 and has since been translated into 20 languages. The ASRS-5 was developed in 2017, calibrated according to the criteria of the DSM-5 (Ustun et al., 2017). Naturally, to date, there are fewer studies verifying the psychometric properties and clinical usefulness of the ASRS-5 compared with the ASRS-v1.1 (Ziobrowski et al., 2023). The ASRS-5 was translated into the Italian language by Somma et al., in 2021, who reported it to be a psychometrically sound self-reported instrument that can be used safely and reliably to diagnose symptoms of ADHD in both adolescents and adults. Baggio et al. (2021) verified the psychometric properties of the French version of the ASRS-5 on a sample of 557 adults, and their results showed that the tool had good validity and reliability indexes. Their sample consisted of outpatients with no comorbid disorders. The ASRS-5 was found to be a good predictor of ADHD, with a cutoff score of 13/24, sensitivity of 84.3%, and specificity of 91.9%. The tool was also translated into the German language by Ballmann et al. (2022) who verified its psychometric properties on a sample of 262 patients, aged 18 to 65 years, in the primary care setting. The scale showed good psychometric properties (sensitivity, 95.60%; specificity, 72.30%), and results of confirmatory factor analysis revealed that the best fit was achieved for the general factor with one correlated error.
Objectives
This study represents one of the rare community surveys screening for ADHD in adults in different regions of Saudi Arabia. It aims to verify the psychometric properties of the Arabic version of the ASRS-5 (ASRS-5-AR) and to detect differences in ADHD screening based on sociodemographic characteristics. The study helps to raise awareness of ADHD in the society and detect cases in the general population that require comprehensive diagnosis and treatment.
Methods
Participants and Procedures
This study utilized a convenience sampling method. Participants were recruited from public areas such as markets, gardens, and public squares in the regions of Riyadh, Makkah, and the Eastern Province. The inclusion criterion was adults aged 18 years or older. Individuals who had a prior diagnosis of a neurological or psychiatric disorder other than ADHD were excluded. While randomization was not feasible due to the inherent limitations of convenience sampling, efforts were made to enhance sample diversity by recruiting participants from various locations across the three regions and at different times throughout the data collection period.
Data were collected from participants between January 27 and October 8, 2023, after the researchers received ethical approval. Informed consent was obtained from all participants; 196 individuals declined to participate due to lack of time or unwillingness. Following institutional approval, trained research assistants were recruited to administer the ASRS-5-AR to participants through individual self-reporting. The final study sample consisted of 4299 Saudi and non-Saudi adults residing in Saudi Arabia, with an age range of 19 to 66 years (31.16 ± 9.26 years).
Measure
To measure the symptoms of ADHD, the researchers applied the Arabic version of the ASRS-5. Since the ASRS-5 had not been previously used in the local context intended for this study, it underwent a rigorous translation process. A forward translation was conducted by an independent bilingual translator from English into Arabic. Subsequently, a different independent bilingual translator back-translated the Arabic version into English. Following this, the two translators, in conjunction with the current researcher, compared both versions and made necessary modifications to ensure accuracy and cultural appropriateness. The finalized Arabic version was then labeled “ASRS-5-AR.”
The ASRS-5-AR consists of the following six items: “How often do you have difficulty concentrating on what people are saying to you even when they are speaking to you directly? How often do you leave your seat in meetings or other situations in which you are expected to remain seated? How often do you have difficulty unwinding and relaxing when you have time to yourself? When you’re in a conversation, how often do you find yourself finishing the sentences of the people you are talking to before they can finish them themselves? How often do you put things off until the last minute? How often do you depend on others to keep your life in order and attend to details?” The measure uses a 5-point Likert scale (never, rarely, sometimes, often, and very often) with scores ranging from 0 to 24. Ustun et al. applied the ASRS-5 to a sample of 637 participants and showed that the scale has good psychometric properties when used on a general population sample (sensitivity, 91.4%; specificity, 96%) compared with a clinical sample (sensitivity, 91.90%; specificity, 74%).
Statistical Analysis
The demographic characteristics of the study participants were computed in percentages. Means and standard deviations were used for the ASRS-5-AR criteria. The Pearson correlation coefficient was used to verify internal consistency between the six items of the ASRS-5-AR and its total score, and Cronbach’s α and split-half by Spearman-Brown and Guttmann coefficients were used to verify reliability. Structural equation modeling was performed for confirmatory factor analysis (Cheung et al., 2024) to assess the tool’s psychometric properties. We performed the statistical analysis using IBM SPSS Statistics (Version 26) and JASP 0.18.3.0 software.
Results
Participant Sociodemographic Characteristics
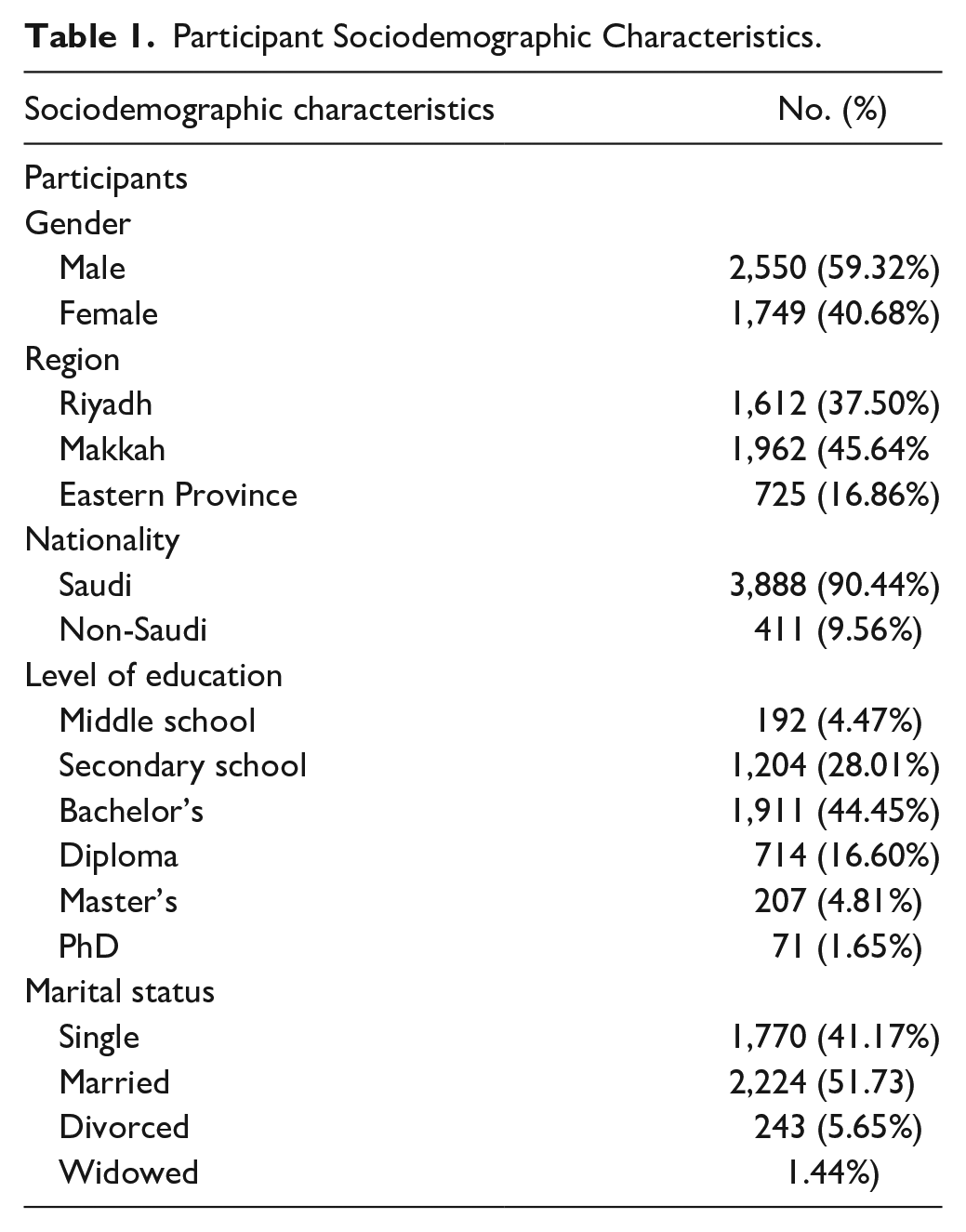
The sample consisted of 4,299 adults (2,550 men and 1,749 women) 19 years old and over residing in Saudi Arabia. Among the sample, 3,888 were of Saudi nationality and 411 were non-Saudi. Also, 1,612 resided in the city of Riyadh, 1,962 in Makkah, and 725 in the Eastern Province. The majority were married (2,224) and educated up to secondary school (1,204) (see Table 1).
Participant Sociodemographic Characteristics.
Internal Consistency of the ASRS-5-AR
The results shown in Table 2 indicate that the ASRS-5-AR has good reliability. All six items showed significant positive correlation with the scale’s total score (correlation coefficient ranged from 0.675 to 0.735). McDonald’s omega, Cronbach’s α, and Spearman-Brown reliability coefficients were all acceptable (0.786, 0.788, and 0.724, respectively).
Correlation of the ASRS-5-AR Items for Adults.
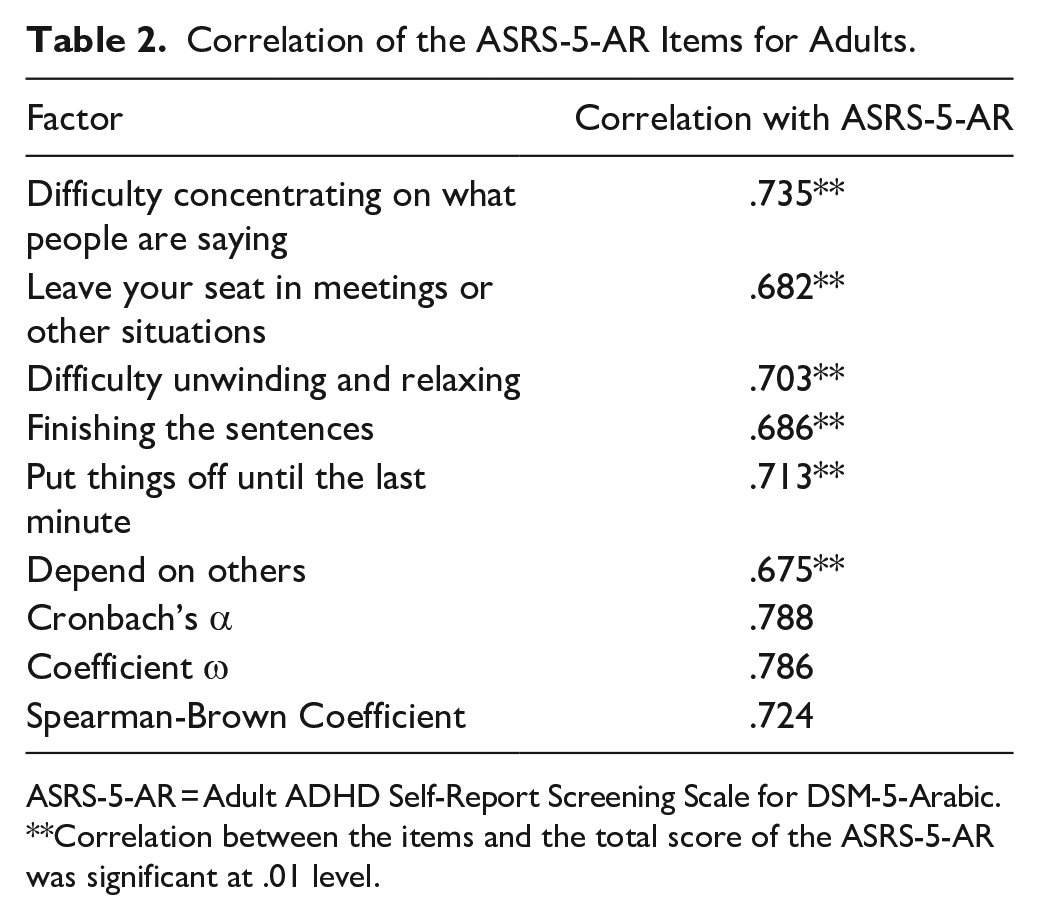
ASRS-5-AR = Adult ADHD Self-Report Screening Scale for DSM-5-Arabic.
Correlation between the items and the total score of the ASRS-5-AR was significant at .01 level.
Confirmatory Factor Analysis
Based on the results of the study conducted by Ballmann et al. (2022), the best fit was achieved for a general factor of the ASRS-5 German version. Also, the results of Somma et al.’s (2021) study showed that the ASRS-5 is a one-factor instrument that is valid and reliable in diagnosing ADHD in Italy. However, in the current results, structural equation modeling was performed to estimate the ASRS-5-AR one-factor standard model validity using JASP 0.18.3.0 software. Results are shown in Tables 3 and 4 and Figure 1.
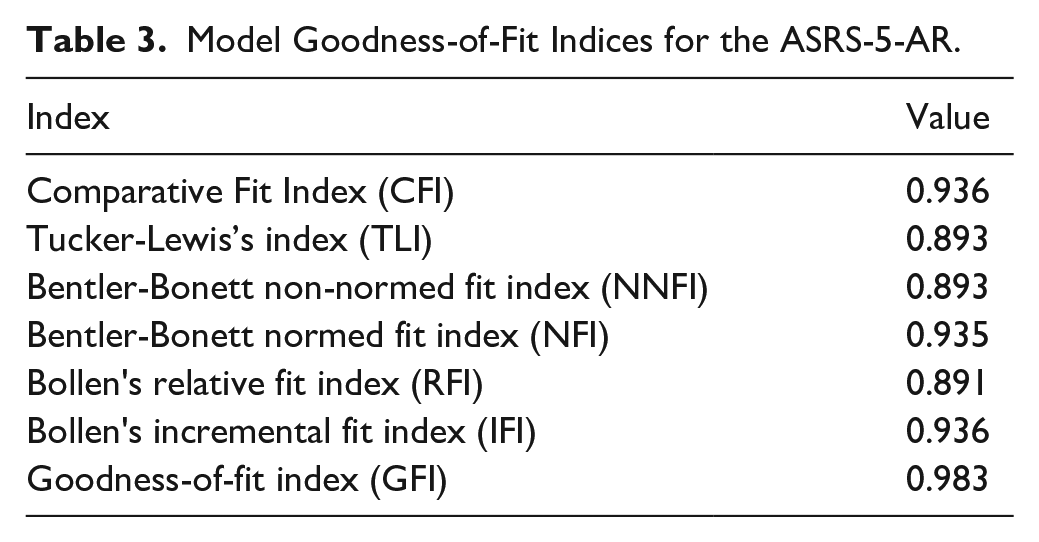
Model Goodness-of-Fit Indices for the ASRS-5-AR.
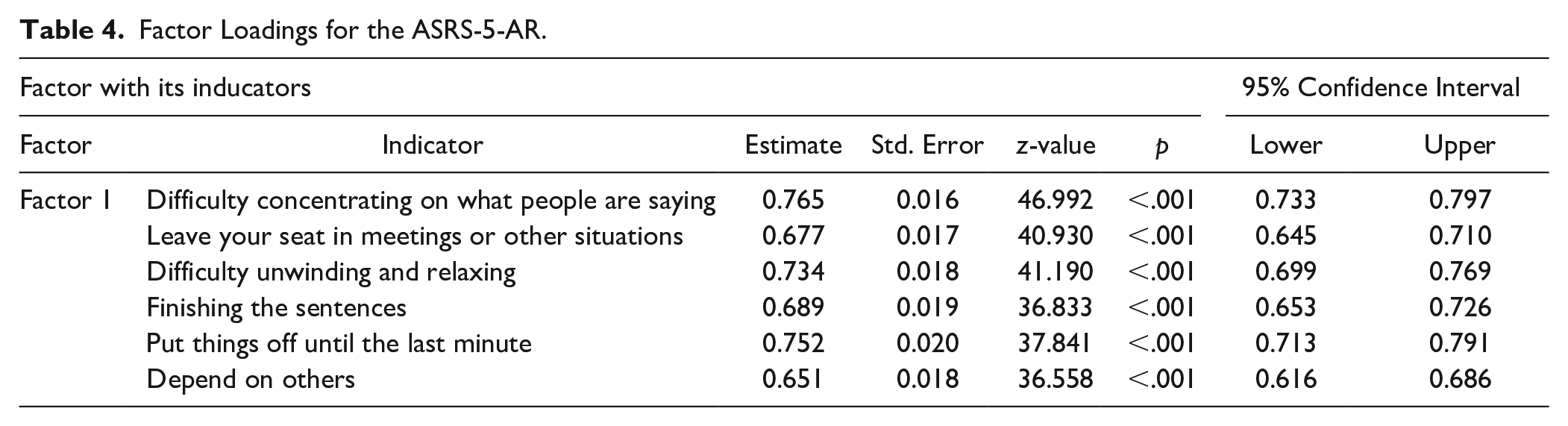
Factor Loadings for the ASRS-5-AR.
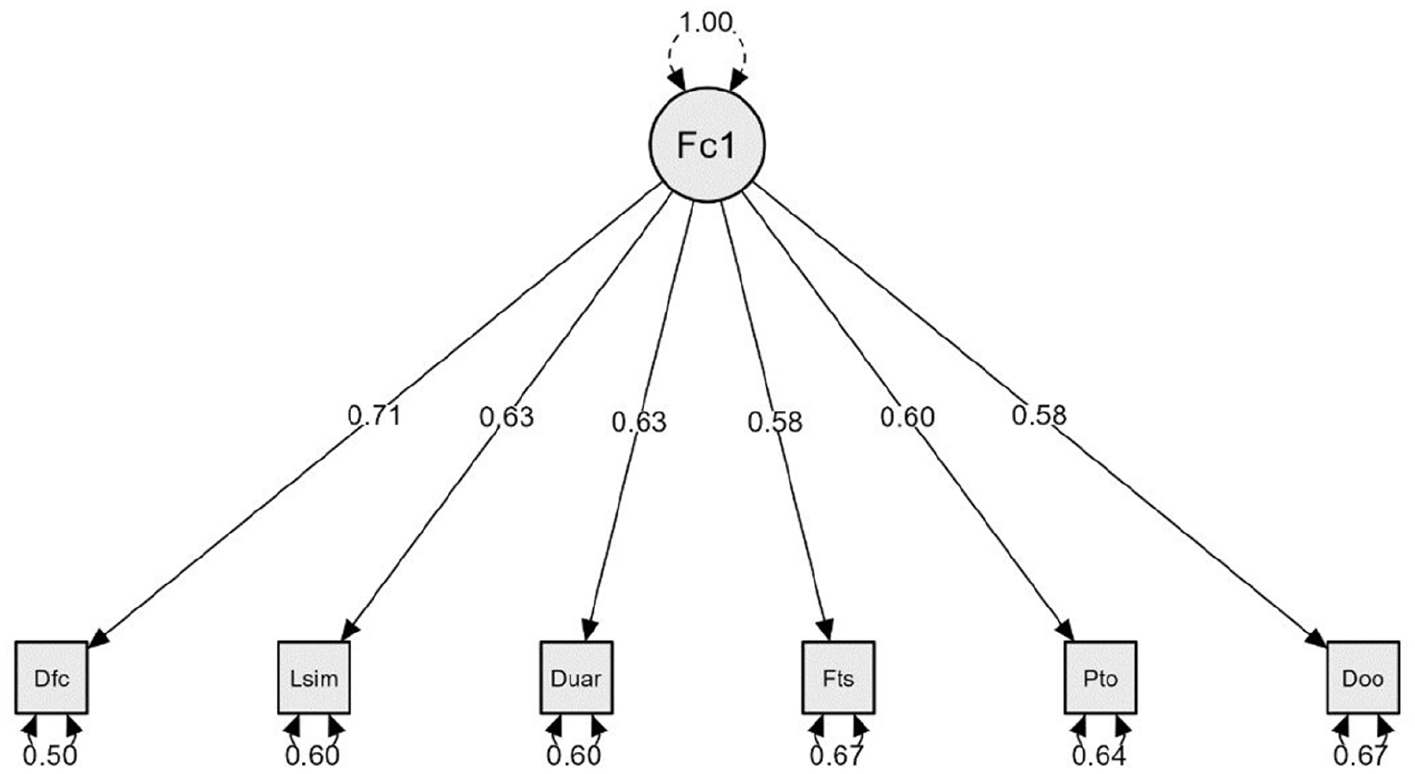
Confirmatory structural equation model for the ASRS-5-AR for adults using JASP 0.18.3.0 software.
As shown in Tables 3 and 4 and Figure 1, the ASRS-5-AR had good goodness-of-fit indices: comparative fit index was 0.936; Tucker-Lewis’s index was 0.893; Bentler-Bonett normed fit index was 0.935; and the goodness-of-fit index was 0.983. All mentioned indices were within an acceptable range, and all paths between the items and the general factor ranged between 0.58 and 0.71, which were significant (p < .001).
Normative Data of the ASRS-5-AR
Normative data were weighted for the participants’ self-assessment of their ADHD symptoms according to gender and age group. Table 5 shows means, standard deviations, and percentiles for participant total scores on the ASRS-5-AR.
Normative Data for the Ratings of Adults on the ASRS-5-AR in Saudi Arabia.
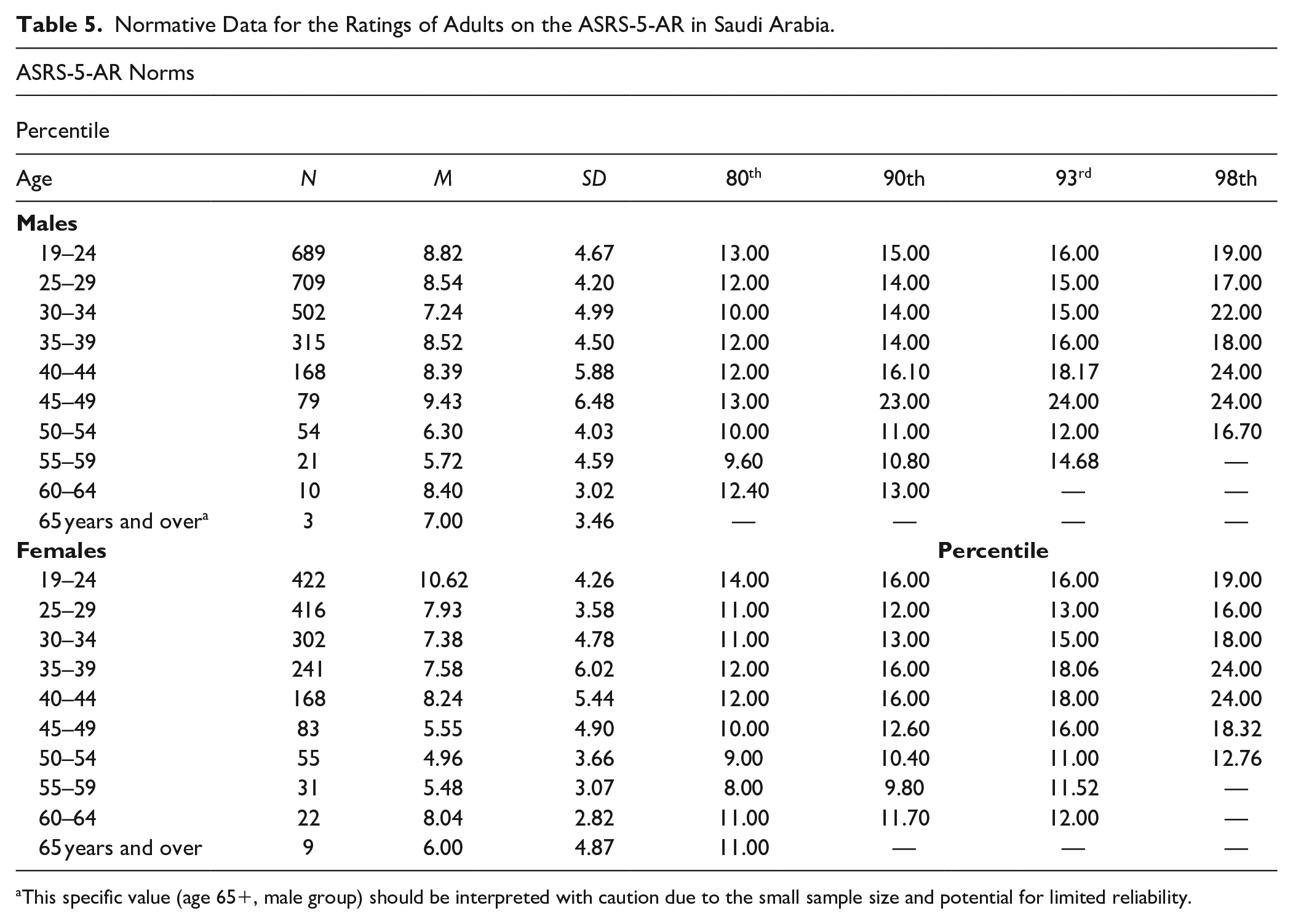
This specific value (age 65+, male group) should be interpreted with caution due to the small sample size and potential for limited reliability.
The results show a variety of scores on the ASRS-AR according to age group and gender (Table 5). For example, in young adult males, 19 to 24 years old (n = 689), 80% scored below 13 on the ASRS-5-AR, while 20% scored over 13. Ninety percent scored below 15, and 10% scored over 15, and so on. In the sample of females of the same age group (n = 422), 80% scored below 14, while 20% scored over 14. Also in this group, 98% obtained scores below 19 on the scale, while only 2% obtained a scores above 19, and so on. If we look at males 60 to 64 years old (n = 10), 90% scored below 13, while 10% scored over 13 on the scale. In females of the same age group (n = 22), 90% scored below 11.70, while 10% obtained scores over 11.70. None of the males 65 years and older (n = 3) obtained a score on the ASRS-5-AR. However, for the females of the same age group (n = 9), 80% obtained scores below 11, and 20% scored over 11.
Differences in ADHD Screening According to Sociodemographic Characteristics
We used t-tests and ANOVA to detect differences based on gender, nationality, age group, residential region, marital status, and level of education. The results are shown in Tables 6 and 7.
Differences Between Males and Females in ASRS-5-AR Results.

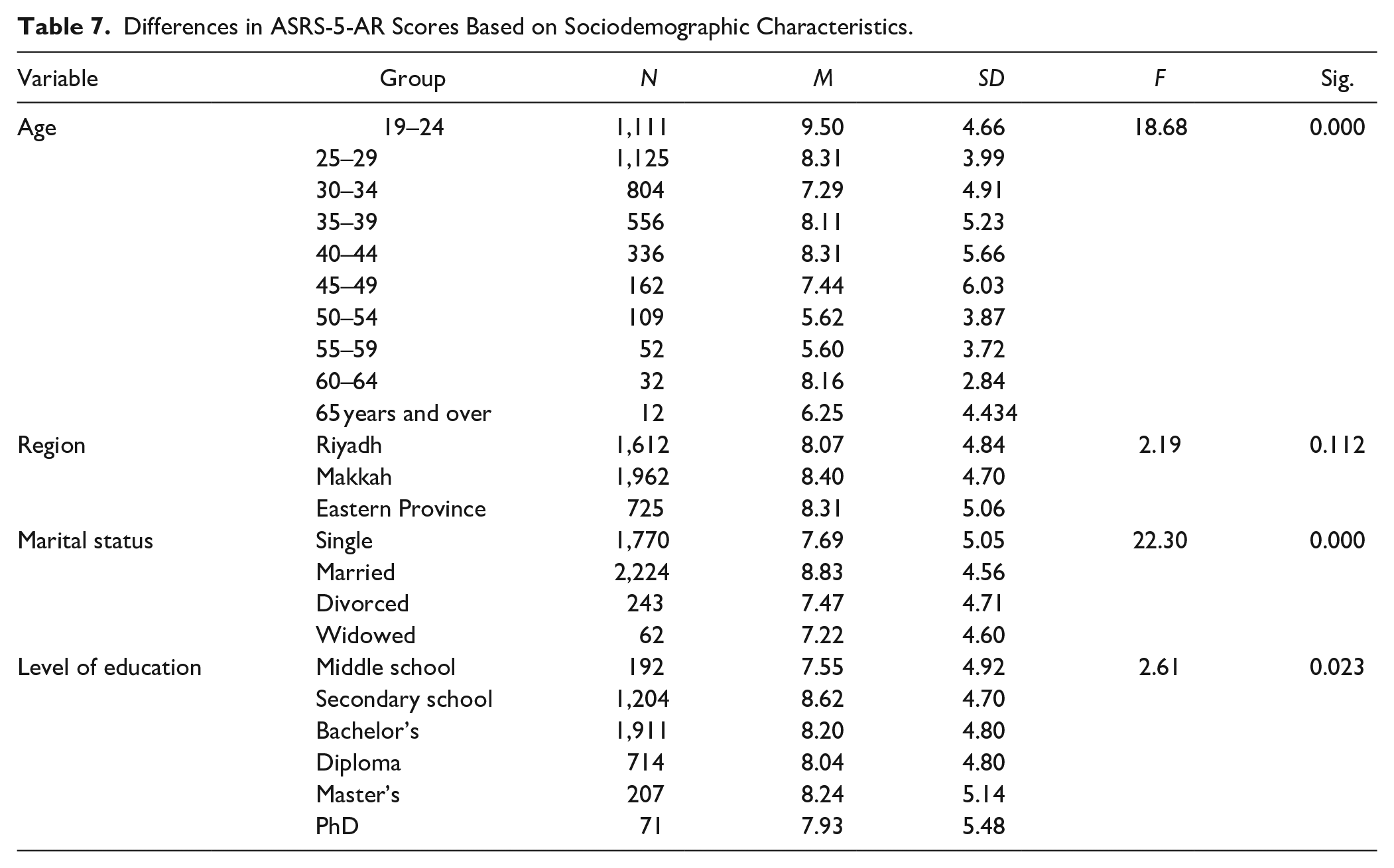
Differences in ASRS-5-AR Scores Based on Sociodemographic Characteristics.
There were no significant statistical differences in ASRS-5-AR scores between males (8.30 ± 4.79) and females (8.21 ± 4.84) (t = 0.625; p value = .532 > .05) or Saudi (8.273 ± 4.754) and non-Saudi (8.161 ± 5.355) participants (t = 0.409; p value = .682 > .05).
As shown in Table 7, total scores differed significantly based on age group (sum of squares between groups = 3,757.074, within groups = 95,846.954, total = 99,604.028; F = 18.68; p value = .000 < 0.001), marital status (sum of squares between groups = 1,527.798, within groups = 98,076.230, total = 99,604.028; F = 22.30; p value = .000 < .001), and level of education (sum of squares between groups = 302.104, within groups = 99,301.924, total = 99,604.028; F = 2.61, p value = .023 < .05). However, total scores showed no significant differences based on region of residence (sum of squares between groups = 101.586, within groups = 99,502.442, total = 99,604.028; F = 2.19; p value = .112 > .001).
We employed Tukey’s test to determine the direction of the differences in scores within the age, marital status, and level of education subgroups. The results revealed that adults aged 19 to 24 years had significantly higher mean scores compared with the other age groups (means of differences = 1.1867, 2.206, 1.386, 1.187, 2.055, 3.876, and 3.903); all of the mean differences were significant (p value = .000 < 0.05) using the harmonic mean sample size (63.707) (Figure 2). Also, individuals who were widowed had significantly higher mean ASRS-5-AR scores compared with those who were married, single, divorced, or separated (mean differences = 1.145, 1.365, 1.608; p value = .000 < .05) (Figure 3). Adults with a secondary school educational level had significantly higher mean ASRS-5-AR scores (mean difference = 1.07; p value = .048) compared with those with a middle school level of education, using the harmonic mean sample size (223.229) (Figure 4)
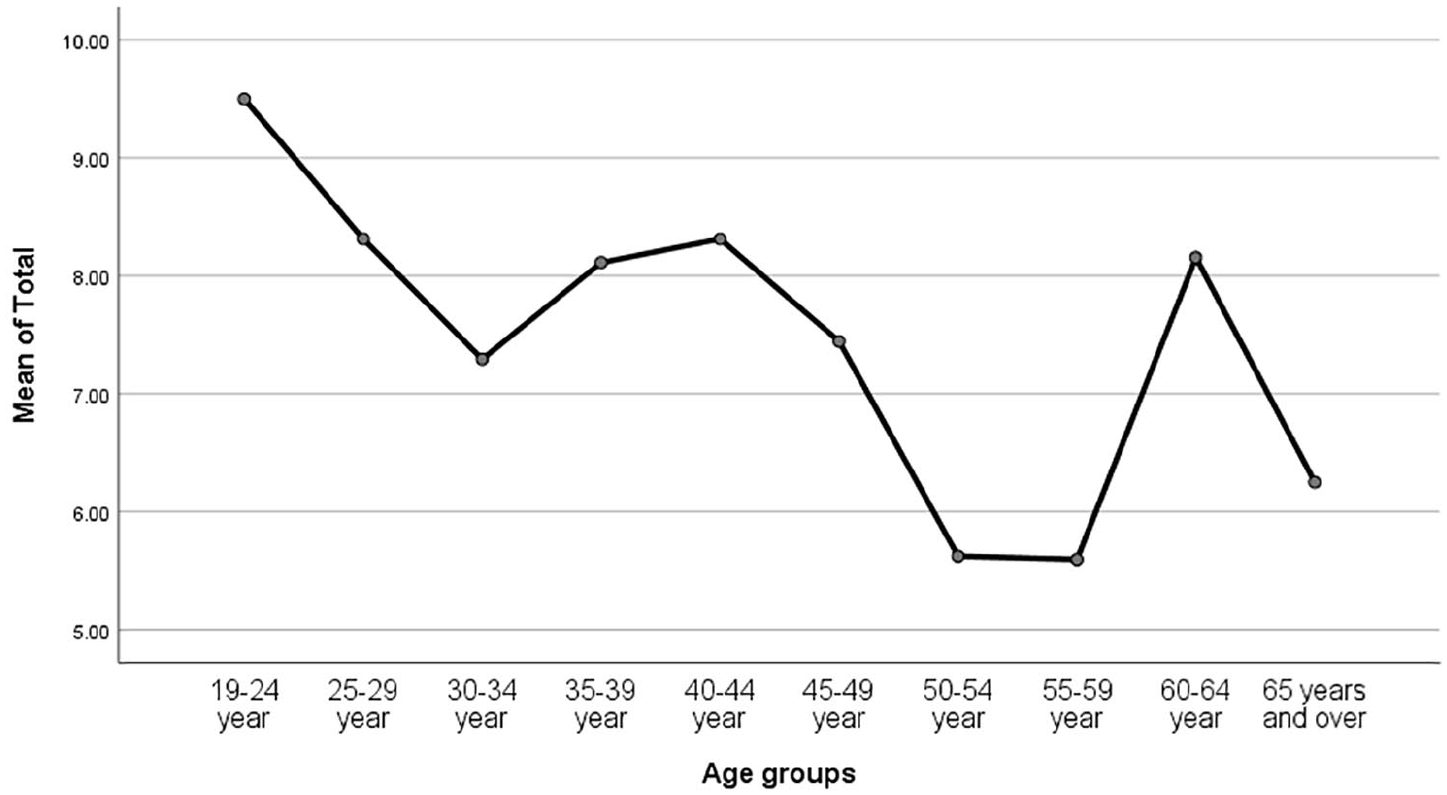
Means plot for different age groups.
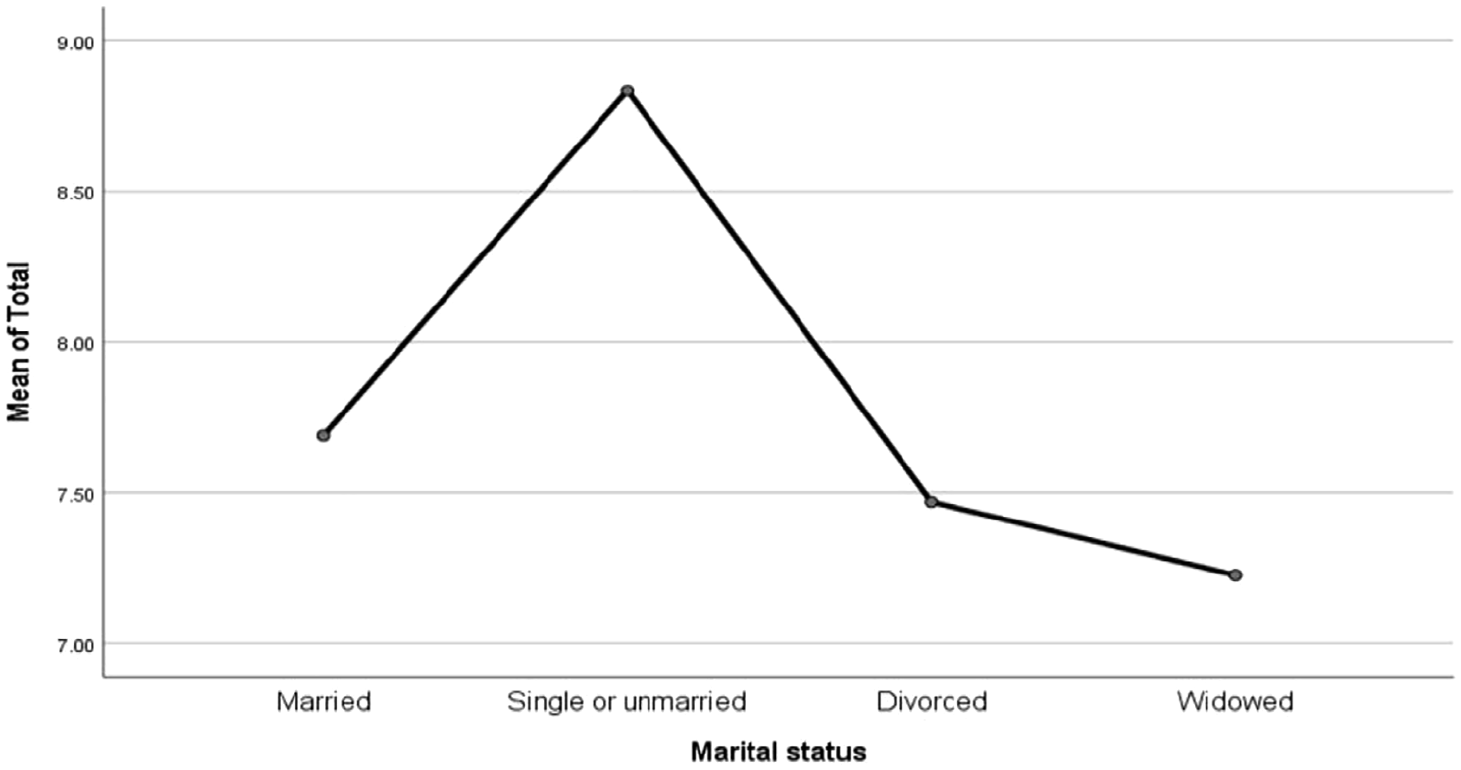
Means plot of different marital-status groups.
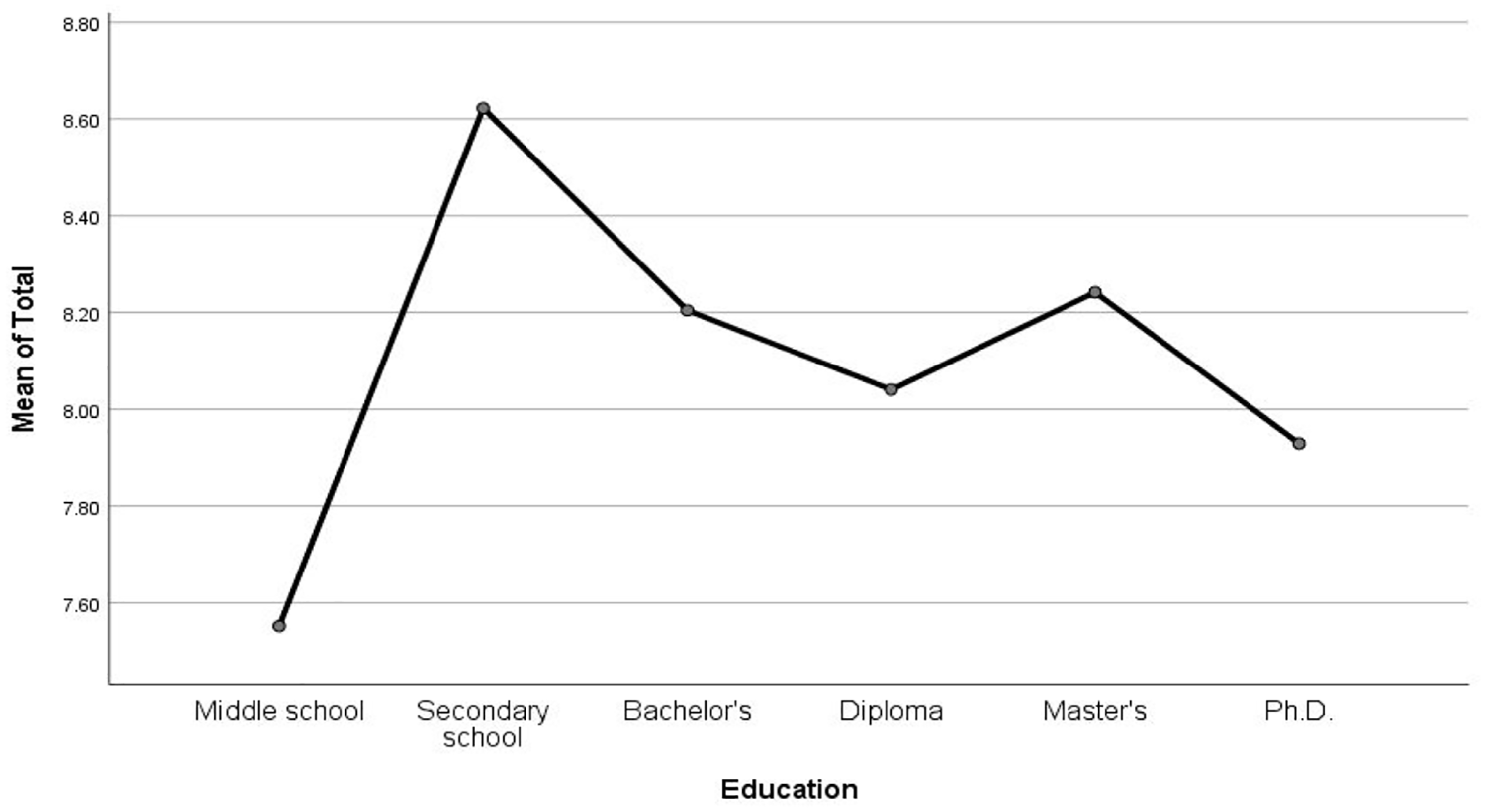
Means plot of different level-of-education groups.
Discussion
This study aimed to verify the psychometric properties of the ASRS-5 among adults in the Saudi environment, extract normative data for future screening purposes, and examine the association between ASRS-5 score and several demographic variables in a large sample of adults from the general population. It is important to note that this study did not involve a clinical sample and, therefore, does not provide a basis for ADHD screening or diagnosis. While the present study provides preliminary normative data on ADHD symptoms in the Saudi Arabian population, it is important to acknowledge that some unexpected trends in ASRS-5-AR scores were observed across age groups. These variations may be attributed to several factors, including the sample variability inherent in the convenience sampling method, the potential influence of unmeasured confounding factors such as socioeconomic status, occupation, and lifestyle, and the potential impact of age-related life events and transitions on ADHD symptom presentation. Further research with larger and more representative samples is warranted to investigate these observed trends and explore the underlying factors contributing to the observed variability in ADHD symptoms.
In the current study, the ASRS-5-AR showed good internal consistency indicators, as its six items exhibited significant positive correlation with the scale’s total score (ranging from .675 to .735). The scale also exhibited good psychometric indicators, based on structural equation modeling, that matched the empirical data collected from the participants. The standard model’s goodness-of-fit coefficient was .95, indicating a good fit. The scale also showed good reliability indicators when applied to adults (ω coefficient = .786; Cronbach’s α = .788; and Spearman-Brown coefficient = .724).
This study also examined normative data collected from the large sample of adults, results of which revealed variable performance on the ASRS-5 related to age group. After comparing these results with total scores from previous studies in the literature, we can state that a total score of 12 or 13, as reported in the literature, would result in a positive screening for approximately 20% of Saudi adults (those scores fall approximately under the 80th percentile for most subgroups in Table 5). Thus, the higher total scores might result in fewer cases being identified, which might not be preferable given the clinician’s goals and the balance between the actual prevalence of ADHD in adults and the risk of missing actual cases.
However, these results on ASRS-5 norms in a general population sample are still uncertain due to the lack of clinical evidence. We recommend conducting a future study for precise determination of the cutoff score by comparing population and clinical samples. As Harrison and Edwards (2023) concluded in their meta-study, the diagnosis of ADHD cannot be based solely on such measures, but rather more rigorous evaluation must be conducted for people who screen positive for ADHD. Similarly, cutoff scores for diagnosing ADHD through measurement scales cannot be decisive, as Sonnby et al. (2014) concluded in their study.
In addition, we cannot be certain that the appearance of ADHD symptoms in the general population is caused by the disorder, because most adults occasionally have problems with inattention, impulsivity, distractibility, and insomnia; nonetheless, ADHD often manifests as problems related to executive function that can lead to many difficulties in managing daily life. Further, ADHD symptoms are not unique to ADHD alone, but are indeed part of most other disorders (e.g., concentration problems and restlessness in anxiety or concentration problems and psychomotor agitation observable to others in depression). To put it differently, ADHD is a disorder that does not have any unique symptoms.
Interestingly, the current study detected no statistically significant differences between males and females in total score on the ASRS-5-AR (t = 0.625; p > .05), contrary to results reported by previous studies. Lutfi (2022) found differences in ADHD in favor of males. Yáñez-Téllez et al. (2021) reported that ADHD was more prevalent among males (22.14%) than females (13%). In the more recent meta-analysis by Al-Wardat et al. (2024), the prevalence was also higher in males (11.10% vs. 7%). Al-Masry (2012) and Al-Shahrani (2019), however, found the disorder to be more prevalent among females. These conflicting results may be due to different assessment tools used for screening. We also found no statistically significant differences in ASRS-5-AR total score between Saudi and non-Saudi adults (t = 0.409; p > .05), which may be explained by the fact that all of the participants were residents of Saudi Arabia, and they and their families received the same health services and social support.
However, total score showed statistically significant differences based on age (F = 18.68; p < .001), educational level (F = 2.61; p < .05), and marital status (F = 22.30; p < .001). Other studies have found ADHD to be more prevalent in younger adults. ADHD usually appears at an early age and may continue to advanced stages, causing significant deficiency in academic, social, and occupational performance (Bálint et al., 2009; Canu et al., 2020; Klassen et al., 2010; Kwon et al., 2018; Lutfi, 2022; Sobanski et al., 2007). On the other hand, a meta-analysis by Ramos-Quiroga et al. (2013) reported that older adults were more likely to report ADHD symptoms than younger adults. According to Ayano et al. (2023) ADHD prevalence is high among adults, at 3.10%. Widowed adults scored higher for distress, as a result of difficult living conditions and, perhaps, experiencing a lack of attention and support.
Region of residence did not show a significant association with total score (t = 2.19; p > .05), as is consistent with Lutfi’s (2022) findings. However, in some reports, adults in lower economic environments scored higher for ADHD symptoms than those in higher economic environments (Russell et al., 2016; Zwirs et al., 2007). The Kingdom of Saudi Arabia cares for its citizens of all ages and in all regions of the country and provides them with health and social services (Saudi Vision 2030, 2016).
Conclusion
The findings demonstrate that the Arabic version of the ASRS-5 has strong psychometric properties, with good indicators of internal consistency and reliability, making it a suitable tool for assessing ADHD symptoms in Arabic-speaking populations. It is important to note that this study did not involve a clinical sample and, therefore, does not provide a basis for ADHD screening or diagnosis. Future research should investigate the clinical utility of the ASRS-5-AR in a clinical setting to establish its validity and reliability for the diagnosis of ADHD in the Saudi population.
Study Strengths and Limitations
This study has several strengths, including the large and diverse sample of adults residing in various regions of the country, which provides valuable insights into the characteristics of the ASRS-5 within this population. Also, the inclusion of a broad demographic spectrum enhances the generalizability of the findings to a significant portion of the adult Saudi population.
However, this study has limitations. As a descriptive, cross-sectional survey, it cannot establish causal relationships or draw final conclusions about the prevalence of ADHD in the Saudi population. The absence of clinical assessments prevents the determination of accurate cutoff scores for the ASRS-5 and limits its use for screening or diagnosing ADHD in this context. Future research should include clinical evaluations to establish more precise cutoff scores and investigate the prevalence of ADHD using a combination of assessment methods.
Footnotes
Acknowledgements
The authors would like to thank all participants and parents for their interest and willingness to contribute to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Saudi ADHD Society (Project number 03). The funders had roles in the study’s design, data collection, analysis, the decision to publish, and preparation of the manuscript.
Compliance with Ethical Standards
The Research Ethics Committee at the Saudi ADHD Society approved this study (Approval no.23-06). All methods were carried out following relevant guidelines and regulations, and informed consent was obtained from all participants.
Ethics
The Saudi ADHD Society Ethics Review Committee approved our study (approval: IRB-06-23) on July 10, 2023. Respondents gave written consent for review and signature before starting the survey.
ORCID iDs
Availability of Data and Materials
All data are fully available upon reasonable request.