
Abstract
Objective:
Adverse childhood experiences (ACEs) are early life experiences that influence mental health outcomes, though there are mixed findings reported in relation to attention deficit hyperactivity disorder (ADHD) symptoms. The current study compared adults who experienced ACEs on measures of ADHD symptom reporting, psychological symptoms, and neurocognitive test performance.
Method:
The sample (n = 115) had mean age of 28.42 (SD = 6.46); educational attainment of 16.47 years (SD = 1.99); and was 35% male/65% female and racially/ethnically diverse. Participants completed measures of ACEs, ADHD symptoms, psychopathology, and perceived stress, as well as neuropsychological tests.
Results:
The high ACEs group endorsed higher levels of childhood/adulthood inattentive, impulsive, and hyperactive symptoms, and overall childhood symptoms when compared to the low ACEs group.
Conclusions:
This study provides a more comprehensive understanding of the association between ACEs and cognitive/mental health outcomes. Greater ACEs resulted in higher ADHD symptom reporting but not significantly greater psychological symptoms or worse neurocognitive performance.
Keywords
Adverse childhood experiences (ACEs) are early life experiences that have the potential to impact early development and subsequent health outcomes across an individual’s lifespan (Shonkoff et al., 2011). Examples of ACEs include child abuse (e.g., physical, sexual, emotional), child neglect (e.g., emotional, physical), and environmental/psychosocial stressors (e.g., exposure to domestic violence, exposure to mental illness and/or substance use in the home; Ports et al., 2020). Although the experience of adversity is not uncommon, ACEs are associated with poorer health outcomes, including mental health concerns and aberrant cognitive development (Ports et al., 2020). Broadly, potential negative outcomes from ACEs include a higher risk for developing multiple mental health disorders (e.g., anxiety, mood dysregulation), neurodevelopmental challenges, and increased risk for poorer physical health outcomes and risky health behaviors (Sheffler et al., 2020; Vig et al., 2020). Specifically, prior research found that 83% of outpatient subjects with major depressive disorder (MDD) reported at least one ACE in childhood (Thompson, 2018). These experiences are associated with a younger age of diagnosis with MDD, suicidal thoughts across the lifespan, and symptoms of posttraumatic stress disorder (PTSD; Thompson, 2018). Furthermore, children who experience ACEs have significantly higher odds of developing symptoms of anxiety disorders (Elmore & Crouch, 2020).
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by heterogeneous presentations of inattentive and behavioral symptoms and frequently co-occurs with a range of other disorders, for example, depression, anxiety; Drechsler et al., 2020). Previous studies have explored the relationship between ACEs and ADHD in child and young adult samples. Notably, children exposed to four or more ACEs were significantly associated with being diagnosed with ADHD and presenting with more moderate-severe symptoms (Crouch et al., 2021). In addition, higher levels of ACEs were associated with higher reports of ADHD symptom in a cohort of college students (Windle et al., 2018). ACEs may have an additive impact on ADHD such that individuals who experienced four or more ACEs were linked to a higher probability of developing ADHD (Crouch et al., 2021).
Unlike with ADHD, there are conflicting results amongst studies exploring the relationship between ACEs and objective cognitive performance. Studies in young adult populations have found that higher number of ACEs have been associated with poorer performance on objective tasks of learning and memory, deficits in executive function (e.g., problem-solving), and reports of higher subjective cognitive difficulties (Brown et al., 2022; Kalia et al., 2021). As people age, ACEs may also be associated with poorer cognitive outcomes (O’Shea et al., 2021). In contrast, more recent studies with multiethnic samples found that higher number ACEs were not associated with poorer cognition but were associated with reports of more psychological symptoms (Bing-Canar, Khan, et al., 2022; Gold et al., 2021). However, it is important to note that most of these studies have not explored the relationship between ACEs and objective cognitive performance among individuals with ADHD symptom reporting.
Given this gap in the literature, the present study aimed to compare ADHD symptom reporting, psychological symptoms (e.g., depression, anxiety), and cognitive performance (e.g., verbal learning and memory, processing speed, working memory, executive function) in adults who endorse a low (0–3 on ACEs questionnaire) versus high (≥4 ACEs) level of ACEs. In line with most recent literature, it was predicted that adults with higher ACEs levels would report more symptoms of ADHD and psychological symptoms, but groups would not differ on cognitive test performance. A more comprehensive understanding of the influences of ACEs on cognitive deficits, psychological symptomatology, and ADHD, may help to inform knowledge on neurodevelopmental disorders, as well as inform best practices for adult ADHD assessment.
Method
Participants
This cross-sectional study examined data from a consecutive series of 144 adults referred for neuropsychological evaluation at large urban university academic medical center. All patients provided written informed consent to include their clinical evaluation data as part of a larger, ongoing IRB-approved neuropsychological database study. All patients were referred following screening by their treating providers, most often primary care/family medicine physicians or psychiatrists, to assist with ADHD diagnostic clarification and treatment planning. One patient was missing a measure of interest, 9 had invalid cognitive test performance per performance validity tests (PVTs), and 19 had evidence of invalid ADHD symptom reporting. These 29 patients were excluded, resulting in a final sample of 115 unique cases. The overall sample was diverse with a mean age of 28.42 (SD = 6.46); educational attainment of 16.47 years (SD = 1.99); sex distribution of 35% (N = 40) male/65% (N = 75) female; racial/ethnic composition of 42% White, 19% Black, 16% Hispanic, 12% Asian, and 9% other (Table 1). Although all patients were English-dominant and all testing was completed in English, approximately 37% (N = 49) of the sample self-identified as bilingual. Finally, 73% (N = 84) of the sample were active college students at the undergraduate (N = 29) or graduate/professional (N = 55) level (Table 1).
Demographic Characteristics for the Sample Stratified by Group.
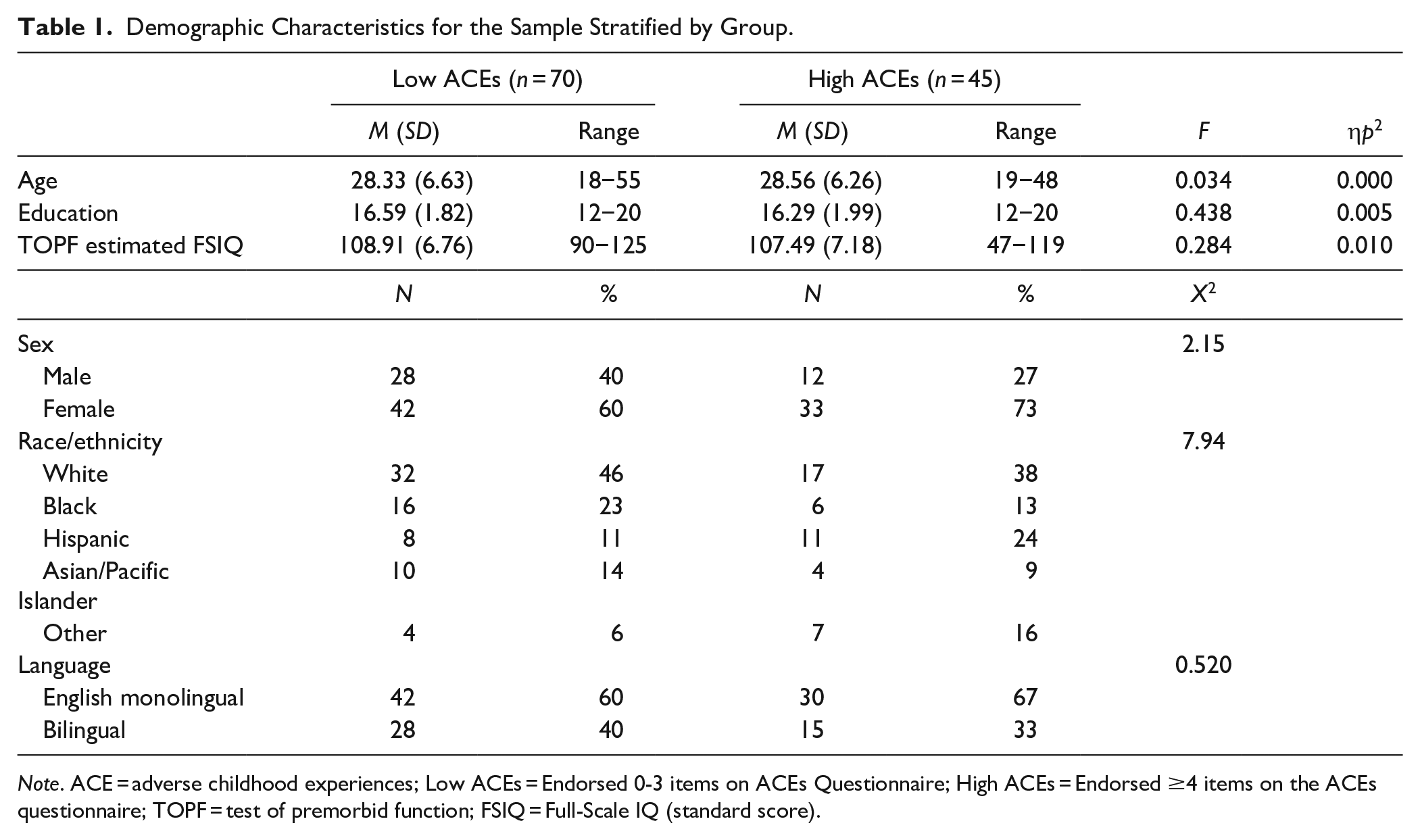
Note. ACE = adverse childhood experiences; Low ACEs = Endorsed 0-3 items on ACEs Questionnaire; High ACEs = Endorsed ≥4 items on the ACEs questionnaire; TOPF = test of premorbid function; FSIQ = Full-Scale IQ (standard score).
Measures
Adverse Childhood Experiences
All patients completed the Adverse Childhood Experiences (ACE; Felitti et al., 1998) Questionnaire, a measure of adverse events during childhood on which examinees self-report whether they have experienced each event with a “yes” or “no” answer. The 10 items include questions about emotional, physical, and sexual abuse, neglect, and witnessing violence, among others. ACE scores are grouped into high versus low raw scores, as defined in prior research, with 4 or more “yes” answers denoting a high level of ACEs as those with ≥4 ACEs have shown to be 4 to 12 times more likely to experience negative outcomes (Felitti et al., 1998).
ADHD Symptom Reporting
The Clinical Assessment of Attention Deficit-Adult (CAT-A; Bracken & Boatwright, 2005) is a symptom-validity controlled measure of ADHD symptoms in which examinees self-rate core ADHD symptoms of inattention, impulsivity, and hyperactivity on a four-point scale at two time points: in childhood and currently. Along with the validity scales and specific symptom scores, the CAT-A also provides composite index scores for childhood symptoms, adult/current symptoms, and total ADHD symptoms. Scores presented are age- and sex-adjusted T-scores with ≥60T denoting clinical elevation and higher scores indicating greater symptom endorsement.
Psychopathology Symptoms and Perceived Stress
All patients were administered the Beck Depression Inventory-Second Edition (BDI-II; Beck et al., 1996), Beck Anxiety Inventory (BAI; Beck et al., 1988), and Perceived Stress Scale (PSS; Cohen et al., 1994), which are self-report instruments of depressive and anxiety symptoms and perceived stress, respectively. BDI-II, BAI, and PSS scores are presented as raw scores with higher scores representing higher levels of mood, anxiety, and perceived stress symptoms/levels.
Neuropsychological Testing
All patients completed a standardized neuropsychological testing battery that included the Rey Auditory Verbal Learning Test (RAVLT; Schmidt, 1996); Working Memory (WMI) and Processing Speed (PSI) Indices from the Wechsler Adult Intelligence Scale-Fourth Edition (WAIS-IV; Wechsler, 2008); Trail Making Test Parts A/B (TMT; Heaton et al., 2004), and the Stroop Color-Word Test, Color-Word Inhibition Trial (SCWT; Golden, 1978). RAVLT scores are presented as age-corrected T-scores, WMI and PSI as age-corrected standard scores; TMT as age/education/sex/race-corrected T-scores; and SCWT as age/education-corrected T-scores. As part of the test battery, all patients were administered two freestanding PVTs: Dot Counting Test (Abramson et al., 2023) and Rey 15-Item/Recognition (Poynter et al., 2019), and three embedded PVTs: RAVLT Effort Scale (Phillips et al., 2023); Reliable Digit Span (Bing-Canar, Phillips, et al., 2022); and Stroop Word Reading T-score (Khan et al., 2022), all of which have been cross-validated in ADHD clinical samples. Consistent with current practice guidelines and empirical findings (e.g., Jennette et al., 2022; Rhoads et al., 2021), patients with two or more PVT failures (n = 9) were classified as having invalid neuropsychological test performance and excluded from analyses.
Data Analysis
Descriptive statistics for ADHD (childhood/current) and psychological symptom reporting, as well as neurocognitive test performance were calculated for low and high ACEs groups. Analyses of variance (ANOVAs) compared childhood and current ADHD symptom reporting, psychological symptom reporting, and cognitive test performance to test for significant differences between low ACEs and high ACEs groups. The false discovery rate procedure (FDR; Benjamini & Hochberg, 1995) with a 0.05 maximum FDR was implemented to control the familywise error rate associated with multiple ANOVAs. To examine the effect of ACEs on ADHD symptom severity, chi-square tests assessed significant differences between low and high ACEs groups and ADHD symptom severity in childhood and adulthood via the CAT-A childhood, current, and overall clinical index scores. For this analysis, ADHD symptom severity was operationalization as minimal (≤59T), mild (60–69T), moderate (70–79T), or severe (≥80T).
Transparency and Openness
Methods for determining sample size, data exclusions, manipulations, and all measures in the study were reported, and the study adhered to Journal Article Reporting Standards (JARS). Data were analyzed using IBM SPSS Statistics Software (Version 26). This study’s design or its analysis were not preregistered. Materials and analysis code for this study are not available.
Results
Significant main effects were found for mean-level self-reporting on all CAT-A scales measuring childhood and current ADHD symptoms (e.g., inattention, impulsivity, hyperactivity; Table 2). Specifically, the high ACEs group consistently endorsed higher levels of childhood inattentive, impulsive, and hyperactive symptoms, as well as greater overall childhood symptoms when compared to the low ACEs group. Similarly, the high ACEs group endorsed higher levels of perceived stress, current/adulthood inattentive, impulsive, and hyperactive symptoms as well as overall current ADHD symptoms, when compared to the low ACEs group, although the effect sizes were not as large relative to what was observed with childhood symptoms. By contrast, there were no significant differences in self-reported current psychopathology symptoms between the low ACEs and high ACEs groups. There also were nonsignificant performance differences for all the measures of neurocognitive functioning between the two ACEs groups. Finally, as seen in Table 3, those with high ACEs endorsed significantly greater ADHD symptom severity in childhood, whereas nonsignificant differences emerged in terms of ADHD symptom severity for current/adult symptoms and the CAT-A overall ADHD index scores.
ADHD Symptom Reporting, Psychological Symptom Reporting, and Neurocognitive Test Performance Across Study Groups.
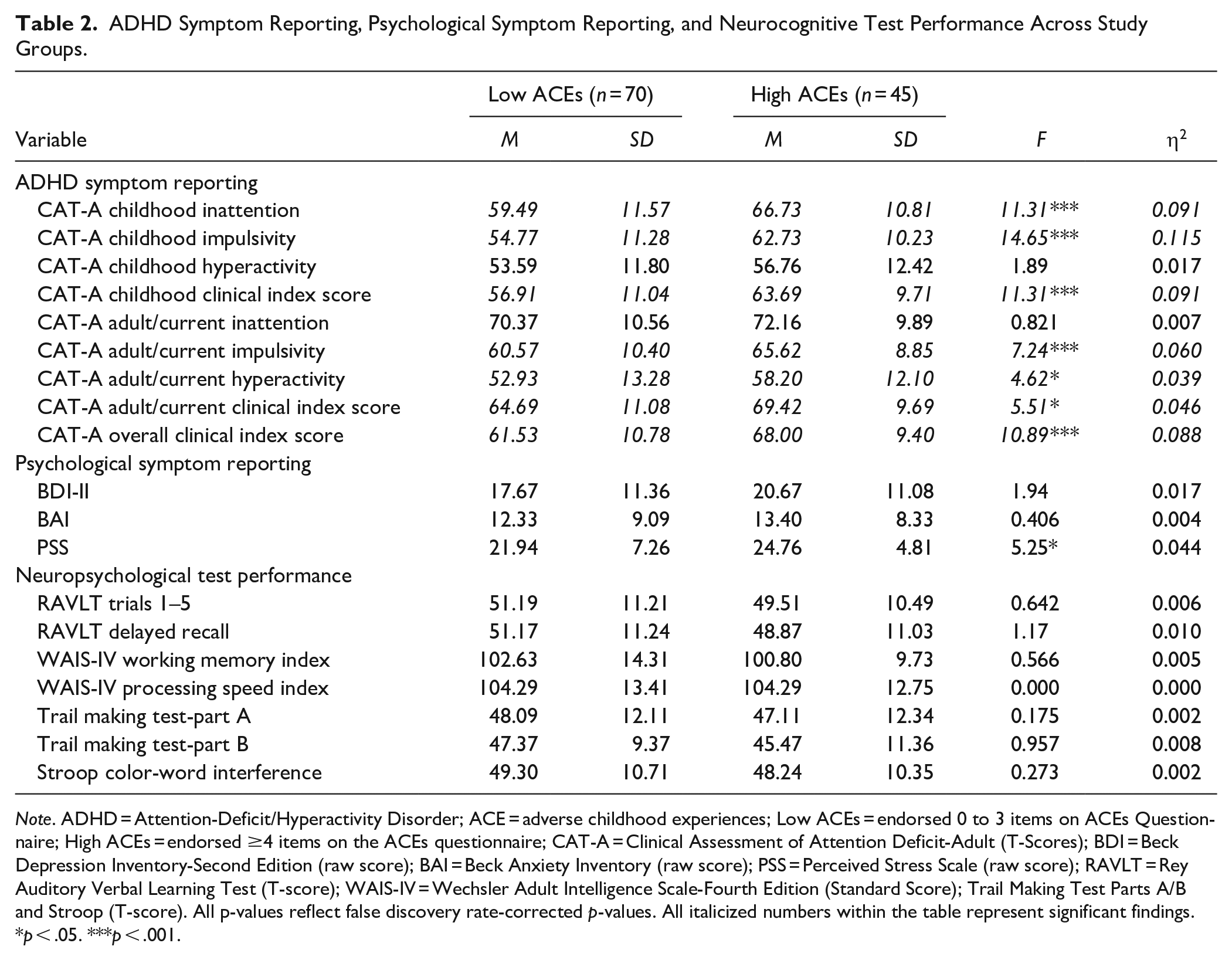
Note. ADHD = Attention-Deficit/Hyperactivity Disorder; ACE = adverse childhood experiences; Low ACEs = endorsed 0 to 3 items on ACEs Questionnaire; High ACEs = endorsed ≥4 items on the ACEs questionnaire; CAT-A = Clinical Assessment of Attention Deficit-Adult (T-Scores); BDI = Beck Depression Inventory-Second Edition (raw score); BAI = Beck Anxiety Inventory (raw score); PSS = Perceived Stress Scale (raw score); RAVLT = Rey Auditory Verbal Learning Test (T-score); WAIS-IV = Wechsler Adult Intelligence Scale-Fourth Edition (Standard Score); Trail Making Test Parts A/B and Stroop (T-score). All p-values reflect false discovery rate-corrected p-values. All italicized numbers within the table represent significant findings.
p < .05. ***p < .001.
ADHD Symptom Severity Across Study Groups.
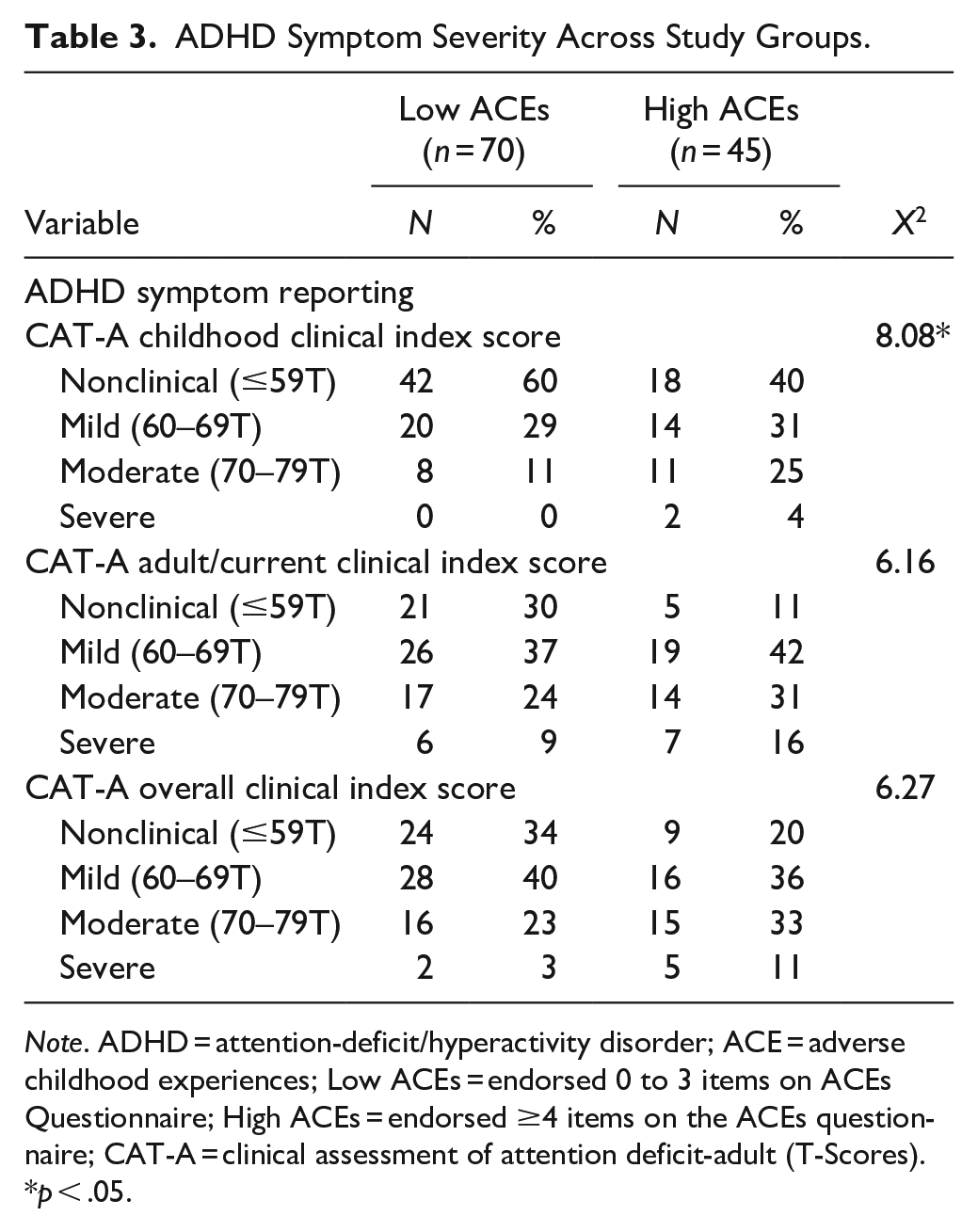
Note. ADHD = attention-deficit/hyperactivity disorder; ACE = adverse childhood experiences; Low ACEs = endorsed 0 to 3 items on ACEs Questionnaire; High ACEs = endorsed ≥4 items on the ACEs questionnaire; CAT-A = clinical assessment of attention deficit-adult (T-Scores).
p < .05.
Discussion
A growing literature has begun to characterize the long-term consequences of ACEs which include greater risk for psychological dysfunction and poorer quality of life. This study examined adult psychological symptom reports and objective cognitive performance, as well as retrospective childhood and current reports of ADHD symptomatology among adults with a high versus low number of ACEs. This study is among the first studies, to our knowledge, to examine self-reported ADHD symptoms in childhood/adulthood in the same sample within the context of ACEs, offering a unique window into the role of ACEs across the lifespan. Consistent with prior literature, our results showed adults with a higher number of ACEs endorsed higher rates of both childhood and current cognitive/ADHD symptoms, overall and across symptom domains (i.e., inattentive, impulsive, and hyperactive), particularly in childhood. Surprisingly, our study did not find that ACEs are associated with greater psychological dysfunction in adulthood, as high/low ACE groups reported similar levels of anxiety and depression in contrast with prior work (Bing-Canar, Khan, et al., 2022; Windle et al., 2018). This dissociation indicates our finding of greater ADHD symptom endorsement cannot simply be explained by higher levels of general psychological dysfunction or broad symptom endorsement among those with high ACEs. Although there was a significant difference in reported perceived stress between the high and low ACEs groups, higher perceived stress is to be expected in individuals reporting higher levels of adverse experiences. Finally, our results add to the literature suggesting ACEs were not associated with cognitive functioning in young adulthood, with no significant differences evidenced across tests of verbal learning, working memory, speed, and executive functions between high/low ACEs groups.
The presence of a relationship between ACEs and ADHD diagnosis and severity has been consistently documented (Brown et al., 2022; Crouch et al. 2021; Windle et al., 2018); however, the pathophysiological and environmental mechanisms subserving this association are not yet fully understood. Chronic stress, due to repeated exposure to traumatic events, maltreatment, and impoverished environments early in childhood, can alter the trajectory of typical neurodevelopment and has been implicated in the neurobiology of ADHD. Chronic stress confers greater risk for more severe and persistent ADHD symptoms, while reductions in environmental stress have been associated with remitting ADHD symptoms (Hartman et al., 2019). Together, this suggests that there is a bidirectional relationship between adverse events and stress with ADHD symptoms expression that may result in fluid clinical presentations across the life span that evolve with changing environments. Additionally, counter-ACEs, or positive childhood experiences (e.g., good friends, supportive teachers, predictable environments) may mitigate the negative effects of ACEs on long term outcomes (Crandall et al., 2019). However, this study did not assess counter-ACEs, which should be explored in future studies.
Although the results of the present study identified greater ADHD symptom reporting in both retrospective childhood reports and current symptoms among those with higher ACEs, this effect was stronger for childhood symptomatology across ADHD symptom domains (η2 = 0.091, 0.115, 0.091 for childhood inattention, impulsivity, and clinical score respectively compared to η2 = 0.007, 0.060, 0.046 for adult/current inattention, impulsivity, and clinical score respectively). One possible explanation for this pattern of findings is that adult participants in the high ACEs group may no longer be exposed to the same intensity of adverse events or experiencing chronic stress in adulthood relative to childhood, which may in turn contribute to a reduction in the severity of ADHD symptomatology reporting. Conversely, greater self-reported childhood ADHD symptoms may in fact reflect symptoms of traumatic stress, rather than true ADHD symptomatology, and individuals with ADHD symptoms may recall their childhood differently than those without ADHD symptoms. In other words, higher ACEs, and in turn higher childhood traumatic stress, may have contributed to clinical presentations that appear qualitatively similar to ADHD symptoms. It is important to note that the two groups in the sample (low vs. high ACEs) were demographically matched which suggests that other protective factors (e.g., high educational attainment; differences in IQ) are not underlying the significant differences found. Despite this remaining uncertainty regarding underlying mechanism as the cross-sectional nature of this study preclude determination of causality, our results and the growing body of literature demonstrating links between ADHD and ACEs highlight the need for clinicians to consider ACEs during ADHD diagnostic assessments and treatment planning. Specifically, given the near ubiquitous reliance on retrospective self-report of symptoms in adult ADHD evaluations, it is important to assess for ACEs independently and directly via formal measures as this important factor influencing symptom reporting is not readily apparent when examining only at broad measures of general psychopathology or stress. Put another way, all of the patients in this study were referred for ADHD evaluation; thus, all presented with attention complaints. Despite ubiquitous cognitive/attention complaints across patients, those with higher ACEs reported significantly greater ADHD/cognitive complaints, particularly in childhood, relative to patients with low ACEs. This suggest that ACEs may contribute to higher reports of ADHD childhood symptoms, which can result in misattribution of attention problems due to childhood adversity/traumatic stress and potential misdiagnosis of ADHD when retrospective, self-report ADHD inventories are administered as part of a psychological/neuropsychological evaluation.
We hypothesized higher ACEs would contribute to higher reports of ADHD and psychological symptoms, in light of the high rates of comorbidity between mood symptoms and ADHD and the association between ACEs and adult psychopathology established by prior research. Surprisingly, we found no differences in self-reported symptoms of anxiety and depression among high and low risk ACEs groups. As with ADHD symptomatology, current stress levels and counter ACEs throughout development mediate adult psychological symptoms, which may also explain the lack of findings in the present study (Crandall et al., 2019; Hartman et al., 2019; Narayan et al., 2018). We also found no difference in cognitive performance among high and low risk ACEs groups, which is largely consistent with existing literature and adds to the growing evidence that there is no significant association between ACEs and long-term cognitive outcomes. However, previous studies have evidenced poorer cognition performance among individuals who have suffered sexual abuse, specifically, along with low socioeconomic status (Hawkins et al., 2021). Further exploration of the relationships between ACEs and ADHD symptom reporting and cognition may prove beneficial, especially considering specific differences by varying types and duration of ACEs, as well as age at which ACEs were experienced. As research supports that differences in outcomes may be influenced by the categories of ACEs, duration and chronicity of ACEs, as well as differences in age at which ACEs are experienced, these factors should also be considered in the context of ADHD symptom reporting (Briggs et al., 2021; Jones et al., 2022; Schroeder et al., 2020).
Although this study had many methodological strengths including a racially/ethnically diverse clinical sample and demographically matched groups, the results should also be interpreted in light of the study’s limitations. First, the study only included patients referred for ADHD evaluations who consented to participate in research. Data collected regarding adverse childhood experiences and childhood ADHD symptom reporting also were retrospective, making exact recall of details more difficult for the patient. As such, future researchers should aim for longitudinal studies of ACEs where concurrent reporting throughout time is made possible.
In sum, this study provides important results that inform a more comprehensive understanding of how ACEs impact psychological, cognitive, and ADHD-related symptom reporting. Importantly, understanding and assessing ACEs are important to consider in differential diagnosis and treatment planning for individuals reporting ADHD-related symptoms, and may inform intervention and resources to reduce negative outcomes in this population.
Footnotes
Author Contributions
DA was involved with formal analysis, methodology, project administration, writing-original draft, and writing-review and editing. KB, JG, HBV, and CG were involved with writing-original draft. GPO was involved with data curation. VJR was involved with supervision, writing-original draft, and writing-reviewing and editing. ZJR and DMU were involved with writing-reviewing and editing. JRS was involved with data curation, formal analysis, investigation, methodology, project administration, resources, supervision, writing-original draft, and writing-reviewing and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data,Materials,and Code
Methods for determining sample size, data exclusions, manipulations, and all measures in the study were reported, and the study adhered to Journal Article Reporting Standards (JARS). Data were analyzed using IBM SPSS Statistics Software (Version 26). This study’s design or its analysis were not preregistered. Materials and analysis code for this study are not available.
Prior Dissemination
There is no prior dissemination of the data or narrative interpretations of the data/research appearing in this manuscript.