
Abstract
Objectives:
This study investigated the unique associations of motor competence and ADHD risk status on school functioning. Additionally, this study examined the factor structure of the Bruininks-Oseretsky Test of Motor Proficiency, Short Form (BOT2-SF).
Methods:
Participants included early elementary school children (N = 202, Mage = 6.83, SD = 0.96, Male = 53.5%, ADHD-risk = 46.5%). Child assessments of motor competence and teacher and parent reports of school functioning were used.
Results:
A two-factor model of the BOT2-SF with correlated fine and gross motor factors and correlated residuals best fit the data. Fine and gross motor competence were unique positive predictors of academic performance, after accounting for the effects of ADHD-risk on academic performance. ADHD-risk was the only unique predictor of adaptive school behavior.
Conclusion:
Findings suggest that assessing for ADHD and motor competence in children demonstrating school functioning problems may better allow for targeted intervention in school.
To receive a diagnosis of ADHD, a neurodevelopmental disorder defined by developmentally inappropriate levels of hyperactivity/impulsivity (HI) and/or inattention (IA), symptoms must contribute to functional impairment in more than one setting (American Psychiatric Association, 2022). School is one setting in which children with ADHD often display impairment. Specifically, higher levels of ADHD symptoms are associated with poorer grades and lower standardized test scores (Daley & Birchwood, 2010; Loe & Feldman, 2007). Compared to typically developing (TD) children, children with ADHD are also more likely to use academic services or be placed in special education classes (Biederman et al., 1996; Daley & Birchwood, 2010). Moreover, many children with ADHD exhibit lower levels of motor competence (i.e., inappropriate and inefficient control of fine and gross motor movements; Robinson et al., 2015), which in itself is associated with lower levels of school performance (for a review see Macdonald et al., 2018). Thus, children with ADHD and/or lower levels of motor competence may be at particular risk for impaired school functioning. It is unclear, however, whether motor competence uniquely contributes to school functioning (i.e., academic performance and adaptive school behavior) above and beyond ADHD-risk. The current study examines this in an early elementary-aged sample in which children were identified as at risk for ADHD or TD.
ADHD and Motor Competence
Motor activity is a component of several ADHD symptoms listed in the Diagnostic and Statistical Manual of Mental Disorders 5 TR (DSM-5 TR; i.e., fidgeting, running about or excessive climbing, acting as if “driven by a motor”; American Psychiatric Association, 2022). Although these behaviors suggest increased motor activity, evidence suggests that many children with ADHD have difficulty with motor control and/or show lower levels of motor competence. In fact, approximately 50% of children with ADHD meet criteria for Developmental Coordination Disorder (DCD; Farran et al., 2020; Kaiser et al., 2015; Pitcher et al., 2003), a movement disorder characterized by motor performance below the age-expected norm (American Psychiatric Association, 2022). Lower levels of both fine (i.e., the ability to make small muscle movements with the hands and wrists) and gross (i.e., the ability to make large muscle movements with the torso, legs, and arms) motor abilities have been observed in children with ADHD (for reviews see Demers et al., 2013; Emck et al., 2009; Kaiser et al., 2015).
Importantly, fine motor deficits in the areas of handwriting and tracking tasks have been observed in individuals with ADHD. For example, Langmaid et al. (2014) examined variability in handwriting strokes between children with combined-type ADHD and TD controls and found that children with ADHD showed more variability and inconsistency in stroke length and height than their TD peers. Similarly, when asked to complete a tracking task using a mouse cursor to trace an inner and outer circle, children diagnosed with ADHD performed significantly worse on accuracy and stability of movements than their TD peers (Slaats-Willemse et al., 2005). Additionally, children diagnosed with ADHD exhibit high rates of specific learning disorders with impairment in written expression (American Psychiatric Association, 2022). Fine motor deficits may impair the ability to manipulate a pencil or pen to write information integral to displaying knowledge in school (DeBono et al., 2012). In light of this, it is important to examine if fine motor competence deficits compound school functioning challenges in children with ADHD-risk.
Varying degrees of stability, accuracy, and consistency in gross motor skills have also been observed in children with ADHD (Tseng et al., 2004; Verret et al., 2010). For example, in a study of school-aged children in Taiwan, children with ADHD scored lower on gross motor skill subtests of running speed and agility, balance, and bilateral coordination compared to TD children (Tseng et al., 2004). Similarly, in a sample of school-aged boys, children diagnosed with ADHD scored lower on a locomotion subtest (comprised of motor skills such as, run, gallop, hop, leap, catch, kick) than TD children (Verret et al., 2010). These results are concerning given that motor competence is positively associated with physical activity (PA) in children, an important contributor to cardiorespiratory fitness and musculoskeletal fitness (for a review, see Cattuzzo et al., 2016). Importantly, given higher levels of PA are positively associated with academic performance (for a review, see Rasberry et al., 2011), children with lower levels of gross motor competence may be less likely to experience school functioning benefits related to PA. Therefore, it is also important to examine if gross motor competence compounds school functioning challenges in children with ADHD-risk.
ADHD, Motor Competence, and School Functioning
The relation between motor competence and school functioning in children with ADHD has received limited research attention (exceptions include Davis et al., 2009; Jelle Vuijk et al., 2011; Magistro et al., 2015; Palácio et al., 2016). Additionally, studies on this topic either examine associations between motor competence and school functioning in samples of children with ADHD, or they compare differences in motor competence and school functioning between children diagnosed with ADHD and TD children. For example, Jelle Vuijk et al. (2011) examined the relation between motor competence and academic performance in children with learning disabilities (16.8% of whom were diagnosed with ADHD). They observed that fine motor skills were positively associated with performance on spelling, whereas gross motor skills were positively associated with performance on reading and math (Jelle Vuijk et al., 2011). Davis et al. (2009) also observed a positive association between both fine and gross motor skills and academic achievement in children diagnosed with ADHD. Specifically, academic achievement was related strongly to grip strength, finger tapping, and bilateral coordination tasks. Although correlations between ADHD, motor competence and school functioning have been observed, there is a lack of work examining the unique associations of motor competence and ADHD-risk status on school functioning in the same model (i.e., while accounting for the overlapping associations of ADHD and motor competence). Therefore, this study examines the unique links between fine and gross motor competence and school functioning, after accounting for any associations between ADHD-risk status or the other focal motor competence variable and school functioning, in early elementary aged children.
Lower levels of motor competence are not only associated with school impairment in children with ADHD. Across the literature employing TD samples of children, motor competence deficits are linked with academic underperformance. A systematic review shows both fine and gross motor competence to be positively associated with academic performance in mathematics and reading (Macdonald et al., 2018). Yet, building on the work of Duncan et al. (2007), Grissmer et al. (2010) found that pre-kindergarten fine motor skills, but not gross motor skills, significantly predicted academic achievement in the fifth grade. Such findings emphasize the importance of examining the unique associations of motor competence with school functioning in a sample that includes TD children. Additionally, it is still important to examine the unique associations of both fine and gross motor competence with school functioning after accounting for impairment in school functioning due to ADHD-risk status and the non-focal motor competence predictor.
Significant relations between ADHD status, motor competence, and school functioning have not been observed in all studies. Palácio et al. (2016) examined correlations between motor performance and school performance in 110 early elementary school students in which half were diagnosed with ADHD and half demonstrated typical motor development. They found no significant associations between motor competence and any school performance measures of reading, writing, or arithmetic in the ADHD group. Additionally, there was only one significant correlation between manual dexterity and writing performance in the control group. Palácio and colleagues attributed their unexpected findings to differences from other studies in the measurement of school performance and potential lack of power to detect significant effects in their study. Therefore, it is important that investigations examining associations between ADHD, motor competence, and school functioning utilize larger samples and various assessments of school functioning. In the current study we utilized measures of both academic performance (i.e., how well a child is doing in specific subjects as rated by parents and teachers) and adaptive school behavior (i.e., adaptive functioning at school as rated by the child’s teacher).
Additionally, Palácio et al. (2016) work may have been limited by their measure of motor competence. Specifically, they utilized a measure of motor competence that only assessed manual dexterity, aiming and catching, and dynamic balance. Although both fine and gross motor competence are captured in these categories, other measures of motor competence such as fine motor integration skills (e.g., tracing, cutting) may be more related to school functioning. Therefore, in the current study we utilized a measure of motor competence that more broadly assessed both fine and gross motor competence.
Motor Competence Measurement
One widely used assessment of motor competence in young children is the Bruininks-Oseretsky Test of Motor Proficiency, Second Edition, Short Form (BOT2; Bruininks & Bruininks, 2005). The BOT2 is a 53-item comprehensive assessment of motor skills comprised of eight components of motor competence: three related to fine motor competence (i.e., fine motor precision, fine motor integration, and manual dexterity) and five related to gross motor competence (i.e., balance, bilateral coordination, running speed and ability, upper-limb coordination, and strength). Because the BOT2 is a performance-based measure, requiring the child to demonstrate a motor skill for each item, the full 53-item BOT2 is lengthy, taking considerable time to administer. Consequently, the BOT2 Short Form (BOT2-SF) was developed as a broadband screener of motor competence. Though the BOT2-SF was not developed to provide detailed feedback on fine and gross motor domains separately, the BOT2-SF is comprised of both fine and gross motor elements. Accordingly, Farran et al. (2020) split the BOT2-SF items into fine and gross motor components based on the type of motor category the item assessed on the full-form BOT2. However, they did not examine the two-factor structure of the BOT2-SF. Thus, we examined the factor structure of the BOT2-SF as proposed by Farran et al. (2020) to determine if distinct fine and gross motor components emerged.
Current Study
Our preliminary aim was to conduct an investigation into the factor structure of the BOT2-SF. Using the fine and gross motor scales proposed by Farran et al. (2020), we examined one and two factor models of the BOT2-SF items and evaluated fit statistics and factor loadings to determine which model best fit the data. We hypothesized that a two-factor model would best fit the data.
The primary aim of this study was to determine whether motor competence uniquely predicts school functioning after accounting for ADHD-risk status. Importantly, past studies examining the relations between ADHD, motor competence, and school functioning only examined academic achievement as an indicator of school functioning (Jelle Vuijk et al., 2011; Palácio et al., 2016). We expanded on this past work to include teacher reports of students’ adaptive school behavior (i.e., behavior, work ethic, ability to learn, and happiness), another critical component of school functioning. ADHD is known to be associated with poorer performance in school (Daley & Birchwood, 2010; Loe & Feldman, 2007), therefore, we predicted that children identified as ADHD-risk would have lower academic achievement and adaptive school behavior scores than TD children. Additionally, given that motor competence has been found to be positively associated with school performance (Grissmer et al., 2010; Harrowell et al., 2018), we hypothesized that fine and gross motor competence would be unique predictors of school functioning, even after accounting for ADHD-risk status and the other focal motor competence variable. Specifically, we predicted that higher levels of fine and gross motor competence would be linked with higher levels of school functioning.
Methods
Participants
Baseline data from 202 early elementary school children, originally recruited as part of a randomized controlled trial investigating the effects of a before school PA program on ADHD behaviors (see Hoza et al., 2015), were utilized in this study. The age of the children ranged from 4.44 to 8.90 years old (Mage = 6.83, SDage = 0.96, 53.5% male, 46.5% ADHD-risk). Parents reported the racial identities of children represented in this sample as follows: 68.3% identified their children as White, 14.4% as multiracial, 7.9% as Black, 2.0% as Asian, and 7.4% as another race.
Measures
ADHD-Risk Status
ADHD-risk status was determined as part of the two-step eligibility screening process in the original intervention study (Hoza et al., 2015). At step 1, after providing informed consent, parents and teachers completed the ADHD-IV Rating Scale (DuPaul, 1991), an age and gender-normed scale of DSM-IV symptoms of ADHD. Those children at or above the 90th percentile for parent or teacher ratings of HI or total symptoms were eligible for secondary screening for the ADHD-risk group. Those children below the 90th percentile on both parent and teacher ratings of HI, IA, and total symptoms were eligible for secondary screening as potential TD children.
At Step 2, parents attended an in-person screening to complete additional study measures to establish final eligibility for the ADHD-risk and TD groups. Children being screened for the ADHD-risk group were identified as ADHD-risk based on the following criteria: (a) parent endorsement of at least five HI symptoms on the ADHD module of the National Institute of Mental Health Diagnostic Interview Schedule for Children (DISC-IV; Shaffer et al., 2000) or at least three HI symptoms on the DISC-IV and two non-overlapping teacher-reported HI symptoms on the ADHD-IV rating scale and (b) reported impairment in two or more domains by parents and/or teachers on the Impairment Rating Scale (Fabiano et al., 2006), or the DISC-IV. For children being screened for the TD group, they were eligible if their parent endorsed four or fewer HI symptoms and four or fewer IA symptoms.
Children in both the ADHD-risk and TD groups were also required to have a non-verbal, verbal, or total IQ score no less than 1.5 SD below the mean (i.e., standard score ≥78) on the Kaufman Brief Intelligence Test, Second Edition (KBIT-2; Kaufman & Kaufman, 2004); no current diagnosis of pervasive developmental disorder, intellectual disability, or a seizure disorder; no medical condition that would restrict participation in PA; not currently on medication for attentional or behavioral issues; have lived with their current caretaker for at least 6 months; and have at least one English-speaking caretaker with telephone access.
Motor Competence
Motor competence was measured using the BOT2-SF (Bruininks & Bruininks, 2005). The BOT2-SF consists of 14-items and was developed to represent all eight subtests included in the full BOT2 53-item form. Five items are related to fine motor ability and nine are related to gross motor ability (Bruininks & Bruininks, 2005).
The BOT2-SF was administered by a trained graduate student or research assistant. Prior to administration of the BOT2-SF, the child’s hand and foot preferences were determined (i.e., having the child draw a line, pick up and throw a tennis ball, and kick a ball). Motor competence was evaluated by examining the five fine motor items followed by the nine gross motor items in the following order: drawing a line through paths-crooked (path), folding paper task (fold), copying a square (square) and star tasks (star), transferring pennies task (pennies), jumping in place-same side synchronized (jump), tapping feet and fingers-same side synchronized (tapping), walking forward on a line (walk), standing on one leg on a balance beam-eyes open (balance), one-legged stationary hop (hop), dropping and catching a ball-both hands (drop), dribbling a ball-alternating hands (dribble), knee pushups and full pushups (pushup), and sit-ups (sit-up). Higher scores indicate better motor abilities.
School Functioning
Academic performance measures were taken from the school subscale of the Child Behavior Checklist (CBCL) and the academic performance item of the Teacher Report From (TRF) from the Achenbach System of Empirically Based Assessments, (ASEBA; Achenbach & Rescorla, 2001).
The CBCL is a parent report of child behavior across multiple domains. The CBCL school subscale is comprised of four items that represent academic performance. One item asks parents to rate on a 4-point Likert scale from 0 (Failing) to 3 (Above Average) how well their child does in each subject the child takes. The others inquire about special education services (i.e., “does your child receive special education or remedial services or attend a special education class”), grade repetition (i.e., “has your child repeated any grades”), and academic or other problems in school (i.e., “has your child had any academic or other problems in school”), using yes (0) or no (1) questions with queries if the parent answers “yes.” The ratings of how well the child is doing across academic subjects are averaged and added to the special education services, grade repetition, and academic problems items. Higher scores indicate higher academic performance (Achenbach & Rescorla, 2001).
The TRF is a teacher report of child behavior across multiple domains. This study utilized the TRF academic performance item which asks teachers to list the student’s academic subjects and rate their performance on each using a 5-point Likert scale from 1 (far below grade) to 5 (far above grade). An average score is calculated across academic performance items with higher scores indicating higher academic performance (Achenbach & Rescorla, 2001).
The TRF adaptive functioning subscale was used as a measure of adaptive school behavior. The TRF adaptive functioning subscale is comprised of four items related to a child’s ability to work hard (i.e., “how hard is he/she working”), behave (i.e., “how appropriately is he/she behaving”), and learn (i.e., “how much is he/she learning”), as well as the teacher’s perception of the child’s overall happiness (i.e., “how happy is he/she”). The working hard, behaving, learning, and happy items ask teachers to compare the student to their same aged peers and rate performance on a 7-point Likert scale from 1 (much less), to 7 (much more), (Achenbach & Rescorla, 2001). A raw score is calculated by summing the scores across the four adaptive functioning questions. Higher scores indicate greater adaptive functioning. The TRF adaptive functioning subscale demonstrated good reliability in this sample, α = .82.
For each subscale score used from the CBCL and TRF, raw scores were converted into T-scores based on sex and age. Parent and teacher reports of academic performance and teacher reports of adaptive school behavior were collected during the second step of the eligibility screening process and at a time that would allow ample time for the teachers to assess each child’s performance.
Demographic Data
Participant age, sex, and race demographic information were collected from parent reports.
Data Analysis
The lavaan package, version 0.6-9 (Rosseel, 2012) in R (R Core Team, 2017) was used to conduct preliminary confirmatory factor analyses (CFA). A one-factor CFA was utilized to examine model fit of a one-factor solution of the BOT2-SF and a two-factor CFA, based on the subscales proposed by Farran et al. (2020), was utilized to examine and compare model fit of a two-factor model of motor competence with correlated fine and gross motor factors. Model fit was evaluated using the comparative fit index (CFI), Tuker-Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Criteria used to evaluate good model fit were as follows: CFI and TLI values of 0.95 or greater, RMSEA value less than or equal to 0.06, and SRMR value less than or equal to 0.08 (Hu & Bentler, 1999).
Following CFA analyses, data were analyzed using SPSS software version 27. Hierarchical multiple regression analyses were used to identify the unique effects of ADHD-risk and motor competence on the measures of school functioning (academic performance as reported by teacher and parent, respectively, and adaptive school behavior).
Results
Preliminary Data Analysis
Across all 202 children, four were missing at least one motor competence test. Therefore, the robust full information maximum likelihood estimator (FIML) was used in CFA analyses, which produces robust fit statistics, standard errors, and chi-square test statistics and is the suggested method for conducting analyses with missing data (Schafer & Graham, 2002).
Two original CFAs were conducted to determine the best model fit. Indicator variable correlation coefficients are presented in Table 1. All indicators were freely estimated. Additionally, to ensure model identification, the factor variance(s) were constrained to 1.00.
Intercorrelations of BOT2-SF Indicator Variables.
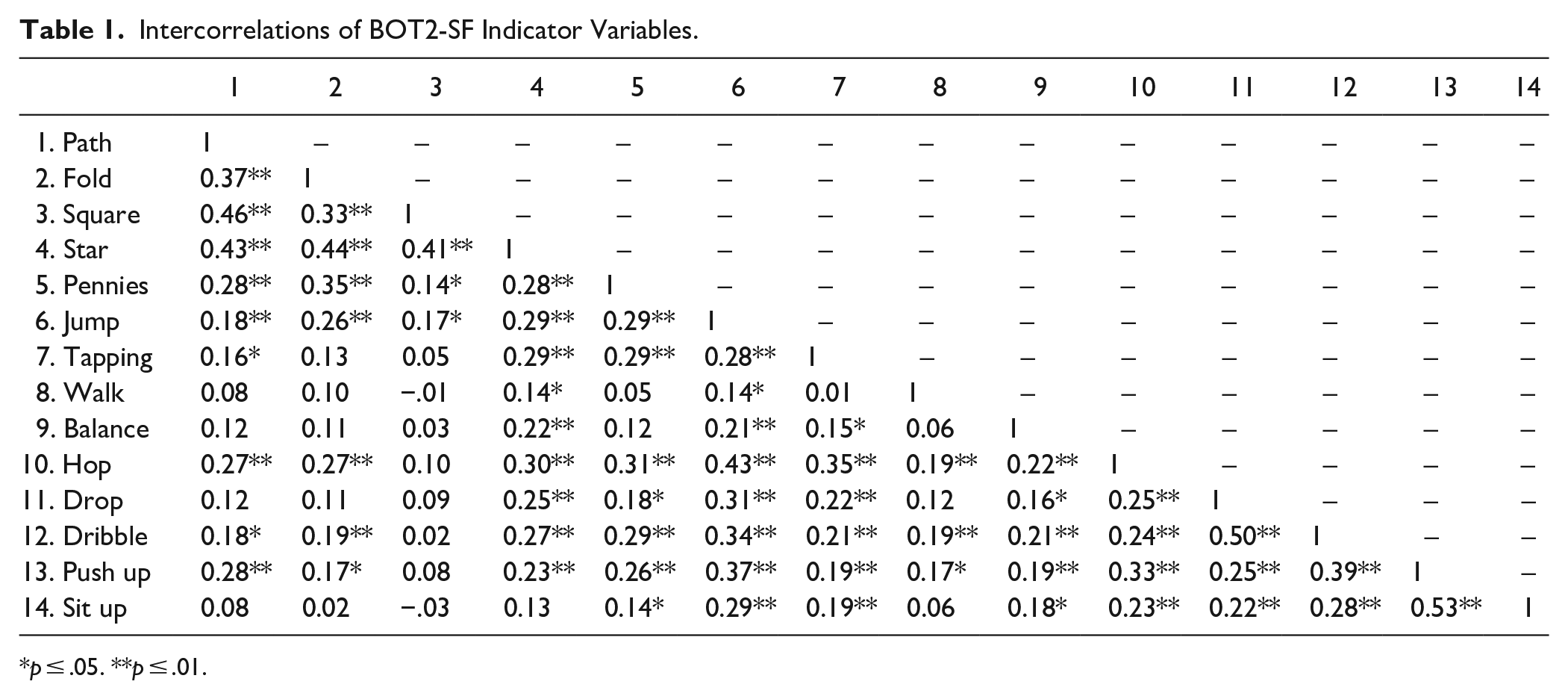
p ≤ .05. **p ≤ .01.
Model fit of the one-factor CFA with all 14 fine and gross motor indicator items loading onto a single factor of total motor competence was poor (CFI = 0.73, TLI = 0.69, robust RMSEA = 0.10, CI [0.08, 0.11], SRMR = 0.08). All factor loadings were significant; however, factor loadings for three indicator variables were lower than 0.40, suggesting weaker loading onto the factor.
To determine if loading the 14 items onto their respective fine and gross motor factors fit the data better, a two-factor CFA was conducted. Fine and gross motor factors were estimated to covary. Model fit of the two-factor solution was mixed (CFI = 0.87, TLI = 0.85, robust RMSEA = 0.07, CI [0.05, 0.08], SRMR = 0.07). Additionally, all standardized factor loadings were significant. Two item loadings were smaller than 0.40, indicating poor association of those items with the gross motor factor.
Given the mixed fit of the two-factor solution, modification indices were examined. Modification indices suggested that the indicator variable residuals be correlated for those indicator items from the same subscale of the full BOT2. Therefore, two follow-up CFAs were conducted to reflect this suggestion (see Table 2 for factor loadings and standard errors). Model fit of the one-factor CFA with correlated residuals was adequate (CFI = 0.89, TLI = 0.86, robust RMSEA = 0.06, CI [0.04, 0.08], SRMR = 0.06). Model fit of the two-factor solution with correlated residuals was good (CFI = 0.96, TLI = 0.95, robust RMSEA = 0.04, CI [0.01, 0.06] SRMR = 0.05). Additionally, all standardized factor loadings were significant across both models. The chi-square difference test comparing the fit between the one- and two-factor models with correlated residuals was significant, χ2 diff (1) =26.44, p < .001, suggesting that the two-factor model with correlated residuals fit the data better than the one-factor model with correlated residuals (Satorra & Bentler, 2001).
Unstandardized and Standardized Factor Loadings and Standard Errors of BOT2-SF Indicator Variables.
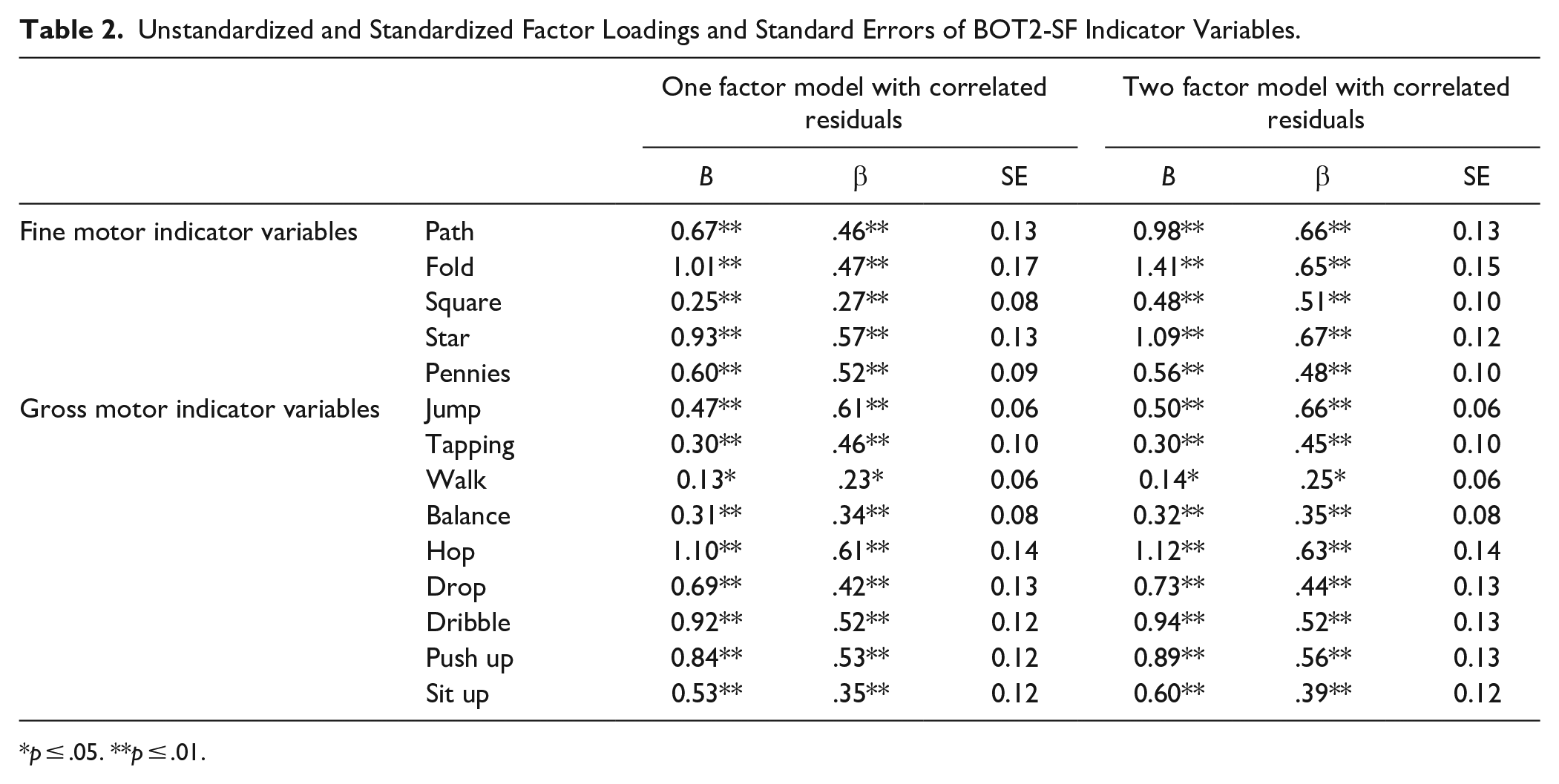
p ≤ .05. **p ≤ .01.
Given the results of the CFA, primary analyses utilized separate fine and gross motor subscales of the BOT2-SF. Specifically, fine and gross motor total raw scores were calculated by summing the scores on the five fine motor tasks and nine gross motor tasks, respectively, following procedures by Farran et al. (2020). Internal consistency reliability estimates in this sample were sufficient for the fine motor, α = .71, and gross motor, α = .74, subscales.
Regression Models
Hierarchical multiple regression analyses were used to identify the unique effects of ADHD-risk and fine and gross motor competence on the three measures of school functioning. Since raw motor competence scores were used, child age and sex were entered as covariates at Step 1, ADHD-risk status (1 = TD, 2 = ADHD-risk) was entered at Step 2, and fine and gross motor competence were entered at Step 3.
Data were missing across 12 study variables with no more than 2.5% of data missing for any one variable. Results of the Little’s Missing Completely at Random (MCAR) test were not significant, χ2 (108) =106.34, p = .53, indicating the data was MCAR. Given that data was MCAR, listwise deletion was used in SPSS throughout analyses with n’s ranging from 191 to 202.
Correlation coefficients were calculated to determine linear associations between ADHD-risk status, motor competence, school functioning, and demographic variables (see Table 3). There was a significant negative association between ADHD-risk status and fine motor competence, academic performance, and adaptive school behavior, suggesting that the children in the ADHD-risk group scored significantly lower than the TD group on fine motor competence and all school functioning measures. There was not a significant association between ADHD-risk status and gross motor competence, suggesting that children in the ADHD-risk and TD groups did not significantly differ in levels of gross motor performance. Results also indicated that higher levels of fine and gross motor competence were significantly associated with higher levels of academic performance, but not adaptive school behavior. Finally, fine and gross motor competence were significantly associated with age. Specifically, being older was linked with higher levels of fine and gross motor competence. Fine motor competence, but not gross motor competence, was also significantly associated with sex such that girls had higher levels of fine motor competence than boys.
Means, Standard Deviations, and Intercorrelations Among Study Variables.
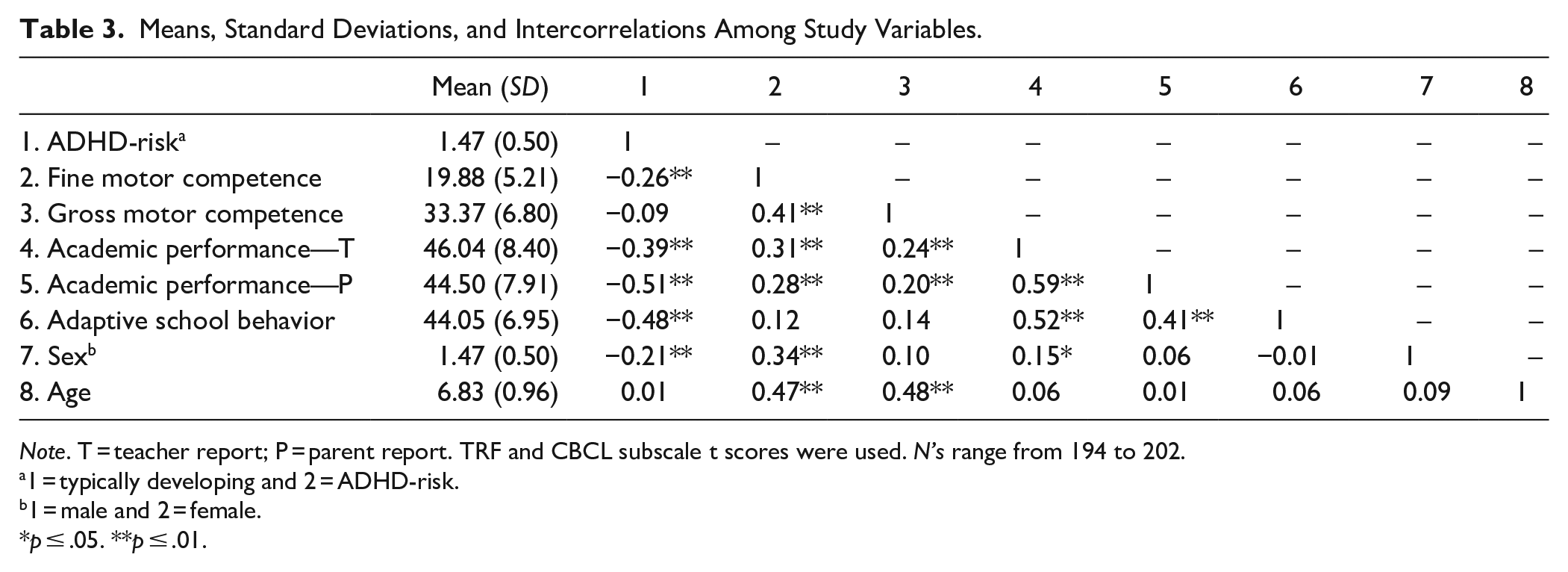
Note. T = teacher report; P = parent report. TRF and CBCL subscale t scores were used. N’s range from 194 to 202.
1 = typically developing and 2 = ADHD-risk.
1 = male and 2 = female.
p ≤ .05. **p ≤ .01.
Results of the regression analyses demonstrated that across models there were similar patterns of unique effects of ADHD-risk and motor competence on school functioning outcomes (Table 4). After adding ADHD-risk to the covariates at step 2 there was a significant change in R-squared and ADHD children exhibited less adaptive school behavior and lower academic performance than their TD peers. Then, at Step 3 in the model, ADHD-risk status was uniquely associated with all school functioning outcomes indicating that ADHD-risk children exhibited less adaptive school functioning than TD children after accounting for any associations between motor competence and school functioning. Additionally, at Step 3, fine and gross motor competence were both uniquely associated with teacher and parent reports of academic performance. Thus, over and above ADHD-risk status and the other focal motor competence predictor, higher levels of fine and gross motor competence were linked with higher levels of academic performance. Neither fine nor gross motor competence were uniquely associated with adaptive school behavior.
Associations of ADHD-Risk Status and Motor Performance With School Functioning.
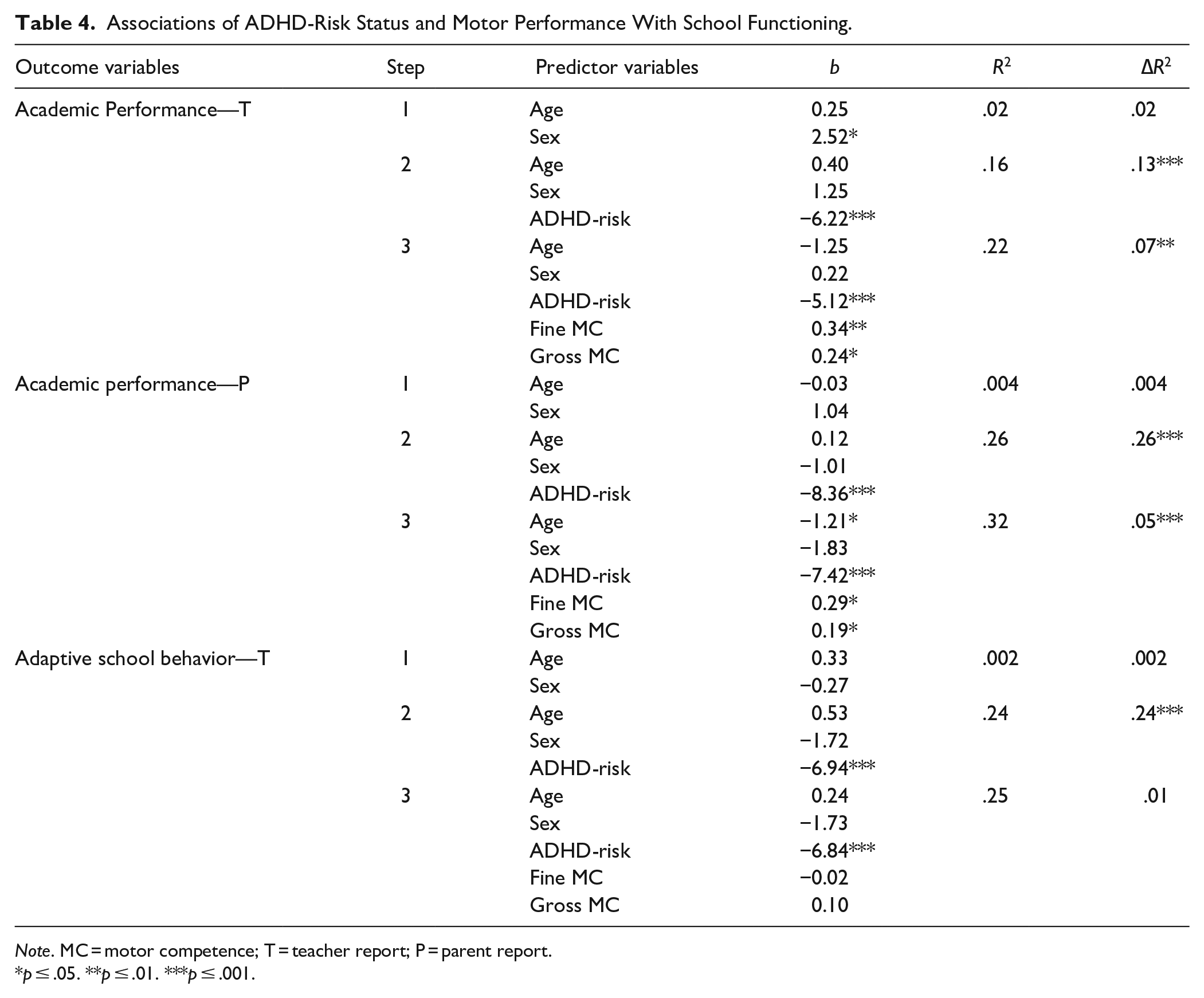
Note. MC = motor competence; T = teacher report; P = parent report.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Discussion
The preliminary aim of this study was to examine the factor structure of the BOT2-SF. Specifically, we examined if a two-factor solution for the BOT2-SF, splitting the fine and gross motor subscales as done by Farran et al. (2020), better fit the data than a one-factor solution. CFA fit statistics and chi-square difference test results determined that a two-factor model with correlated fine and gross motor factors and correlated residuals best fit the data. Given the results of the preliminary analyses, fine and gross motor competence were both entered as focal predictors in the regression models at step three. Being able to examine the unique relation between school functioning and motor competence separately for fine and gross motor competence is important given that some have found that fine and gross motor deficits are differentially associated with school functioning (Grissmer et al., 2010; Macdonald et al., 2018). Utilizing the BOT-SF as a measure of fine and gross motor competence allows evaluators to assess for fine and gross motor deficits more quickly than if they used the full BOT2. If an evaluator suspected impaired fine or gross motor competence after using the BOT2-SF they could then conduct additional assessments if needed to target specific deficits in these areas (e.g., deficits in fine motor precision or balance). Future research should examine the usability of the BOT2-SF as a screener for detecting lower levels of fine and gross motor competence in children.
The primary aim of this study was to determine whether fine and gross motor competence uniquely predict school functioning above and beyond ADHD-risk status. Our first hypothesis that ADHD-risk status would uniquely predict school functioning was fully supported. Across all hierarchical regression models, ADHD-risk status uniquely predicted academic performance and adaptive school behavior. Specifically, children identified as ADHD-risk were rated lower by parents and teachers on all ratings of academic performance and adaptive school behavior than their TD peers. This finding supports prior research on the relation between ADHD and school functioning (Daley & Birchwood, 2010).
Our second hypothesis that fine and gross motor competence would be unique positive predictors of school functioning, above and beyond ADHD-risk status and the non-focal motor competence variable, was partially supported. After controlling for ADHD-risk status and the non-focal motor competence variable, fine and gross motor competence were both positively linked with academic performance, but not adaptive school behavior. Prior research has demonstrated similar findings. For example, motor competence has been found to be positively associated with GPA in a TD sample (Batez et al., 2021). Thus, motor competence may be more closely related to academic performance than functional aspects of school performance (i.e., classroom behavior, work ethic, and ability to learn), after controlling for ADHD-risk. However, it could be that our measure of adaptive school behavior was unable to capture the wide range of functional skills underlying the constructs of classroom behavior, work ethic, and ability to learn. Specifically, the assessment of cognitive and executive functioning skills may be important to consider when assessing adaptive school behavior. Indeed, prior work has demonstrated that above ADHD severity, executive functioning was associated with worse academic performance and the ability to follow directions in school (Tamm et al., 2021). Future research should consider utilizing a measure of adaptive school behavior that includes additional skills that are important for success in the classroom (e.g., working memory, attention, inhibitory control).
These findings also suggest that it is important to consider the unique impact that both types of motor competence (i.e., fine and gross motor competence) may have on academic performance. Prior research has demonstrated similar findings in which higher levels of both fine and gross motor competence were uniquely associated with higher levels of academic performance in both mathematics and reading abilities (for a review see Macdonald et al., 2018). Additionally, research suggests that whereas fine motor competence is often more strongly associated with academic achievement, gross motor competence is more strongly associated with a child’s ability to engage in learning and social activities (Cameron et al., 2016). Therefore, both types of motor competence may play separate but related roles in promoting academic performance. Future research should continue to examine the unique and complementary roles of fine and gross motor competence in children’s academic performance.
Furthermore, given the robust literature examining the relation between ADHD and school functioning, the findings that fine and gross motor competence uniquely predict academic performance above ADHD-risk status have important clinical implications. Beyond experiencing high comorbidity rates with language disorders, dyslexia, and dysgraphia, children with DCD often experience decreased self-esteem, show reduced participation in play groups, and demonstrate higher levels of emotional disorders (Lino & Chieffo, 2022). Therefore, for children experiencing academic impairment, it could be beneficial to examine motor competence in addition to other typical assessments for learning or psychological disorders to gain a more comprehensive view of the child’s functioning. If lower levels of motor competence are observed, interventions targeting skills related to both fine and gross motor competence would be important to use, given both sets of skills are uniquely associated with academic performance.
It is important to note that contrary to prior research, preliminary correlational analyses indicated that ADHD-risk was not associated with gross motor competence. Specifically, children identified as ADHD-risk scored similarly in terms of gross motor competence as their TD peers. This finding is surprising because, although not everyone with ADHD will exhibit lower levels of motor competence, it is estimated that approximately 50% of individuals with ADHD experience impaired motor competence (Kaiser et al., 2015; Pitcher et al., 2003). CFA results demonstrated that some of the gross motor skills (i.e., walk and balance) did not load as strongly onto the gross motor factor as hopping on one foot. Thus, it could be that the gross motor items on the BOT2-SF were unable to measure aspects of gross motor functioning in which children with ADHD typically exhibit deficiencies, such as bilateral coordination (Tseng et al., 2004) and other more complex locomotion skills such as galloping or hopping (Verret et al., 2010). Therefore, future research should utilize motor competence measures that include a broader variety of gross motor skills.
In sum, the results of our study align with previous research in that ADHD-risk status uniquely predicted all aspects of school functioning examined in this study. Additionally, our results indicated that after accounting for ADHD-risk status and the other focal motor competence variable, fine and gross motor competence uniquely predicted academic performance but not adaptive school behavior. These results highlight the importance of screening for ADHD and motor competence deficits in school-aged children demonstrating school functioning problems. However, screening for motor competence in the early school years may be particularly important in children struggling academically. Research suggests that early identification of impaired motor competence in children, and consequently early intervention, is an effective way to buffer against problems associated with lower levels of motor competence (L. Lopes et al., 2020; McIntosh et al., 2000). One such intervention that has been shown to improve elementary aged children’s functional movement skills (i.e., locomotor, object control, and stability skills) is the Supporting Children’s Outcomes using Rewards, Exercise, and Skills intervention (SCORES; Cohen et al., 2015). Future research should examine how interventions like these contribute to long-term benefits of increased motor competence on academic achievement.
In light of our findings, it is important to consider interventions with the potential to simultaneously target ADHD behaviors and motor competence. Specifically, physical activity interventions have been shown to decrease ADHD behaviors (Hoza et al., 2015; Hoza et al., 2016) and increase motor competence (Zeng et al., 2017). Additionally, physical activity (including school-based physical activity) has been shown to benefit cognitive functioning and academic achievement in children of all ages (for reviews see Marques et al., 2018; Rasberry et al., 2011). Therefore, implementing a physical activity intervention in a school setting has the potential to benefit school functioning in all children, with especially meaningful benefits to children experiencing ADHD behaviors or lower levels of motor competence. Introducing such an intervention can occur within a school’s existing curricular framework. For example, participation in two or three physical education classes a week has been shown to increase motor skills (e.g., gymnastic skills, soccer skills, basketball skills, and handball skills) in elementary aged children (V. P. Lopes et al., 2017). More research is needed, however, to determine the long-term effects of physical activity on motor competence, ADHD behaviors, and school functioning.
Limitations
The findings of this study are not without their limitations. First, although the original study screened for and placed children into ADHD-risk and TD groups, a formal diagnosis was not required to be in the ADHD-risk group and symptoms of HI were emphasized over IA for inclusion. Therefore, findings from this study may not replicate in a sample of children with clinical diagnoses of ADHD or children with a predominantly IA presentation of ADHD. Second, although the two-factor model with correlated residuals better fit the data than the two-factor model without correlated residuals, modifications were necessary to increase model fit. It is recommended that to run a factor analysis, a sample of 10 subjects per indicator variable is required (Nunnally & Bernstein, 1967). Therefore, our sample of 202 met this criterion. However, future research should aim to replicate this study in similar sized or larger samples to better determine the appropriate factor structure for the BOT2-SF. Finally, the measure of adaptive school behavior may not have captured the functional skill deficits that lead to behavioral problems a student may exhibit at school. Therefore, future research examining school behavior should utilize a more extensive measure of adaptive school behavior and consider executive functioning deficits that can contribute to behavioral problems.
Conclusion
The results of this study suggest that lower levels of motor competence are linked with lower levels of academic performance, even after accounting for associated impairment due to ADHD-risk status. Therefore, for children with lower levels of academic performance, there is a need to increase early screening and intervention opportunities that target motor competence. Importantly, physical activity interventions can be implemented at a school-wide level and have been shown to benefit both motor competence and ADHD behaviors. Future research should examine whether increased physical activity is linked with increased academic performance through increased motor competence and decreased ADHD behaviors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute of Mental Health (R01MH082893 to B. Hoza & J. T. Green). The funding agency does not necessarily endorse the researchers’ findings and/or conclusions.