
Abstract
Background:
Recent work highlights the role of emotion dysregulation in the pathology of Attention-Deficit/Hyperactivity Disorder (ADHD). As such, emotion-related impulsivity (ERI), the trait-like tendency toward disinhibited thoughts (Pervasive Influence of Feelings, PIF) and actions (Feelings Trigger Action, FTA) during heightened emotional states, may be particularly relevant. We explored whether Inattention (IN) and Hyperactivity/Impulsivity (HI), two core symptom dimensions of ADHD, would relate to distinct facets of ERI, and whether externalizing and internalizing symptoms would moderate these relations.
Method:
Using structural equation modeling, we examined hypotheses among 364 adults recruited for high internalizing and externalizing symptoms.
Results:
We identified significant paths for FTA regressed on HI and PIF regressed on IN, supporting our hypotheses about main effects. Moderating paths were not significant.
Conclusions:
IN and HI correlate with distinct forms of ERI, These effects appear to generalize across co-occurring internalizing and externalizing symptoms. Theoretical and clinical implications are discussed.
Attention Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterized by age-atypical inattention, hyperactivity, or impulsivity that causes impairment in multiple settings and begins before age 12 (American Psychiatric Association, 2013). ADHD symptoms and impairment often persist into adulthood, with approximately half of children with ADHD continuing to meet diagnostic criteria as adults (Kessler et al., 2010) and well over half experiencing continuing impairment (Sibley et al., 2022). Manifestations of ADHD may change over the lifespan, as hyperactive and impulsive symptoms often decline across development (e.g., Kessler et al., 2010; Mick et al., 2004). In contrast, inattentive symptoms are more likely to persist across time and to be linked with impairment in adulthood (Kessler et al., 2010; Vitola et al., 2017). Overall, between 2.1% and 4.4% of the adult population meets diagnostic criteria for ADHD (Kessler et al., 2006; Vitola et al., 2017).
Adult ADHD diagnoses are associated with negative outcomes across important life domains (Hinshaw et al., 2022). Adults with ADHD are less likely to graduate from high school or college, less likely to be employed, and more likely to report workplace impairment (Biederman, Faraone, et al., 2006; Küpper et al., 2012). Psychosocial problems are also linked with ADHD (Moyá et al., 2014), along with lower basic and instrumental functioning (Kessler et al., 2006). Even subsyndromal adult ADHD symptoms are associated with poorer well-being (e.g., Owens et al., 2017), including lower life satisfaction (Oerbeck et al., 2019), poorer quality social relationships (Das et al., 2012), and more frequent tobacco and marijuana use (Upadhyaya & Carpenter, 2008). Jointly, this literature indicates that even subsyndromal ADHD symptoms are associated with marked negative repercussions in adulthood (see also Sibley et al., 2022).
The negative consequences associated with ADHD arise, in part, from the poor inhibitory control and related impulsivity believed to be core to the disorder (Barkley, 1997). In both self-report and behavioral measures, adults with ADHD show high attentional, motor, and cognitive impulsivity (Malloy-Diniz et al., 2007) and report frequent engagement in impulsive behaviors such as reckless driving, overspending (Bernardi et al., 2012), and unplanned pregnancy (Owens et al., 2017).
Impulsivity related to emotional arousal may be particularly important in the pathology of ADHD (Faraone et al., 2019; Hirsch et al., 2018). Researchers have theorized that ADHD is specifically related to difficulties with emotional impulsivity and emotion dysregulation (e.g., Barkley, 2015; Faraone et al., 2019). In the context of ADHD, emotional impulsivity entails difficulty in controlling one’s responses to emotion-related and evocative stimuli, whereas emotion dysregulation involves difficulty down-regulating emotion following affective arousal (Faraone et al., 2019). These designations align well with facets of the transdiagnostic construct of Emotion-Related Impulsivity (ERI), defined by the tendency to engage in regrettable speech, behavior, and unconstrained cognitions during either positive or negative emotional states (Carver et al., 2011). One well-validated measure of ERI is the Three Factor Impulsivity Index (TFI, Carver et al., 2011). It includes two factor-analytically distinct subscales which capture variants of ERI (Feelings Trigger Action [FTA] and Pervasive Influence of Feelings [PIF]). The former measures the tendency to respond reflexively to emotion states; the latter consists of items related to failure to constrain cognition and motivation in the face of emotions. A third subscale (Lack of Follow Through [LOFT]) captures impulsivity without regard to emotion states.
In studies of children and adults, ADHD diagnoses and symptoms have been tied to higher scores on measures of Negative Urgency and Positive Urgency, which are components of FTA (e.g., Miller et al., 2010; Mitchell et al., 2012). Although the relation between ADHD and this form of ERI has been established, Faraone et al. (2019) argue that this association may differ based on ADHD subtype (or “presentation”). In particular, the hyperactive/impulsive symptom dimension appears related to high emotional impulsivity, whereas the inattentive dimension may be more specifically related to challenges with emotion dysregulation. Individuals with the combined subtype, who display both symptom dimensions, may experience dysregulation in both aspects of emotion experience.
Despite theory, studies linking ERI with specific ADHD symptom dimensions have yielded mixed results (e.g., Christian et al., 2020; Daurio et al., 2018; Ducey, 2016). These mixed findings for specific symptom dimensions may be partially due to disparate patterns of comorbidity across samples. ADHD commonly co-occurs with many internalizing and externalizing psychiatric syndromes (Kessler et al., 2006). Among adults, ADHD is related to a two-fold increase in rates of substance use and externalizing disorders relative to the general population (e.g., Biederman, Monuteaux, et al., 2006; Kessler et al., 2006). As for internalizing conditions, up to 60% of adults with ADHD have a lifetime history of anxiety and/or mood disorders, a rate considerably higher than that found in the general population (e.g., Bernardi et al., 2012). Comorbidity predicts poorer outcomes and greater disability among those with ADHD (e.g., Fredriksen et al., 2014; Sobanski et al., 2007). Thus, it is crucial to better understand the contributors to and consequences of these high rates of comorbidity.
ERI may be particularly relevant to comorbidity in the context of ADHD. For example, among adults with ADHD, Negative and Positive Urgency are tied to alcohol symptoms and alcohol dependency (Daurio et al., 2018; Pedersen et al., 2016), suggesting that those with ADHD and comorbid externalizing symptoms may experience uniquely high ERI. Although the broader literature suggests that ERI is elevated among those with high anxiety and depressive symptoms (Dekker & Johnson, 2018; Johnson et al., 2013), this has not been tested among those with ADHD.
In sum, although ADHD symptoms have been linked with elevated levels of some forms of ERI, several gaps remain unaddressed. To the best of our knowledge, researchers have not conjointly considered the effects of multiple facets of ERI on ADHD, internalizing, and externalizing symptoms within the same model. Thus, we aimed to examine how three forms of impulsivity relate to inattentive and hyperactive/impulsive ADHD symptoms, while considering main and moderating effects of co-occuring internalizing and externalizing symptoms. Based on prior work and theory connecting inattention to emotion dysregulation specifically, we hypothesized that inattention would correlate with PIF. Theory and prior findings highlight the association between hyperactivity/impulsivity and emotional impulsivity, which maps onto the construct of FTA. Thus, we hypothesized that hyperactivity/impulsivity would relate to FTA. We further anticipated that both inattention and hyperactivity/impulsivity would relate to LOFT, an emotion-unrelated form of impulsivity. Previous research outside of ADHD indicates that the FTA subscale is more closely related to externalizing symptoms, whereas PIF is more closely linked with internalizing symptoms (Johnson et al., 2013, 2017). Therefore, we hypothesized that internalizing would relate to PIF and that externalizing would relate to LOFT and FTA, both directly and as moderators.
We examined these questions in a large sample of adults recruited for a broad range of internalizing and externalizing symptoms. We hypothesized the following:
(1) Inattentive, hyperactive/impulsive, and externalizing symptoms will each correlate with LOFT.
(2) Inattentive and internalizing symptoms will each correlate with PIF.
(3) Hyperactive/impulsive and externalizing symptoms will each correlate with FTA.
(4) Internalizing symptoms will amplify (moderate) the relation between inattention and PIF.
(5) Externalizing symptoms will amplify (moderate) the relation between hyperactivity/impulsivity and FTA and between hyperactivity/impulsivity and LOFT.
Method
Sample
The study took place at two sites, one in the Western United States and the other in the Southeastern United States. Procedures were approved by the IRB at each institution before data collection. Participants were recruited using flyers, online advertisements, public service announcements, and referrals from outpatient treatment providers. Participants were financially compensated for their participation using standard payment rates at each site.
Participants completed a phone interview to assess preliminary eligibility criteria. Eligible participants were aged 18 to 55 years. Most experienced functional impairment due to mental health symptoms (subscale score of ≥5 on the Sheehan Disability scale or receiving government disability payments tied to mental illness) or had seen a mental health provider at least once in the preceding 6 months. Additional participants without current functional impairment (as defined previously) were included so that a full range of functioning was available for analyses.
Exclusion criteria included cognitive impairment (>5 mistakes on the Orientation Memory Concentration Test; Katzman et al., 1983), head trauma with lasting effects or loss of consciousness for >5 min, use of daily antipsychotic medication or other sedating medication, medical conditions/treatments that would confound diagnosis (e.g Cushing’s syndrome, dementia, or interferon treatment), language difficulties or vision problems that would prevent completion of study procedures, and receipt of electroshock therapy in the past year. In addition, we excluded those with alcohol use disorder or substance use disorder within the last 6 months, a lifetime primary psychotic episode, or a lifetime manic episode as assessed with the Structured Clinical Interview for DSM-5 (SCID-5, described below). A subset of participants also completed MRI scans and fulfilled standard inclusion criteria for fMRI.
Those who failed more than half of the attention checks embedded in self-report questionnaires (n = 3), who failed to complete key measures for analyses (n = 14), and/or who were later deemed ineligible for the study (n = 2) were excluded. A final sample of 364 participants was used for analysis (Mage = 29.1, SDage = 9.9, Range 18–55). Of these participants, 68.7% identified as female, 29.1% as male, and 1.6% with another gender identity. Racially, 52.2% of participants were Caucasian, 18.1% were Asian, 1.1% were Native Hawaiian/Pacific Islander, 11.8% were Black or African American, 12.9% identified with more than one race, and 1.6% declined to answer questions about racial identity. Ethnically, 29.7% identified as Latinx/Hispanic. Demographic and DSM-5 diagnostic information are reported in Table 1.
Demographics.
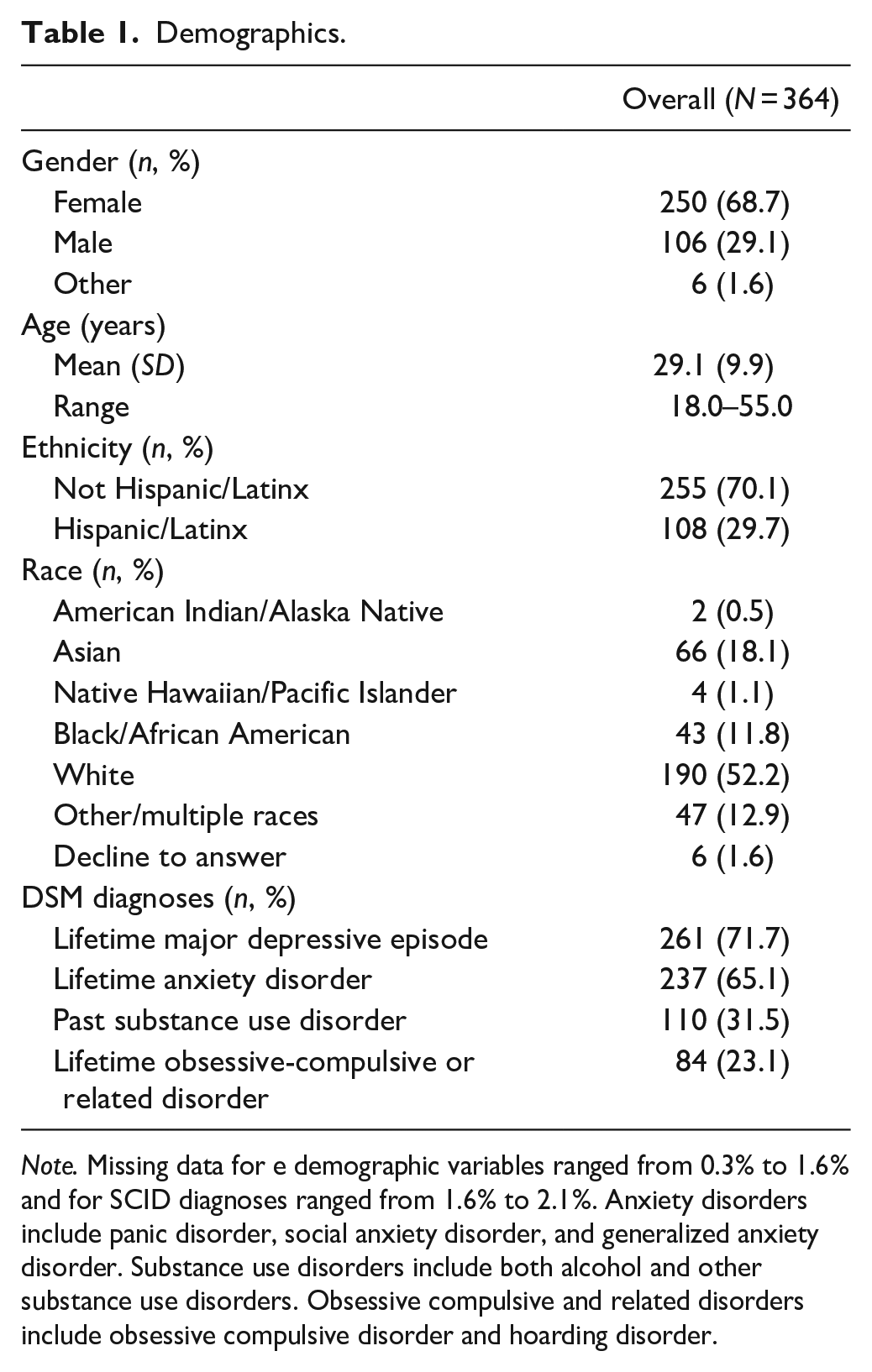
Note. Missing data for e demographic variables ranged from 0.3% to 1.6% and for SCID diagnoses ranged from 1.6% to 2.1%. Anxiety disorders include panic disorder, social anxiety disorder, and generalized anxiety disorder. Substance use disorders include both alcohol and other substance use disorders. Obsessive compulsive and related disorders include obsessive compulsive disorder and hoarding disorder.
Procedures
Participants who met inclusion criteria were invited to complete a clinical diagnostic interview. Sessions were conducted in-person before March 2020 and over HIPAA-compliant Zoom afterwards because of the COVID-19 pandemic. The Structured Clinical Interview for the DSM-5 (SCID-5; First et al., 2015) was used to assess current and lifetime diagnoses of psychotic and substance use disorders (for exclusion criteria) as well as internalizing and externalizing disorders. After the diagnostic interview, participants completed self-report questionnaires online using Qualtrics. These assessed internalizing and externalizing symptoms, ADHD symptoms, and ERI. Participants then completed behavioral and/or neuroimaging sessions, which are beyond the scope of the present project. Detailed information about relevant study procedures can be found elsewhere (e.g., Johnson et al., 2022).
Measures
The Orientation Memory Concentration Test (Katzman et al., 1983) was used to measure cognitive impairment. This validated assessment shows high correlations with other measures of cognitive functioning (e.g., Tombaugh & McIntyre, 1992). Participants are asked to state the current year, month, and time; count backwards; state the months in reverse order; and repeat a phrase told to them earlier. Unweighted scores range from 0 to 12, with higher scores indicating a greater number of errors.
The Sheehan Disability Scale (Leon et al., 1997) was used to assess functional impairment in three domains (work/school, social, family) related to mental health symptoms in the worst month of the past 6 months. Impairment due to symptoms was rated from 0 to 10 for each domain. A score of ≥5 in one domain is validated as a threshold for significant functional impairment (Williams, 2008).
The Structured Clinical Interview for DSM-5 (SCID-5; First et al., 2015) is a semi-structured interview assessing current and past diagnoses of psychopathology according to DSM-5 diagnostic criteria. Before interviewing participants, interviewers were trained to administer the SCID-5 using didactic instruction, sample interviews, review of interview tapes, and evaluation of reliability of ratings against gold standard tapes. Throughout the study, interviewers attended reliability meetings to prevent rater drift. There was substantial diagnostic agreement between raters (92%; κ = .79).
The Mood and Anxiety Symptoms Questionnaire (MASQ, Clark & Watson, 1991) is a self-rated measure of anxiety and depressive symptom severity. We used the 30-item version of the MASQ, which has shown high correspondence with interview-based measures of symptoms (e.g., Lin et al., 2014), and adequate construct validity well as internal consistency (Wardenaar et al., 2010). Each item was rated on a 5-point Likert scale from 0 (not at all) to 4 (extremely), with higher scores indicating greater symptoms. Anhedonia, anxious arousal, and general distress subscales were formed by summing 10 items each. Subscales were averaged to obtain a total MASQ score.
The Adult ADHD Rating Scale version 1.1 (ASRS v. 1.1, Kessler et al., 2005) is an 18-item measure of self-reported inattentive and hyperactive-impulsive ADHD symptoms among adults. Each item is rated on a five-point scale with responses ranging from 0 (Never) to 4 (Very Often), with higher scores indicating more severe ADHD symptoms. Continuous rather than dichotomous scoring was used on each item to retain statistical power (Cohen, 2013). The ASRS has considerable reliability and validity as a measure of ADHD symptoms among adults (Adler et al., 2006). Consistent with prior work (e.g., Gjervan et al., 2014), separate subscale scores for Inattentive (IN) and Hyperactive-Impulsive (HI) symptoms were created by summing scores on 9 items each. In this sample, internal consistency was good: standardized Cronbach’s alphas were .87 and .80, respectively (Gliem & Gliem, 2003).
The 160-item Externalizing Spectrum Inventory—brief form (ESI, Patrick et al., 2013) was designed to assess externalizing symptoms of callous aggression, substance abuse, and general disinhibition. Items are each rated on a four-point scale ranging from 0 (False) to 3 (True). Higher scores indicate greater externalizing symptoms. Scores on individual items were summed to form a total ESI score. This scale has been chosen as the recommended HiTOP measure of externalizing symptoms based on its strong psychometric characteristics (HiTOP Friendly Measures, 2022).
The Three Factor Impulsivity Index (TFI, Carver et al., 2011) contains three factor-analytically derived subscales: Feelings Trigger Action (FTA), Pervasive Influence of Feelings (PIF), and Lack of Follow Through (LOFT). The former two are forms of ERI. The latter is a form of impulsivity believed to be unrelated to emotion. This factor structure has been replicated (e.g., Auerbach et al., 2017). The FTA subscale contains items from the Urgency Scale (Whiteside & Lynam, 2001), Positive Urgency Measure (Cyders et al., 2007), and Reflexive Reactions to Feelings Scale (Carver et al., 2011). The PIF subscale contains items from the Generalization Scale (Johnson et al., 2013), Sadness Paralysis Scale (Carver et al., 1988), and Emotions Color Worldview Scale (Carver et al., 2011). The LOFT subscale contains items from the Lack of Perseverance Scale (Whiteside & Lynam, 2001) and the Distractibility Scale (Carver et al., 2011). Each item was rated on a 5-point Likert scale, with responses ranging from 1 (“I agree a lot”) to 5 (“I disagree a lot”). Subscale scores were calculated from the mean of subscale items. ERI scores have been shown to correlate with psychopathology, including depression, bipolar disorder, suicidal ideation and behavior, and self-harm, as well as trauma and serotonergic functioning, more robustly than the LOFT subscale (e.g., Carver et al., 2011; Johnson et al., 2017, 2022).
Data Analytic Plan
All methods and analyses were pre-registered. Analyses were conducted in R (version 4.0.5) with α = .05 (two-tailed). Confirmatory Factor Analyses (CFAs) and Structural Equation Models (SEMs) were conducted using the Lavaan package (Rosseel, 2012). Before model estimation, all indicators were rescaled (to 0–10). Mean substitution was used for single missing values when scoring subscales. For CFAs and SEMs, Full Information Maximum Likelihood (FIML) was used to account for missing data, and all variables were z-standardized.
Four measures of model fit were used, per recommendations by Hu and Bentler (1999): (1) χ2 statistic with p > .05, (2) Comparative Fit Index (CFI) > .95, (3) Root Mean Square Error of Approximation (RMSEA) < .08, and (4) Standardized Root Mean Square Residual (SRMR) < .08 indicated adequate model fit. If models indicated poor fit, modification indices were used to explore potential sources of misspecification. Upon inspection, models were altered accordingly. Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) were used for model comparison. Smaller values indicate better model fit while penalizing for model complexity.
We conducted a CFA that aimed to replicate the structure of the TFI, published in other samples (e.g., Johnson et al., 2013). FTA was modeled as a latent factor derived from observed Urgency, Positive Urgency, and Reflexive Reactions to Feelings scores. PIF was modeled as a latent factor defined by observed Emotions Color Worldview, Sadness Paralysis, and Generalization scores. LOFT was modeled as a latent factor based on Lack of Perseverance and Distractibility scores. Externalizing (ESI total scores), Internalizing (MASQ total scores), and ASRS HI and IN were modeled as observed factors. Adjustments in the use of these indices are discussed in our pre-registration.
To test hypotheses, we examined an SEM with predicted main effects of IN, HI, internalizing, and externalizing symptoms on specific facets of FTA, PIF, and LOFT. In particular, FTA was regressed on externalizing symptoms and HI; PIF was regressed on IN and internalizing symptoms; and LOFT was regressed on IN, HI, and externalizing symptoms.
We then tested three moderators: externalizing symptoms as a moderator of the relation between HI and LOFT; externalizing symptoms as a moderator of the relation between HI and FTA; and internalizing symptoms as a moderator of the relation between IN and PIF. Significant moderation would be indicated by (a) improved model fit compared with the absence of the moderator and (b) significant regression paths between the moderator and the TFI dimensions. For our final model, we omitted nonsignificant paths to present the most parsimonious model possible.
Results
Descriptive statistics for study variables are reported in Table 2. As shown, lifetime rates of depression, anxiety, and substance use-related diagnoses were high (Table 1). Bivariate correlations among all variables are reported in Table 3. Coefficients, standard errors, and confidence intervals for final models are reported in Table 4. All coefficients are reported as standardized values.
Descriptive Statistics for Study Variables.
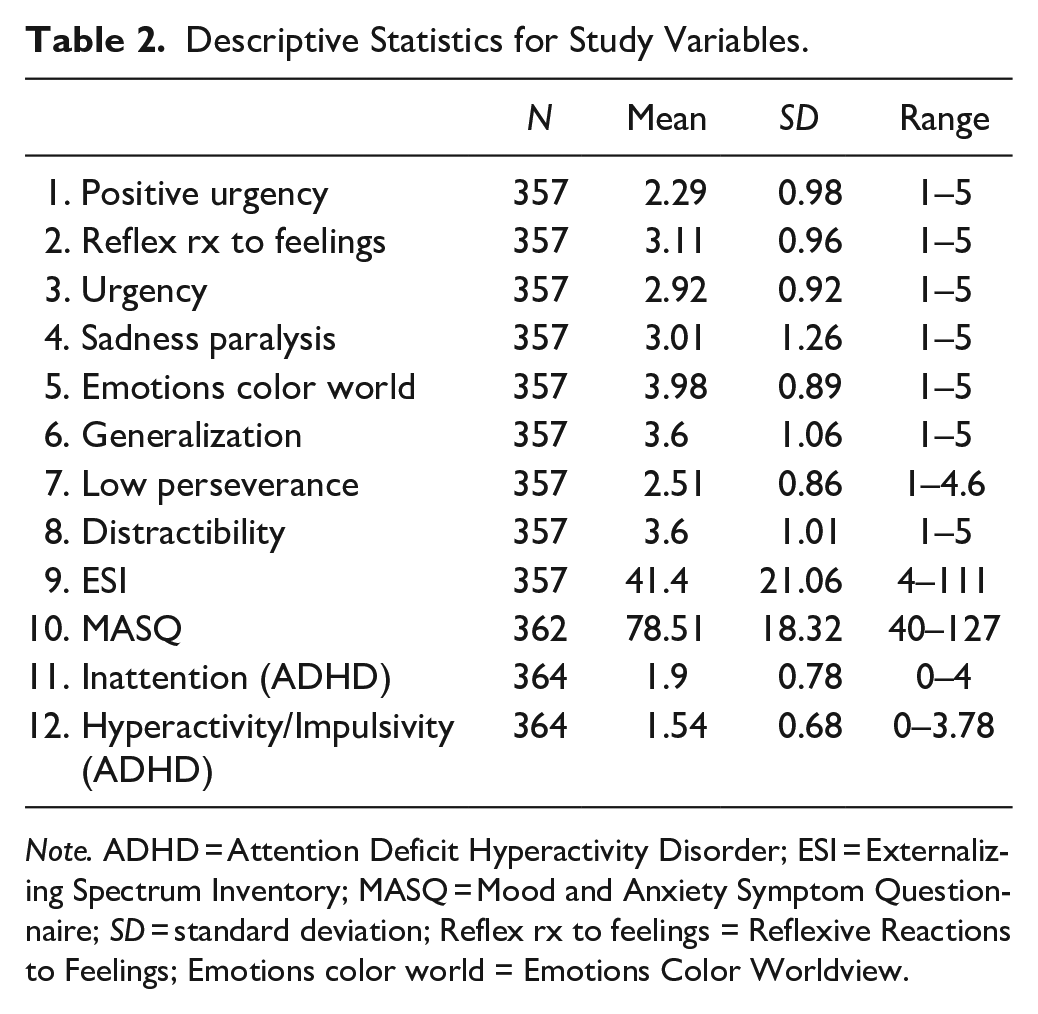
Note. ADHD = Attention Deficit Hyperactivity Disorder; ESI = Externalizing Spectrum Inventory; MASQ = Mood and Anxiety Symptom Questionnaire; SD = standard deviation; Reflex rx to feelings = Reflexive Reactions to Feelings; Emotions color world = Emotions Color Worldview.
Correlations Among Study Variables.
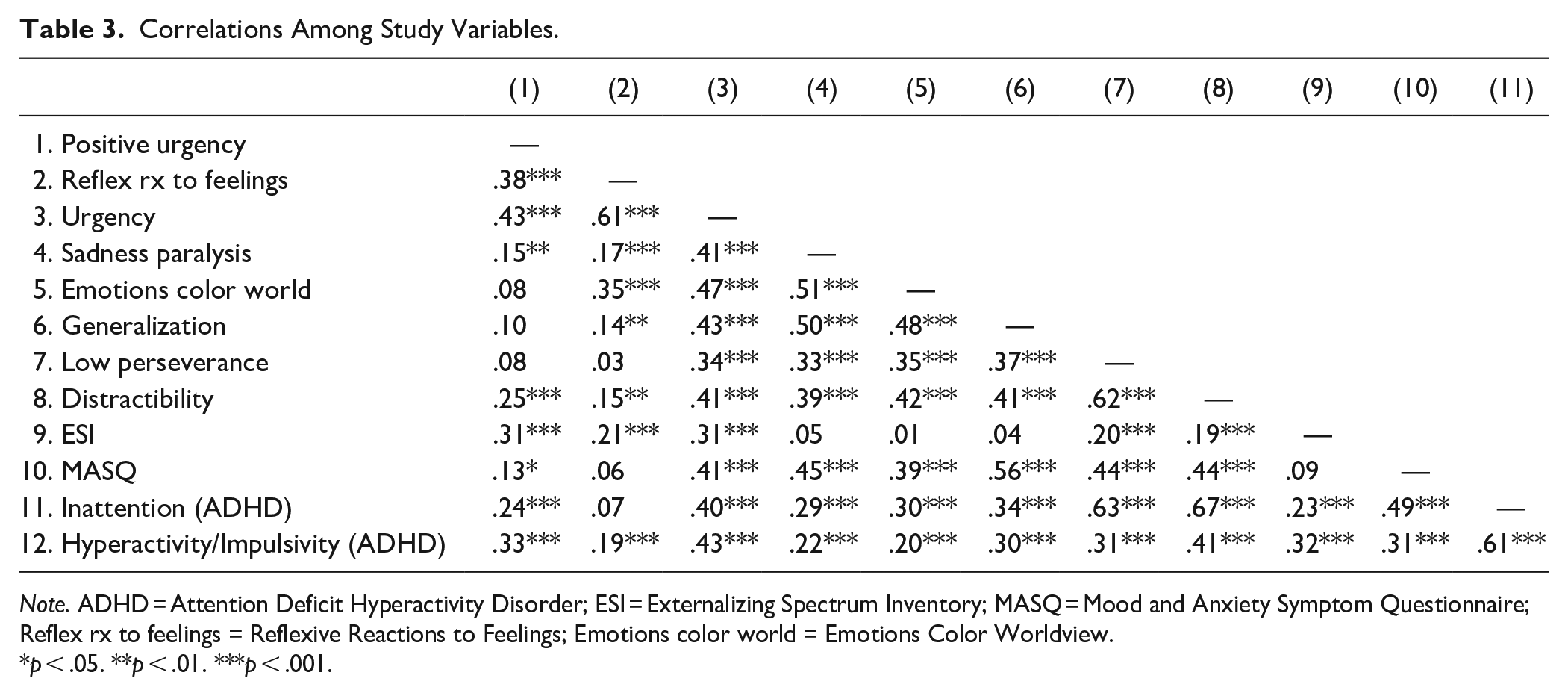
Note. ADHD = Attention Deficit Hyperactivity Disorder; ESI = Externalizing Spectrum Inventory; MASQ = Mood and Anxiety Symptom Questionnaire; Reflex rx to feelings = Reflexive Reactions to Feelings; Emotions color world = Emotions Color Worldview.
p < .05. **p < .01. ***p < .001.
Standardized Path Coefficients, Standard Errors (SE), 95% Confidence Intervals (CI), and Direct and Indirect Effects for the Main Effects Structural Model Tested.
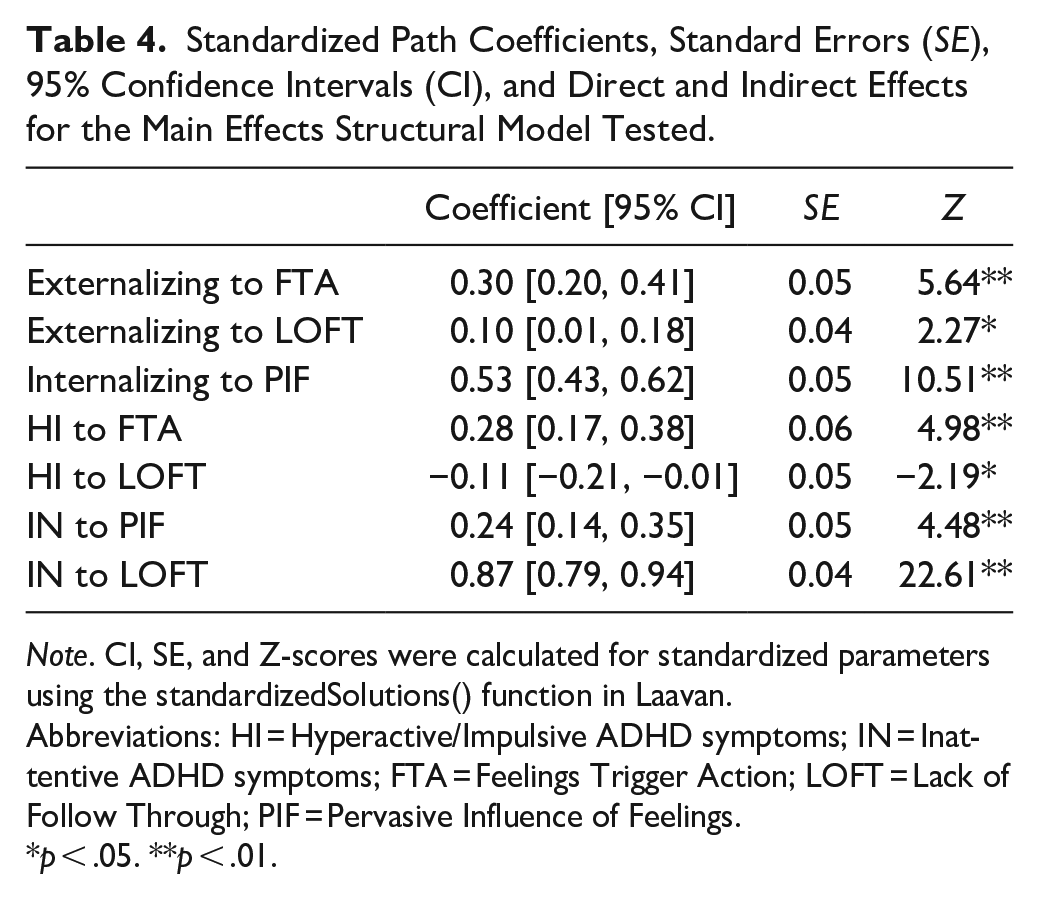
Note. CI, SE, and Z-scores were calculated for standardized parameters using the standardizedSolutions() function in Laavan.
Abbreviations: HI = Hyperactive/Impulsive ADHD symptoms; IN = Inattentive ADHD symptoms; FTA = Feelings Trigger Action; LOFT = Lack of Follow Through; PIF = Pervasive Influence of Feelings.
p < .05. **p < .01.
Measurement Model of Impulsivity
Following modification, the measurement model of impulsivity had good fit according to all indices (CFI = .98; RMSEA = .06, SRMR = .03), except the chi-square (χ2(15, N = 357) = 31.98, p = .006). Of note, χ2 is influenced by sample size, and is often significant in large samples (Schwab et al., 2011). Figure 1 depicts the measurement model following modification.
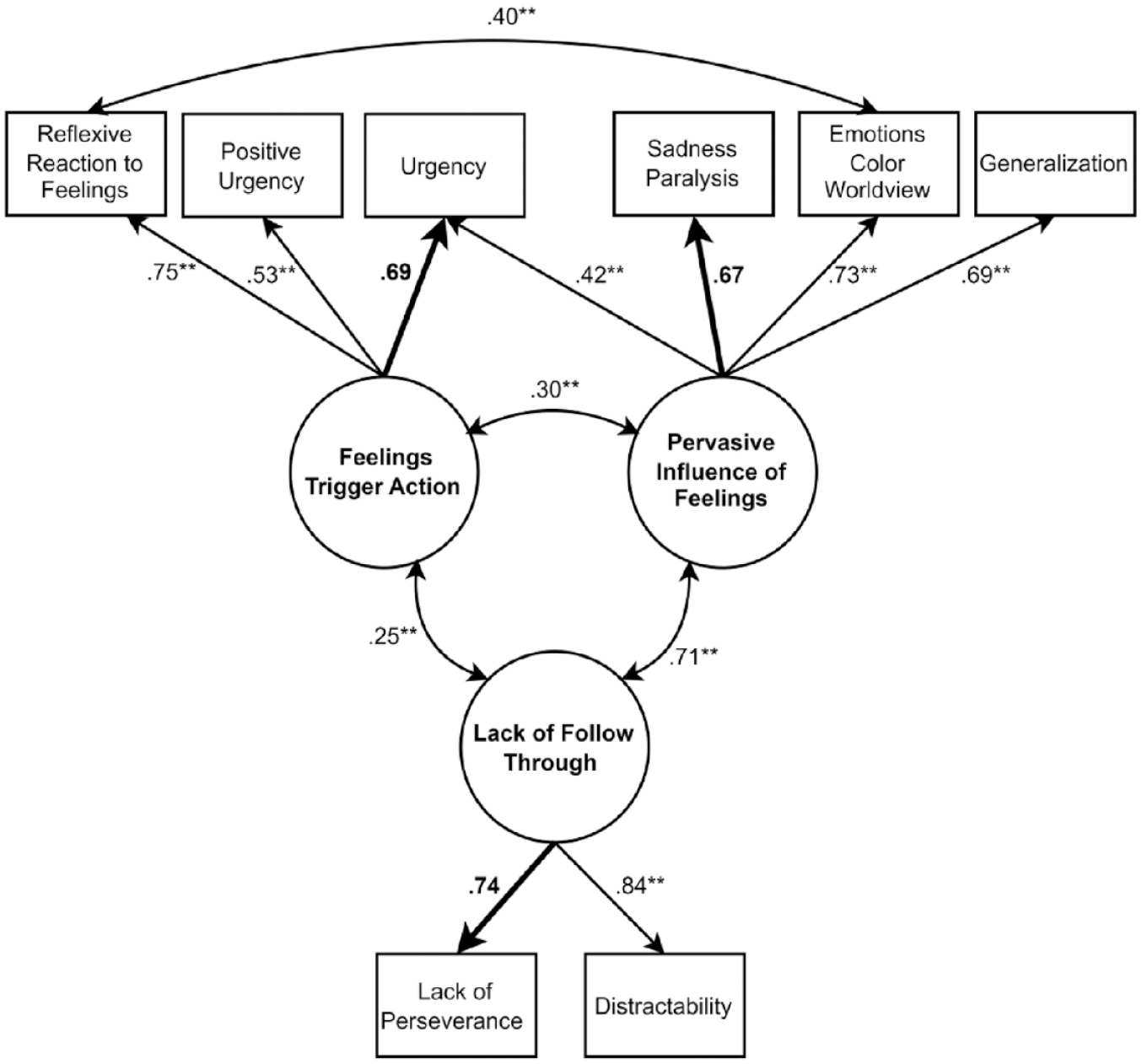
Measurement Model of the Three Factor Impulsivity Index.
Structural Models
The main effects structural model (see Figure 2) showed adequate fit according to the RMSEA and the SRMR (χ2(40, N = 356) = 116.27, p < .001, CFI = .945, RMSEA = .07, SRMR = .05). FTA regressed significantly on both HI (β = .28, p < .001) and externalizing symptoms (β = .30, p < .001), in line with predictions. LOFT regressed significantly on HI (β = –.11, p = .03), IN (β = .87, p < .001), and externalizing symptoms (β = .10, p = .03). The direction of the relation between HI and LOFT was opposite of our prediction, in that high HI symptoms predicted lower emotion-unrelated impulsivity. As hypothesized, PIF regressed significantly on both IN (β = .24, p < .001) and internalizing symptoms (β = .53, p < .001).
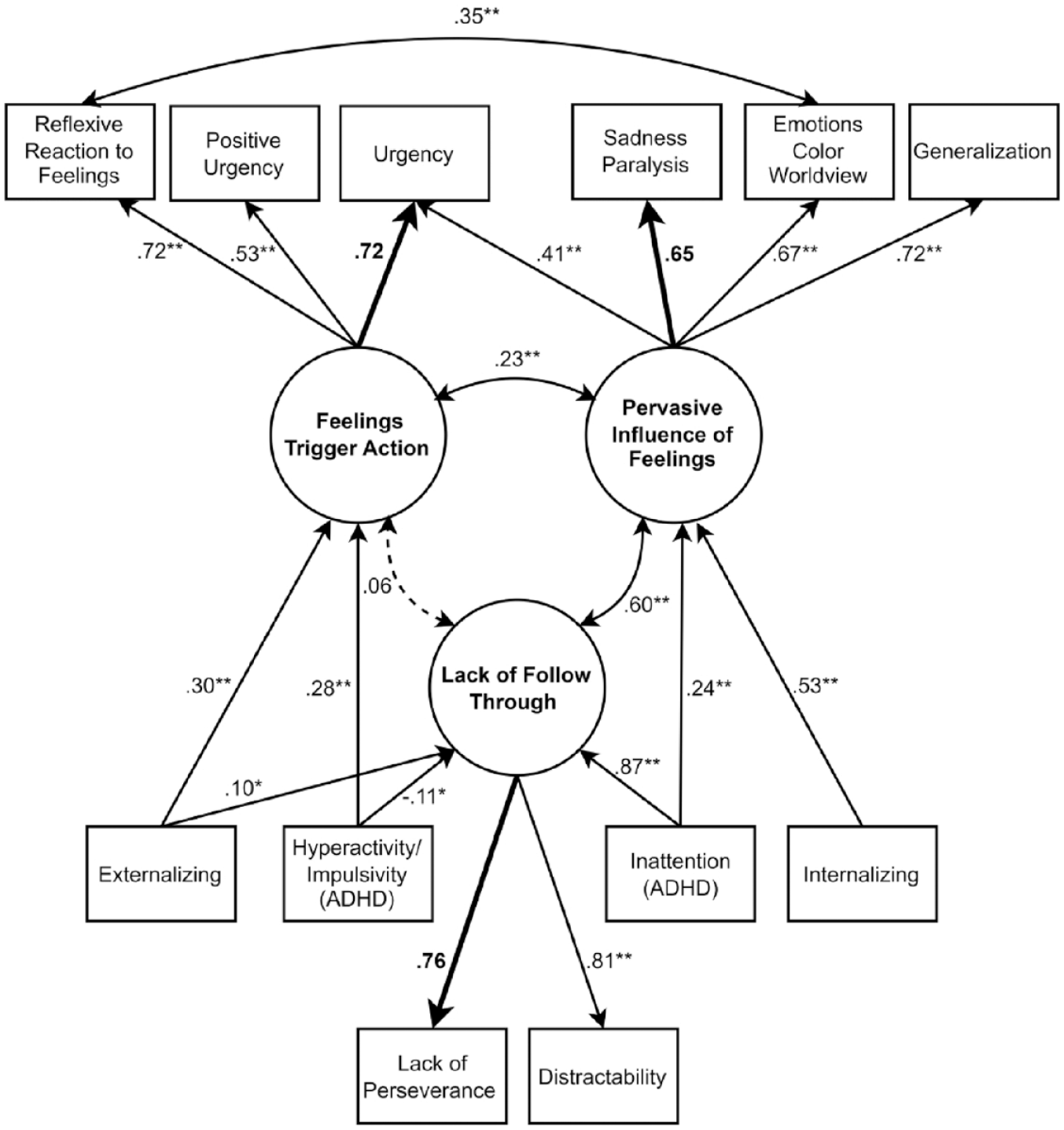
Main Effects Structural Model.
The full structural model, including moderation, had adequate fit according to the RMSEA and SRMR (χ2(53, N = 356) = 139.19, p < .001, CFI = .94, RMSEA = .07, SRMR = .05). There was no evidence that externalizing symptoms moderated the relation between HI and FTA (β = –.25, p = .20) or between HI and LOFT (β = .01, p = .96). Internalizing symptoms did not significantly moderate the relation between IN and PIF (β = –.23, p = .20). As well, the AIC and BIC were worse for the model with moderation (AIC = 11,968.20, BIC = 12,119.33) compared to that without (AIC = 11,965.49, BIC = 12,104.99). Accordingly, we decided to interpret the main effects model with no moderating paths (see Figure 2).
Discussion
We aimed to evaluate the associations between ERI and ADHD, internalizing, and externalizing symptom dimensions. We drew on an existing conceptualization of hyperactive/impulsive symptoms as related to heightened reactions to strong emotions and inattentive symptoms as related to difficulty returning to baseline after emotional arousal (e.g., Faraone et al., 2019). Our work is novel in considering two forms of ERI, one which involves impulsive action (FTA) and another which involves unconstrained thought and motivation (PIF). We drew on well-established links of these forms of impulsivity with internalizing and externalizing symptoms (Johnson et al., 2013, 2017) to hypothesize a novel model of how comorbid syndromes may moderate the relation between distinct facets of impulsivity and ADHD symptom dimensions. Critically we explored how FTA and PIF might conjointly relate to internalizing, externalizing, and ADHD symptoms in a large, well-characterized, transdiagnostic clinical sample.
Prior work has argued that hyperactivity/impulsivity is specifically tied to emotional impulsivity, or impulsive action while experiencing strong emotions (Faraone et al., 2019), which aligns with the construct of FTA. In contrast, inattention is thought to relate more closely with emotion dysregulation (also termed dysregulated emotional self-regulation), which instead reflects a prolonged internal experience of emotions (Faraone et al., 2019), mapping onto the construct of PIF. Interestingly, in parallel, hyperactive/impulsive ADHD symptoms are often characterized by actions (e.g., fidgeting, interrupting others, difficulty waiting one’s turn), whereas inattentive ADHD symptoms often reflect internal cognitive experiences (e.g., forgetfulness, distractibility, difficulty with sustained attention). Thus, our work extends prior theories on the link between ADHD and dysregulated emotional experiences by connecting these to specific facets of ERI.
We observed several patterns that were consistent with our hypotheses. Inattentive ADHD symptoms and internalizing symptoms both related to higher PIF, or lack of constraint over cognition and motivation in the face of heightened emotions. On the other hand, higher hyperactive/impulsive ADHD symptoms and higher externalizing symptoms related to higher FTA, or the tendency toward unconstrained speech and behavior in the face of heightened emotions.
In bivariate correlations, both inattention and hyperactivity/impulsivity were related to higher LOFT, or non-emotion-related impulsivity. Nonetheless, when examining inattention and hyperactivity/impulsivity conjointly, higher hyperactivity/impulsivity unexpectedly related to lower LOFT. Although the direction of this path was surprising, it reflects the unique variance of hyperactive/impulsive symptoms that does not overlap with other related constructs. Given the high bivariate correlations among variables, shared variance between predictors may well account for the counterintuitive relation between hyperactive/impulsive symptoms and LOFT. Alternatively, this may be an example of cooperative suppression (Paulhus et al., 2004).
Beyond examining direct links, we also explored whether comorbid internalizing and externalizing symptoms magnified the predictions from ADHD symptoms to respective facets of impulsivity. We expected moderation given that those with ADHD and comorbid conditions have considerably worse outcomes compared to those with each disorder on its own (e.g., Fredriksen et al., 2014; Gjervan et al., 2014). This sample was uniquely well-suited for such analyses, as data were drawn from a large transdiagnostic sample with a broad range of psychiatric conditions. We observed no significant moderation by comorbid internalizing or externalizing symptoms. Inattentive, hyperactive/impulsive, internalizing, and externalizing symptoms evidenced independent relations to their respective facets of ERI irrespective of the level of co-occurring symptoms and without any multiplicative effects. As such, each dimension of ADHD symptoms appears to predict ERI even when not accompanied by comorbid internalizing or externalizing symptoms. This pattern supports claims that challenges with emotion regulation may be part of the syndrome of ADHD, per se, rather than a unique facet of comorbid conditions (Barkley, 2015).
If replicated, findings may have clinical implications for the treatment of ADHD. Many existing therapeutic interventions for adult ADHD focus on executive functioning, with modules to improve organization, planning, and task breakdown (e.g., Langberg et al., 2008). In other populations, researchers have effectively implemented interventions that specifically target ERI, leading to success in addressing emotion dysregulation, impulsive responses to emotion, aggression, and self-harm (Johnson et al., 2020; Peckham & Johnson, 2018). If additional research replicates the unique association of inattentive and hyperactive/impulsive symptoms with PIF and FTA, respectively, targeting these forms of ERI could prove clinically useful in adults with ADHD.
Despite the strengths of this study, we note several limitations. Our sample size was sufficient to find large interactions, but we were underpowered to identify interactions that were smaller in magnitude. To avoid confounds in assessment, individuals with current substance use or alcohol use disorder were excluded, which may have truncated the highest levels of externalizing symptoms. Moreover, the exclusion of this subgroup may have interfered with our ability to fit conventional latent factor models of internalizing and externalizing symptoms, thus limiting our ability to use this modeling approach. In addition, our models were based on self-report data, which can be biased, as people may systematically under-report the severity of their symptoms and impulsivity. Still, these self-reported symptoms were highly related to SCID-based diagnoses in this sample. Finally, all symptoms were assessed in adulthood, and we do not have data on childhood ADHD symptoms. Although scores on the ASRS relate to impairment (e.g., Fredriksen et al., 2014) and show considerable validity (Adler et al., 2006), our design is unable to explore additional developmental questions, such as how the age of onset of symptoms affects relations with ERI. Given the neurodevelopmental nature of the disorder, future work should explore the relation between dimensions of childhood ADHD symptoms and ERI across the lifespan as well as how and if these associations change across time.
In summary, we found evidence that two dimensions of ADHD symptoms demonstrate differential associations with two forms of ERI in a large transdiagnostic sample of adults. Impulsive action following strong emotions was particularly related to hyperactivity/impulsivity, and poor constraint over negative thoughts and low motivation was particularly related to inattention. These effects generalized across levels of comorbid internalizing and externalizing symptoms, even when adjusting for the independent contributions of internalizing and externalizing symptoms to these forms of impulsivity. To our knowledge, this is the first study to explore the distinction between symptom dimensions of ADHD in the context of the Three Factor Impulsivity Index, a well-replicated measure of three forms of impulsivity. Our findings extend prior work by highlighting the role of distinct facets of emotion dysregulation in ADHD and provide a new potential direction for the development of clinical interventions for ADHD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health (grant number R01MH110477).