
Abstract
Keywords
Introduction
ADHD is a neurodevelopmental disorder characterized by symptoms of inattention, hyperactivity, and impulsivity, which lead to significant functional impairments and a diminished quality of life (QoL; American Psychiatric Association, 2013). The prevalence of ADHD among school-aged children worldwide is approximately 5.3% to 7.2% (Faraone et al., 2021; Polanczyk et al., 2014; Thomas et al., 2015). Longitudinal studies have demonstrated high rates of ADHD persistence into adulthood (approximately 55%), which are associated with detrimental consequences for functional outcomes and QoL (American Psychiatric Association, 2013; Di Lorenzo et al., 2021; Fayyad et al., 2017; Kessler et al., 2006; Polanczyk et al., 2014; Thomas et al., 2015).
The negative repercussions of ADHD in adulthood span multiple functional domains, including social relationships (Asherson et al., 2016; Barkley & Fischer, 2010; Brod et al., 2012). Specifically, there is ample evidence of ADHD-related impairments in romantic relationships among adults with ADHD and their partners. Studies show that partners of individuals with ADHD report unfavorable patterns in their marriages, such as poor conflict resolution, lower intimacy, and less marital satisfaction (Ben-Naim et al., 2017; Öncü & Kişlak, 2022). Additionally, these couples experience more financial difficulties and a higher risk for domestic violence, compared to couples without ADHD (Arrondo et al., 2023; Steele et al., 2022). Ersoy and Topçu Ersoy (2019) found that women without ADHD, who are in a relationship with a partner diagnosed with ADHD, reported a more substantial negative impact of ADHD on their marriage compared to men in the same situation. This aligns with studies revealing that marital challenges disproportionately affect women’s psychological well-being (Hafner & Spence, 1988; Whitton & Kuryluk, 2012). A recent qualitative study examined the experiences of women in a relationship with a men diagnosed with ADHD. Findings highlighted women’s experiences of: (a) persistent functional impairments of partners with ADHD, (b) the burden associated with these impairments as being “like another child,” and (c) the coping strategies they employed (Zeides Taubin & Maeir, 2023). In sum, the evidence of relational impairment is compelling and suggests the need to further examine partner function to better understand ADHD-related impairment.
Research into the impact of mental health conditions, such as depression and bipolar disorder, on partners can shed light on the potential effects of ADHD on partner functioning. Evidence suggests that partners, especially women, face significant challenges that detrimentally affect their health (Chappell et al., 2015; Cormican et al., 2022; Vaingankar et al., 2012). Informal caregivers frequently report increased psychological distress, perceived burden, and decreased quality of life (QoL; S. Gupta et al., 2015; P. Gupta et al., 2022; Kim et al., 2012; Kniepmann & Cupler, 2014; Koyama et al., 2017; Naga Pavan Kumar et al., 2019; Nehra et al., 2005; Rudman et al., 2006; Vaingankar et al., 2012). Such individuals often show diminished engagement in health-promoting activities, such as physical, social, and leisure activities compared to those not in caregiving roles (H. Bourke-Taylor et al., 2014; Farrugia et al., 2019; Hanzawa et al., 2010; Kniepmann & Cupler, 2014; McDougall et al., 2014; Schüz et al., 2015; Wakui et al., 2012). On the other hand, engaging in health-promoting activities (HPA) has been demonstrated to alleviate some of the burdens associated with caregiving (Acton, 2002; H. M. Bourke-Taylor et al., 2022; Losada et al., 2010). Concerning women living with individuals diagnosed with ADHD, there is a need to examine their mental health, as well as the potential positive impact of engaging in HPA.
This study aims to investigate the mental health, defined as depressive symptoms and quality of life (QoL) of women living with men diagnosed with ADHD, and to explore the role of engagement in health-promoting activities on these outcomes. Our hypotheses are as follows: (a) women’s ratings of their partners’ ADHD-related impairments will be associated with the severity of the women’s depressive symptoms and inversely associated with their QoL; and (b) the level of women’s participation in health-promoting activities will be positively associated with their QoL and inversely associated with the severity of their depressive symptoms. By examining these dynamics, this research aims to illuminate the broader implications of ADHD on women who are partners of men with ADHD.
Materials and Methods
Design
The present study employed a quantitative, cross-sectional explanatory design, integrating both descriptive and correlational methods. Structural Equation Modeling (SEM) played a significant role among the statistical approaches used. The minimal sample size was determined using G*Power. For a paired t-test, assuming an alpha of .05, a power of 80%, and a small effect size (d = 0.3), the calculation resulted in a requirement for 71 pairs. However, for SEM analyses, a minimum sample size of 100 to 150 participants is recommended (Tabachnick & Fidell, 2001).
Participants
The study recruited adult dyads, between ages 20 and 60 years, who had been in a cohabiting relationship for at least 2 years. This criterion was set to ensure that the relationships studied were stable and representative of long-term dynamics. Men partners were included if they had a self-reported diagnosis of ADHD from a certified medical professional at any point in their lives and currently exhibited ADHD symptoms above a predefined threshold, as measured by the ADHD Self-Report Scale-Screener (ASRS-S; Kessler et al., 2005). This dual criterion of historical diagnosis and current symptomatology was employed to ensure the sample specifically included men likely to have persistent ADHD. Women partners were included if they did not have an ADHD diagnosis, verified by their self-reports and confirmed by scoring below the ADHD cutoff on the ASRS-S.
Exclusion criteria for all participants included other major health conditions that could potentially impact daily family functioning, as determined through self-reports. This study focused on heterosexual couples, based on existing literature indicating gender disparities in adult ADHD (Ersoy & Topçu Ersoy, 2019; Williamson & Johnston, 2015). Participants were required to be under the age of 60 years to minimize the influence of aging-related factors.
Measures
The current study used various tools to assess ADHD symptoms and functional impairment in men, as well as symptoms of depression, quality of life, and engagement in health-promoting activities among their women partners.
For ADHD symptom assessment in both partners, the Adult ADHD Self-Report Scale Symptom Checklist (ASRS-v1.1; Kessler et al., 2005) was utilized. Based on the DSM-IV criteria, this tool consists of 18 items scored on a 5-point scale (0 = “never” to 4 = “very often”). Higher scores indicate greater symptom severity. For recruitment, we used the ASRS screener’s first six items with a cut-off of ≥ 4 (positive rating for items 1–3: ≥ 2; for items 4–6: ≥3) based on the self-reports of men (Kessler et al., 2005). The Hebrew version of the ASRS demonstrates robust psychometric properties, including an internal reliability of α = .89, sensitivity of 65%, and a specificity of 68% (Zohar & Konfortes, 2010). The reliability of the scale within the context of the current study was confirmed at α = .80.
The Weiss Functional Impairment Rating Scale (WFIRS; Weiss et al., 2018) was utilized to evaluate functional impairment attributable to ADHD in men, with assessment based on informant reports provided by their women partners. The comprehensive WFIRS, with its 69 items, evaluates seven functional domains: Family, Work, School, Life Skills, Self-Concept, Social, and Risk. With its 4-point scoring system (0–3), the scale provides mean scores for each domain and an overall mean score. A domain is considered functionally impaired when at least two items score a 2 or when any item scores a 3. The WFIRS-S has undergone psychometric validation in ADHD populations, demonstrating strong internal consistency (Cronbach’s alpha α > .80), high test-retest reliability, and significant correlation with symptom variations. It provides detailed impairment percentages for each evaluated domain (Canu et al., 2020). The scale is available in 19 languages, including Hebrew. The scale’s reliability in this study was 0.93.
The Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001) was utilized to assess depression symptoms in women partners. This self-report tool aligns with DSM-IV criteria and includes nine items that assess symptoms of depression occurring over the past 2 weeks, such as loss of interest, depressed mood, changes in sleep, appetite, and energy, feelings of low self-worth, difficulty concentrating, alterations in psychomotor activity, and suicidal ideation. Each item scores from 0 to 3, with cumulative scores representing symptom severity. Higher total scores denote more severe symptoms, and based on these, depression severity can be categorized as: none (0–4), mild (5–9), moderate (10–14), moderately severe (15–19), and severe (20–27; Kroenke & Spitzer, 2002). The Hebrew version’s reliability ranged from .79 to .83 (Yona et al., 2021). In the current study, the PHQ-9 exhibited a reliability of .82.
The quality of life of women partners was evaluated using the World Health Organization Quality of Life assessment (WHOQoL-BREF; The WHOQOL Group, 1998), a 24-item questionnaire that is an abbreviated version of the WHOQOL-100. The questionnaire evaluates four domains: physical health, psychological health, social relationships, and environment. Each item uses a 5-point Likert scale, with higher scores indicating better quality of life. Domain scores were computed as the mean score of items in each domain, linearly transformed to a 100-point scale according to guidelines. We also averaged the scores of all four domains to derive the total WHOQoL-BREF score for correlation with the research variables. The WHOQOL-BREF has displayed good discriminant validity and internal consistency and has been used in previous caregiver studies (Angermeyer et al., 2006; Skevington et al., 2004). The Hebrew version demonstrated high reliability in an Israeli sample, with an average Cronbach’s alpha of 0.93 (Lev-Wiesel & Amir, 2000). In the current study, the WHOQoL-BREF showed reliability of Cronbach’s alpha greater than .80 across all domains and the entire scale.
The participation of women partners in social, emotional, physical, and spiritual leisure activities was assessed using the Health Promoting Activities Scale (HPAS; H. Bourke Taylor-et al., 2012). This eight-item scale measures the frequency of participation in health-promoting activities and is scored from 1 (never) to 7 (once or more every day). The HPAS is characterized by good internal consistency (α = .78) and has demonstrated construct validity, evidenced by its correlation with mental and general health indicators among adult women, encompassing both caregivers and the general population (H. Bourke-Taylor et al., 2012, 2014; Farrugia et al., 2019). The HPAs showed a reliability of .80 in the current study.
Lastly, a socio-demographic questionnaire was employed to gather data on participants’ backgrounds, including age, marital status, education level, household income, number of children, and the ADHD medication status of the man partner.
Procedure
The study received approval from the Hebrew University’s institutional review board (IRB; Approval no. 2072020). Participants were recruited using a combination of methods to reach a diverse participant pool. The majority were reached through social media advertisements, which accounted for approximately 80% of the participants, while the remaining 20% were recruited through flyers and personal referrals. Researcher credentials, and contact information provided in each recruitment call. Of the 146 couples who expressed interest, 36 men were excluded for not meeting the ADHD symptom criteria as per their ASRS scores, and 2 others were excluded due to significant health conditions.
After passing the screening, each participant received an anonymous identifier to ensure confidentiality. They accessed the questionnaires via a digital link, with a paper version available upon request. However, eight participants did not complete the questionnaires. As a token of appreciation for their time and effort, each participating couple was awarded 100 ILS.
Demographic Data
The study’s final sample consisted of 100 heterosexual couples. The women had an average age of 32.76 years (SD = 7.14), and 94% were employed at the time of the study. Among the women partners, 9 had completed high school, 47 had undergone post-secondary education or held a degree, and 44 had pursued post-graduate studies. On average, couples had been in their relationships for 9.27 years (SD = 6.42), with 65 married and 35 in non-marital relationships. In terms of family income, 40 couples reported earnings below the national average, 23 at the average, and 37 above it. Fifty-seven of these couples had children, with an average of 2.69 children (SD = 1.48) per family. The men partners were on average 33.93 years old (SD = 7.68), with 90% currently employed. Among the men partners, 31 had finished high school, 49 had completed post-secondary education or held a degree, and 20 had post-graduate qualifications. The average duration since their ADHD diagnoses was 15.5 years (SD = 8.67). Detailed demographic breakdowns for each group are presented in Table 1.
Demographic Characteristics.
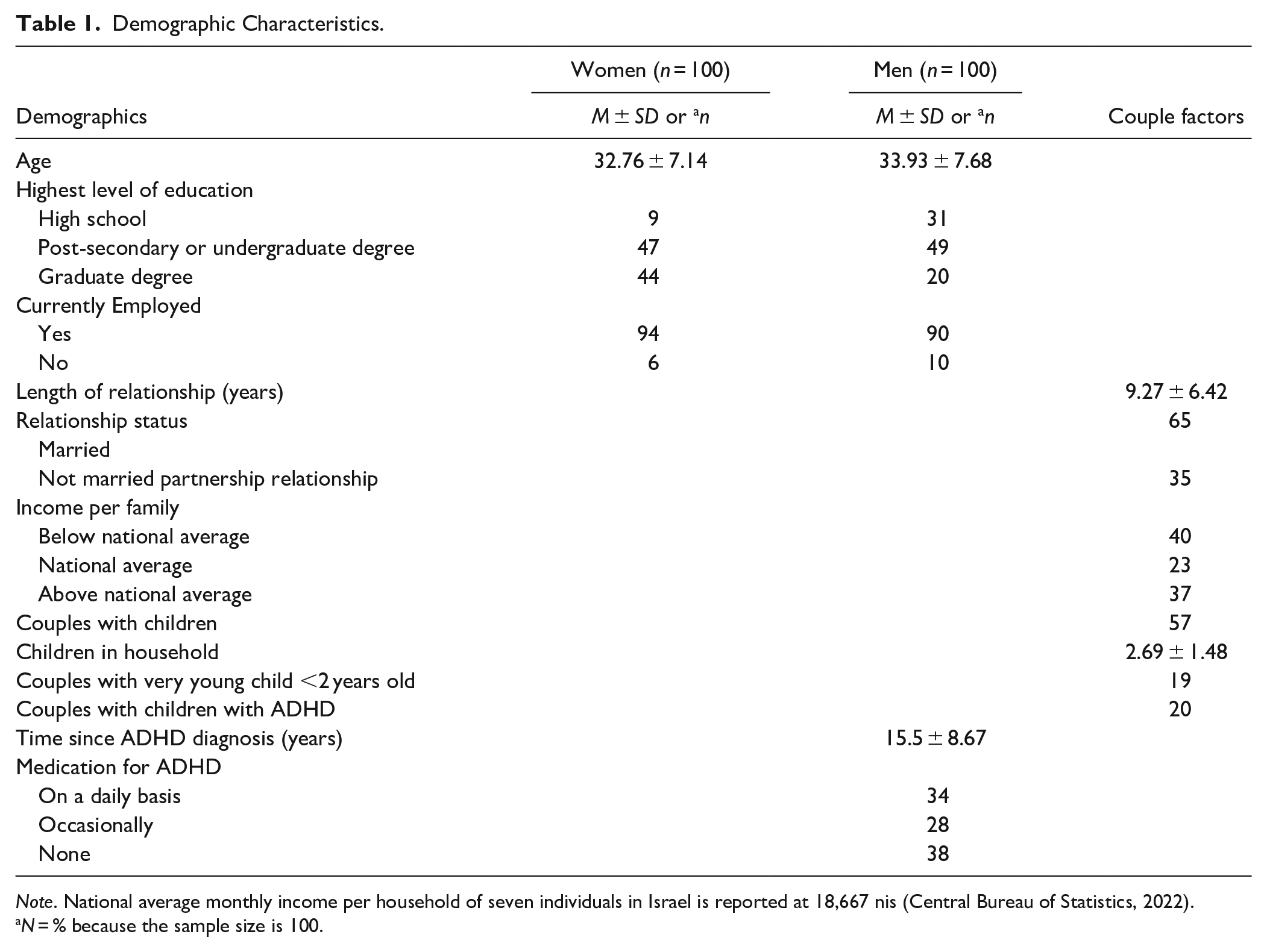
Note. National average monthly income per household of seven individuals in Israel is reported at 18,667 nis (Central Bureau of Statistics, 2022).
N = % because the sample size is 100.
Data Analyses
Data analysis was conducted using SPSS statistical software (Version 25.0; IBM Corp, 2017), with a significance threshold set at p < .05. Descriptive statistics, including means, percentages, and frequencies, were computed for demographic data and scores on various measures. The dataset had less than 1% missing data, which were excluded from relevant variable analyses. Specifically, for the WFIRS questionnaire, “not applicable” responses were omitted from mean score calculations, affecting 25% of responses regarding the “study” domain.
To assess the distribution of all variables, we calculated z-scores for skewness and kurtosis. Most variables exhibited z-scores within ±2.58, suggesting a normal distribution. However, the PHQ-9 and WFIRS datasets showed right-skewness, as indicated by skewness z-scores deviating from the norm. A square root transformation was applied to normalize these distributions.
Pearson’s correlation analysis was used to explore relationships among the study variables, including men’s ADHD symptoms and functional impairment, women’s participation in HPA, depressive symptoms, and QoL. Spearman’s correlation analysis was used to assess the associations between socio-demographic factors, depressive symptoms, and QoL. An independent samples t-test was conducted to examine differences in QoL between women whose partners consistently took ADHD medication and those whose partners were inconsistent or did not medicate at all.
To examine the association between men’s ADHD functional impairment, women’s participation in HPA, and their depressive symptoms and QoL, we employed Structural Equation Modeling (SEM) using maximum likelihood estimation. SEM allows for the analysis of complex relationships between variables by combining correlation and regression analyses, enabling validation of theoretical models against empirical data. Covariates such as age, number of children, duration of the relationship, and household income were considered in the initial analysis. However, these variables did not show significant associations with the primary outcomes (p > .05) and were therefore excluded from the final SEM model to focus on the primary relationships of interest.
We assessed the model fit using various goodness-of-fit indices, including Chi-square, Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), and Root-Mean-Square Error of Approximation (RMSEA). A satisfactory model fit was characterized by a non-significant chi-square, CFI and TLI values of .95 or higher, and an RMSEA of .06 or lower (Hu & Bentler, 1999; Tabachnick & Fidell, 2001). We further analyzed standardized path coefficients to determine the statistical significance and directionality of relationships between variables.
Results
Women’s Reports on Partners’ ADHD Functional Impairment
In this study, although men completed part of the ADHD Self-Report Scale (ASRS) to determine their eligibility for the study, our analyses focused on the informant reports provided by women regarding their perceptions of ADHD functional impairments (WFIRS) in their partners. Women reported WFIRS average score of 0.94 (SD = 0.46) and identified about 3.94 (SD = 1.90) domains as impaired. These findings highlight the perspective of women on the ADHD-related challenges faced by their partners. Moreover, women rated their partners’ functional impairment lower than the men’s self-rating, with men reporting an average WFIRS score of 1.12 (SD = 0.48), identifying approximately 4.55 (SD = 2.01) domains as impaired. These findings are further detailed in Table 2.
Partners’ ADHD Symptoms and Functioning Impairment (N = 100).
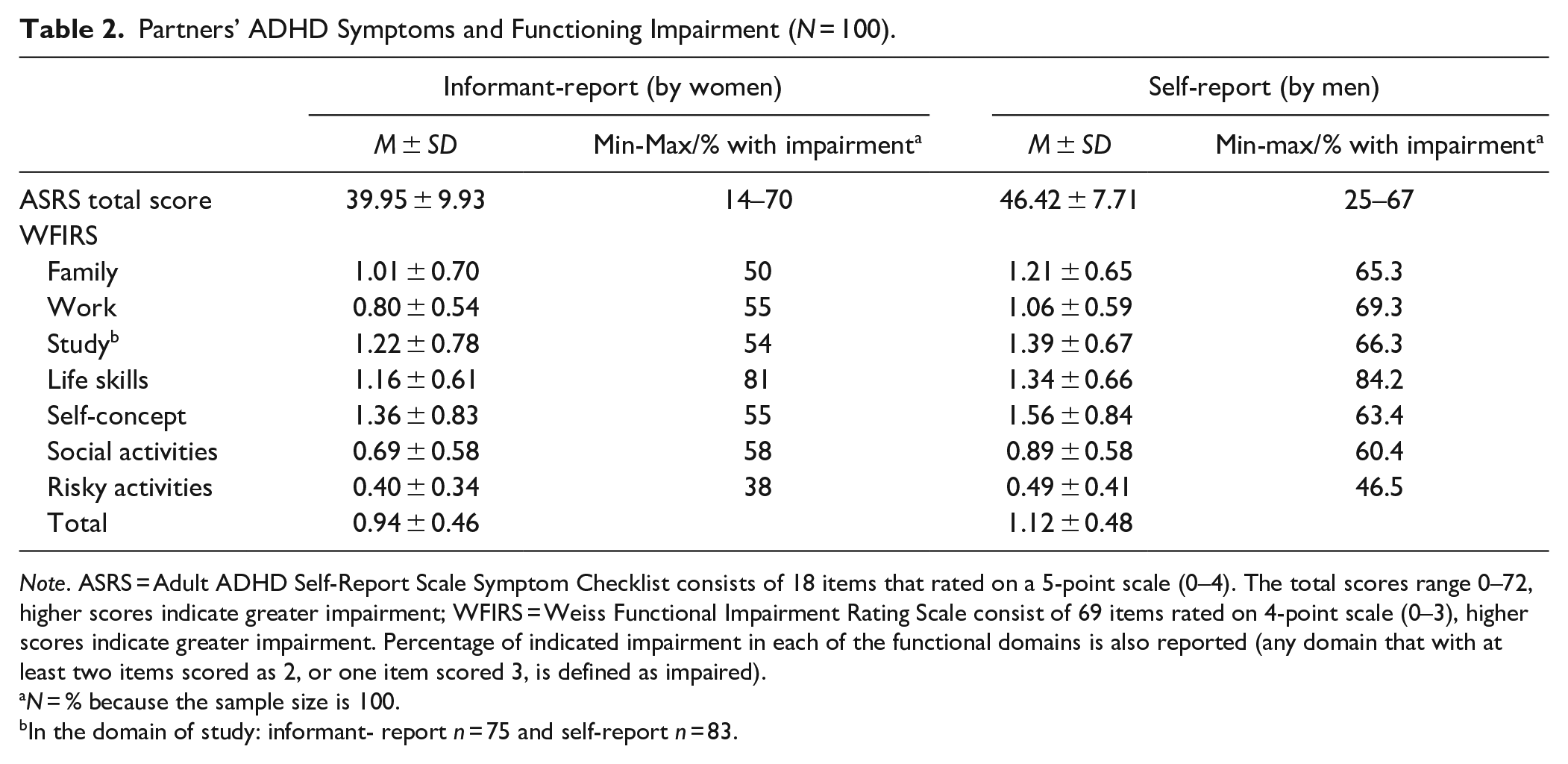
Note. ASRS = Adult ADHD Self-Report Scale Symptom Checklist consists of 18 items that rated on a 5-point scale (0–4). The total scores range 0–72, higher scores indicate greater impairment; WFIRS = Weiss Functional Impairment Rating Scale consist of 69 items rated on 4-point scale (0–3), higher scores indicate greater impairment. Percentage of indicated impairment in each of the functional domains is also reported (any domain that with at least two items scored as 2, or one item scored 3, is defined as impaired).
N = % because the sample size is 100.
In the domain of study: informant- report n = 75 and self-report n = 83.
Women’s Depressive Symptoms, Quality of Life, and Health-Promoting Activities
Women’s Quality of Life (QoL) was evaluated across various domains. The social (M = 65.66, SD = 18.32) and psychological health domains (M = 66.79, SD = 13.18) reported the lowest scores, while the physical health domain had the highest score (M = 70.46, SD = 12.78). According to the Patient Health Questionnaire-9 (PHQ-9), 59% of women reported experiencing depressive symptoms ranging from mild to severe. Detailed statistics for these measures are provided in Table 3.
Women’s Mental Health Outcomes (N = 100).
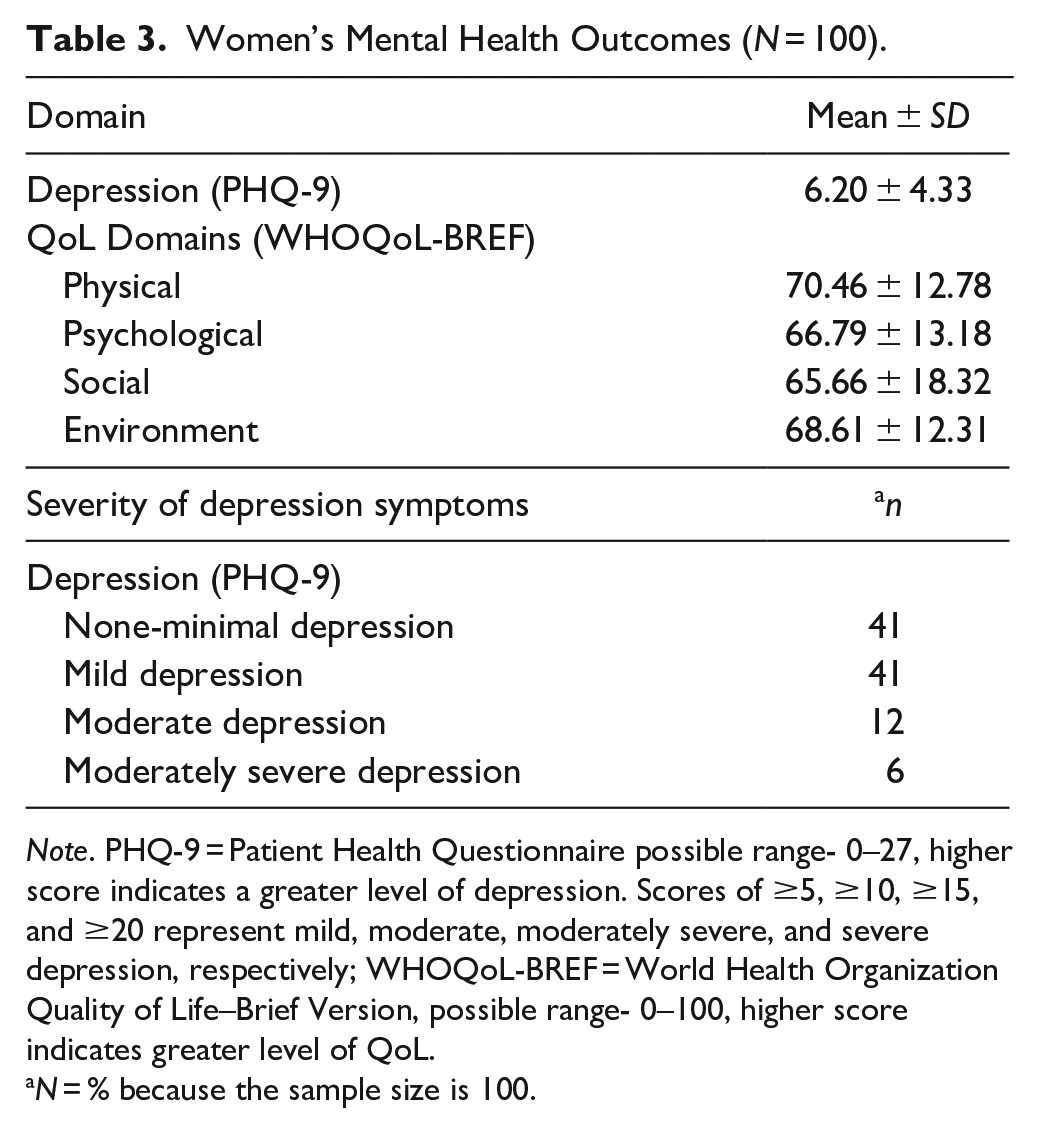
Note. PHQ-9 = Patient Health Questionnaire possible range- 0–27, higher score indicates a greater level of depression. Scores of ≥5, ≥10, ≥15, and ≥20 represent mild, moderate, moderately severe, and severe depression, respectively; WHOQoL-BREF = World Health Organization Quality of Life–Brief Version, possible range- 0–100, higher score indicates greater level of QoL.
N = % because the sample size is 100.
Regarding participation in health-promoting activities, as assessed by the Health Promoting Activities Scale (HPAs), women had an average score of 31.28 (SD = 8.99). This mid-range score can reflect a moderate level of participation, with higher scores indicating increased frequency in health-promoting activities. Weekly participation in these activities ranged from 31% to 63%. Activities such as “physically active recreational pursuits with others” and “spiritual/rejuvenating personal time” were less frequent. In contrast, “personal healthcare tasks” and “social activities with close ones” were more commonly reported. These findings are further detailed in Table 4.
Frequency Women Participate in Health Promoting Activities, HPAS, (an = 100).
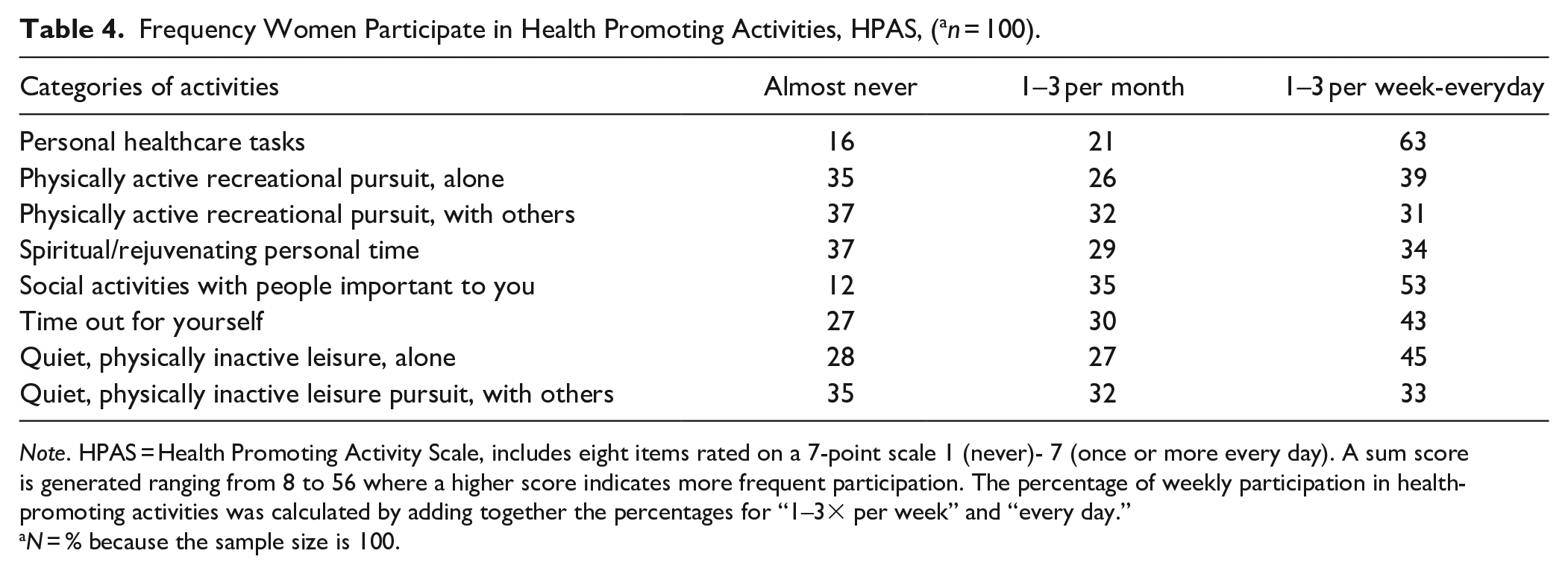
Note. HPAS = Health Promoting Activity Scale, includes eight items rated on a 7-point scale 1 (never)- 7 (once or more every day). A sum score is generated ranging from 8 to 56 where a higher score indicates more frequent participation. The percentage of weekly participation in health-promoting activities was calculated by adding together the percentages for “1–3× per week” and “every day.”
N = % because the sample size is 100.
Associations Between Study Variables
We explored correlations between the perceived functional impairment due to ADHD in men, women’s participation in HPA, and their mental health outcomes. The functional impairment rating (WFIRS) for men with ADHD was found to be negatively correlated with the overall QoL of women partners (WHOQoL-BREF total score; r = −.28) and specifically their Social Qol (r = −.38). Additionally, a positive correlation was observed between WFIRS scores and depressive symptoms in women partners (PHQ-9; r = 27), indicating that higher perceived functional impairment in men with ADHD is linked with more severe depressive symptoms in women. Women’s participation in HPA showed a positive association with their QoL (WHOQoL-BREF total score; r = .36) and an inverse relationship with depressive symptoms (PHQ-9; r = −.22).
The study also examined potential confounders that might influence the study’s outcomes. Notably, the age of both partners, number of children, and the duration of the relationship did not exhibit a significant association with outcomes (p > .05), except for a small negative correlation between age, duration of the relationship, and social QoL (r = −.25 to −.29, p < .05). Regarding household income, small negative correlations were found with psychological QoL and depressive symptoms (r = .20; −26 accordingly). The results of the correlation analyses are presented in Table 5.
Associations Between Study Variables (N = 100).
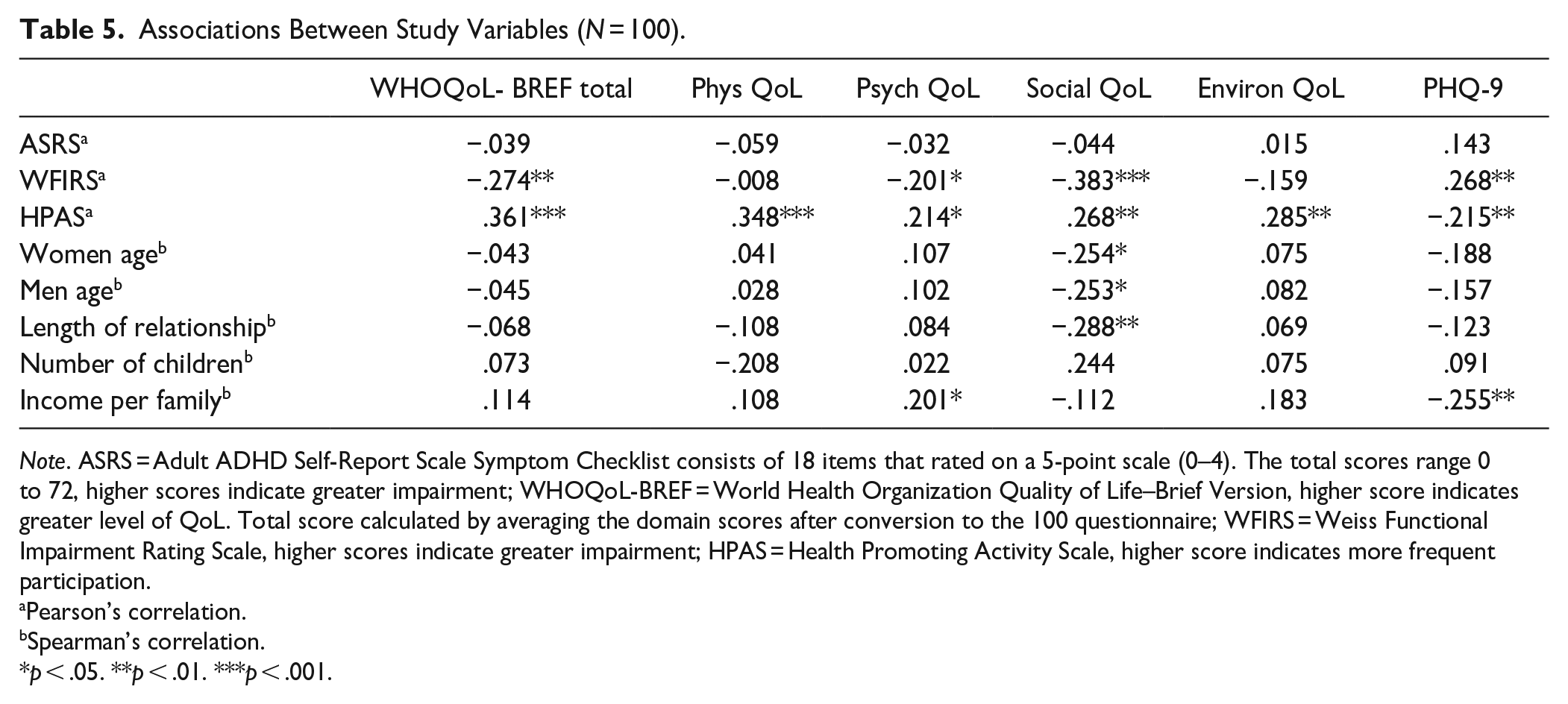
Note. ASRS = Adult ADHD Self-Report Scale Symptom Checklist consists of 18 items that rated on a 5-point scale (0–4). The total scores range 0 to 72, higher scores indicate greater impairment; WHOQoL-BREF = World Health Organization Quality of Life–Brief Version, higher score indicates greater level of QoL. Total score calculated by averaging the domain scores after conversion to the 100 questionnaire; WFIRS = Weiss Functional Impairment Rating Scale, higher scores indicate greater impairment; HPAS = Health Promoting Activity Scale, higher score indicates more frequent participation.
Pearson’s correlation.
Spearman’s correlation.
p < .05. **p < .01. ***p < .001.
In addition, women whose partners consistently took ADHD medication experienced significantly better QoL (M = 71.38, SD = 9.87) than those whose partners were inconsistent or did not medicate at all (M = 65.99, SD = 11.09), t(98) = 2.396, p = .02, Cohen’s d = 0.51.
Associations Between ADHD-Related Impairment, Participation in Health-Promoting Activities, and Women’s Health Outcomes: Structural Equation Modeling
All variables associated with mental health outcomes were entered into the model; however, only the variables which had significant associations with other variables are presented. In our Structural Equation Modeling (SEM) analysis, we sought to explore the associations between the functional impairment associated with ADHD in men, women’s participation in health-promoting activities, and their depressive symptoms and QoL. The model underscored significant associations for both perceived ADHD-related functional impairment and the extent of participation in health-promoting activities with depressive symptoms and QoL aspects, with the exception of the association between ADHD-related functional impairment and physical QoL. Figure 1 highlights the significant variables, coefficients, and correlations, emphasizing the model’s alignment with the data (χ2 (4) = 4.131, p = .389, CFI = 0.999, NFI = 0.983, RMSEA = 0.018, and TLI = 0.996).
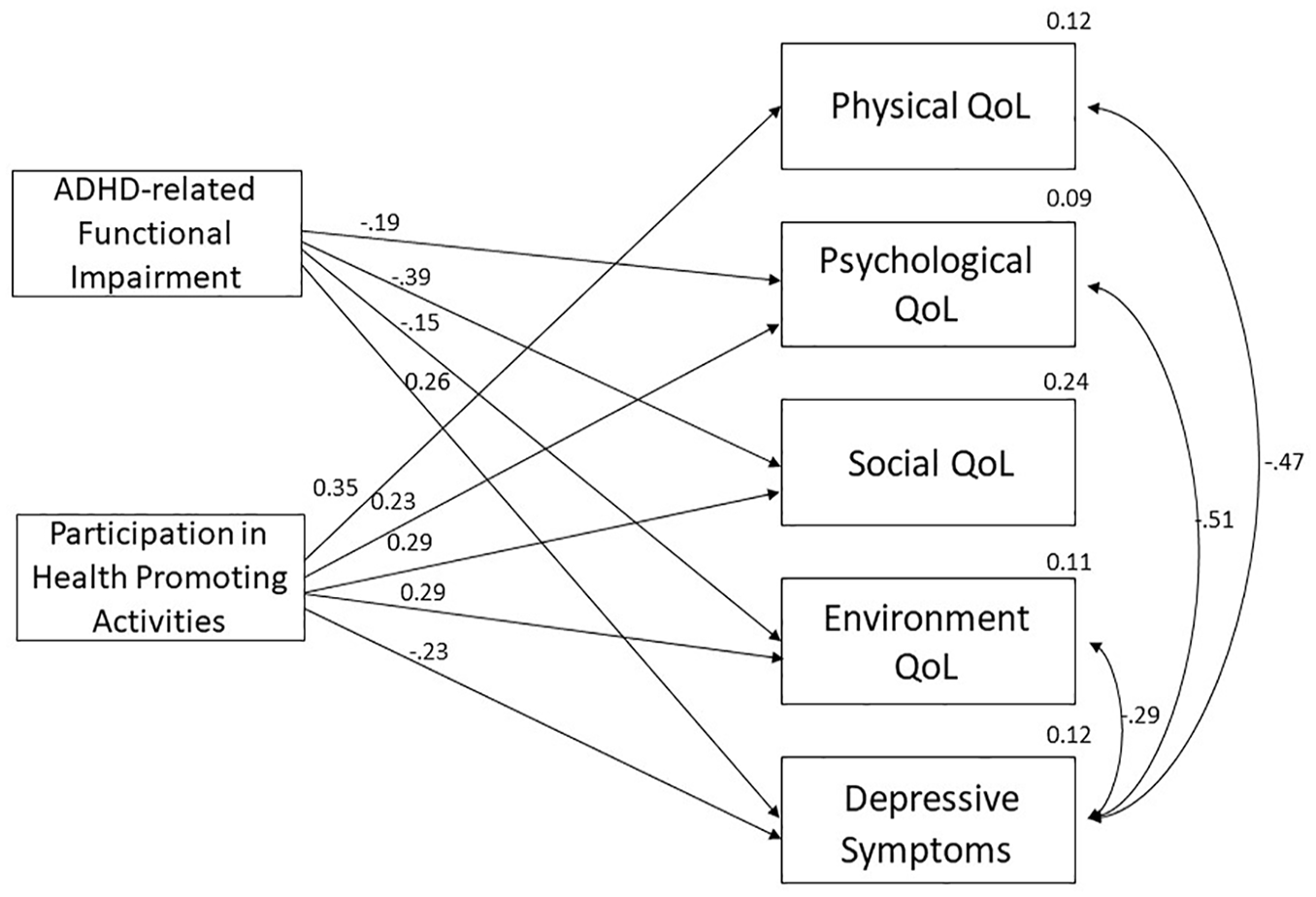
Structural equation model.
Examination of the associations of ADHD-related functional impairment with QoL domains revealed significant negative associations with the psychological, social, and environmental aspects of QoL (β = −.19, −.39, and −.15, respectively). Moreover, ADHD-related functional impairment was significantly associated with higher depressive symptoms among women (β = .26), suggesting that greater ADHD functional impairment correlates with poorer mental health outcomes. Conversely, participation in health-promoting activities by women was associated with lower depressive symptoms (β = −.23) and enhancements across all QoL domains (β = .35, .23, .29, and .29), suggesting that higher engagement in these activities is associated with better mental health.
When contrasting the absolute beta coefficient values, it appears that men’s functional impairment has a stronger associated with the social QoL domain (β = −.39) compared to participation (β = .29). In addition, the men’s functional impairment is not significantly associated with the physical QoL domain. Both men’s functional impairment and women’s participation exhibited comparable associations with the women’s depressive symptoms (β = −.19 and .23).
Discussion
This study focused on women living with partners diagnosed with ADHD. Our results revealed significant associations between the ADHD functional impairments of their partners and the women’s depressive symptoms and QoL. Specifically, functional impairment in partners with ADHD was positively associated with women’s depressive symptoms and negatively associated with their QoL. Additionally, the women’s engagement in health-promoting activities (HPA) was positively associated with their QoL and negatively associated with their depressive symptoms.
Regarding the ADHD diagnoses in men partners confirmed by self-report, it is important to note that our inclusion criteria required not only a previous diagnosis of ADHD in the partners but also the measurement of current ADHD symptoms. This methodology ensured that our sample consisted of individuals with persisting ADHD, allowing for a more accurate exploration of the condition’s ongoing associations with partners’ mental health outcomes.
Depressive Symptoms and Quality of Life in Women Cohabiting With ADHD-Diagnosed Partners
Our findings indicated that 59% of the participants experienced symptoms indicative of mild to moderately severe depression. This prevalence aligns with existing research on caregivers managing diverse health conditions (Farrugia et al., 2019; Lewis, 2017; Li et al., 2022; Mavounza et al., 2020; Paschou et al., 2018). Notably, the depression rates in our study exceeded those reported for the broader Israeli female population (Yona et al., 2021). Additionally, our cohort’s QoL scores were lower than those from comparable studies on partners of individuals with other health challenges such as schizophrenia, major depressive disorder, anxiety disorders, and stroke (Angermeyer et al., 2006; Baumann et al., 2012; Kavitha et al., 2014). Alongside these comparisons with adult caregiving literature, our findings also show similarities with those reported among caregivers of children with ADHD (Budman et al., 2023; Cappe et al., 2017; Xiang et al., 2009). While comparing the women in this study to caregivers offers one possible interpretation of the findings, caution is warranted as other interpretations may also be valid.
Functional Impairment in Partners With ADHD: Its Relationship With Women’s Depressive symptoms and Quality of Life
The findings of our sample are consistent with other studies on the functional disability of adults with ADHD, aligning with research emphasizing functional impairment as a critical element in understanding and managing ADHD (Bölte et al., 2018; Sonuga-Barke et al., 2023). Our data indicated that a considerable precent of the women (38%–81%) reported impairment in all the functional domains. These rates of impairment are similar to those self- reported in a large sample (n = 2,093) of adults with ADHD (Canu et al., 2020). Interestingly, in our study, women reported lower levels of their partners’ functional impairment compared to the partners’ self-reports. This divergence may be attributed to the study’s inclusion criteria, which required men to have a validated ADHD diagnosis and meet the ASRS symptom threshold at present. Such criteria might have contributed to heightened self-awareness among the men participants.
This study focused on the spouses’ perspective, expanding the understanding the associations of partner ADHD-related dysfunctions and women’s mental health outcomes. The consistent use of ADHD medication by partners was associated with higher perceived QoL among the women, aligning with Kosheleff et al. (2023) review, who suggest that pharmacological treatments can mitigate ADHD symptoms and lessen their functional repercussions. These findings may imply that pharmacological treatments may also have a beneficial effect on partners as well as individuals with ADHD.
In accordance with our hypotheses, relationships were found in the expected direction between the severity of ADHD-related functional impairments and the women’s health indicators. However, the percentage of explained variance of the health indicators is not high, suggesting the need to consider additional explanatory variables unrelated to the man’s ADHD, such as factors related to the woman and her life contexts. Furthermore, the cross-sectional nature of our study does not allow for causal conclusions. The direction of these associations requires further investigation through longitudinal studies to determine whether the functional impairments in partners directly lead to depressive symptoms and lower QoL in women or if other factors are at play. Future research should consider multi-informant data and longitudinal designs to gain a more comprehensive understanding of the impact of ADHD on relationships and the mental health of partners.
The Role of Health-Promoting Activities on Mental Health
Our study further investigates the role of participation in HPA in the daily lives of these women. The SEM results support the positive association between women’s engagement in HPA and their mental health outcomes, even when accounting for the negative effects of their partner’s ADHD-related functional impairment. While this model does not indicate a moderating effect of engaging in HPA on the association between partners’ impairment and women’s health, it points to a potential independent benefit of engaging in HPA, despite the presence of ADHD in their partners. This finding echoes the universal principles of occupational science, emphasizing the link between participation and health, underscoring the importance of HPA in this population as well (Law et al., 1998; Townsend & Polatajko, 2007).
This study highlights an area of need within the ADHD literature by focusing on the experiences of partners of adults diagnosed with ADHD, a topic often overlooked in traditional intervention models. Historically, intervention models designed for partners of adults with chronic health conditions have been predominantly patient-focused. For example, the ‘Spouse-Assisted Coping Skills Training’ model by Keefe et al. (1996) is primarily tailored to address the needs of the patient, which may inadvertently overlook the well-being of the partner. Such approaches may not fully address the relational tensions experienced by couples (Martire et al., 2010). There is, therefore, an emerging need for more inclusive intervention models that consider the well-being of both partners in the context of ADHD. For example, the collaborative model proposed by Tankha et al. (2020) for chronic pain treatment, which emphasizes emotional aspects of illness management, could be adapted to the context of ADHD.
Further research should also consider exploring other plausible explanations for the associations found, including the bidirectional nature of psychological distress and mutual influences within the relationship.
Limitations
This study provides valuable insights into the lives of women with ADHD-diagnosed partners; however, it is not without its limitations. The sample consisted exclusively of heterosexual women partners, and the data collection did not include information on gender, race, and ethnic identities, limiting the generalizability of our findings. The exclusion of same-sex relationships and cases where both partners have ADHD may lead to a biased interpretation, overlooking unique dynamics and challenges within these groups. We also did not consider other health conditions within the family, which are common in such dynamics and could influence partners’ experiences differently. Our focus was on women partners of men with ADHD, but there is also a need to study men partners of women with ADHD and include diverse representation of gender and ethnicity in order to understand the broader impact of ADHD on diverse couples.
The study’s cross-sectional design and reliance on self-reported measures present inherent limitations, such as the inability to infer causality and the potential for recall and social desirability biases. Moreover, we did not obtain corroborating evidence of prior ADHD diagnoses for the men partners, relying solely on self-reports, which may affect the validity of the findings. Additionally, the study did not differentiate between men diagnosed in childhood versus adulthood, which may be significant as literature suggests those diagnosed in childhood may experience more severe impairments if symptoms persist into adulthood. The use of an earlier version of the Adult ADHD Self-Report Scale (ASRS), due to its availability when the study commenced, could be considered a limitation, as the updated version includes DSM-5 criteria and offers improved screening accuracy. The educational levels of our participants were generally higher than typical levels in the general population of the recruitment area, which may affect the generalizability of our findings to populations with different educational backgrounds. Furthermore, the questionnaires were administered in Hebrew, excluding non-Hebrew speakers, such as those who speak Arabic, Russian, and Amharic, thus not representing these linguistic and cultural groups.
Finally, while the sample size was adequate for the analyses conducted, its relatively small scale may limit the robustness and broader applicability of the findings. Future research should seek to diversify participant demographics, implement longitudinal study designs, and use objective assessment tools alongside self-reports to better understand relationship dynamics when one or both partners are diagnosed with ADHD.
Conclusion and Recommendations
This study provides insights into associations between living with an ADHD-diagnosed partner and women’s mental health. The findings suggest that these women might be at an elevated risk for depressive symptoms, akin to that described in caregiver literature. However, it is important to note that the cross-sectional design of this study does not allow for causal conclusions, and other plausible explanations for these associations should be considered. Further longitudinal research is needed to examine the direction of these associations and to develop targeted interventions that support both individuals with ADHD and their partners.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.