
Abstract
Objective:
In this study, to investigate the place of T cell-mediated immunity in the etiology of ADHD, for which we do not have enough information; we aimed to investigate the activity of DPP IV and ADA, which are T cell-related enzymes, and the relationship of these enzymes with ADHD symptoms in children with ADHD.
Methods:
Twenty-seven children aged 6 to 12 years with a diagnosis of attention deficit hyperactivity disorder and 27 children aged 6 to 12 years without any psychiatric disease were included in the study.
Results:
While serum ADA and DPP-IV activity were found to be statistically significantly higher in the group with ADHD. There was no statistically significant correlation between serum ADA and DPP-IV activities and CTRS-R-L and CPRS-R-L in both groups.
Conclusion:
We think that T cell mediated inflammation may play a role in the etiology of ADHD due to changes in ADA and DPP-IV levels in children.
Introduction
Attention Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder with attention problems, mobility and impulsivity (APA-American Psychiatric Association, 2013) The pooled prevalence of ADHD worldwide is 5.29% (Polanczyk et al., 2007). It is 3 to 9 times more common in boys than girls (Polanczyk & Rohde, 2007). Although the etiology of ADHD is not yet fully known, genetic, neurochemical, neuroendocrine, neuroimmunology, and environmental effects are held responsible (Millichap, 2008; Tripp & Wickens, 2009).
Adenosine deaminase (ADA) and dipeptidyl peptidase IV (DPP IV) are enzymes required for normal immune responses, involved in T cell activation and formation of cellular immunity (Yolaç Yarpuz et al., 2008). DPP IV is an exopeptidase enzyme that cleaves dipeptides originating mainly from T cells. It plays a key role in T cell-mediated immune response. Serum DPP IV levels reflect enzyme levels in T lymphocytes involved in cellular immunity (Elgün, Keskinege, Akan, et al., 1999). ADA is involved in T lymphocyte-monocyte development and functions (Da Cunha, 1991). ADA enzyme level increases during mitogenic and antigenic responses of lymphocytes. In addition, ADA is known as an ectoenzyme that interacts with DPP IV and some membrane proteins on the cell surface. This interaction of ADA and DPP IV generates costimulatory signals that lead to the activation of T cell receptors in T cells (Elgün et al., 2001).
ADHD shows high comorbidity with T cell-mediated humoral and cellular immunity disorders (Verlaet et al., 2014). Atopic diseases such as T cell-mediated hypersensitivity, asthma, rhinitis, and eczema were more common in ADHD patients than healthy controls (Fasmer et al., 2011; Schmitt et al., 2009). T cell-mediated cellular immunity can damage neuronal cells and cause ADHD through chronic T cell-mediated inflammation (Ceylan et al., 2012). In a study conducted; it has been suggested that T cell-mediated reactions in a group of children led to an imbalance in adrenergic activity in the central nervous system, resulting in ADHD symptoms (Marshall, 1989). Despite all this information, T-cell-mediated inflammation in ADHD has not been systematically investigated.
In summary; in this study, to investigate the place of T cell-mediated immunity in the etiology of ADHD, for which we do not have enough information; We aimed to investigate the activity of DPP IV and ADA, which are T cell-related enzymes, and the relationship of these enzymes with ADHD symptoms in children with ADHD.
Materials and Methods
Sample
A total of 54 children between the ages of 6 and 12 who applied to Ankara University Faculty of Medicine Child and Adolescent Psychiatry Outpatient Clinic were included in the study. The Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (K-SADS-PL) was applied to diagnose ADHD and exclude cases with other comorbid psychiatric disorders (such as psychotic disorders, bipolar disorder, tic, and behavioral disorders). Children who were determined to have autism spectrum disorder, language development delays, intellectual disability and learning disabilities in the clinical evaluation according to DSM 5 were not included in the study. In clinical interviews, Wechsler Intelligence Scale for Children (WISC-R) was applied to cases with suspected intellectual disability, and WISC-R and Learning Disorder Battery were applied to cases with suspected Specific Learning Disorder. While selecting the cases for the study, a total of 72 children were evaluated. Eight of them met the diagnostic criteria of specific learning disorder, 4 of them intellectual disability, and 6 of them were not included in the study because they met the diagnostic criteria of attention deficit, comorbid anxiety disorder and depression. The patient group consisted of children who were diagnosed with ADHD for the first time and did not receive medication, while the control group consisted of 27 healthy children in the same age group who applied to the Ankara University Faculty of Medicine Child Psychiatry Outpatient Clinic and did not have any psychiatric disorders.
Inclusion criteria for both groups; to be between the ages of 6 and 12, to be at a clinically normal level of intelligence, not to have chronic medical diseases such as pathologies affecting the immune system, allergic diseases and epilepsy, not to have used an infectious disease and related drugs in the last 1 week, and not to have entered puberty. HPA axis of hormonal changes experienced during puberty. Adolescent teenagers were not included in the study, considering the possibility that it may affect the ADA and DPP IV levels by changing it. To exclude possible medical diseases, the paediatrician performed clinical examinations of all children, and the results of routine laboratory tests were evaluated, including biochemical, haematology, and thyroid function measurements. None of the children was taking nutritional supplements such as antioxidants.
The study was approved by the Ankara University Faculty of Medicine Ethics Committee (08.05.2020 decision no: İ4-253-20). All families and children were informed verbally and in writing about the study and signed the informed consent form prepared in accordance with the rules set out in the Declaration of Helsinki.
Instruments
The sociodemographic information form, K-SADS-PL, the Conners Parent Rating Scale- Revised-Long Form (CPRS-R-L) for parents and the Conners Teacher Rating Scale Revised-Long Form (CTRS-R-L) for teachers were applied to the patients and the control group who were included in the study.
The sociodemographic information form is an information form prepared by us to obtain sociodemographic information about the child and the family before the semi-structured clinical interview “K-SADS-PL” and filled by the researcher by asking the parents.
Procedure
A K-SADS–PL interview was conducted with all children and their parents to diagnose and exclude accompanying psychiatric disorders. Parents were administered the CPRS-R-L and the teachers were administered the CTRS-R-L.
Venous blood samples in the amount of 10 mL were taken from the participants of both groups, who were approved to participate in the study, between 9:00 and 11:00 in the morning on a full stomach. Collected blood samples were centrifuged for 5 minutes at 3,500 × g relative centrifugal force to separate the plasma from the cells. After separation, the obtained plasmas were stored in Eppendorf tubes at −80°C until biochemical analysis. Measurement of serum DPP-IV activity was based on the spectrophotometric quantification of glycyl-prolyl-paranitroanilide hydrolysis and subsequent release of paranitroaniline. Absorbances were read at 385 nm. Results are expressed as IU/L. Measurement of serum ADA activity was based on assessing the formation of ammonia produced in a Berthelot reaction. Ammonia is generated when ADA reacts with adenosine (substrate). In the final chemical reaction, the formation of a blue color by indophenol was measured with a spectrophotometer at 628 nm. ADA enzyme activity is expressed as IU/L. Absorbance readings for all methods were performed on a Shimadzu UVmini-1240 device (UV-VIS spectrophotometer, Shimadzu Corporation, Kyoto, Japan). Serum DPP-IV and ADA activities were studied at Ankara University Medical Faculty Hospital, Medical Biochemistry Laboratory. All chemicals were purchased from Sigma Chemical. Serum ADA and DPP IV activities were measured spectrophotometrically and the results were given in IU/L.
Statistical Analysis
After the data were obtained, statistical evaluations were made in the SPSS (Statistical Package for Social Sciences) 22.0. Shapiro-Wilk test was used to test whether the variables obtained from the data were suitable for normal distribution. Mann-Whitney U test was applied for age from sociodemographic data, ADHD and control groups’ Conners Teacher and Parent form total scores and subscale scores. In a comparison of WISC-R scores, a t-test was used because the data showed normal distribution. Fisher’s Exact test was used for the gender parameter.
Mann-Whitney U test was used to compare the ADA activity of the ADHD and control groups, and the independent sample t-test was used because the DPP IV parameter was normally distributed. The Spearman Correlation test was applied to the data to examine the relationship between the ADA and DPP IV activities of the ADHD and control group with the scales. The statistical significance level (p) was accepted as .05.
Results
There was no significant difference between ADHD (n = 27) and Control (n = 27) groups in terms of age (9.19 ± 2; 9.7 ± 1.9, respectively) (p > .05). Gender distribution was similar between groups (p > .05) (Table 1). Patients and controls did not differ significantly in parents’ education and income levels, or any medical condition or adverse life events. Likewise, no significant difference was found between the groups in terms of delivery type or presence of trauma, surgical operation, and seizures in the postpartum period. In addition, there was no difference in terms of drug supplement use by children, allergic diseases in children, and psychiatric disease history in parents.
Sociodemographic Characteristics of Patients and Controls.
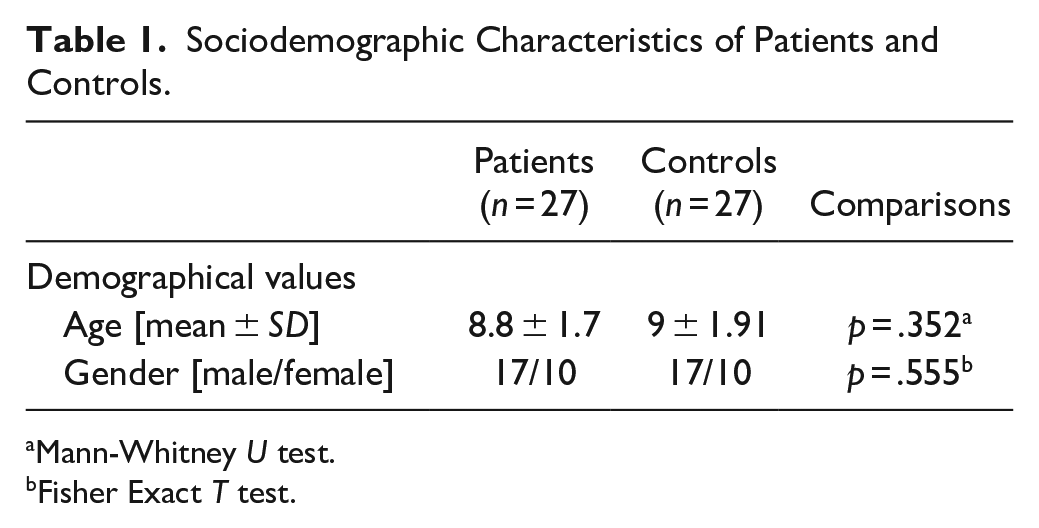
Mann-Whitney U test.
Fisher Exact T test.
There was no significant difference between the total intelligence scores of the children in the ADHD and Control groups who underwent WISC-R (p > .05). The patient group scored high on the CTRS-R-L and the CPRS-R-L.
Serum ADA and DPP IV distributions are shown in Figures 1 and 2. Serum ADA and DPP IV activities of the patients were significantly higher than the control group (Table 2). No correlation was found between serum ADA and DPP IV activities, and the subscales and total scores of the CTRS-R-L and the CPRS-R-L.
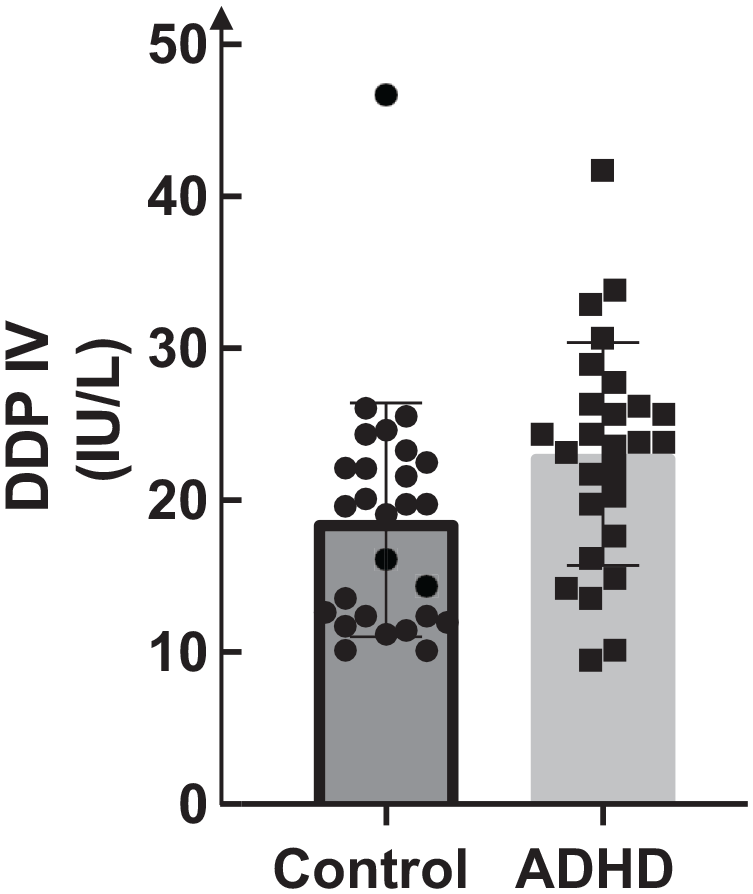
DPP IV distribution.
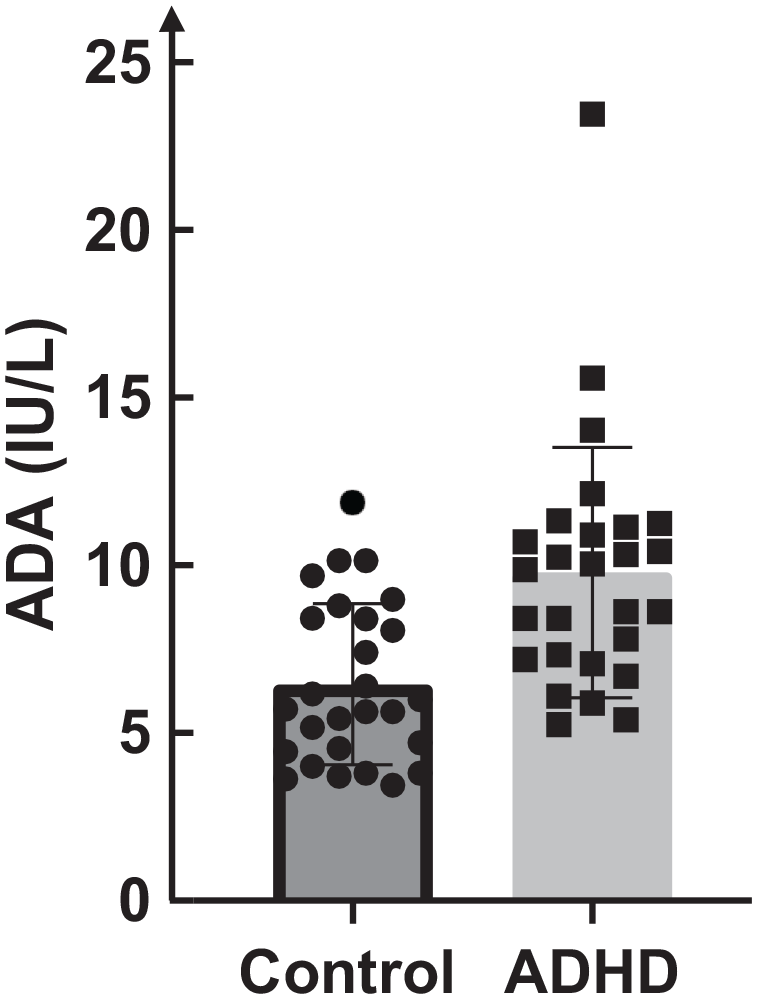
ADA distribution.
ADA and DPP IV Levels in the Patients and Controls.
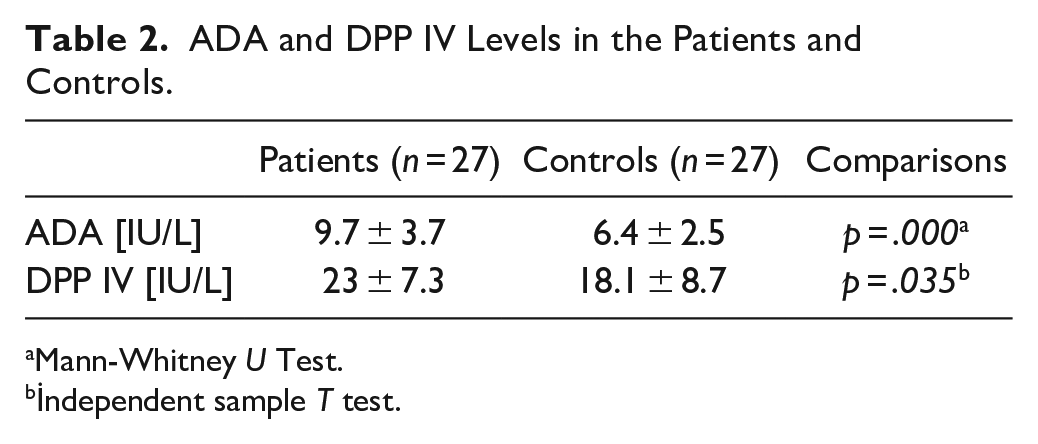
Mann-Whitney U Test.
İndependent sample T test.
Discussion
In our study, the ADA and DPP IV enzyme activities of children with attention deficit hyperactivity disorder and healthy children were evaluated, and the relationship of enzyme activities with CTRS-R-L and CPRS-R-L scale scores was investigated. It is thought that it will contribute to the pathophysiology of the disease in terms of neuroimmunology by aiming to determine the levels of ADA and DPP IV enzymes, which play a role in the formation of the cellular immune response, in ADHD.
In this study, ADA and DPP IV enzyme activities were found to be significantly higher in children with ADHD compared to healthy children. ADA has previously been investigated within the parameters of oxidative stress in the etiology of some psychiatric diseases. In a study, oxidative stress parameters were investigated in adults with major depressive disorder, ADA and xanthine oxidase levels were found to be higher than healthy controls, and after 8 weeks of antidepressant treatment, ADA levels increased compared to pre-treatment (Herken et al., 2007). In a study published by Ozdemir et al. (2012), when 60 people with panic disorder between the ages of 18 and 65 were compared with healthy controls, ADA levels were found to be increased. In a study by Herken et al. (2006) in cases with panic disorder, ADA and Xanthine oxidase levels were found to be high and, in a study, conducted by Ceylan et al. (2012) ADA levels were evaluated to evaluate oxidative stress parameters and cellular immunity in children with ADHD. The reason for this high ADA level has been interpreted as the increase in oxidative stress by the changes in DNA and purine metabolism of the ADA enzyme. In addition, it has been reported that high ADA enzyme activity may play a role in the etiology of ADHD by creating neuroinflammation due to an increase in the cellular immune response. In light of all this information, ADA activity, which was found to be high in our study, may indicate an increase in cellular immune response in individuals with ADHD. It can be thought that the increase in this cellular immune response causes ADHD by creating neuroinflammation in accordance with the literature. Neuroinflammation caused by increased cellular immune response may increase oxidative stress, suggesting that increased ADA activity plays a role in the etiology of ADHD. It has been reported that ADA inhibitors have neuroprotective effects by increasing adenosine levels. In our study, serum ADA activity was found to be high in children with ADHD. For this reason, ADA may have contributed to the formation of ADHD as a result of decreasing the neuroprotective effect by decreasing the amount of adenosine. The results of our study have similar results with the literature, as a result of this literature information; We think that cellular immunity may play a role in the etiology of ADHD due to the role of ADA enzyme in T cell-mediated immunity, and impaired cellular immunity may lead to the formation of ADHD by causing increased oxidative stress.
DPP IV has been evaluated in various psychiatric diseases and there are variable results in the literature. It has been reported that amino peptides may be responsible for the etiopathogenesis of various neuropsychiatric diseases. DPPIV, TNF α, and TGF β levels were evaluated in patients with anorexia nervosa, and it was found that TNF α levels responsible for cachexia increased and DPP IV levels decreased by inhibiting mRNA expression (Maes et al., 2001). Zheng et al. (2020) evaluated BDNF and DPP IV levels in 1,640 non-diabetic individuals aged 37 to 76 years, and a positive correlation was found between increased DPP IV levels and depressive symptoms. In a study by Maes et al. in 1991, serum DPP IV activity was found to be low in depressed adults, and in another study conducted in 1996, DPP IV enzyme activity was found to be low in depressed patients (Maes et al., 1991, 1997). In the same study, it was reported that the use of tricyclic antidepressants and selective serotonin reuptake inhibitors did not affect DPP IV activity in the small group (Maes et al., 1991). In a study by Maes et al. (1997) DPP IV levels of 36 patients with major depression were found to be lower than those of healthy controls, and increased CD4 T cells and serum DPP IV levels were found to be associated. Maes et al. (2001), it was observed that DPP IV levels decreased, depressive symptoms occurred in patients who received interferon treatment, and there was a negative correlation between these depression symptoms and DPP IV. Elgün et al. evaluated ADA and DPP IV activities in patients with major depression, minor depression, and healty controls. Ada and DPP IV levels were found to be lower than healthy controls. DPPIV activity was significantly lower in major depressives than the minor depressives (Elgün, Keskinege & Kumbasar, 1999). Deng et al. (2013) evaluated DPP IV activities in patients with unipolar depression, and DPP IV levels were found to be lower than healthy controls. In a study evaluating patients with first-episode psychosis, basal DPP IV levels were found to be higher than healthy controls, and it was observed that they reached the highest level in the first month. A negative correlation was found between DPP IV levels and depressive symptoms in the first month (Fernández-Atucha et al., 2015). In a study, serum DPP IV, ADA activities in adult panic disorder patients were examined and it was found to be higher than healthy controls (Yolaç Yarpuz et al., 2008). Frenssen et al. (2015), compared 18 cases diagnosed with ASD between the ages of 13 and 20 with healthy individuals and found no significant difference between DPP IV levels. However, the relationship between Child Behavior Checklist [CBCL] and DPP IV was examined, and a positive significant relationship was found especially in the attention, aggression and expressive behaviors subscale. Hunter et al. (2003) opioid peptides and DPP IV were investigated in individuals with autism spectrum disorder, 10 children aged 2 to 10 years with ASD were compared with adults aged 25 to 55 years who developed normally and serum DPP IV levels were evaluated by measuring ELISA. In this study, no statistically significant difference was found between the two groups, and CD26-labeled cells were measured as a percentage and these cells were found to be lower in children with ASD than in healthy adults. All this information shows that the results of DPP IV are contradictory in the literature. In our study, the high DPP IV enzyme activity in children with ADHD is seen as a different finding from the literature. This difference may have arisen because our study included the childhood age group and DPP IV had not been evaluated in ADHD patients before in the literature. The results of our study are similar to the study that showed increased serum ADA and DPP IV enzyme activity in adults with panic disorder (Yolaç Yarpuz et al., 2008). It has been reported that increased ADA and DPP IV activity in patients with panic disorder are associated with cellular immunity-mediated neuroinflammation. The increase in ADA and DPP IV enzyme activity in our study suggests that neuroinflammation may play a role in the etiology of ADHD through T cell-mediated immunity.
The limitations of our study; the small number of samples, including data from a single centre, and other parameters that indicate inflammation were not included in the study. And also, the strengths of the study are that the individuals included in the study were diagnosed with ADHD through a semi-structured interview, newly diagnosed children who did not use drugs were included in the study, individuals with medical and psychiatric comorbidities, children with mental retardation were not included, and similar groups were compared in terms of age and gender. In addition, taking the blood samples from all the patients in the morning by considering the diurnal rhythm, it was ensured that the diurnal rhythm effects on ADA and DPP IV activity were minimized.
In summary, to the best of our knowledge, this is the first study in which neuroinflammation was investigated by ADA and DPP IV activity in children with ADHD. Our study shows that there may be a relationship between cellular immunity and ADHD in children. In addition, this study is a pioneer for investigating the modulation of cellular immunity in the treatment of ADHD in children in the future.
Conclusion
As a result, in our study, we measured the neuroinflammation of children with ADHD with ADA and DPP IV activity and found that these activities were statistically significantly higher than healthy children. As far as is known, our study is the first study in the literature to evaluate serum ADA and DPP IV activities in children with ADHD. Studies investigating the role of cellular immunity in the etiology of children with ADHD are limited. Since these studies are limited, there is a need for further studies on the evaluation of serum ADA and DPP IV activities in various age groups, the evaluation of cellular immunity with other immune parameters, and the modulation of cellular immunity in treatment.
Footnotes
Acknowledgements
None
Authorship Contribution Statement
Yüksel Sümeyra Naralan designed the study, collected the data, wrote a first draft, and revised the manuscript critically. Özlem Doğan conducted the analyses. Serenay Elgün, Didem Behice Öztop, and Birim Günay Kılıç conducted the analyses, revised the manuscript critically, and wrote the final version of the article. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.