
Abstract
Objective:
The mental health of adults with ADHD was compared to neurotypical controls, and associations between cardiorespiratory fitness (CRF) and mental health were examined.
Method:
Seventy-two participants (n = 36 with ADHD) completed demographic questions assessing ADHD and mental health symptoms. CRF was estimated using the 6-Minute Walk Test and a self-perception question.
Results:
Those with ADHD had significantly poorer mental health outcomes than controls (p < .001), with 50% of adults with ADHD reporting severe to extremely severe symptoms of depression, anxiety, or stress. Critically, lower CRF was associated with worse depression, anxiety, and stress (all p ≤ .03) across both groups. Within the ADHD group, those with higher estimated CRF had significantly lower stress. Among participants with less severe ADHD symptoms, those with higher perceived CRF had significantly lower depressive symptoms.
Conclusion:
In our cross-sectional study, participants with ADHD had poorer mental health than neurotypical controls, and higher fitness was associated with better mental health.
Introduction
ADHD is a common neurodevelopmental disorder that affects approximately 5% of adults globally (Song et al., 2021). In addition to the traditional symptoms of inattention and impulsivity (Felt et al., 2014), many people with ADHD also suffer from mental illness (Katzman et al., 2017; Riglin et al., 2021; Sciberras et al., 2009). Approximately 80% of adults diagnosed with ADHD also present with a psychiatric comorbidity at least once in their lifetime (Klassen et al., 2010). Common comorbidities include major depressive disorder, anxiety disorders, substance use disorders, and personality disorders (Katzman et al., 2017). Unfortunately, when ADHD is comorbid with a mental illness it can be difficult to diagnose and devise a treatment plan to manage the constellation of symptoms (Katzman et al., 2017).
The first approach for managing both ADHD and mental illness typically involves pharmacotherapy (Meppelink et al., 2016); however, prescribing mood stabilizers for conditions such as depression and anxiety on top of stimulant medications for ADHD is not typically recommended given the negative side effects of the drug-to-drug interactions (Brown et al., 2018; Y. Kim et al., 2021; Miklós et al., 2019). Consequently, patients may only be medicated for the most severe symptoms (Katzman et al., 2017). Unfortunately, treating one disorder does not always lead to improvements in the other and in some cases, ADHD medications can exacerbate symptoms of depression (Miklós et al., 2019).
In contrast, treatment approaches that incorporate physical activity can have a potent impact on both symptoms of ADHD (Den Heijer et al., 2017; Y. S. Kim et al., 2012; Ng et al., 2017) and mental illness (Hosker et al., 2019; Oddie et al., 2014) with minimal side effects (Vina et al., 2012). Physical activity is effective at reducing depression and anxiety in neurotypical populations (Kandola, Ashdown-Franks, Stubbs, Osborn, & Hayes, 2019; McDowell et al., 2019; Rebar et al., 2015) and emerging evidence suggests the same may be true for people with ADHD (Da Silva et al., 2020; Den Heijer et al., 2017; K. M. Fritz & O’Connor, 2016).
A key adaptation afforded by long-term engagement in physical activity is improved physical fitness (Boulé et al., 2003; Lin et al., 2015) including better aerobic or cardiorespiratory fitness (CRF). Higher CRF, which reflects our ability to intake and circulate oxygen throughout the body to meet task demands (Caspersen et al., 1985), has been associated with better mental health and fewer incidents of mental illness in neurotypical populations (Kandola, Ashdown-Franks, Hendrikse, et al., 2019; Schuch et al., 2016) and individuals with stress-related exhaustion disorder (Lindegård et al., 2019). Importantly, there is some evidence to suggest that those with ADHD may have lower CRF (K. Fritz & O’Connor, 2018; Jeoung, 2014) and higher incidences of mental illness (C. M. Jensen & Steinhausen, 2015). However, the relationship between CRF and mental health in adults with ADHD has yet to be explored.
The present study aimed to document the relationship between CRF and mental health outcomes. First, we examined the cross-sectional differences in mental health outcomes (depression, anxiety, and perceived stress) between those with ADHD compared to their neurotypical peers. Then, we investigated whether higher CRF was associated with better mental health and explored whether an ADHD diagnosis or ADHD symptom severity moderated that association. We hypothesized that those with an ADHD diagnosis and worse ADHD symptoms would have poorer mental health, but that higher CRF would be associated with a more positive mental health profile across both groups, and perhaps more so for ADHD participants. Given that those with more severe ADHD tend to have worse mental health (Daviss, 2008), and prior research has failed to adequately control for comorbid mental illnesses (Carr et al., 2006; Fisher et al., 2011; Maoz et al., 2018), this research represents an important step in evaluating the effectiveness of alternative approaches for symptom management for adults with ADHD.
Methods
Participants
Eighty-five Canadian young adults between 18 and 35 years old completed this study (May 2021–February 2022). Eligible participants completed the Physical Activity Readiness Questionnaire (PAR-Q) to confirm they could safely complete the physical activity protocol. In addition, eligible participants needed to be fluent in English (read, write, and speak), and have access to a computer and the internet. Finally, they could not have a disorder affecting color vision, for a separate study not included in this manuscript. While those with comorbid mental illnesses were eligible to participate, participants with additional neurodevelopmental diagnoses (e.g., autism spectrum disorder) were deemed ineligible. Those in the ADHD group required a self-reported formal diagnosis from a healthcare professional. In addition, all participants completed the Connors Adult ADHD Rating Scale (CAARS) to assess ADHD symptoms. In the final analysis, all participants in the ADHD group scored above the CAARS 65-point threshold, which is the criteria used to screen for ADHD, while those in the control group needed to score below 65. In total, 13 participants were excluded after completing the protocol (control = 7; ADHD = 6) due to missing data (n = 1), no formal ADHD diagnosis (n = 1), or not meeting CAARS score cut-offs (control = 7; ADHD = 4). As part of a broader study exploring CRF on cognition, a sample size calculation was conducted using G*Power version 3.1.9.2 (Faul et al., 2009), for linear multiple regression (fixed model, R2 deviation from zero) with Cohen’s f set to = 0.23 (Newson & Kemps, 2008), a conservative β = .95 and α = .05. Results indicated that 71 participants were sufficient. The final analysis consisted of 72 participants (36 ADHD, 36 non-ADHD). All participants provided informed consent before study participation and were provided with monetary compensation. The study was approved by the McMaster Research Ethics Board (MREB) of McMaster University (Project ID 5111).
Materials
Conner’s Adult ADHD Rating Scale (CAARS)
The CAARS was used to assess ADHD symptoms (Conners et al., 1999). The CAARS is a 30-item self-report questionnaire and is a commonly used validated tool to “screen for the presence and severity of ADHD symptoms in adults aged 18 and older” (MHS Assessments, 2021). Each item was ranked by participants on a scale from 0 to 3 in increasing severity (“not at all, never” = 0, “just a little,” “once in a while” = 1, “pretty much, often” = 2, and “very much, very frequently” = 3). Overall scores were calculated manually using guidelines outlined by Multi-Health Systems, with a score of 65 or higher indicating the presence of ADHD and higher scores indicating greater ADHD symptom severity. The CAARS assessment has been used frequently in research examining adults with ADHD and has demonstrated good reliability and validity with an overall efficiency rate of 85% (Adler et al., 2008; Conners et al., 1999).
Depression Anxiety and Stress Scale (DASS)
The DASS was used to assess mental health and well-being. The DASS consists of 42 items that evaluate the severity of depression, anxiety, and perceived stress symptoms (Imam, 2008). Items specific to each disorder include a list of four statements graded on a scale from 0 to 3 in increasing severity (“did not apply to me at all” = 0, “applied to me to some degree” = 1, “applied to me to a considerable degree” = 2, and “applied to me very much” = 3). The total score within each category was then summed, with a higher score indicating greater symptom severity for each category. Cut-offs have been established to determine normal, moderate, severe, or extremely severe symptoms of depression, anxiety, and stress (see Lovibond & Lovibond, 1995 for cut-off details). The DASS is a valid and reliable measure when used in both clinical and non-clinical populations (Pooravari et al., 2017; Vignola & Tucci, 2014).
Estimated Cardiorespiratory Fitness
Distance reported from the six-minute walk test (6MWT) was combined with the participant’s self-reported body weight, sex, age, and resting heart rate (which was the average of three measurements) to estimate one’s maximal oxygen consumption or VO2 max, an indicator of CRF (Burr et al., 2011). The “6WT” mobile application was used to record the distance of the 6MWT, which is used to estimate CRF (Stienen et al., 2019). This application has been validated and used in previous research (Marashi et al., 2021; Stienen et al., 2019). Participants completed the test outside and were required to walk as fast as they could in a straight line for 6 min, without running or jogging. Additionally, participants were advised to find a flat path and avoid walking in areas with tall buildings where possible, to eliminate disruptions to the GPS signal used to calculate the distance walked. At the end of the 6 min, the application provided a total distance which participants reported once they returned from their walk. Heart rate measurements were completed using the “Instant Heart Rate” mobile application by Azumio. The application uses photoplethysmography, changes in blood volume during circulation, to measure heart rate (Castaneda et al., 2018). Participants held their finger over their smartphone camera for 30 s while the flashlight was on and using an advanced algorithm, the application calculated their heart rate by monitoring color changes each time there was a heartbeat. The application has shown concurrent validity with other more accurate heart rate measures such as the “FT7 Polar” and has acceptable test-retest reliability (Mitchell et al., 2016). Equation 1 was used to calculate CRF (Burr et al., 2011), as it is a valid and reliable measure that accounts for approximately 72% of the variance associated with the gold-standard measure for cardiorespiratory fitness (Burr et al., 2011; Marashi et al., 2021).
Perceived Cardiorespiratory Fitness
Participants reported perceived CRF by responding to the question: “In general, I would say that my current aerobic fitness (ability to walk/run distances) is: Excellent (4), Very Good (3), Good (2), Fair (1), Poor (0).” Given the virtual nature of our estimated-CRF measure (which was necessary due to COVID-19 pandemic restrictions), perceived CRF was included as a secondary estimate of fitness. Previous literature reports positive correlations between estimated CRF and perceived fitness in neurotypical populations (K. G. Jensen et al., 2018; Monroe et al., 2010).
Procedure
As part of a larger project, participants completed a 2.5-hr virtual visit via Zoom (Version 5.11.10) during which the primary measures were assessed. Participants completed a series of questionnaires including a demographic questionnaire, the CAARS, the DASS, and the question on perceived CRF. Then, participants took a 5-min quiet rest (monitored by the researcher) before taking three samples of their resting heart rate using the Instant Heart Rate application. Participants then left the Zoom call to independently complete the 6MWT, which was used to estimate CRF. Once completed, participants returned to the Zoom call to report their results and debrief with the researcher.
Statistical Analysis
Data were analyzed using IBM SPSS (Version 28). Descriptive statistics were computed for all variables, and normality was assessed via the Shapiro-Wilk statistic, skewness and kurtosis, and visual inspection. Perceived fitness was treated as an ordinal variable, which was originally measured on a 5-point scale (i.e., Excellent, Very Good, Good, Fair, Poor); however, to meet the assumptions of a chi-squared test, the categories were collapsed into (1) Excellent/Very Good, (2) Good, and (3) Fair/Poor. This three-category perceived fitness variable was then used for subsequent analyses. Estimated CRF was treated as a continuous variable. A two-tailed Spearman’s correlation was used to test whether estimated and perceived CRF were related to one another. Independent samples t-tests were computed to determine whether mental health outcomes and estimated CRF differed by group (ADHD vs. Control). A chi-squared test was used to investigate whether perceived CRF was different between groups. Regression analyses were used to test whether estimated CRF and perceived CRF predicted mental health outcomes. Hayes PROCESS Macro, Version 4.1 SPSS plug-in (Model 1) was used to conduct exploratory moderation analyses to determine whether the relationship between CRF (IV) and mental health (DV) differed by group (ADHD vs. Control) or CAARS score within the ADHD group (moderator). All analyses were set to an alpha level of less than 0.05. Biological sex was used as a covariate in all regression and moderation analyses as sex differences have been noted in ADHD symptoms (Fedele et al., 2012), CRF (Al-Mallah et al., 2016; Dimech et al., 2019), and mental health (Altemus et al., 2014). ADHD medication was used as a covariate in analyses for the ADHD group to determine whether the association between CRF and mental health remained after controlling for ADHD medication use.
Results
Descriptive Statistics
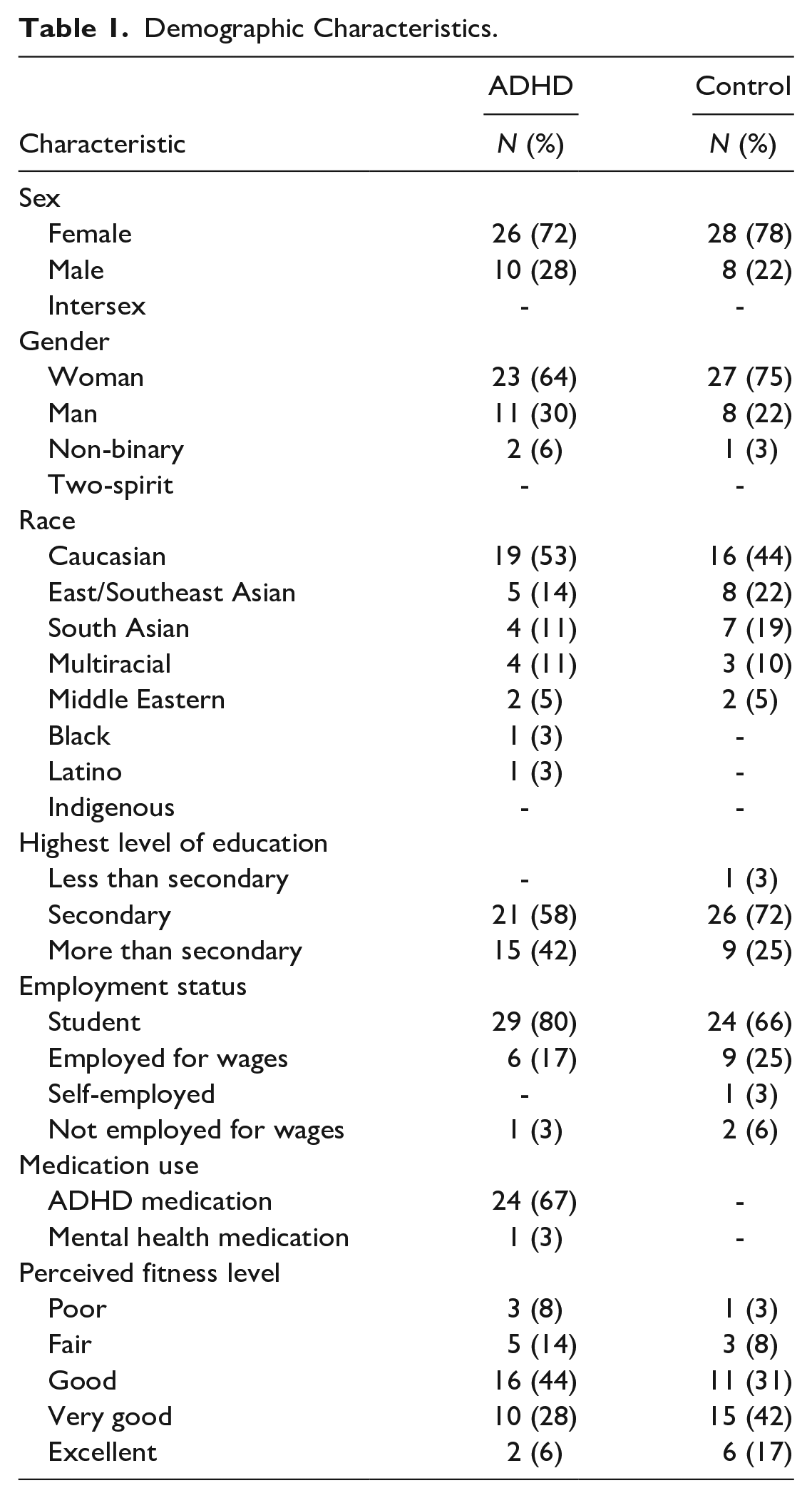
Descriptive statistics are presented in Table 1. Participants on average were 21.0 years old (±3.0) and were predominately female (75%). Most participants were white university students. Sixty-seven percent of participants with ADHD were currently taking medication for their ADHD symptoms, and 81% had been prescribed ADHD medication at some point. All participants with ADHD had a CAARS score of 65 or higher (79.9 ± 7.0) whereas all controls had a CAARS score below 65 (49.1 ± 8.3) (See Table 2).
Demographic Characteristics.
Mental Health and CRF Outcomes.
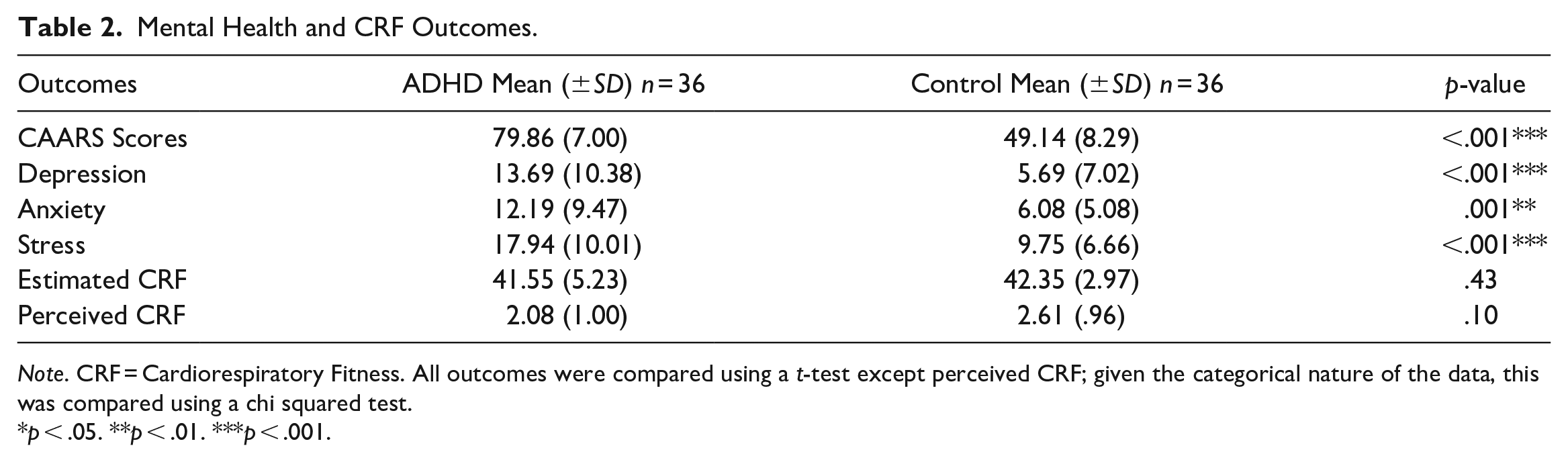
Note. CRF = Cardiorespiratory Fitness. All outcomes were compared using a t-test except perceived CRF; given the categorical nature of the data, this was compared using a chi squared test.
p < .05. **p < .01. ***p < .001.
Mental Health
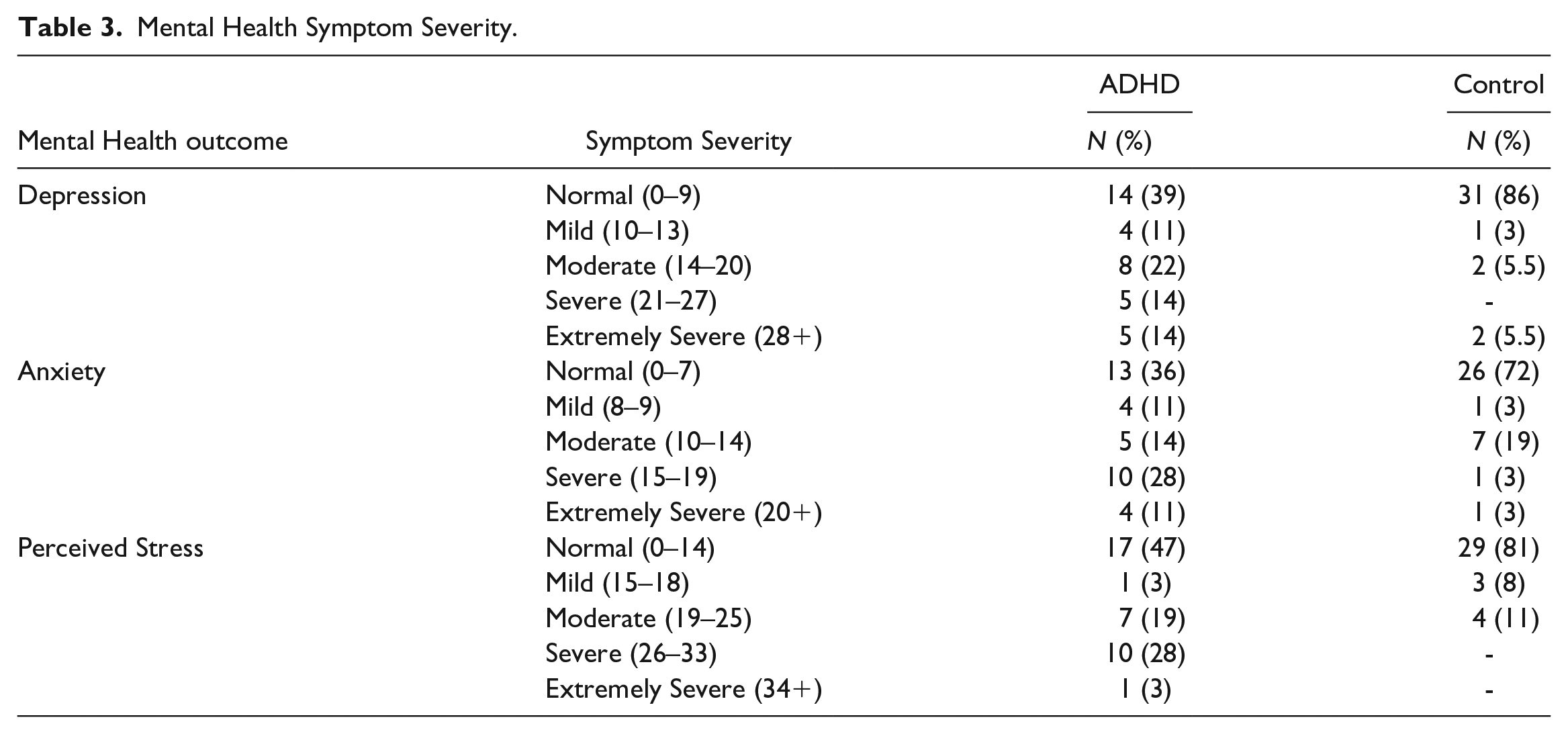
Individuals in the ADHD group had significantly greater depression (t(70) = 3.83, p < .001), anxiety (t(70) = 3.41, p = .001), and perceived stress (t(70) = 4.09, p < .001), indicating worse mental health compared to controls (See Table 2). Sixty-seven percent of participants with ADHD reported moderate to extremely severe symptoms in at least one subscale of depression, anxiety, or perceived stress, while the same was only observed for approximately 36% of controls (Table 3; Figure 1).
Mental Health Symptom Severity.
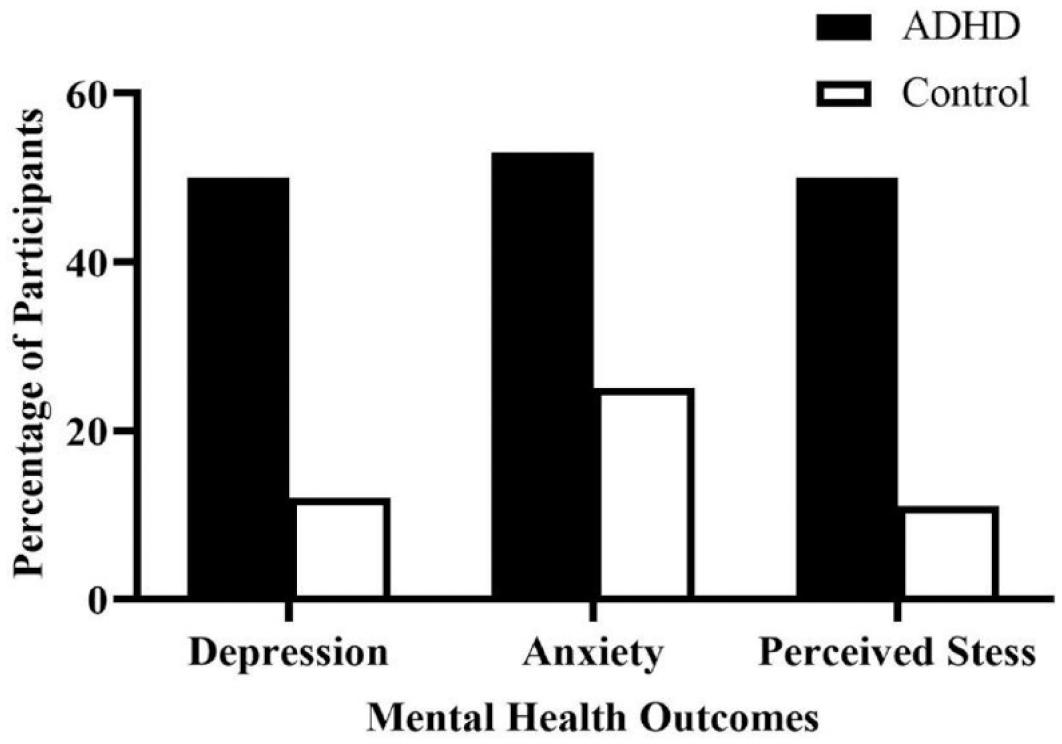
Percentage of participants experiencing moderate to severe depression, anxiety, and perceived stress symptoms, as measured by the DASS.
Fitness
Estimated CRF and perceived CRF were positively correlated (r(70) = .34, p < .01). Neither estimated CRF (p = .43) nor perceived fitness (p = .10) were significantly lower in the ADHD group compared to controls.
Fitness × Mental Health
Higher estimated CRF was associated with lower perceived stress scores [ΔR2 = .07, F(2, 69) = 3.35, p = .03], accounting for 7% of the variance (Table 4). This relationship was not moderated by the group (Table 5), but it was moderated by ADHD symptom severity for participants with ADHD (b = 0.10, SE b = 0.05, 95% CI [.004, .19] (Figure 2). Specifically, the relationship between higher estimated CRF and less perceived stress was statistically significant for the individuals with less severe ADHD symptoms but not for those with more severe symptoms (Figure 2; Table 6).
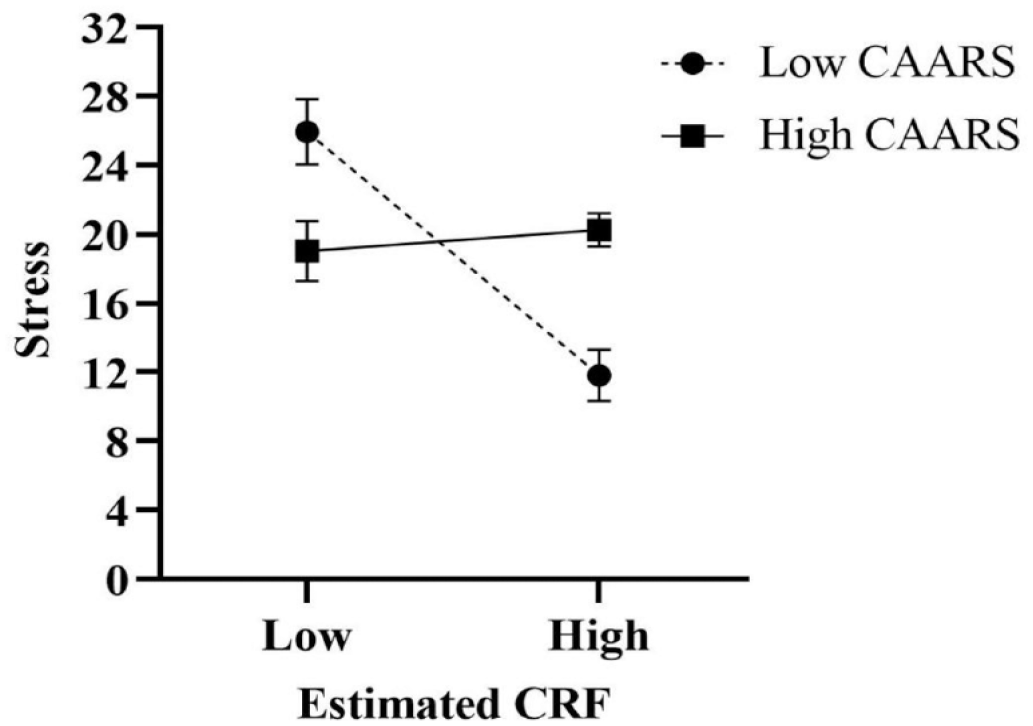
The moderating effect of ADHD symptom severity (CAARS) within the ADHD group on the relationship between estimated CRF and stress. Error bars represent standard error. “Low CAARS” represents one standard deviation below the mean CAARS score (65.0–72.9) and “High CAARS” represents one standard deviation above the mean CAARS score (86.9–90.0), within the ADHD group.
Linear Regression Table for Estimated and Perceived CRF Predicting Mental Health Outcomes.
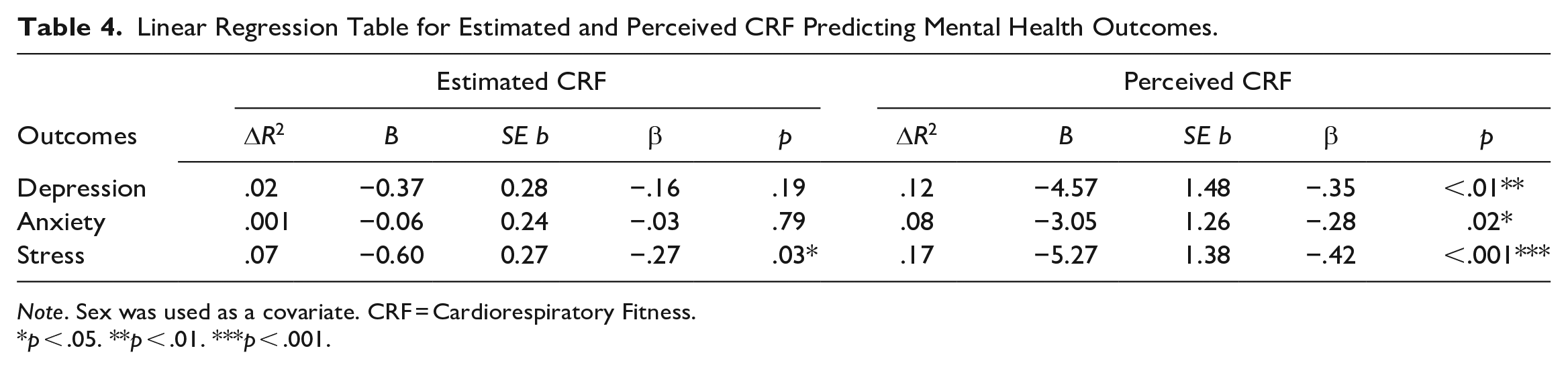
Note. Sex was used as a covariate. CRF = Cardiorespiratory Fitness.
p < .05. **p < .01. ***p < .001.
Regression Coefficients of the Moderating Effect of Group (ADHD vs. Control) on Estimated CRF and Mental Health Outcomes.
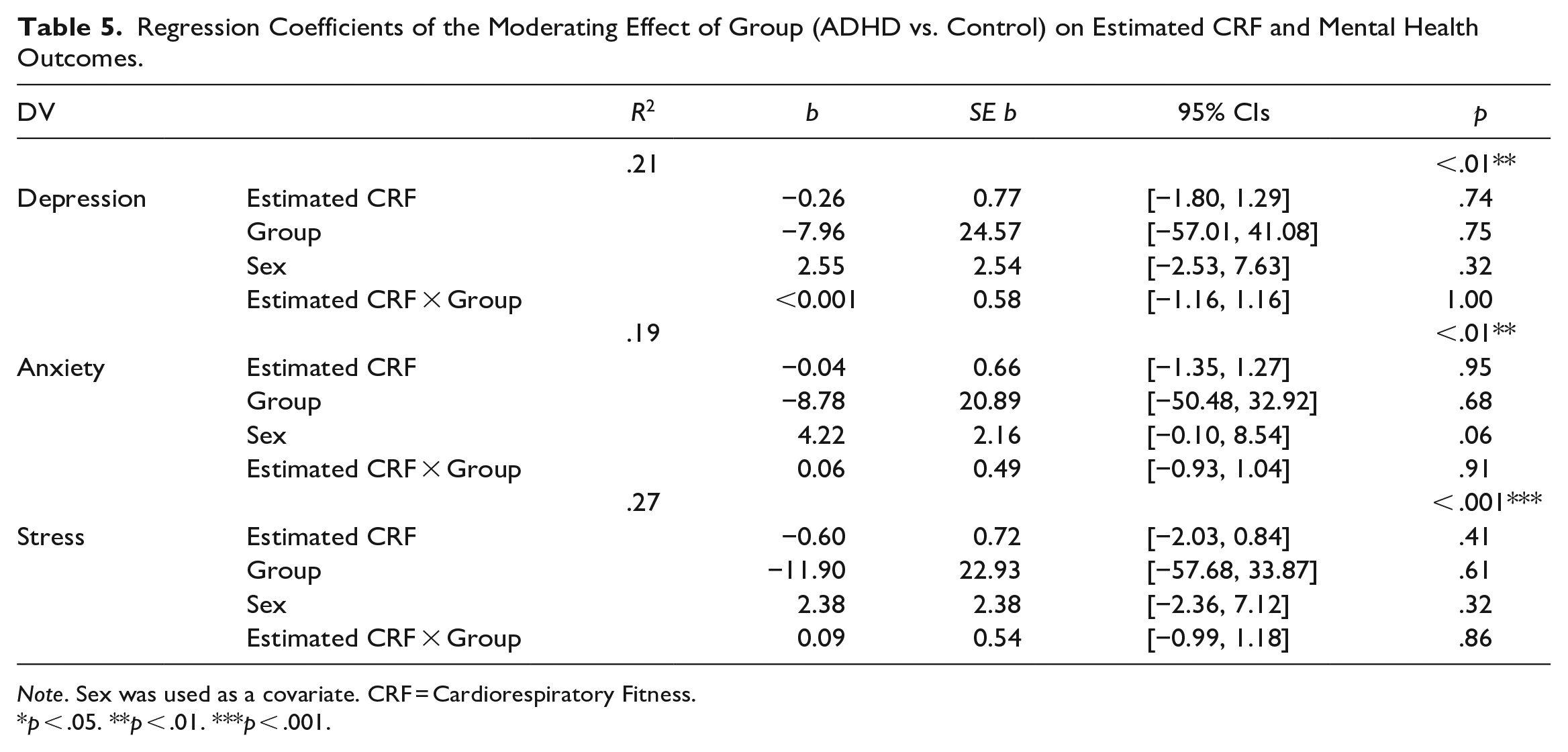
Note. Sex was used as a covariate. CRF = Cardiorespiratory Fitness.
p < .05. **p < .01. ***p < .001.
Regression Coefficients of the Moderating Effect of ADHD Symptom Severity (CAARS Score) on Estimated CRF and Mental Health Outcomes.
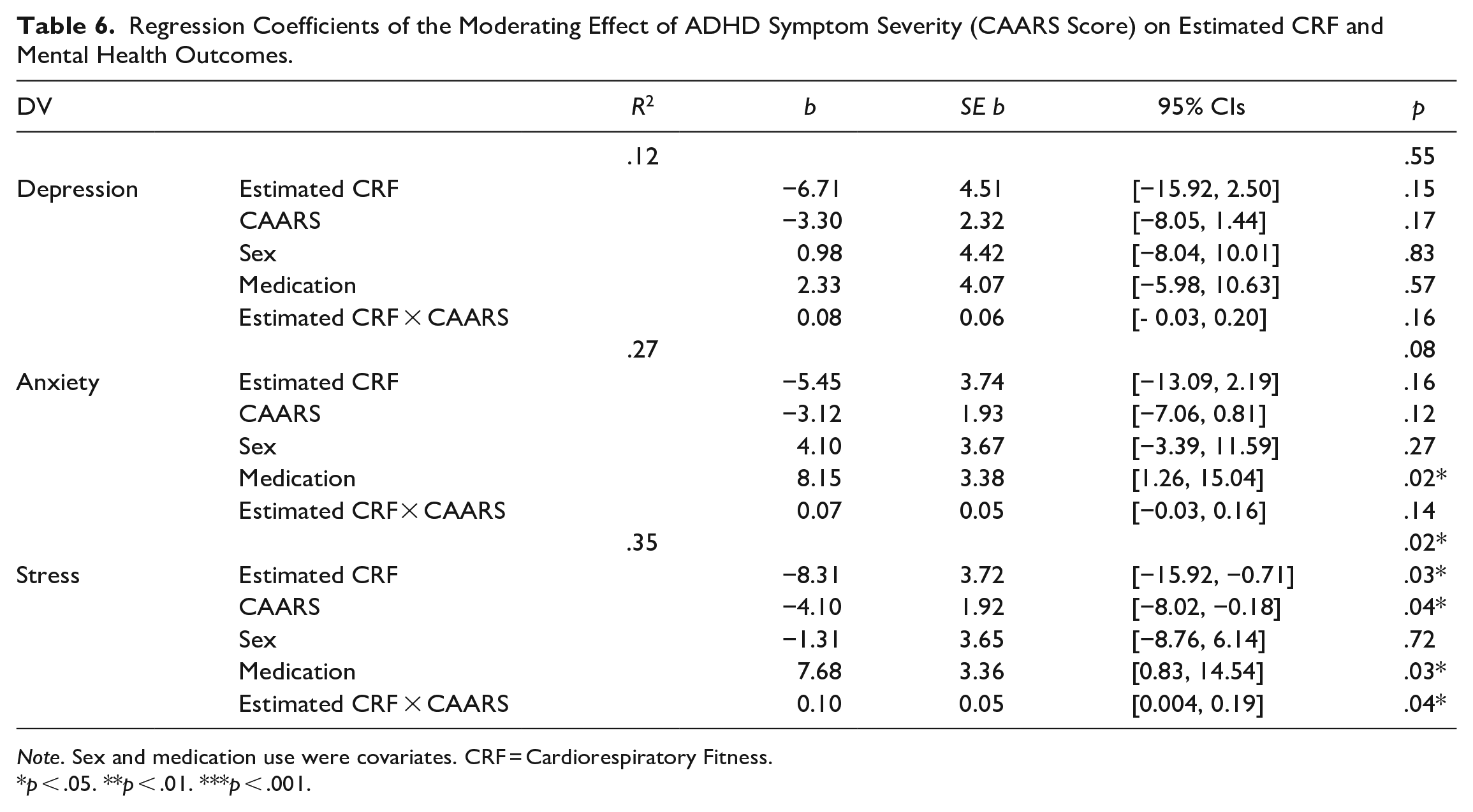
Note. Sex and medication use were covariates. CRF = Cardiorespiratory Fitness.
p < .05. **p < .01. ***p < .001.
Higher perceived fitness was associated with less depression [ΔR2 = .12, F(2, 69) = 5.40, p < .01], anxiety [ΔR2 = .08, F(2, 69) = 4.44, p = .02], and perceived stress [ΔR2 = .17, F(2, 69) = 8.20, p < .001], accounting for 12%, 8%, and 17% of the variance, respectively (Table 4). However, only the relationship between perceived CRF and depression was moderated by the presence of ADHD (b = 7.39, SE b = 2.71, 95% CI [1.98, 12.80] (Figure 3). Specifically, the relationship between higher perceived CRF and less depression was stronger in people with ADHD than in those without (Figure 3; Table 7). Symptom severity within the ADHD group did not moderate the relationship between perceived CRF and mental health outcomes (Table 8).
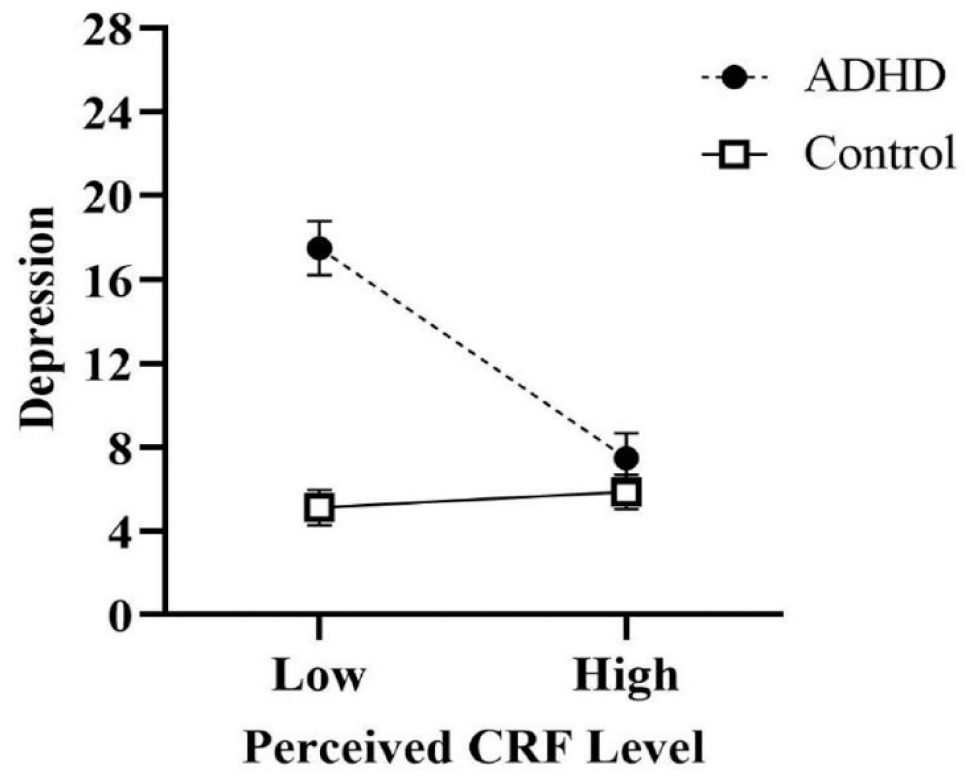
The moderating effect of group (ADHD vs. Control) on the relationship between perceived CRF and depression. Error bars represent standard error.
Regression Coefficients of the Moderating Effect of Group (ADHD vs. Control) on Perceived CRF and Mental Health Outcomes.
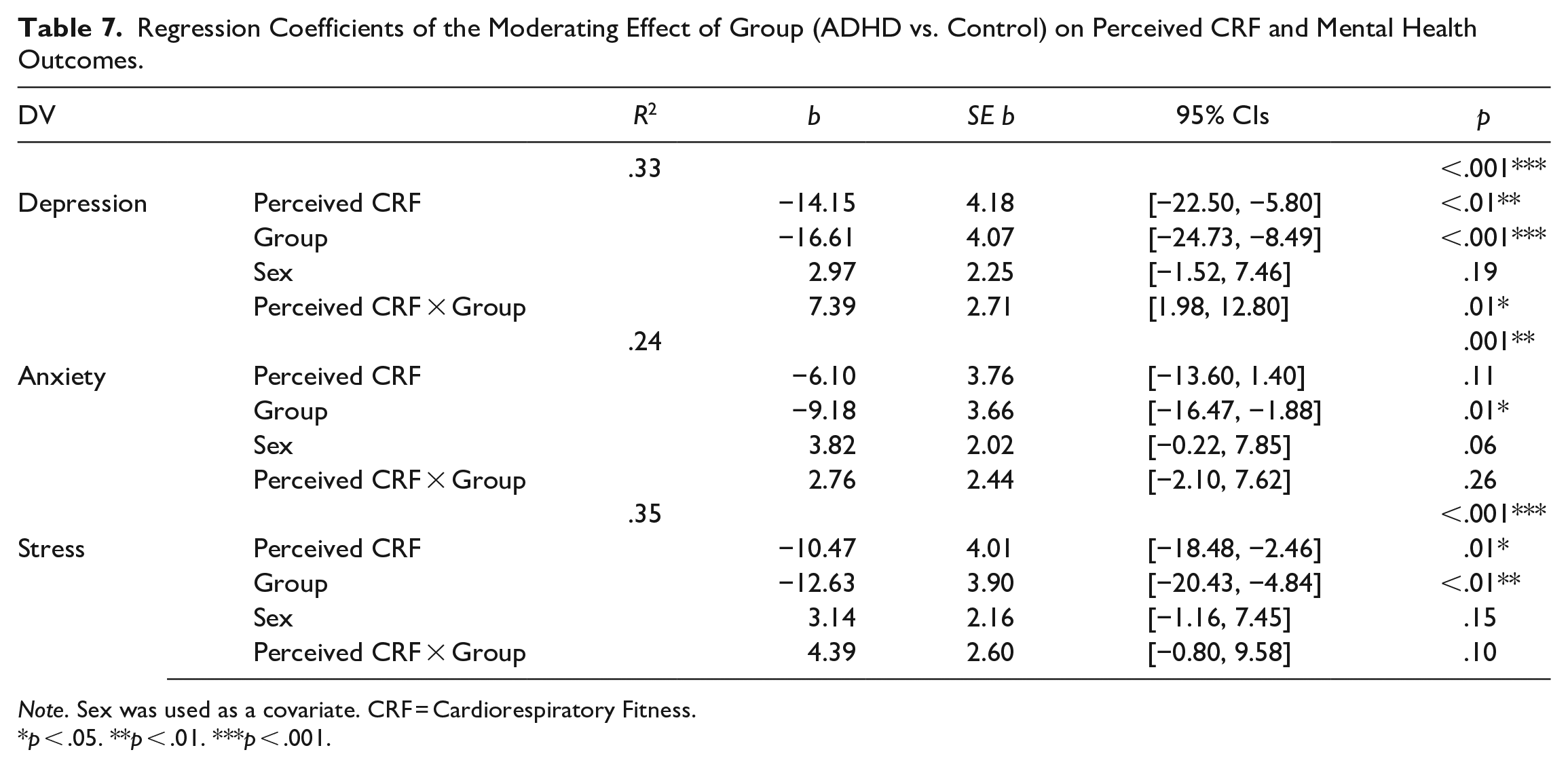
Note. Sex was used as a covariate. CRF = Cardiorespiratory Fitness.
p < .05. **p < .01. ***p < .001.
Regression Coefficients of the Moderating Effect of ADHD Symptom Severity (CAARS) on Perceived CRF and Mental Health Outcomes.
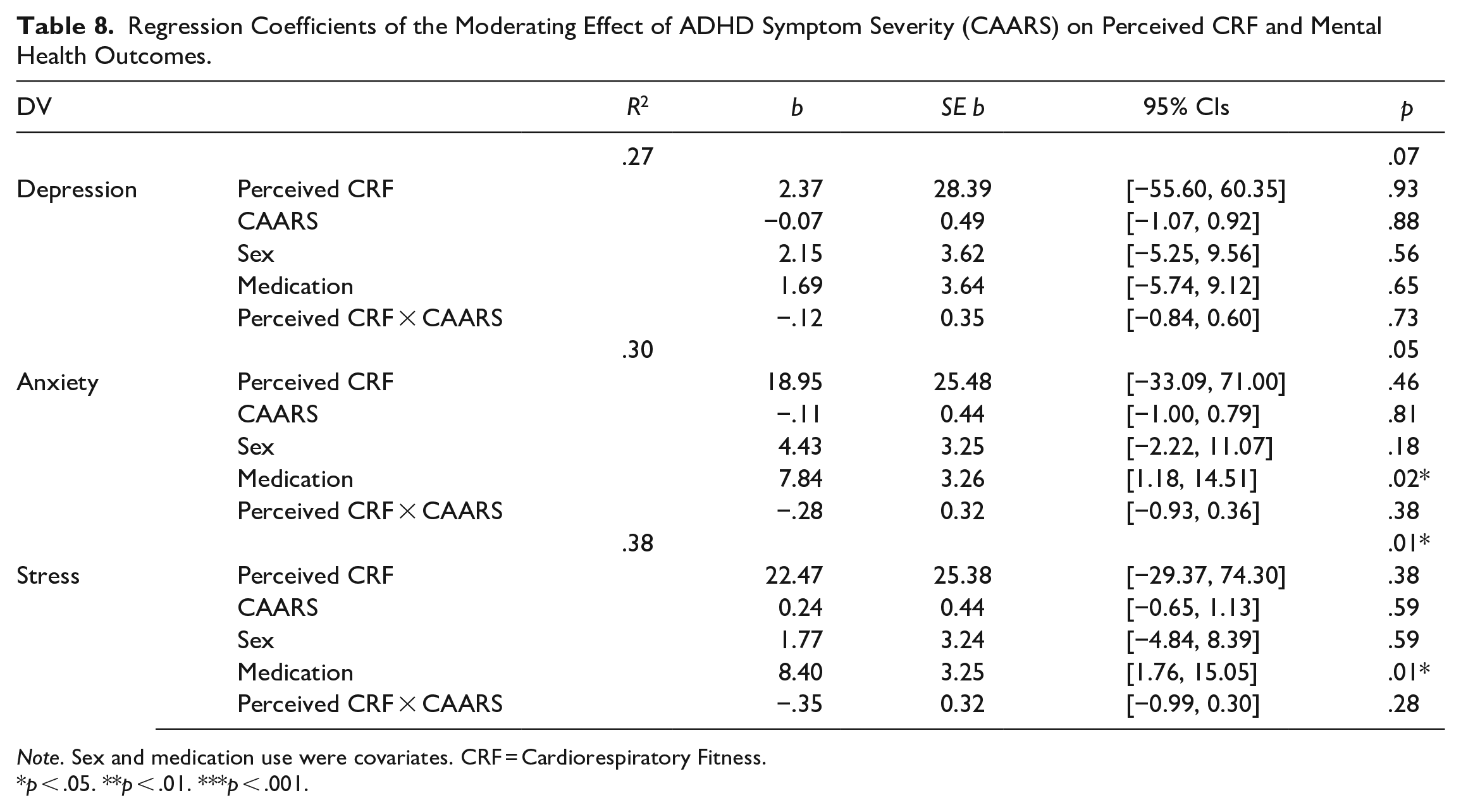
Note. Sex and medication use were covariates. CRF = Cardiorespiratory Fitness.
p < .05. **p < .01. ***p < .001.
Discussion
The present study examined the incidence of poor mental health among individuals with ADHD compared to their neurotypical peers, while also exploring the association between mental health and cardiorespiratory fitness (CRF). Compared to neurotypical participants, those with ADHD had poorer mental health. Critically, higher CRF was associated with less depression, anxiety, and perceived stress, especially for those with ADHD.
The comorbidity between ADHD and mental illness is challenging for many reasons including the issue of treating both conditions simultaneously given the negative interactions between their respective pharmacotherapies (Brown et al., 2018). Alarmingly, 50% of ADHD participants reported severe or extremely severe symptoms of depression, anxiety, or perceived stress and those with more severe ADHD symptoms were more mentally distressed. Critically, this degree of mental health symptom severity was not reported by the control group, highlighting the unique vulnerability to mental health issues faced by adults with ADHD. Notably, over 80% of our participants in the ADHD group reported taking medication for their ADHD symptoms (either currently or at some point since their diagnosis) and those currently taking ADHD medication (67%) reported greater anxiety and stress symptoms than those who were not. In contrast, only one participant formally disclosed taking medication for their mental health, suggesting there may be an important treatment-gap for mental health in adults with ADHD.
The bidirectional relationship between ADHD and mental health means that the two can exacerbate each other (Austerman, 2015). Mental illnesses like depression and anxiety can impair concentration and augment the cognitive and behavioral symptoms of ADHD (Pan & Yeh, 2017). Although it is true that mood and emotional problems can be a side effect of ADHD medications (Tobaiqy et al., 2011), many people with ADHD report experiencing anxiety and depression from the sheer act of navigating in a world that is constrained by neurotypical societal expectations (e.g., the expectation that one must sustain focus for long periods of time at work or school) (Björk et al., 2018). Poorer academic achievement, poorer occupational attainment, and lower socioeconomic status are some of the negative fallouts of such a mismatch (Arnold et al., 2020; Goffer et al., 2022), which in turn, can exacerbate their psychological burden. Therefore, in addition to advocating for societal shifts to promote the inclusivity of neurodivergence, there is an immediate need for mental health support for individuals with ADHD.
While acknowledging the cross-sectional nature of our data, our results suggest that increasing physical fitness may be a promising mental health strategy for adults with ADHD. Across both groups, higher CRF was associated with less depression, anxiety, and perceived stress symptoms. Among participants with ADHD, those with higher perceived CRF had fewer depressive symptoms and those with higher estimated CRF had lower perceived stress levels. Notably, these fitness-related differences for ADHD participants were associated with categorical differences in mental health symptom severity. Specifically, higher fit individuals were classified as “normal” for depression and perceived stress, whereas lower fit individuals were classified as “moderate” for depression and “severe” for perceived stress. When compared to their neurotypical peers, the average estimated CRF for participants with ADHD was not statistically different. Prior research has reported lower CRF in men with ADHD (K. Fritz & O’Connor, 2018; Jeoung, 2014), whereas our sample was predominantly women (ADHD = 64%; control = 75%), suggesting there may be gender or sex differences to explore. It is also important to note that the association between fitness and perceived stress was only observed for individuals with mild ADHD symptoms. Those with more severe ADHD symptoms did not see a similar pattern, suggesting that this subset may require additional support to protect against poor mental health.
Strengths and Limitations
Although the virtual nature of the protocol provided engagement opportunities for those who may not have been able to participate in a laboratory-based setting, it created limitations too. Gold-standard measures for estimating CRF were unavailable (i.e., VO2 max tests); instead, participants self-completed HR measurements and a 6MWT which was unsupervised and completed on an unstandardized path. Although both measures were correlated (r = .34, p < .01), the self-reported measure of CRF was more sensitive to individual variations in mental health. Specifically, higher perceived CRF was associated with lower depression, anxiety, and perceived stress, whereas higher estimated CRF was only associated with lower perceived stress. These minor differences in associations with the CRF measurements may reflect the risk of measurement error due to the virtual nature of the study design and point to the need for further lab-based studies that include standardized questionnaires to assess perceived CRF (e.g., Monroe et al., 2010) and gold standard approaches for estimated CRF (e.g., VO2 max). Virtual protocols also introduce selection biases; participants needed a computer, smartphone, and internet access to participate. Furthermore, given the cross-sectional study design, we are unable to speak about the causality of the observed relationships between CRF and mental health in adults with ADHD; it is possible that those with poor mental health are less likely to maintain a regular exercise regime needed to increase fitness. Through randomized controlled trials, both causality and mechanisms can be explored to determine whether CRF is a modifiable and protective factor for this population and, therefore, such an approach would be advisable for future research.
Conclusions
In our sample, participants with ADHD had poorer mental health than neurotypical controls. However, having higher fitness was associated with better mental health. Specifically, among those with less severe ADHD symptoms, higher CRF was associated with less depression, anxiety, and perceived stress. Future research is needed to examine the causal relationship between fitness and mental health in adults with ADHD, while also accounting for individual differences in the severity of both ADHD and mental health symptoms.
Footnotes
Acknowledgements
The authors would like to thank Victoria Cirone for her support on the project and members of the NeuroFit Lab.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by Tier 2 Canada Research Chair in Brain Health and Aging [20013825].