
Abstract
Objective:
To evaluate care transition and medication use in young adults with ADHD in Sweden.
Method:
Observational retrospective study of patients with ADHD from the Swedish National Patient Register, Prescribed Drug Register, and Cause of Death Register (2018–2020). Last contact with pediatric psychiatric care, first contact with adult psychiatric care, and medication use were described for ages 18 to 21 years, inclusive.
Results:
Of 19,233 patients who had dispensed ADHD treatment, 85.8% had received adult psychiatric care by 21 years of age. The proportion of patients on medication was highest at age 18 years (80.1%), decreasing to 36.1% by age 21 years. By 21 years, there were significantly more patients on versus off ADHD medication who had received healthcare for autism, been prescribed selective serotonin re-uptake inhibitors, and received adult psychiatric outpatient visits (all p < .0001).
Conclusion:
This study demonstrates declining ADHD medication use during the pediatric-to-adult care transition for patients in Sweden.
Introduction
ADHD is a common neurodevelopmental disorder that affects approximately 6% of children and adolescents and 2.8% of adults worldwide (Faraone et al., 2021). A recent observational retrospective study of patients from the Swedish National Patient Register (NPR) and Prescribed Drug Register (PDR) reported that the 2020 prevalence of ADHD among children and adolescents in Sweden was 3.2% and 1.4% in adults (Giacobini et al., 2023). A multimodal approach is recommended for the treatment of patients with ADHD. Alongside pharmacotherapy, psychoeducation, cognitive behavior therapy, and coaching are recommended (Kooij et al., 2019). Pharmacological treatments include psychostimulants and non-psychostimulants. A systematic review into the efficacy and tolerability of ADHD medications found that methylphenidate (for children and adolescents) and amphetamines (for adults), were the preferred first-choice medications prescribed to treat ADHD (Cortese et al., 2018; Giacobini et al., 2023). The consumption of medications for ADHD has increased substantially over the past few years, possibly as a result of increased awareness of mental health issues, changes in diagnostic criteria, and other social influences (Gimbach et al., 2024). Therefore, there is an increasing demand for psychiatric healthcare services to meet the needs of patients with ADHD.
ADHD has long been considered a disorder of childhood, with symptoms declining as patients get older (Song et al., 2021); however, it is now recognized that symptoms persist into adulthood in ~65% of cases (Faraone et al., 2006). Predictors for this persistence over time may include severity of symptoms, psychosocial adversity, and psychiatric co-morbidities (Biederman et al., 2011). As around two thirds of children with ADHD will go on to display symptoms as adults, patient care inevitably needs to transition from pediatric to adult psychiatric services (Kooij et al., 2019). Patients with ADHD are among those least likely to transition successfully from pediatric to adult mental health services, which can affect the patient’s overall outcome (Kooij et al., 2019; Price et al., 2022). A patient’s first referral from child and adolescent mental health services to adult mental health services is understood to be a key time point when patients are lost to follow-up (Janssens et al., 2020). The reasons for this are complex, but could be because: (1) in many countries, after age 18 years, medical services and medications cease to be heavily subsidized or free of charge; (2) the patients themselves, rather than their parents, are expected to keep track of their medical care; (3) after finishing school, patients may relocate from the place of their original clinic for work or to pursue higher education; and (4) patients who finish school but do not go on to higher education may feel that they no longer need to medicate their ADHD.
Because of its historical classification as a childhood condition, many adult mental health services are not equipped to support older patients with ADHD effectively (Janssens et al., 2020). For many chronic conditions, including asthma (Withers & Green 2019), epilepsy (Geerlings et al., 2015), diabetes (Buschur et al., 2017), congenital heart disease (Sable et al., 2011), and cystic fibrosis (Al-Yateem 2013), protocols and guidance are available on how to facilitate the transition of care from pediatric to adult services. The same is true for ADHD (Nutt et al., 2007; Young et al., 2016); however, prescription data reveal a substantial drop in medication use in patients between the ages of 15 and 21 years that is not matched by a decrease in reported symptoms (McCarthy et al., 2009). Data from a multinational population-based study has shown that treatment discontinuation in patients with ADHD is highest in those aged 18 to 19 years (Brikell et al., 2024).
Over the past 15 years, there has been an apparent increase in ADHD diagnoses among children in Sweden (Giacobini et al., 2023; Polyzoi et al., 2018). However, whether this reflects a true increase in the global prevalence of ADHD over time is unclear. It has been suggested that variability in pre-valence rates could be explained by the heterogeneous diagnostic practices used across studies (Polanczyk et al., 2014). Nonetheless, the high prevalence of ADHD in children warrants further investigation into the continuity of care provided to these patients, as well as the extent to which their ADHD is managed as they transition into adulthood. The objectives of this study were to describe patterns in care transition and prescription medication use in patients aged 18 to 21 years who were prescribed ADHD medications (between 2018 and 2020), using real-world data from health registries in Sweden.
Methods
Data Sources
This retrospective population-based study used real-world data obtained from the NPR, PDR, and Cause of Death Register. The NPR collects information on inpatient and outpatient care, including patient characteristics, dates of visits, diagnoses, co-morbidities, primary discharge diagnosis, and secondary diagnoses provided by specialist care physicians. The PDR provides information on all medicines prescribed in Sweden since July 2005, including by general practitioners (Wallerstedt et al., 2016). This study and waiver of patient consent were approved by the Swedish Ethical Review Agency and the Stockholm Regional Ethical Review Committee (references 2012/1315-31, 2013/2177-32, 2017/1395-32, 2018/1678-32, 2018/1835-32, 2020-06376, 2022-06622-02, and 2023-0700402).
Study Design
Patients were included if they were aged 18 to 21 years between 2018 and 2020, and were dispensed ADHD medication (amphetamine, dexamphetamine, lisdexamphetamine, methylphenidate, atomoxetine, or guanfacine) within 180 days before their 18th birthday as identified in the PDR using Anatomical Therapeutic Chemical codes: N06BA01, N06BA02, N06BA04, N06BA09, N06BA12, and C02AC02. Patients were followed from the latest date of January 1, 2018, or their 18th birthday, until death, emigration, or until December 31, 2020. Stockpiling of medications was accounted for assuming one Daily Defined Dose was consumed every day. Last contact with pediatric psychiatric care was defined as either the last day of prescription coverage, as registered in the PDR (calculated as the last dispensation from pediatric care, taking into account stockpiling), or the last visit (discharge date from inpatient or outpatient visit) to pediatric psychiatry services, as registered in the NPR, whichever was latest. First contact with adult psychiatric care was defined as either the first visit (inpatient or outpatient) at an adult psychiatric care unit as registered in NPR, or the first dispensation from a prescription by an adult psychiatric care unit as registered in PDR; whichever was earliest. In the event of pediatric prescription coverage overlapping with the first adult psychiatric visit/prescription, or pediatric visits occurring after first contact with adult psychiatric services, the date of last contact with pediatric care has been defined as the same day as the first contact with adult psychiatric care. Conversely, patients who had not had contact with adult psychiatric care, but whose last contact was with pediatric psychiatric care, were classified as “other or no care”.
Patients were classified to be taking ADHD medication (“on medication”) or no longer taking ADHD medication (“off medication”). “On medication” was defined as those patients who had been dispensed medication and had sufficient doses for that day, accounting for stockpiling. “Off medication” was defined as those patients who did not have medication for that day, accounting for stockpiling. This could mean that patients were temporarily non-adherent or had discontinued medication altogether. As a sensitivity analysis, a grace period was introduced for being considered on medication with 30, 60, and 90 days since last day with medication coverage.
Clinics were categorized as providing adult or pediatric care based on their medical activity (MVO) codes. An MVO code is assigned to each record in the NPR and PDR and indicates the type of clinic, or healthcare center that provided the medical care. MVO codes were used to determine pediatric psychiatry contacts (931, 201, 251, and 024) and adult psychiatry contacts (901, 944, and 991). Data were also stratified by sex and by region (Stockholm, Uppsala, Östergötland, Skåne, Halland, Västra Götaland, and Gävleborg; Supplemental Appendix).
Statistical Analysis
The Proportion of Patients Covered (PPC) was calculated for each day of follow-up with patient age (18–21 years) as the time axis. In this way, patients could enter and exit the study throughout the follow-up. The PPC was calculated as follows:
Statistical analyses were conducted using SAS version 9.4. Descriptive statistics were used to summarize data on the type of care and medication use, and stratified by age. p-Values were calculated using Pearson’s chi-squared test (categorical variables) and two-tailed Mann-Whitney U test (continuous variables).
Results
Study Population
A total of 19,233 patients were included in the analysis (Table 1). The majority of patients were male (57.1%), and 64.3% were aged 18 years at study entry. Patient’s birth month was evenly split across the year. The median follow-up period was 2.5 (interquartile range [IQR] = 1.9–3.1) person-years. The median age at last contact with pediatric psychiatric care was 18.1 (IQR = 17.8–18.4) years; the median age at first contact with adult psychiatric care was 18.3 years (IQR = 18.1–18.8).
Patient Characteristics.
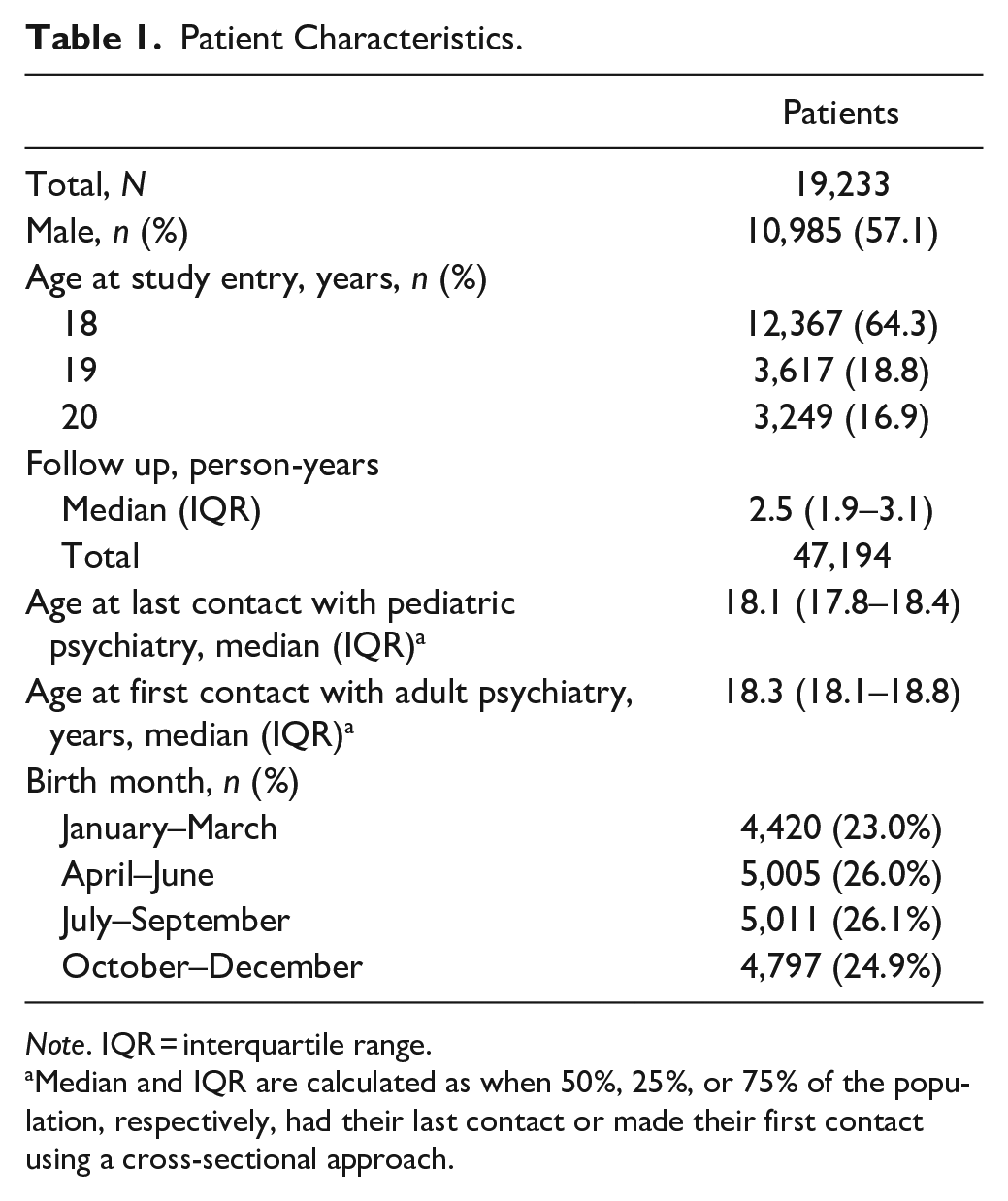
Note. IQR = interquartile range.
Median and IQR are calculated as when 50%, 25%, or 75% of the population, respectively, had their last contact or made their first contact using a cross-sectional approach.
Care Provision for Patients Prescribed ADHD Medications from Age 18 to 21 Years
At age 18 years, 17.1% of patients were classified as being under adult psychiatric care, which increased to 85.8% by 21 years. There was a corresponding decrease in the proportion of patients classified as being under pediatric care services, from 70.8% at age 18 years to 1.0% at age 21 years (Figure 1). Overall, there was a relatively stable proportion of patients classified as receiving undefined or no care after age 18 years through to age 21 years. Data on care provision by region of Sweden are provided in the Supplemental Appendix (Figure S1).
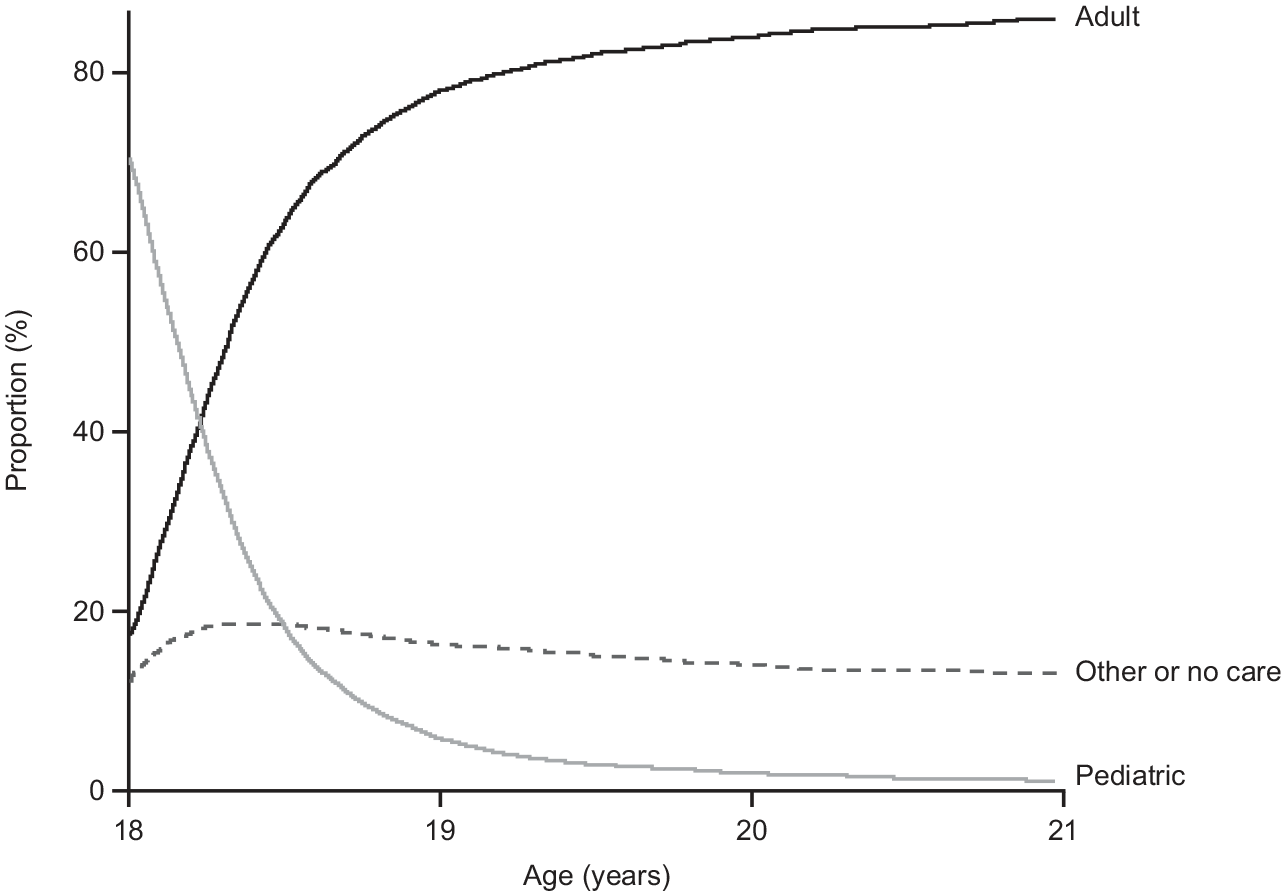
Proportion of patients on ADHD treatment who were receiving adult, pediatric, or undefined care from age 18 to 21 years.
ADHD Medication Use
The overall proportion of patients on medication during the study period was highest among those aged 18 years (80.1%), decreasing to 51.5% at 19 years, 41.9% at 20 years, and 36.1% at 21 years (Figure 2a). By age 21 years, 51.6% of patients had been in contact with adult psychiatric services and were off medication (Figure 2b). There was little difference in the proportions of patients receiving ADHD medication as part of adult and pediatric care when data were stratified by sex (Supplemental Appendix). Sensitivity analysis confirmed a similar proportion of patients not receiving ADHD medication, even when allowing for a 30–90-day grace period for the last day with medication coverage, converging at 21 years of age (Figure 3). Data on ADHD medication use by region in Sweden are provided in the Supplemental Appendix (Figure S2).
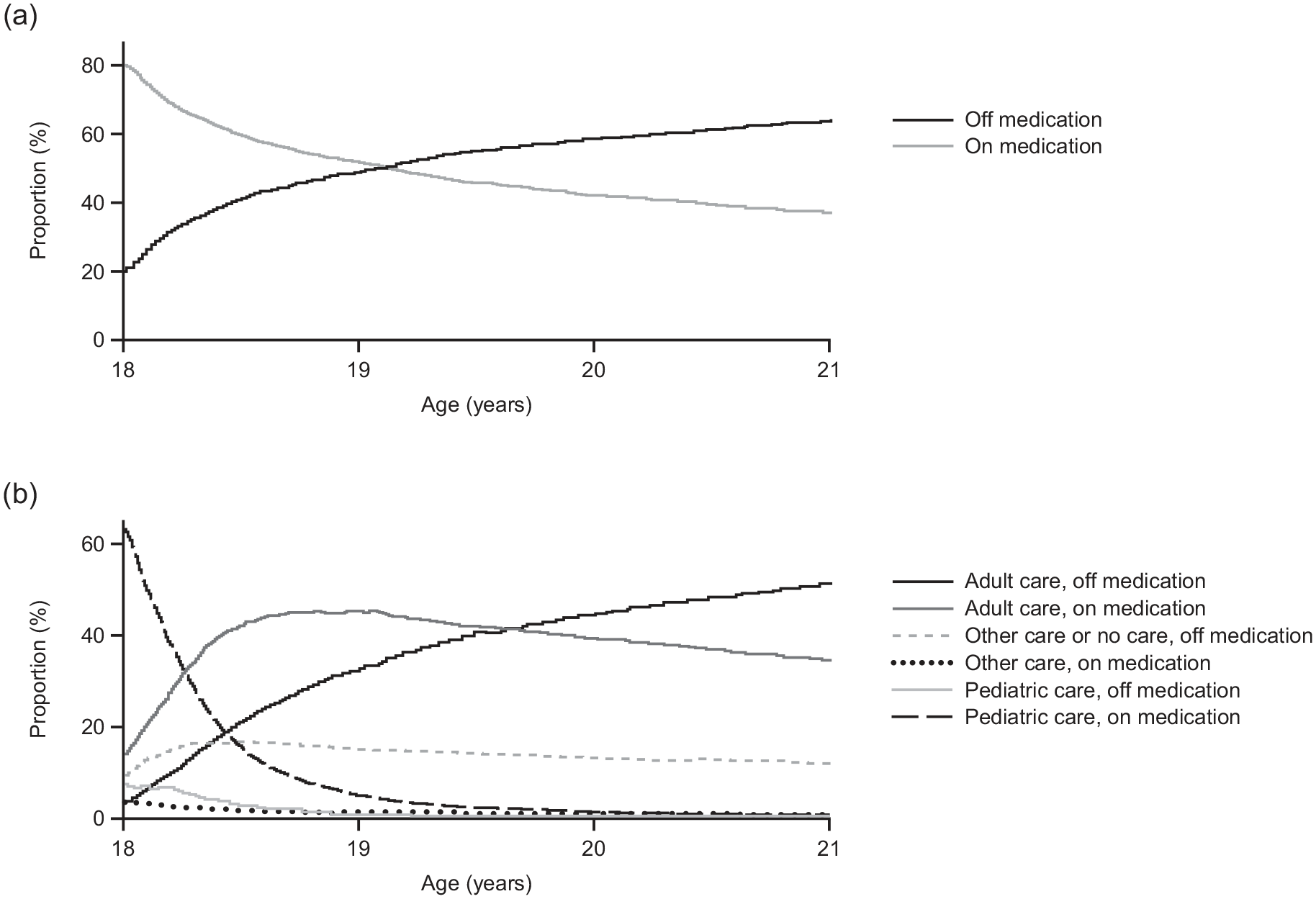
Use of ADHD medication in patients from age 18 to 21 years. (a) Proportion of all patients on and off ADHD medication. “On medication” was defined as patients who had been dispensed medication and had enough medication for that day based on the daily defined dose. “Off medication” was defined as those patients who did not have medication for that day, accounting for stockpiling. This could mean that patients were temporarily non-adherent or discontinued medication altogether. (b) Proportion of patients on and off ADHD medication stratified by adult, pediatric, and undefined care.
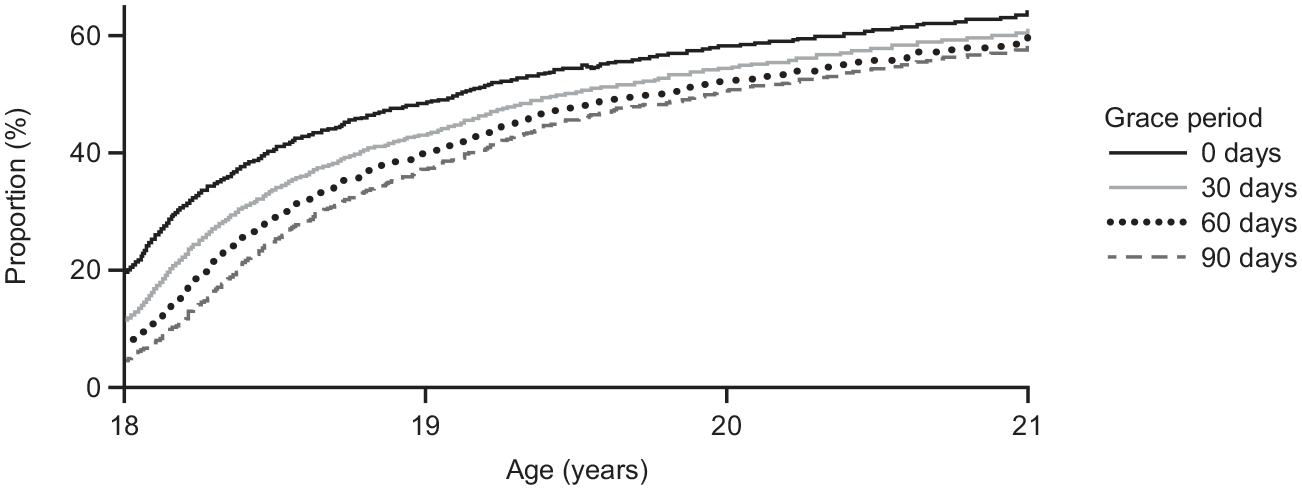
Sensitivity analysis for the proportion of patients off ADHD medication.
Psychiatric Care in Patients at Age 21 Years
Overall, 4,451 (63.9%) patients were off medication and 2,518 (36.1%) were on medication on their 21st birthday (n = 6,969). There was a significantly higher proportion of patients who were on medication and who had had at least one contact with healthcare services with a co-morbid autism diagnosis versus those who were off medication (21.4% and 12.2%, respectively; p < .0001; Table 2). A significantly lower proportion of patients on medication had received healthcare services for co-morbid substance use disorder versus those who were off medication (5.0% and 8.4%, respectively; p < .0001). Among patients aged 21 years, a higher proportion of females than males had received at least one dispensation of selective serotonin reuptake inhibitors (SSRIs) during the study period (females, 39.4%; males, 18.0%). On-medication patients were significantly more likely to have received at least one prescription for SSRIs than those off medication (32.0% and 24.3%, respectively; p < .0001). There was a significantly higher number of annual specialized outpatient visits among patients on medication (mean visits = 2.7 [standard deviation (SD) = 2.6]) versus those off medication (mean visits = 2.4 [SD = 2.9]) at age 21 years (p < .0001). There was also a significantly higher number of annual adult outpatient psychiatry visits in patients on medication compared with those off medication at age 21 years (mean visits = 1.52 [SD = 1.61] vs. 1.10 [SD = 1.65]; p < .0001), whereas there was no difference in the number of annual adult inpatient psychiatry visits between patients on and off medication. Off-medication patients had significantly more inpatient and outpatient visits registered with a substance use disorder (SUD) diagnosis (mean inpatient visits = 0.04 [SD = 0.29] and outpatient visits = 0.09 [SD = 0.49], respectively) than those who were on medication (0.02 [SD = 0.17] and 0.04 [SD = 0.32], respectively; p < .0001 for both inpatient and outpatient visits; Table 2).
Concomitant Psychiatric Care in Patients Who were On or Off Medication at Age 21 Years.
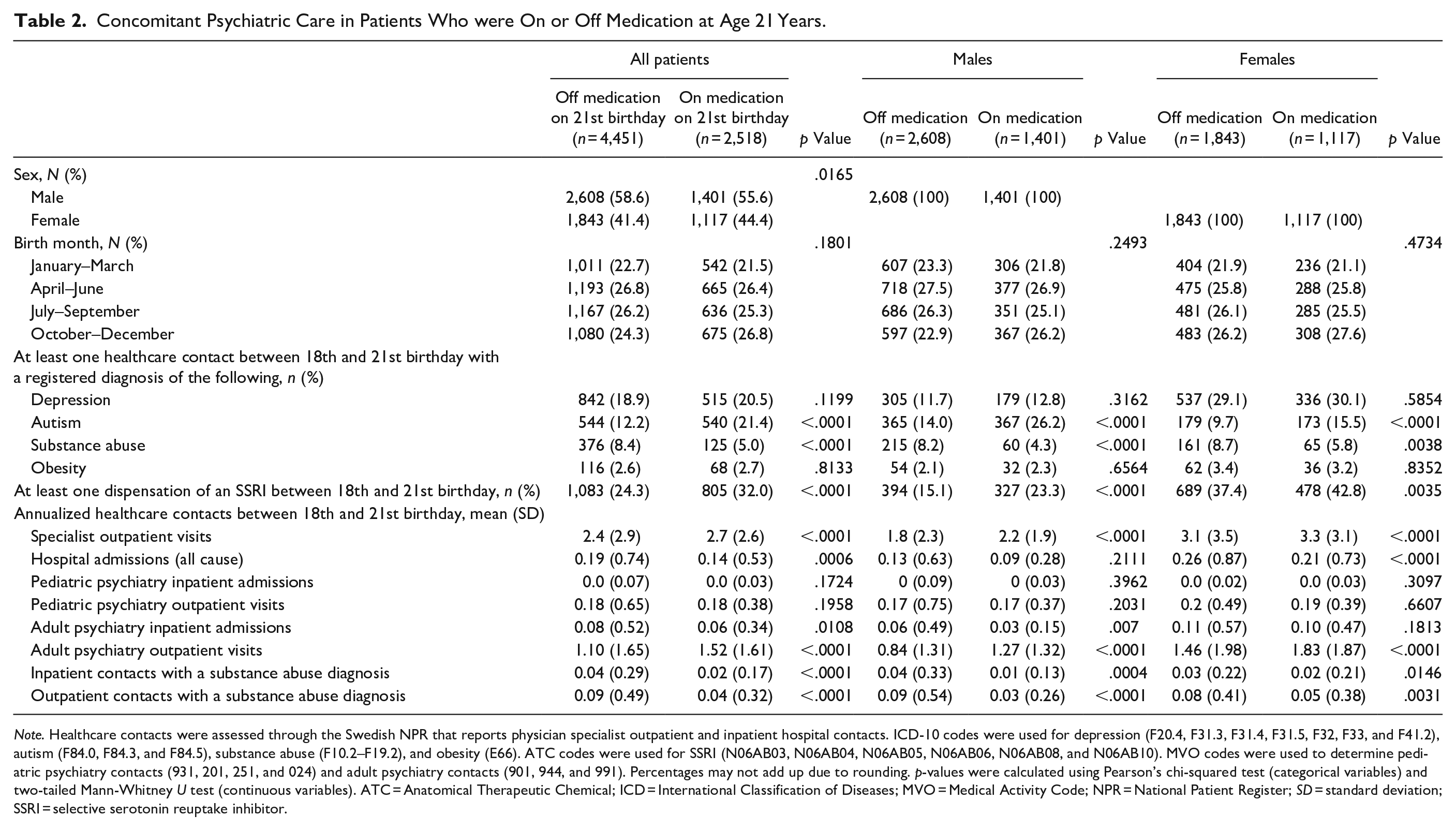
Note. Healthcare contacts were assessed through the Swedish NPR that reports physician specialist outpatient and inpatient hospital contacts. ICD-10 codes were used for depression (F20.4, F31.3, F31.4, F31.5, F32, F33, and F41.2), autism (F84.0, F84.3, and F84.5), substance abuse (F10.2–F19.2), and obesity (E66). ATC codes were used for SSRI (N06AB03, N06AB04, N06AB05, N06AB06, N06AB08, and N06AB10). MVO codes were used to determine pediatric psychiatry contacts (931, 201, 251, and 024) and adult psychiatry contacts (901, 944, and 991). Percentages may not add up due to rounding. p-values were calculated using Pearson’s chi-squared test (categorical variables) and two-tailed Mann-Whitney U test (continuous variables). ATC = Anatomical Therapeutic Chemical; ICD = International Classification of Diseases; MVO = Medical Activity Code; NPR = National Patient Register; SD = standard deviation; SSRI = selective serotonin reuptake inhibitor.
Discussion
In this nationwide population-based study, we examined the baseline characteristics and psychiatric care provision for nearly 20,000 individuals who had been prescribed treatments for ADHD in Sweden over a period of 3 years. Our study demonstrated that, despite approximately 85% of patients who were prescribed ADHD treatments having established contact with adult psychiatric care services by 21 years of age, the use of treatment declined in individuals from age 18 years onwards, suggesting that many patients discontinue their treatment during the transition period from pediatric to adult care. Our results complement the findings of a recent multinational study that investigated treatment adherence in children, adolescents, and adults with ADHD (Brikell et al., 2024). In that study, early discontinuation was highest among adolescents, when compared with children and adults. Taken together, these findings confirm that the transition from pediatric to adult care is a critical juncture in the lifetime of a patient with ADHD and suggests an unmet need in the continuity of care for children with ADHD as they transition to adulthood.
Consistent with the well-documented difference in ADHD diagnosis rates between males and females (Kooij et al., 2019), there was a higher proportion of males than females prescribed ADHD medication in our study. However, the sex difference (57.1% males vs. 42.9% females) was less than expected, which may signify a shift in the ADHD demographic; a larger number of females are now being diagnosed than have been historically. Additionally, in view of the mounting evidence suggesting that birth month may be associated with ADHD diagnosis and treatment (Karlstad et al., 2017; Layton et al., 2018; Morrow et al., 2012), we analyzed the birth-month distribution in this cohort. No major differences in birth-month distribution among those who remained on medication compared to those who had discontinued medication at 21 years of age were observed.
Depression and autism spectrum disorders are two well-known comorbidities of ADHD, so it was unsurprising that a considerable number of patients included in this study had co-morbid diagnoses of depression and autism. While there was a slightly higher percentage of males with autism than females at age 21 years (~18% vs. ~12%), the sex differences for depression were greater, with nearly one third (29%) of females with a registered diagnosis of depression versus just 12% of males. There was a higher proportion of patients with co-morbid depression and autism who were receiving ADHD medication versus those who were not. This might be in part because individuals with ADHD, alongside other co-morbidities, tend to have more frequent interactions with healthcare services and receive additional treatments. Conversely, patients with more healthcare-seeking behavior may be more likely to be diagnosed and/or treated for ADHD, and thus be more likely to be diagnosed and treated for other co-morbid conditions.
Our study showed that nearly one third of patients prescribed ADHD medication at age 21 years had received a dispensation of SSRI medications within the past 3 years. Moreover, the proportion of patients receiving SSRIs was greater than that of patients who had a registered diagnosis of depression, suggesting that these medications were prescribed for indications other than depression. SSRI dispensation was higher among patients on ADHD medication compared with those off ADHD medication, and the use of SSRIs was higher in females than in males. The gender differences observed in our study regarding SSRI prescriptions are consistent with the findings of several studies that report higher use of mental health services, including consumption of psychotropic drugs, in females than in males (Estancial Fernandes et al., 2018; Kovess-Masfety et al., 2014; Maestre-Miquel et al., 2021). Explanations for this could be: (1) females are more likely to seek medical care than males in general; (2) females are more attuned to the signs and symptoms of mental health disorders; and/or (3) physicians perceive a higher level of mental health disorders in females and are therefore more likely to prescribe psychotropic drugs (Estancial Fernandes et al., 2018). In addition, SSRIs are increasingly used for the treatment of premenstrual syndrome (Marjoribanks et al., 2013), which could also explain the observed gender differences in the prescription of SSRIs.
There is a known association between ADHD and SUD (Rohner et al., 2023); in our study, we observed that, by age 21 years, approximately 7% of patients had received healthcare services for SUD within the previous 3 years. Interestingly, among patients with co-morbid SUD, more patients were not taking ADHD medication than were taking ADHD medication. This could be explained by a degree of controversy surrounding the pharmacological treatment of ADHD and SUD. Stimulants, particularly the short-acting ones, although effective treatments for these patients, are at risk of being misused, especially by adolescents and young adults, and clinicians may be reluctant to prescribe them (Crunelle et al., 2018).
A limitation of this study is that it was contingent on the type of information that was recorded in the patient registries; therefore, some caution should be exercised in interpreting certain findings. It is important to note that, although the patients studied had all been prescribed medications to treat ADHD, it was not possible to confirm that they had received an ADHD diagnosis. Additionally, the PDR provided data on SSRI prescriptions but not on the indications for which they were prescribed, so it is unclear what other conditions these may have been used for. It is relevant to note that, in Sweden, the prescription of central stimulants is restricted to specialists in child or adult psychiatry, or in child neurobiology and rehabilitation. Therefore, our sample is likely to predominantly consist of patients with a confirmed diagnosis of ADHD.
A further consideration is that in the NPR, non-physician (e.g., psychologist) visits are not recorded and visits to outpatient clinics (particularly private practices) were incomplete, so it would not be possible to ascertain with any certainty how patients who had apparently “discontinued” treatment were followed-up in the healthcare system. Although we found a considerable level of treatment discontinuation among the patients included in our study, it is unclear whether a similar trend would be observed for children with other neurodevelopment conditions, such as those with autism spectrum disorder (ASD) and co-morbid mental health conditions. It has been recognized that, as with ADHD, the transition from pediatric to adult psychiatric services can pose challenges for individuals with ASD (Maurice et al., 2022). While in ADHD difficulties in transition could stem from impulsiveness, distractibility, and forgetfulness that may limit patients’ abilities to transition independently, obstacles for individuals with ASD could be anxiety toward changes in their healthcare or an impaired ability to communicate issues relating to their condition (Maurice et al., 2022).
Our findings contribute to a growing body of evidence that suggest an unmet need in the continuity of care for patients with ADHD. The reasons for patients being lost during the transition from pediatric to adult psychiatric care warrant further study. As diagnoses and medication prescriptions for ADHD rise, there will be an important need to ensure that children and adults receive uninterrupted support throughout their lifetimes.
Conclusions
In this population-based study from Sweden, we found that ADHD medication use declined after age 18 years, indicating discontinuation during the transition from pediatric to adult care. Co-morbid depression and autism were prevalent among patients, with a higher proportion of females having registered depression diagnoses. By age 21 years, patients who were receiving ADHD medication were more likely to have co-morbidities, including depression and autism, than those patients who were not receiving ADHD medication. The findings emphasize the need for improved continuity of care, early interventions, and personalized support to ensure medication adherence, and address associated co-morbidities in individuals with ADHD.
Supplemental Material
sj-docx-1-jad-10.1177_10870547241303259 – Supplemental material for Transitioning From Pediatric to Adult Psychiatric Care for ADHD in Sweden: A Nationwide Study
Supplemental material, sj-docx-1-jad-10.1177_10870547241303259 for Transitioning From Pediatric to Adult Psychiatric Care for ADHD in Sweden: A Nationwide Study by MaiBritt Giacobini, Jingcheng Zhao, Jonatan Freilich, Carolina Malmgren, Niklas Wallin Bernhardsson and Ewa Ahnemark in Journal of Attention Disorders
Footnotes
Acknowledgements
Medical writing support for this manuscript was provided by Kate Bradford, PhD, of Parexel, under the direction of the authors, and was funded by Takeda Pharmaceuticals International AG. The authors thank Magnus Andersson, formerly of Takeda, for his involvement in discussion of the preliminary results.
Data Availability
The study data cannot be shared due to local data protection regulations.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MG has served as a consultant for Eli Lilly, Janssen-Cilag, and Shire (a Takeda company); has received speaker fees and reimbursement for travel costs from Nutricia; and has been a principal investigator for Novartis, Shire (a Takeda company), and Takeda. CM and NWB are employees of Takeda Pharma AB, Sweden. EA was employed by Shire Sweden AB (a Takeda company) at the time of this research. JZ and JF are/were employed by Parexel International, which has received funding from Takeda for conducting the study. This study was funded by Takeda, who were involved in the study design, collection, analysis, interpretation of data, and drafting of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The original research for this study was funded by Shire Development LLC, which is now part of Takeda. The current analysis was funded by Takeda Pharmaceuticals International AG.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.