
Abstract
Objectives:
To investigate the relationship between screen time and symptom severity in children with ADHD during the COVID-19 lockdown.
Methods:
Caregivers of children with ADHD aged 7 to 16 years completed the screen time questionnaire and ADHD rating scales of the SNAP-IV-Thai version during and after the COVID-19 lockdown. The correlation between screen time and ADHD scores was assessed.
Results:
Of the 90 children, aged 11.31 ± 2.29 years, enrolled, 74.4% were male, 64.4% were in primary school, and 73% had electronic screens in their bedrooms. After adjusting with other factors, recreational screen time, both on weekdays and on weekend days, were positively correlated with ADHD scores (both inattention and hyperactive/impulsive scores). Studying screen time, on the other hand, was not associated with ADHD symptom severity. Compared to during the lockdown, studying screen time decreased after the lockdown, but recreational screen time and ADHD scores were not changed.
Conclusion:
Increasing recreational screen time was associated with worsening ADHD symptoms.
Keywords
Introduction
ADHD is the most common neurobehavioral disorder of childhood, characterized by a persistent pattern of inattention, hyperactivity, and impulsivity, that interferes with functioning or development (G. V. Polanczyk et al., 2014; Shaffer et al., 2012). Symptom manifestation of ADHD may be affected by a variety of environmental and lifestyle factors, including sleeping, physical activities, cognitively stimulating activities, and using electronic media (Ceranoglu, 2018; Peralta et al., 2018).
Excessive use of electronic media has been found to be associated with physical and psychological adverse consequences including poor sleep, decreased social coping, and increased ADHD symptoms (Brand et al., 2014; Goldfield et al., 2011; Liu et al., 2016; Martinez-Gomez et al., 2010; Swing et al., 2010; Wu et al., 2016). In children with ADHD, screen time reduction might reinforce good social coping skills, good physical health, and decreased ADHD-related behaviors (Lissak, 2018). However, studies on the effects of screen time on ADHD symptoms have been limited.
In Thailand, during the pandemic of COVID-19, the government enforced country lockdowns in order to prevent the spread of the infection. During the lockdown, almost all schools in the country provided online teaching to the students, and outdoor activities for children were limited, making children expose to more screen time, both for studying and for recreation. The increased screen exposure might have an effect on children, particularly those with ADHD. This study examined the relationship between screen time and symptom severity in children with ADHD during the lockdown.
Materials and Methods
A prospective cohort study was conducted from October 2021 to September 2022. Participants were recruited from the Child and Adolescent Psychiatric Clinic at the Department of Pediatrics, Siriraj Hospital, Mahidol University, Bangkok, Thailand. The study protocol was approved by the Siriraj Institutional Review Board (COA no. Si 739/2021).
This study included 90 children, aged 7 to 16 years, diagnosed with ADHD, and their primary caregivers. The diagnosis of ADHD was made by the treating child and adolescent psychiatrists, based on the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) criteria. Exclusion criteria were children with other neurological or psychiatric comorbidities.
Demographic data, including presence of electronic screens in the bedroom, were collected by interviewing the participant’s caregivers. The caregivers were asked to complete the screen time questionnaire and the SNAP-IV- Thai version at two different times, during the lockdown (October 2021–April 2022) and after the lockdown (May 2022–September 2022).
Instruments
Screen Time Questionnaire
The screen time questionnaire was developed by the investigators inquiring about the screen time children spent for studying, social media use, watching movies, and playing games on any electronic devices. Screen time was categorized into screen time on weekdays, screen time on weekend days, and total screen time (on weekdays and weekend days combined).
The SNAP-IV-Thai Version
The SNAP-IV Thai version is a parent-report questionnaire translated into Thai from the original Swanson, Nolan, and Pelham IV scale (SNAP-IV)-short version, designed to assess ADHD and oppositional defiant symptoms in children aged 4 to 16 years. It comprises 26 items with three subscales, including inattentive scales (SNAP-Inatt), hyperactivity/impulsivity scales (SNAP-H/Im), and oppositional defiant scales (SNAP-Odd). The scores are rated on a Likert rating scale from 0 to 3; 0 = “never”; 1 = “rarely”; 2 = “often”; 3 = “always.” The summation of inattentive subscales and hyperactivity/impulsivity scales yields a total ADHD scale. Higher scores reflect more symptoms. The internal consistency for all subscales is high; α = .71 for SNAP-Inatt, α = .75 for (SNAP-H/Im), and α = .81 for (SNAP-Odd) (Pityaratstian et al., 2014). In this study, we used SNAP-Inatt and SNAP-H/Im subscales to measure ADHD symptom severity.
Data Analyses
Descriptive statistics were used to describe demographic data. Pearson correlation coefficient or Spearman’s rank correlation coefficient was used to analyze the correlation between screen time and ADHD scores. Multiple linear regression analysis was used to assess the correlation between screen time and ADHD symptoms while adjusting for other factors (gender, presence of physical illness, school level, parents’ education level, family income, and presence of electronic screens in the bedroom). A pair sample t-test and Wilcoxon sign rank test were used to compare the data during and after the lockdown. Significant levels were set at p ≤ .05. Statistical analysis was completed using PASW statistics 18 (SPSS Inc., Chicago, IL, USA).
Results
Participant’s Characteristics
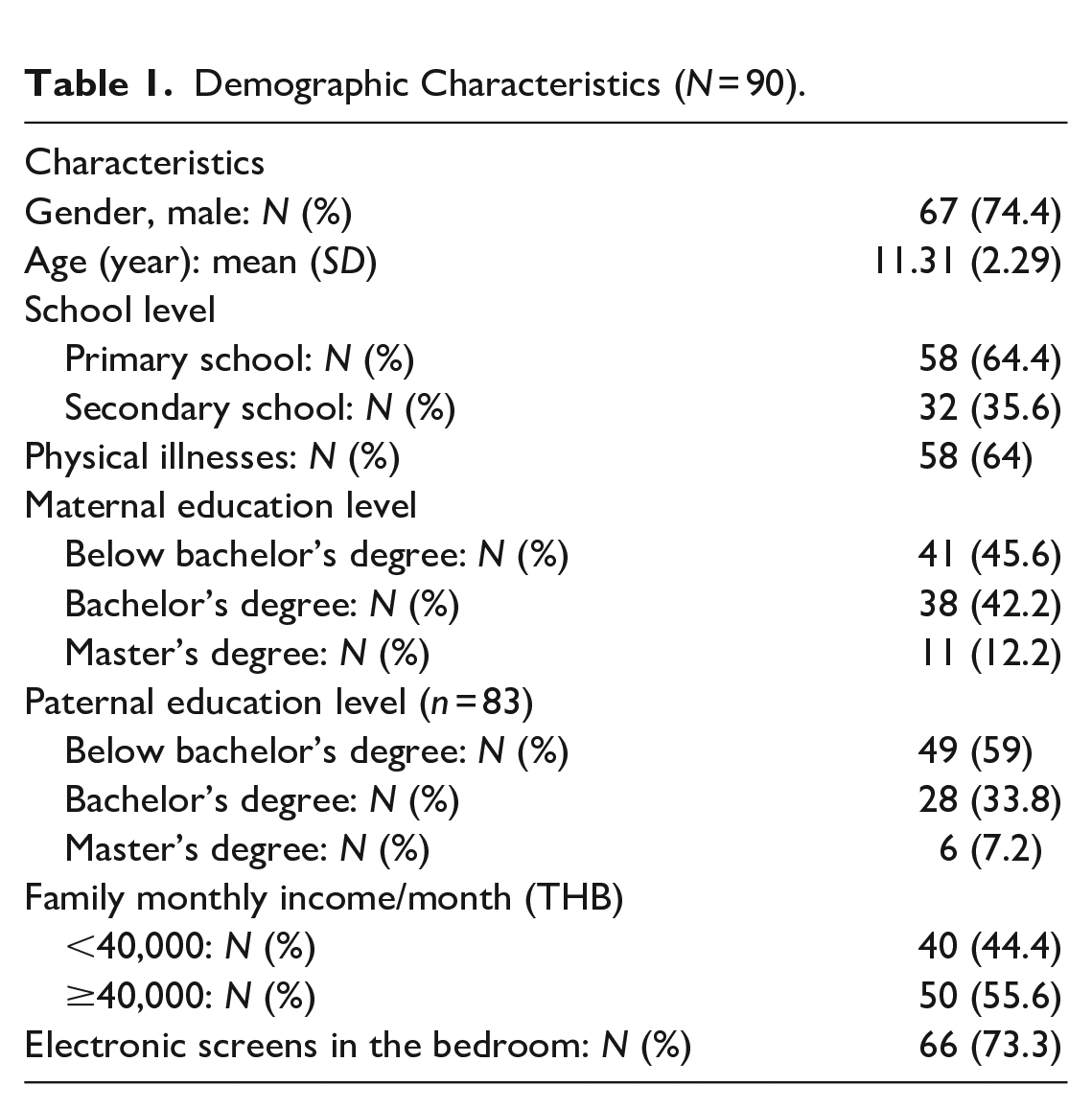
The mean age of the children was 11.31 (SD = 2.29) with the range of 7 to 16 years old. Seventy-four percent of the children (n = 67) were male, and 64% (n = 58) were in primary school. Seventy-three percent of the children (n = 66) had electronic screens in the bedroom (Table 1).
Demographic Characteristics (N = 90).
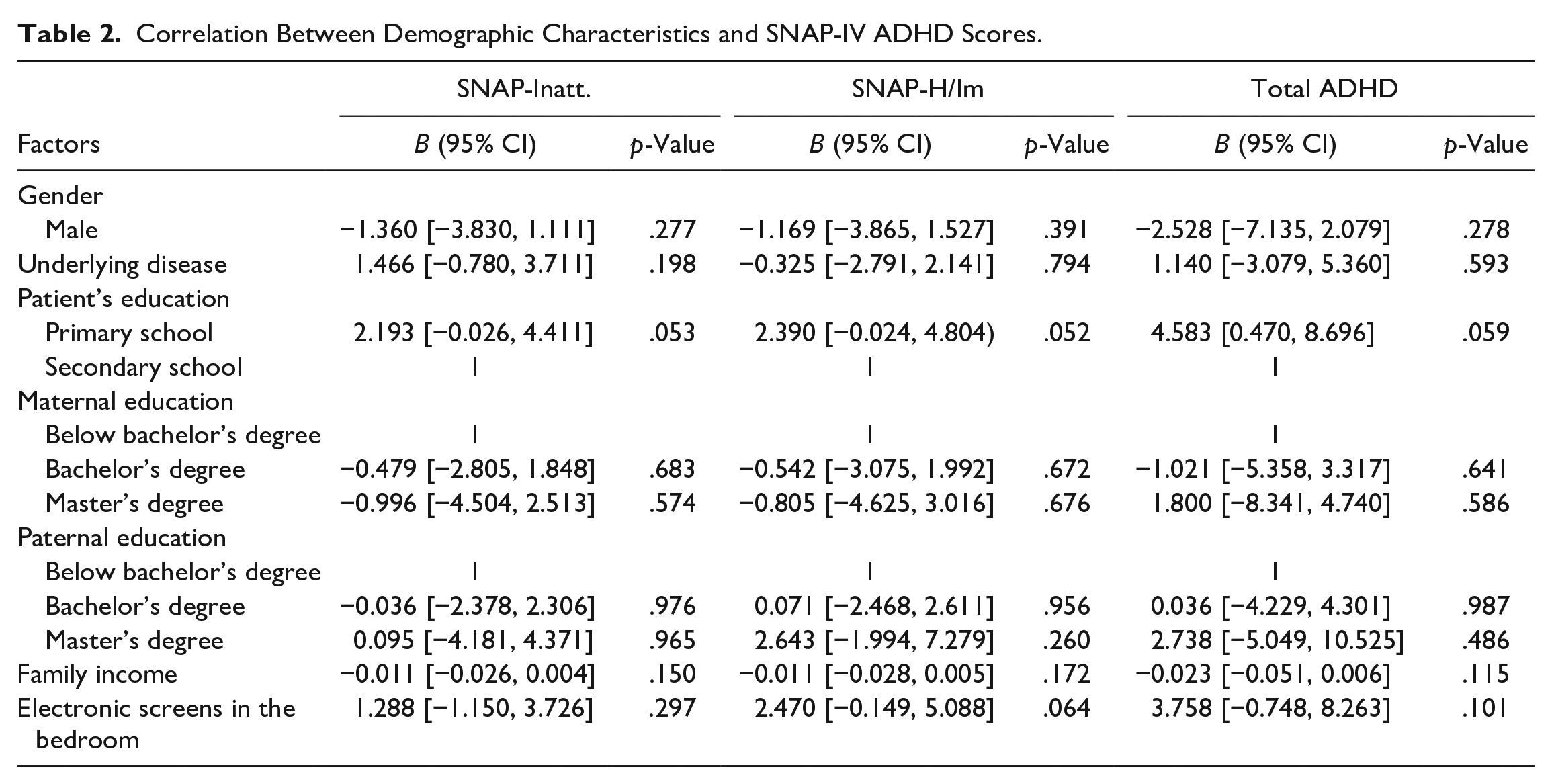
There was no significant association between SNAP-IV ADHD scores and gender, presence of physical illnesses, school level, parents’ education level, family income, and presence of electronic screens in the bedroom (Table 2).
Correlation Between Demographic Characteristics and SNAP-IV ADHD Scores.
Correlation Between Screen Time and ADHD Symptoms
The correlation between screen time and SNAP-IV ADHD scores in primary school and secondary school children assessed by the Pearson correlation coefficient was shown in Table 3. There was a correlation between SNAP-Inatt, SNAP-H/Im, and all categories of screen time in primary school children, and in children of both primary and secondary school combined, but not in secondary school children.
Correlation Between Screen Time and SNAP-IV ADHD Scores During COVID-19 Lockdown.
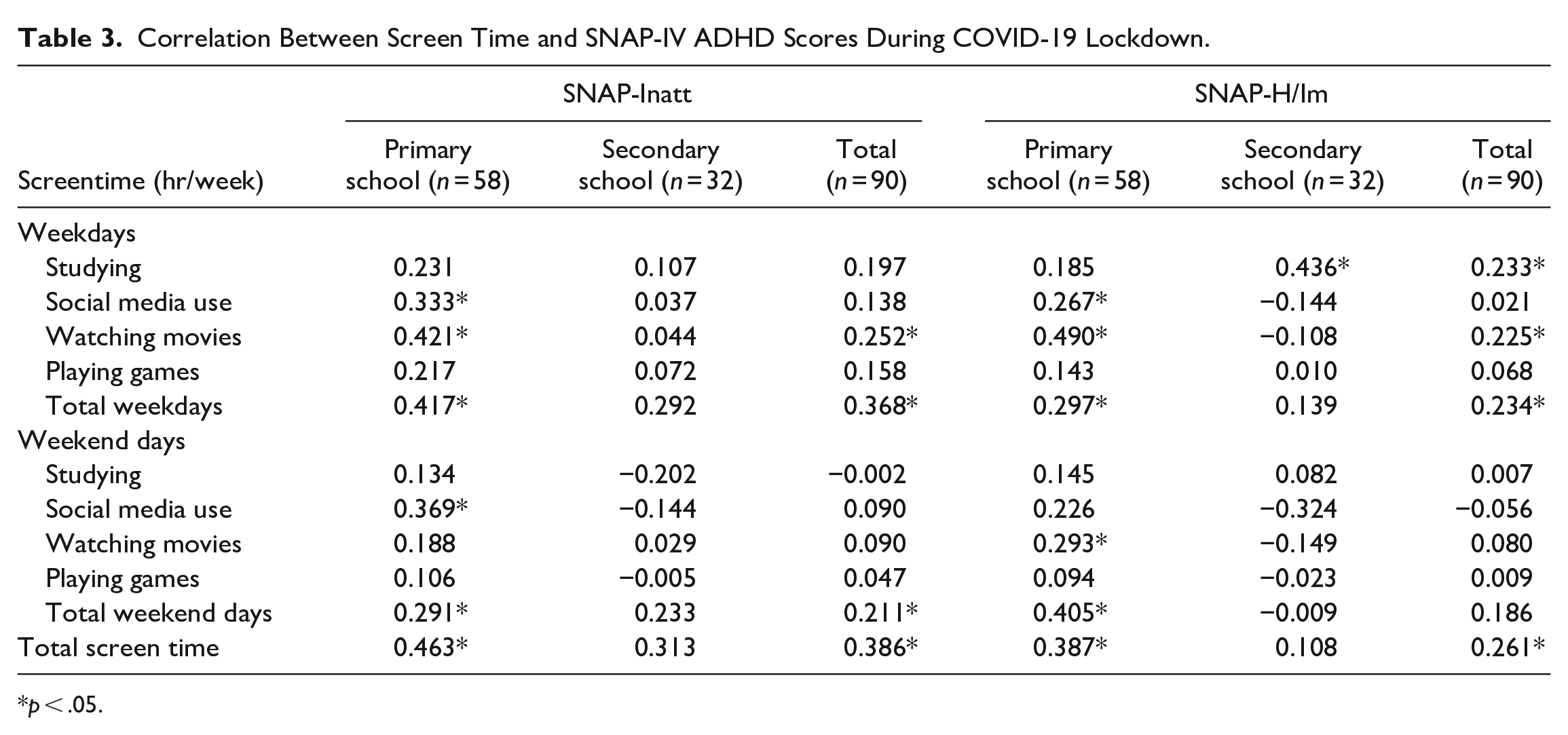
p < .05.
On weekdays, screen time for social media use and watching movies were correlated with SNAP-lnatt and SNAP-H/Im scores in primary school children. Screen time for studying was correlated only with SNAP-H/Im scores in the secondary school children, but not with other scores in both groups of children.
By multiple linear regression analysis, total screen time, total weekdays and total weekend days screen time, and screen time for recreations (summation of time for social media use, watching movies, and playing games) both on weekdays and weekend days, were correlated with SNAP-Inatt and SNAP-H/Im scores in the children (in primary and secondary school combined). Screen time for studying was not correlated with SNAP-IV ADHD scores on either weekdays or weekend days (Table 4).
Correlation Between Screen Time and SNAP-IV ADHD Scores by Multiple Linear Regression Analysis.
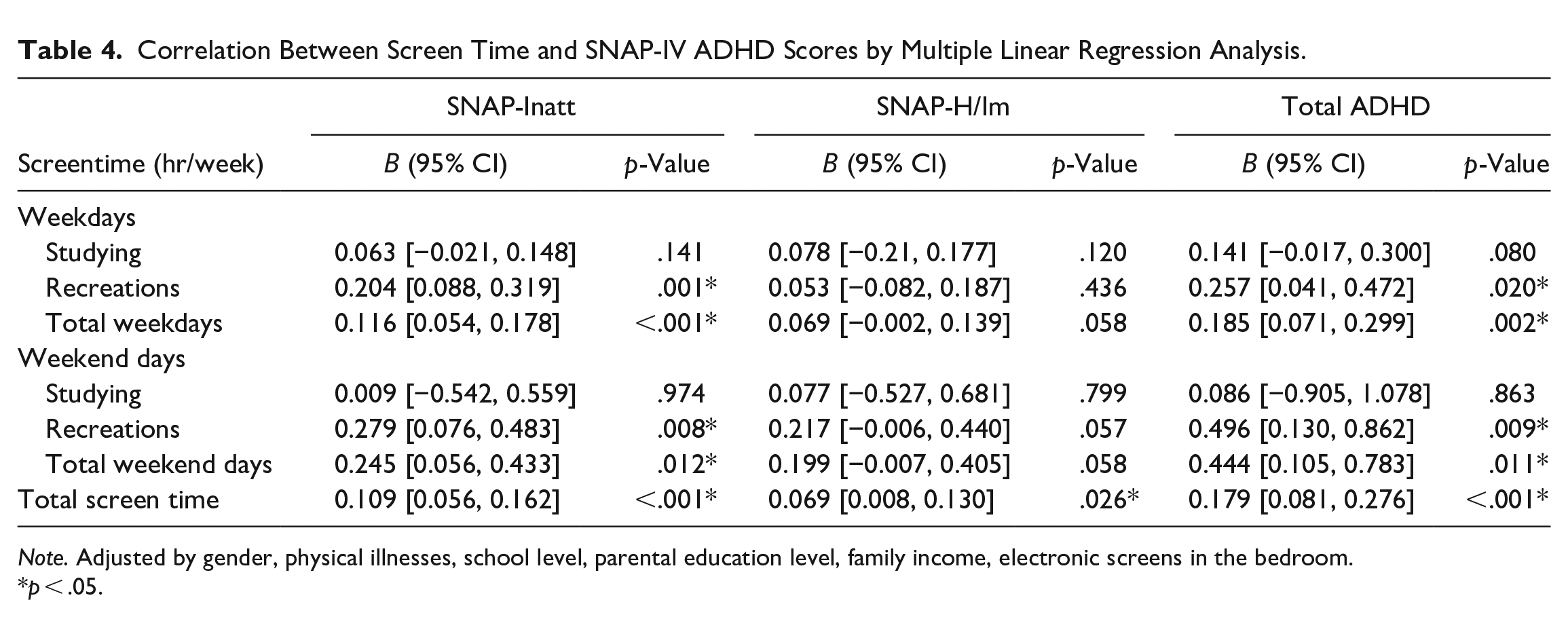
Note. Adjusted by gender, physical illnesses, school level, parental education level, family income, electronic screens in the bedroom.
p < .05.
Screen Time and ADHD Symptoms During and After COVID-19 Lockdown
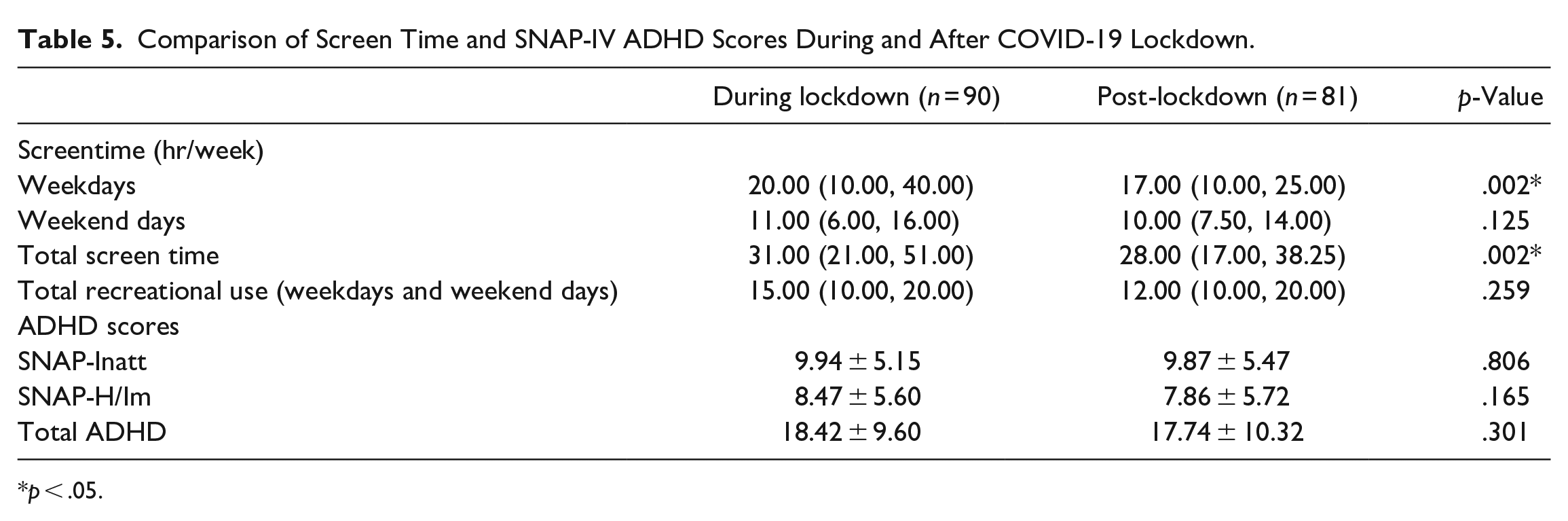
Compared with during lockdown, total screen time and screen time on weekdays were significantly decreased (p = .002). However, screen time on weekend days and the time used for recreations were not significantly changed. ADHD scores (SNAP-Inatt, SNAP-H/Im) were not significantly changed (Table 5).
Comparison of Screen Time and SNAP-IV ADHD Scores During and After COVID-19 Lockdown.
p < .05.
Discussion
This study aimed to investigate the correlation between screen time and symptom severity in Thai children with ADHD during the COVID-19 lockdown. The results of this study showed that, after adjusting with other factors, recreational screen time, both on weekdays and on weekend days, and total screen time, were positively correlated with ADHD scores (both inattention and hyperactive/impulsive subscale scores, and total ADHD scores). Studying screen time, on the other hand, was not associated with ADHD symptom severity. This was supported by the finding that, while the studying screen time was significantly decreased after the lockdown compared to during lockdown, the ADHD scores were not changed.
The results of this study support the hypothesis that, excessive recreational screen time use can affect symptom severity in children with ADHD, particularly during the COVID-19 lockdown period when screen time may have been increased. This is consistent with the finding from the previous study, which found that screen time was associated with negative developmental and behavioral outcomes (Hill et al., 2020; Lissak, 2018). On the other hand, we found that screen time used for studying was not correlated with ADHD symptoms, either inattention or hyperactivity/impulsivity. This finding was in line with the recommendation from the American Academy of Pediatrics (AAP) that does not propose a limitation of screen time for internet-based studying (Council on Communications and Media, 2016).
Compared to during the lockdown period, the children in our study spent less time on screens after the lockdown. The decrease in screen time was due to a decrease in study-related screen time, not recreational screen time. However, the scores on the ADHD scales remained unchanged. This further supports that only recreational screen time affects ADHD symptom severity and that studying screen time does not. Therefore, if there is a situation in which a lockdown is necessary, recreational screen time, not studying screen time, should be limited.
There were some limitations in this study. Firstly, we did not have the data on screen time before the COVID-19 lockdown, so we do not know the extent of the increase in screen time the children used during the lockdown and do not know that the screen time after the lockdown was increased from before the lockdown or not. Secondly, the estimation of screen time might be affected by the recall bias of the participants’ caregivers. Thirdly, we did not control the children’s medication compliance, which could potentially affect the severity of ADHD symptoms. Finally, this study was conducted at a tertiary hospital. Generalization of the results to other clinical settings might be limited.
In conclusion, we found that recreational screen time was correlated with symptom severity in children with ADHD, both inattention and hyperactivity/impulsivity symptoms, during the COVID-19 lockdown, and that studying screen time was not. We recommend that if there is a situation where a lockdown and online education for children are necessary, recreation screen time should be monitored and limited as appropriate, particularly in children with ADHD.
Footnotes
Author Contributions
TS: conception, design, data collection, data analysis and writing of the work. NS: conception, design, critical reviewing and revising of the manuscript. SC: revising of the manuscript. VB: critical reviewing and revising of the manuscript. All authors critically reviewed and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from Siriraj research development fund, Grant number (IO) R016531073, Faculty of Medicine Siriraj Hospital, Mahidol University.