
Abstract
Background
The prevalence of ADHD in community samples of school-aged children (6-18 years old) varies from 5% to 7% in the United States (Polanczyk, Silva de Lima, Lessa Horta, Biederman, & Rohde, 2007; Willcutt, 2012) and is estimated at about 5% in France (Aubron, 2007; Haute Autorité de Santé [HAS], 2012; Quiviger & Caci, 2014). ADHD is associated with significant impairment affecting many domains, including familial, social, and academic functioning. It can also have long-term consequences on quality of life in adulthood (Caci et al., 2014; Cantwell, 1996; Hodgkins et al., 2012; Klein et al., 2012; Shaw et al., 2012).
The long delay between initial onset of the symptoms and formal diagnosis of ADHD has raised concern as it may result in increased functional impairment (e.g., poorer educational and psychosocial outcomes; Cantwell, 1996; HAS, 2012; Klein et al., 2012; Purper-Ouakil et al., 2007). This is particularly regrettable with regard to the extensive scientific evidence showing that children with ADHD may gain considerable benefit from a range of interventions, including medication, individual therapy, and educational support (American Academy of Pediatrics [AAP], Subcommittee on Attention-Deficit/Hyperactivity Disorder and Committee on Quality Improvement, 2001; Swanson et al., 1998). It has been suggested that early identification of ADHD symptoms may facilitate early referral and treatment, and limit individual and social impairment caused by ADHD (AAP, Subcommittee on Attention-Deficit/Hyperactivity Disorder and Committee on Quality Improvement, 2001; Foy & Earls, 2005; Klein et al., 2012). Recent international guidelines highlight the need for a better understanding of how these children and their families access health care services, to identify possibilities for improvement (APA, 2000; AAP, Subcommittee on Attention-Deficit/Hyperactivity Disorder and Committee on Quality Improvement, 2001). In addition, parental satisfaction has been regarded as an important factor in the course of diagnosis and/or treatment of children with ADHD in qualitative studies based on family interviews (Dennis, Davis, Johnson, Brooks, & Humbi, 2008; Dosreis et al., 2003; Johnson & Marsh, 2001; Leslie, Plemmons, Monn, & Palinkas, 2007); however, this assumption has been underinvestigated in studies with sufficiently large samples.
In the “Without Boundaries” survey, conducted in nine countries (Australia, Canada, Germany, Italy, Mexico, Netherlands, Spain, the United Kingdom, and the United States), the mean time from initial contact with a professional to correct diagnosis was nearly 24 months (World Federation for Mental Health [WFMH], 2004). However, regional differences in mental health department structures make extrapolation from international studies difficult. For example, access to services depends on the degree of insurance coverage, which differs in many countries. The only study conducted in France (Purper-Ouakil et al., 2007) reported on 129 children with ADHD referred to a French teaching hospital outpatient clinic. It found that the mean time to diagnosis was 33 months. However, results may have been partly biased due to the fact that participants were recruited in just one teaching hospital outpatient clinic. Regional disparities in access to treatment for ADHD (AAP, Subcommittee on Attention-Deficit/Hyperactivity Disorder and Committee on Quality Improvement, 2001) may also potentially prevent generalization of these results.
The aim of this study is to describe the health care trajectories in a sample of French children with ADHD. Along the trajectory, each time a new health care professional (HCP) is met, it is considered to be a “milestone,” and the time between two consecutive milestones is called a “stage.” The secondary objective is to describe clinical and familial and health care service characteristics, and level of satisfaction of families.
Patients and Methods
Procedure
The multicentric, cross sectional QUEstionnaire on the STages of the ADHD care pathway (QUEST) survey was conducted in France between November 4, 2013 and January 31, 2014. The study was implemented under the supervision of a steering committee of child psychiatrists and child neurologists treating and researching ADHD, and the study sponsor (Shire Legal Entity). A national sample of physicians treating children with ADHD each received 10-paper questionnaires. Physicians took part on a voluntary basis. They were instructed to hand out the questionnaires to caregivers of children in whom ADHD had been confirmed. The questionnaires were also available online. An English version of this questionnaire is available in addition to this article.
Eligible patients were under the age of 18 in whom ADHD diagnosis had been confirmed by the clinician (no exclusion criterion was defined). Caregivers had to fill out the questionnaires. At the end of the inclusion phase, the questionnaires were returned to a central facility for data entry in a specially compiled, confidential database, in which they were added to forms completed online. In accordance with the French data protection law, the survey was declared to the French data protection authority (Commission Nationale de l’Informatique et des Libertés [CNIL]). We collected 599 questionnaires, 473 (79%) of which could be used for the statistical analysis. Questionnaires not stating the number of stages or first meeting with a HCP or questionnaires concerning adults were excluded (Figure 1).
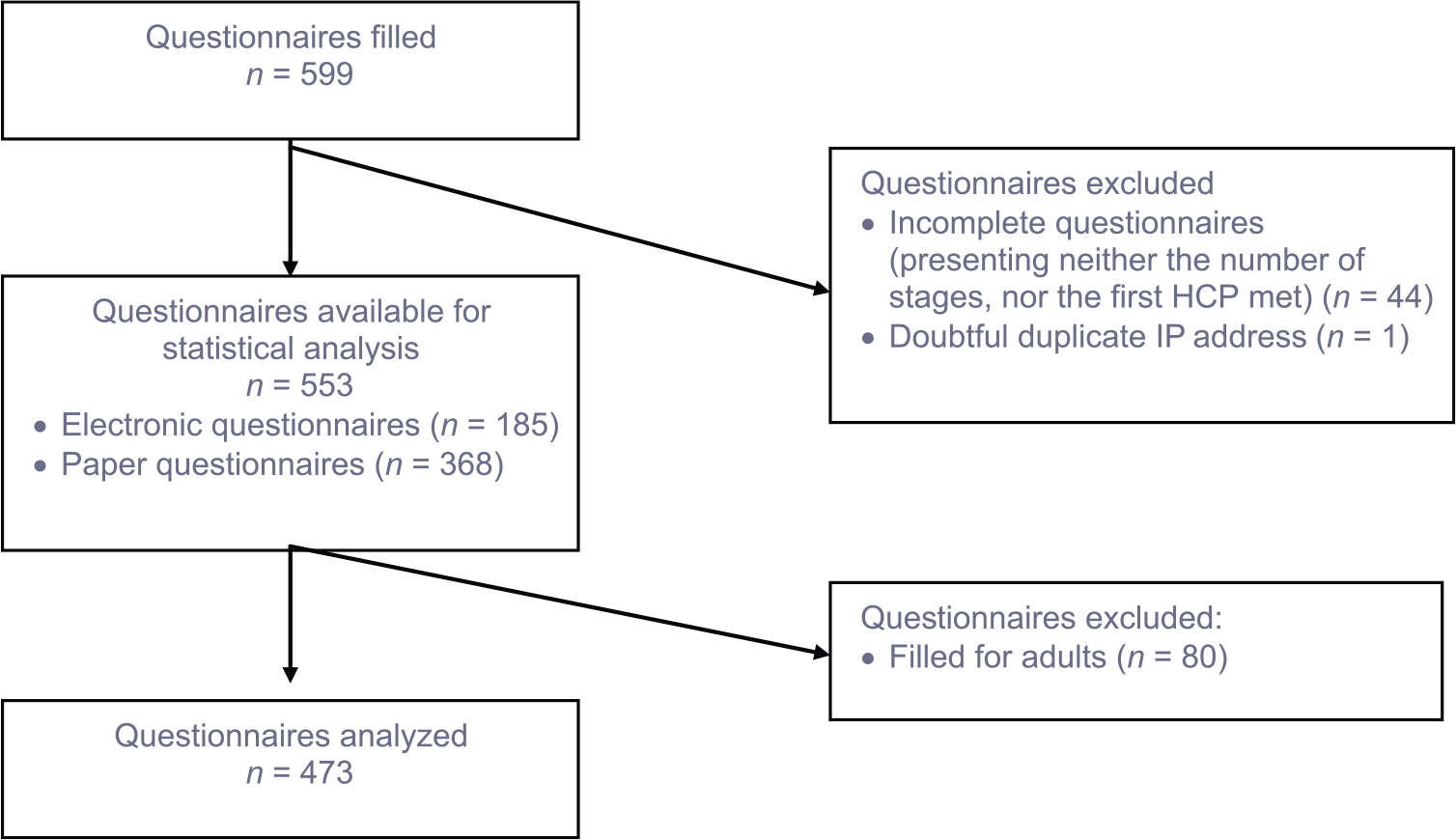
Questionnaire analysis flowchart.
Questionnaire
The QUEST survey was divided into three different parts. The first part involved questions on the child’s sociodemographic characteristics (e.g., age, gender) and the caregiver’s sociodemographic characteristics (e.g., gender, age, education level). The second part described the successive stages of the health care trajectory in detail, in three subsections.
The first subsection focused on the period prior to the first consultation with an HCP: for example, the child’s age when the first symptoms were noticed either by a family member or someone else.
We then examined investigations and referrals from the first to the last consultation with an HCP along the health care trajectory.
Finally, we explored the pharmacological and nonpharmacological treatments offered after ADHD diagnosis was confirmed. Patients and their families also described any paraclinical examinations and current social skills and situation concerning adaptation to school.
The third and last part questioned families on their level of satisfaction at each milestone. It was measured on a Likert-type scale with scores ranging from 0 to 10. A score of 6 and below indicated a “low level of satisfaction.” The main reasons for low level of satisfaction were collected.
Statistical Methods
Incomplete records were not used. The descriptive statistics used included median, mean, quartiles, interquartile range and standard deviation for numerical data, and count with related percentages for categorical data. Patient histories to the time of diagnosis of ADHD were reconstructed from the answers provided and included in the descriptive data analysis. All subsample comparisons were made using statistical hypothesis testing: chi-square tests for categorical data and Student’s t test or Mann–Whitney U test for numerical data (if data distribution was not normal). All p values are given as nominal values without correction for Type I error. Combined multiple correspondence analysis (MCA) and hierarchical clustering analysis (HCA) were used to define patient profiles according to the first ADHD signs reported.
Results
Sociodemographic and Clinical Characteristics
Among the 473 patients in the series, 382 were boys (81%) and the median age was 11.0 years. A total of 237 patients (50%) were in primary school, and 209 in secondary school (44%). Thirty-nine participants (8%) had specific educational needs, and one in four (24%) received care from a classroom assistant. About one third (32%) repeated a grade: in most cases the first year of primary school (32%), followed by the first year of secondary school (11%). The first symptoms of ADHD reported were behavioral problems for 78% of the children, and attention deficit for 70% of them. In half of the participants, the symptoms were identified after the age of 4 (M = 4.45, SD = 2.25). They were noticed by someone who was not a family member in 72% of cases, who happened to be the teacher in more than half of the cases (57%). Interestingly, in more than two thirds of cases, the reporting party recommended referral to a psychiatrist in 22% of cases, a neurologist in 15% of cases, and to the family doctor in 7% of cases. In these two thirds of cases, half of the families made an appointment with a health care professional in the following months.
Analysis of Milestones in Care Pathways
At the first milestone, the person (mostly a relative) completing the questionnaire asked for an appointment with an HCP in 75% of the cases. More often (40% of cases), the HCP was a doctor (usually a child or adult psychiatrist), a paramedical professional (31% of cases), and less commonly a school employee (i.e., school doctor or school psychologist) in 16% of cases. Time to an appointment with a medical professional (i.e., neurologist, psychiatrist, and other categories) was usually longer than 1 month. For family doctors and psychomotor therapists, this interval was generally shorter than 1 month, and between 1 and 3 months for school doctors.
Overall, for half of the families, the first stage lasted more than 12 months (M = 16.02, SD = 18.98). The median age at diagnosis was 7.5 (M = 8.07, SD = 2.59). Half of the families went through at least three stages lasting 16.0 and 9.5 months for the first and fourth stages, respectively. However, 5% of the children had to see more than five HCPs. Table 1 shows that the duration of the stages decreased and that the rate of diagnosis increased from milestone to milestone, resulting in a twofold increase between the first and the fifth milestones (38%-77%). At the first milestone, ADHD diagnosis was rejected for 12% (i.e., false negative). Neurologists (78%) and psychiatrists (53%) evoked ADHD more frequently than any other medical specialist (20%). As seen in Figure 2, the time to diagnosis depended on the first health care professional met. It appeared to be the longest for psychomotor therapists and speech therapists.
Health Care Trajectories of Children With ADHD.
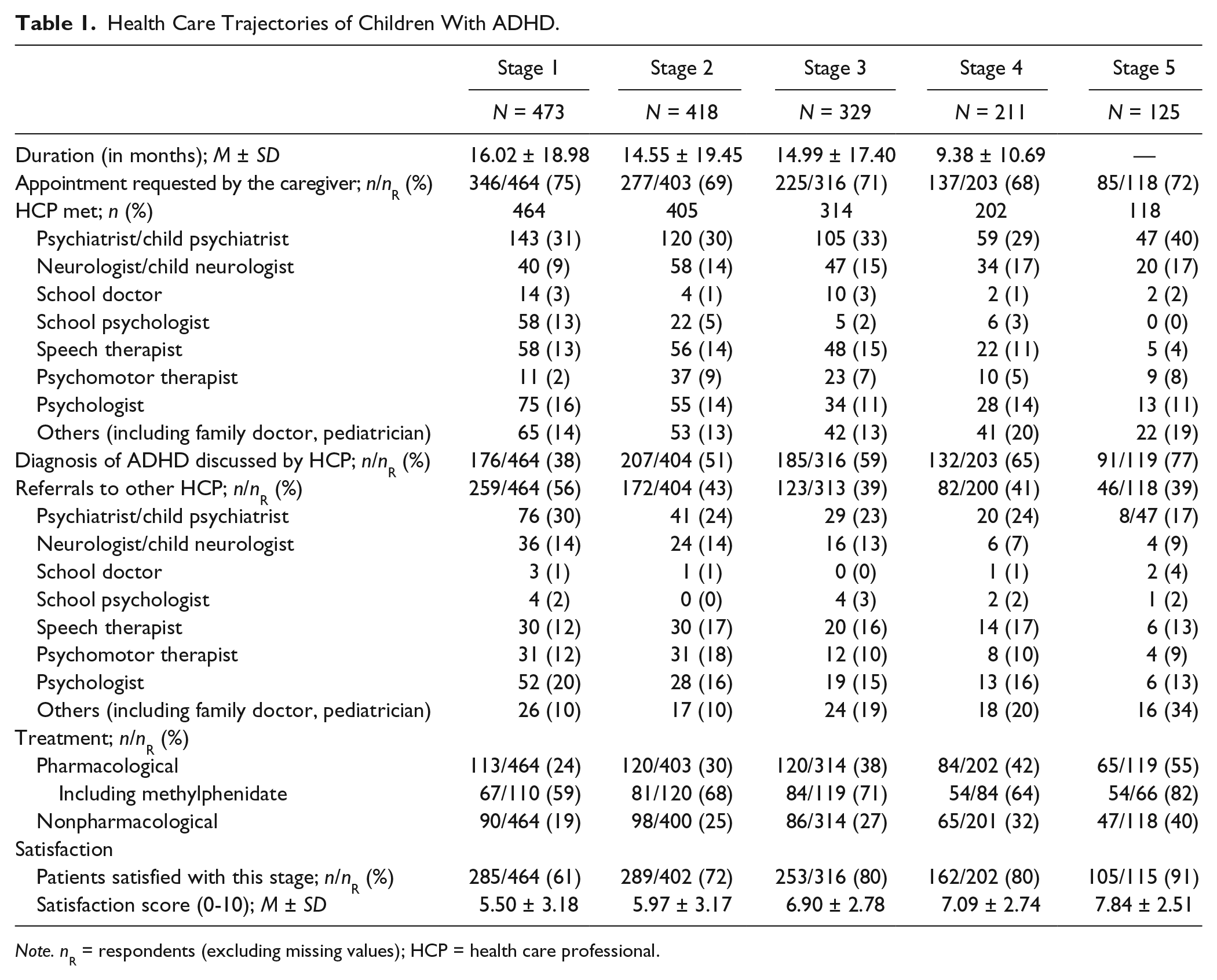
Note. nR = respondents (excluding missing values); HCP = health care professional.
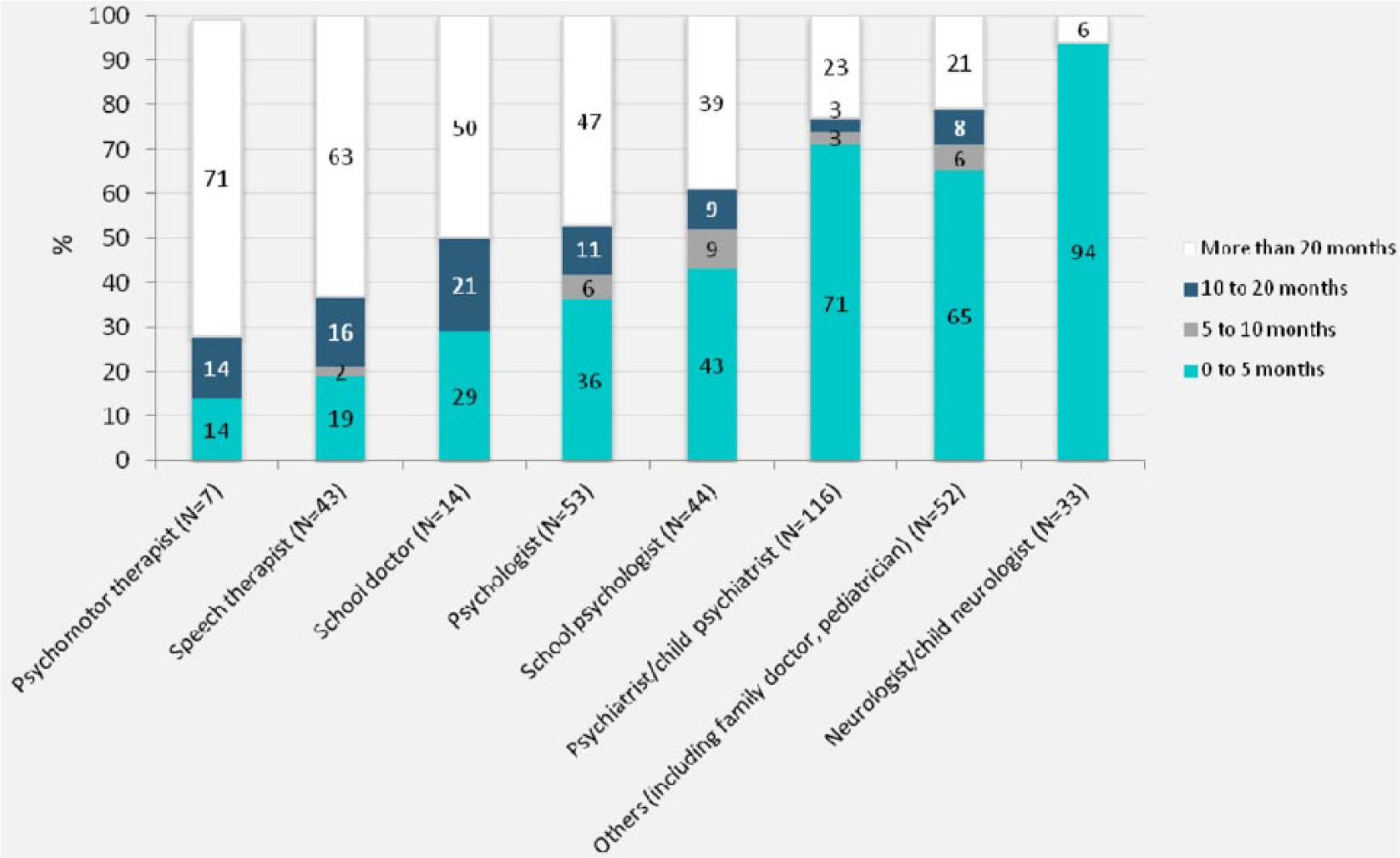
Time before ADHD diagnosis per category of first health care professional met.
The decision to see another HCP (and, therefore, initiate another stage) was generally taken by the family, regardless of the milestone (Table 1). However, referral to another HCP was often suggested by the previous HCP, although referral tended to decrease with the number of milestones. The chances of seeing a psychiatrist or a neurologist tended to increase with the number of milestones, whereas the chances of meeting other professionals (i.e., psychologist, speech therapist or psychomotor therapist) tended to remain fairly stable. School employees (i.e., school doctors and school psychologists) were less frequently contacted over time.
Table 2 shows that a wide variety of examinations were offered after ADHD diagnosis. After that, around 30% of the participants did not undergo any further tests, and less than half received a psychological assessment. A cardiologic examination was given in half of the cases (51%), and this appeared to be consistent with the rate of pharmacological treatment prescription in this sample. Educational adaptation was offered to nearly half of the participants (49%). Although a large majority of families had come into contact with multidisciplinary structures during their health care trajectory, only 24% of families received information about patient advocacy or support groups (e.g., TDAH-France [Trouble Déficit de l’Attention / Hyperactivité (ADHD)] or TDAH-PACA [Provence-Alpes-Côte d’Azur]).
Characteristics of Children With ADHD in the Two Groups Identified by Cluster Analysis.
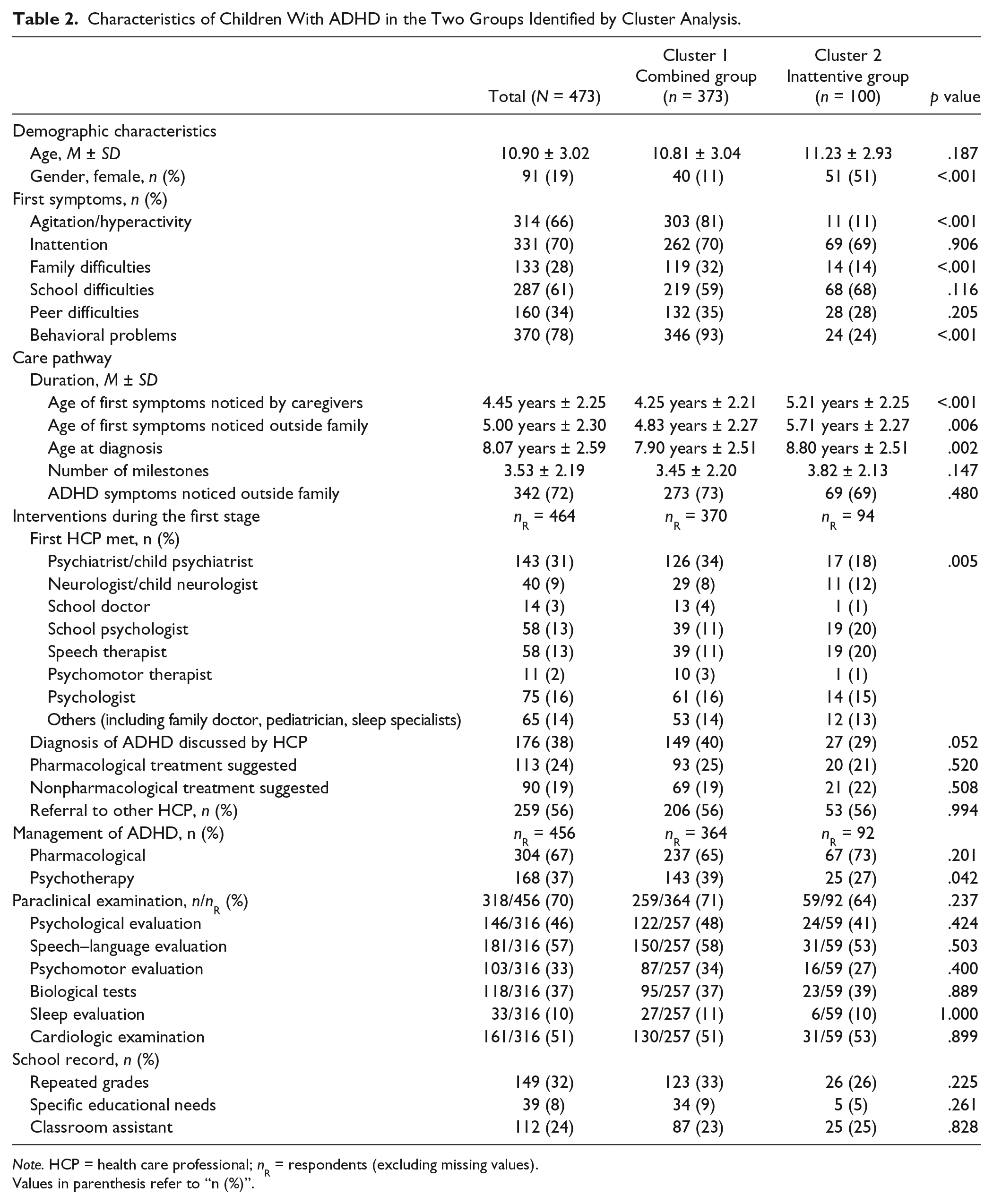
Note. HCP = health care professional; nR = respondents (excluding missing values).
Values in parenthesis refer to “n (%)”.
Treatments
Two thirds of children received pharmacological treatment (69%, n = 314/455) at the time of the study, 289 of whom described their treatment in detail. Methylphenidate (immediate- or extended-release) is the only drug with marketing authorization in France for ADHD. Not surprisingly, it is cited as monotherapy in 91% of the cases (n = 264/289). Other treatments prescribed included antipsychotics (3%, n = 8/289), melatonin (2%, n = 6/289), mood stabilizers (0.6%, n = 2/289), and antidepressants (0.3%, n = 1/289). These drugs have no marketing authorization in ADHD. Children also benefited from a wide variety of nonpharmacological treatments, including from the most to the least common: speech therapy, psychological therapy, psychomotor therapy, orthoptist therapy, occupational therapy, parent support group membership, family consultations and family therapy, and cognitive rehabilitation therapy. As seen in Table 1, nonpharmacological treatments were offered to a quarter of the sample (19%) at the first milestone. The proportion of children having received pharmacological treatment increased with the number of milestones, as did the rate of diagnosis.
Relationship Between Initial Onset of Symptoms and Health Care Trajectories
A cluster analysis on initial, suspected ADHD symptoms revealed four patient profiles. We combined Clusters 1 and 2 as they only differed on gender ratio, and Clusters 3 and 4 for the same reason. Therefore, we retained only two clusters that differed with respect to clinical picture before ADHD was ever suspected. Table 2 shows the frequency of each symptom for the two groups. Cluster 1 (n = 373, 89% boys) was named the “Combined” group as it included children with behavioral problems, agitation, and family problems. Cluster 2 (n = 100, 49% boys) was named the “Inattentive” group as it included children with less pronounced agitation and hyperactivity symptoms. School and peer relation difficulties as well as the repeat grade rates did not differ between the two groups. The first symptoms were noticed 1 year earlier in the Combined group than in the Inattentive group, a difference that persisted throughout the care pathway.
Figure 3 shows that, at the first milestone, patients in the Inattentive group were referred at an equal rate to a school psychologist (20%), a speech therapist (20%), or a psychiatrist (18%) suggesting a kind of indeterminacy with regard to the suspected underlying cause of the symptoms. However, patients in the Combined group were twice as likely to be referred to a psychiatrist as to a psychologist (34% and 18%, respectively) at the first milestone.
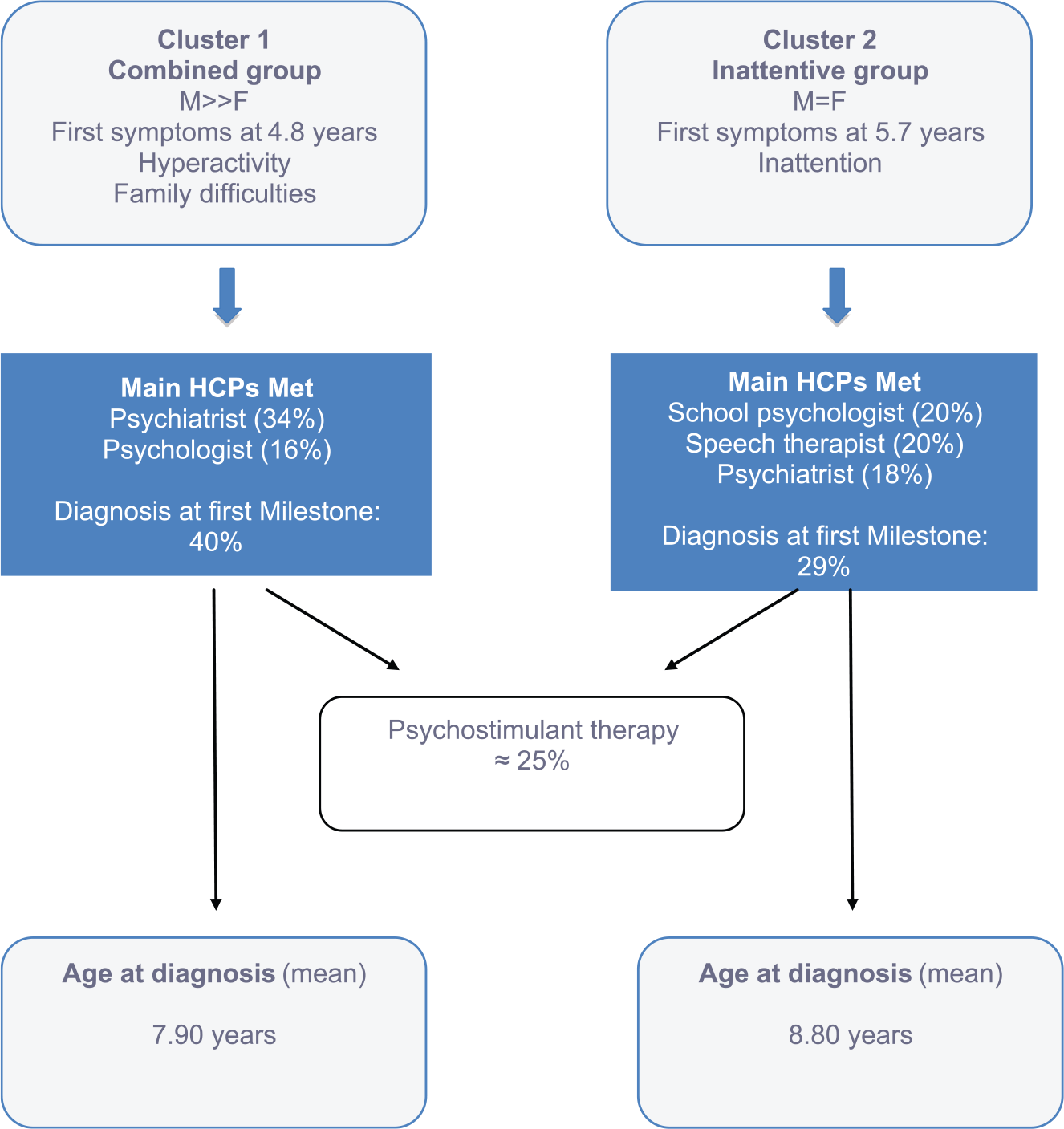
Care pathways of children and adolescents with ADHD in the two clusters (see details in Table 2).
Family Satisfaction Results
Only 61% of the families were satisfied after the first referral (Table 1). This rate increased gradually throughout the care pathway, reaching a 91% satisfaction rate after the fifth milestone. Figure 4 shows the main reasons given by families for their low level of satisfaction. A too large time span between diagnosis and treatment was by far the most common reason given for dissatisfaction. The next two reasons were the lack of early identification of the disorder; that is, “difficulties accessing specialist care” added to “no early identification of symptoms by school professional.” The next two reasons were lack of coordinated care pathway and the social impairment resulting from ADHD symptoms and were identified as a source of concern for families, that is, “loss of chance for the child” added to “lack of specific educational adaptation by the school.” The cost of investigations and treatment was less frequently mentioned as a source of concern.
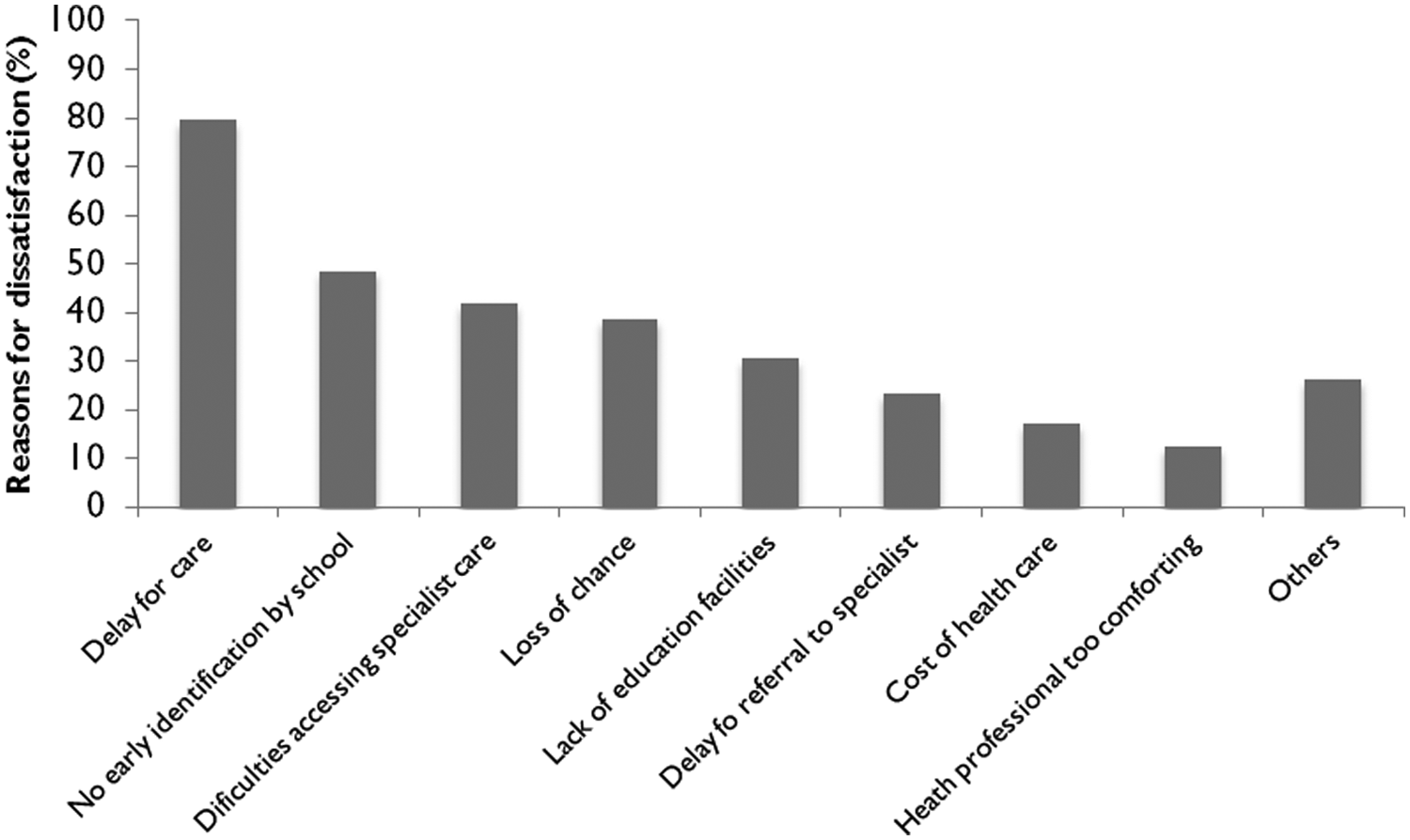
Reasons for dissatisfaction during health care trajectories cited by family with an ADHD child.
Table 3 compares the satisfied and dissatisfied families. In the group of dissatisfied families, mothers were more likely to have a higher level of qualification, and home-referral center distance was further. Few significant differences were found with regard to the clinical picture, except for more oppositional behavior and more refusals to comply with adults’ rules in children from dissatisfied families. No significant difference was found in the severity of the disorder reflected by difficult school, familial and peer relationships, or in the academic consequences of the disorder. Major differences were found between the two groups in the diagnosis and treatment received by children with ADHD. Initial ADHD symptoms were noticed earlier by a nonfamily member or by a caregiver in dissatisfied families compared with satisfied families. The diagnosis came about 1.3 milestones later, which is about 14 months later. Compared with satisfied families, dissatisfied families were less likely to be referred to a psychiatrist or a neurologist (28% vs. 49%, respectively), to be diagnosed at the first milestone (24% vs. 52%, respectively), to receive pharmacological treatment (15% vs. 33%, respectively), to undergo paraclinical investigations (63% vs. 77%, respectively), and to be referred to another HCP (46% vs. 65%, respectively). Finally, no significant differences were seen in the recognition of disabled status, specific educational adaptation, referral to family support organizations, or contact with multidisciplinary structures during the pathway.
Characteristics of Children With ADHD Amongst Satisfied/Dissatisfied Families.
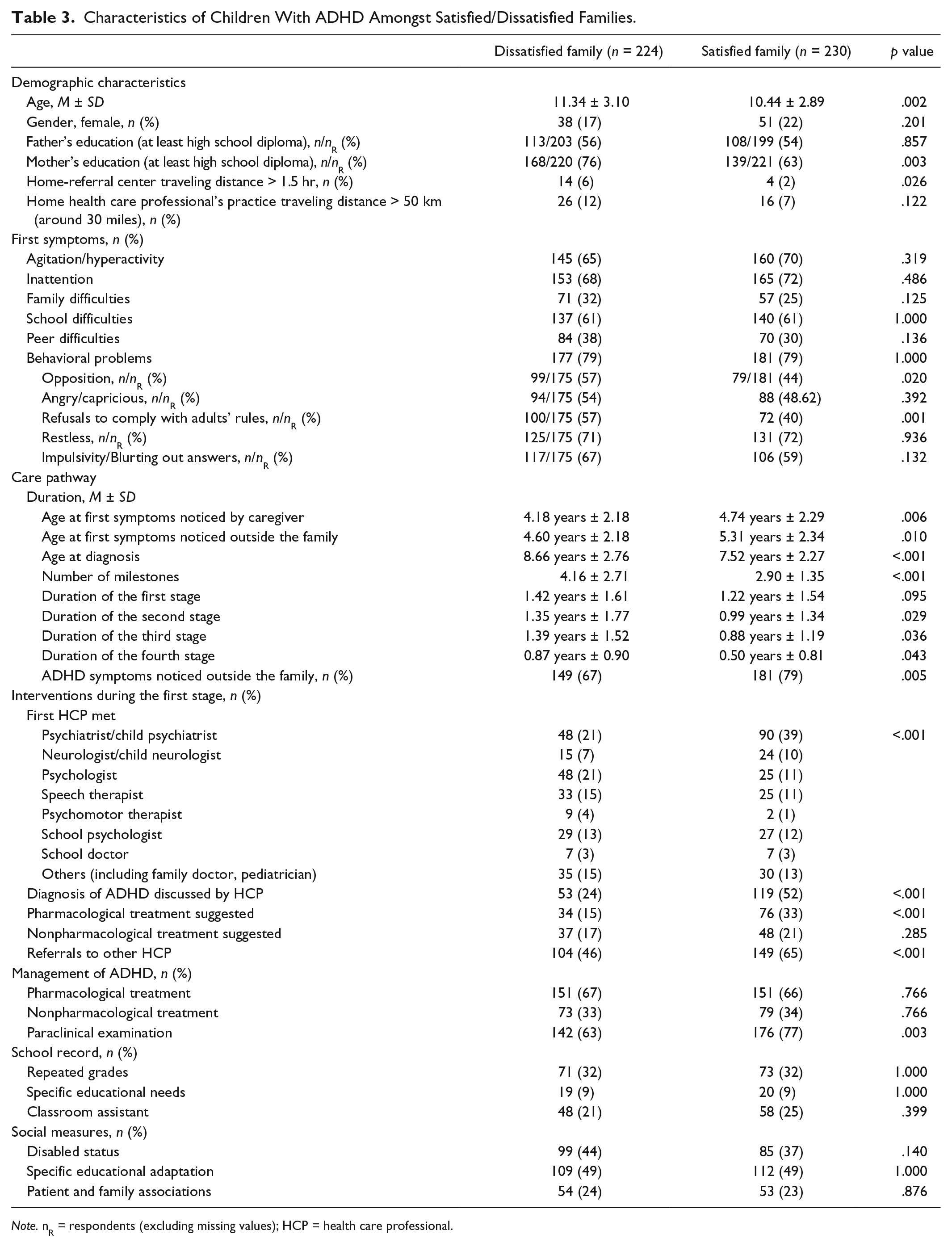
Note. nR = respondents (excluding missing values); HCP = health care professional.
Discussion
Here, we present results from the QUEST survey, the first national (retrospective, multicenter, and naturalistic) survey conducted in children and adolescents treated for ADHD in France.
A Proper Definition for the Time to Diagnosis
These results should be compared closely with those reported in previous studies, given the different outcomes used to determine the time to diagnosis and to define it. We could imagine separating the three successive periods of time. First, the time between observation of the “first” symptoms of the disorder to the first consultation with a health care professional. The length of this period of time is likely to reflect the family’s tolerance to the child’s symptoms. Second, the time between the first consultation with a health care professional to definite diagnosis of ADHD, which is likely to reflect the level of knowledge of the health care professionals or, as noted earlier, the possible existence of a comorbid disorder that was initially suspected, whether rightly or wrongly. Third, more specific to the pharmacological treatment of ADHD, is the time between the definite diagnosis and the prescription of specific psychostimulants or nonpsychostimulants. This last period of time is likely to reflect the availability of the drugs and their image with most HCPs (Quiviger & Caci, 2014). Two studies focused specifically on the second timeline (Purper-Ouakil et al., 2007; WFMH, 2004). The “Without Boundaries” survey reported that the average length of time from the first visit to a physician to diagnosis by a specialist was just under 24 months (WFMH, 2004). This duration differed between countries and ranged from less than 1 year in the United States, to more than 3 years in Italy. A study conducted in a French clinical sample found a 33-month interval between the first consultation with an HCP and diagnosis of ADHD (Purper-Ouakil et al., 2007). In our study, we preferred a broader definition of delay to diagnosis by focusing on the first two types, that is, from observation of the first symptoms to definite diagnosis of ADHD. By doing so, we aimed to examine the effect of clinical and family variables more specifically on the early stages of the care trajectories, namely, prior to consultation with the first HCP. Further research is required to investigate the validity of these three timelines and the main determinants of each.
Sample Characteristics
In this study, ADHD diagnosis had to be formally established by a qualified professional. We did not fully describe the pattern of comorbidities in each case. Side effects of methylphenidate may be inferred from melatonin prescription (i.e., delayed sleep onset), and comorbid conditions may be inferred from concomitant prescriptions or inadequate prescription (e.g., risperidone for conduct disorder as HCP focus on this diagnosis and not on ADHD). Overall, this suggests that the level of comorbidity might be quite low in our sample. Furthermore, in our country, child psychiatrists treat ADHD rather than private practice pediatricians, as it is the case in the United States, for example. Therefore, being treated by a child psychiatrist does not say so much about case seriousness. The 2011 National Survey of Children’s Health (NSCH) reported that the median age of ADHD diagnosis decreased in line with severity: 7.0, 6.1, and 4.4 years, respectively, for “mild,” “moderate,” and “severe” forms as reported by parents (Visser et al., 2014). The median age at diagnosis was 7.5 years in our sample, either suggesting that the patients generally presented with the “mild” form or that the time to diagnosis was longer than that in the United States.
Thirty-two percent of children in our sample had repeated a grade at least once, one third of which repeated the first year of primary school. Children with ADHD were 3 times more likely to repeat a grade than the gender- and age-matched controls in an American birth cohort study (Barbaresi, Katusic, Colligan, Weaver, & Jacobsen, 2007). There is strong cross-national variation with regard to grade repetition associated with contrasting systems of schooling (Pastor & Reuben, 2008). In 2009 in France, 36.5% of 15-year-old pupils had repeated a grade at least once in primary and/or lower secondary school (Education, Audiovisual and Culture Executive Agency [EACEA], 2011).
There is also strong cross-national variation with regard to the proportion of children with special needs, mainly because definitions vary between countries. In 2010 in France, 2.8% of the pupils in compulsory education were identified as having special education needs (http://www.nesse.fr/nesse/activities/reports/activities/reports/disability-special-needs-1), a value that should be compared with the proportion of 8% found in our sample. Furthermore, there are almost 10.2 million children between birth and 17 years with special education needs in the United States (about 13% of the population in this age range), 40% of which are diagnosed with ADHD (Lollar, Hartzell, & Evans, 2012).
Trajectory Depends on Health Care Professionals
Caregivers noticed the first symptoms of ADHD at a mean age of 4.45 years, the diagnosis being made formally approximately 4 years later. Patterns of comorbidities may have had an impact on delay to diagnosis because children might have been treated for another disorder before ADHD was even considered. When the health condition is not known, functional difficulties only are noticed (e.g., learning, paying attention, fidgeting, fighting, and arguing; Lollar et al., 2012). Teachers may believe the child’s behavior to be caused by despondency or boredom, and may mistake certain ADHD symptoms for intellectual giftedness. We believe that the reason behind this is rather lack of awareness of ADHD, because the study shows that the most frequently reported difficulties are behavioral problems and attention deficit.
Impact of School and the Mental Health Care System
The French mental health care system comprises a wide variety of caregivers in the mental health field, including public community care centers (centres médico-psychologiques) across the country, and private general practitioners, pediatricians, psychiatrists, and psychologists. The free access to public health care and the lack of gate control in seeing a mental health specialist may encourage multiple referrals. The lack of guidelines that clearly distinguish the roles of HCPs and a gold standard evaluation for children with ADHD may further contribute to the complexity of care pathways in the French system (AAP, 2000; Graham et al., 2011).
The first consultation with a health care professional is an essential milestone in the health care pathway for children with ADHD (Bussing, Zima, & Gary, 2003). Here, diagnosis was discussed in only 38% of children at the first stage, which lasted roughly 1 year, and treatment differed depending on the specialist consulted (Figure 2). This raises concerns about the general level of knowledge on ADHD among HCPs.
Feedback from school represents an important part of the process for evaluating a child’s difficulties (Caci, Morin, & Tran, 2013; Efstratopoulou, Simons, & Janssen, 2013). Whether schools can make early referral for children with behavioral problems easier remains controversial (Bussing, 2010; Evans, Langberg, Egan, & Molitor, 2014; Foy & Earls, 2005). A recent study highlighted the positive impact of providing information and a consensus protocol to school professionals, to help orientate children requiring assessment (Foy & Earls, 2005). In our study, teachers were mainly the first nonfamily members to notice symptoms and to suggest referrals. However, initial referral to a school doctor or school psychologist, reported in 15% of children, was associated with a longer delay to diagnosis and treatment. Reasons are likely to be diverse but, again, the lack of knowledge on ADHD among these HCPs cannot be ruled out.
Impact of Clinical Picture
Despite a comparable level of difficulties at school, it took a further year for the Inattentive group to receive a diagnosis and treatment. Our study was not designed to investigate the reasons for this. However, clinicians may have been misled by gender bias (Nussbaum, 2012) as ADHD in girls is more frequently associated with emotional dysregulation symptoms (Robison et al., 2008) and a higher rate of comorbidity with internalized disorders (Koyuncu et al., 2014). Despite a similar level of functional impairment, girls are less likely to receive treatment than boys (Nussbaum, 2012; Zarin, Suarez, Pincus, Kupersanin, & Zito, 1998). In an attempt to describe the help-seeking behavior of families with ADHD, Bussing et al. (2003) showed that girls and boys did not differ in terms of recognition of a problem and help seeking. However, girls were less likely to obtain a diagnosis and treatment. Our study suggests that young people in the Inattentive group experienced more difficulties in both access to care (e.g., lower rate of recognition by the family or other adults) and management of the disorder (e.g., the diagnosis was less likely to be made by HCPs). Children in the Combined group were more frequently referred to a psychiatrist or a child psychiatrist after initial referral, whereas young people in the Inattentive group were the subject of varied referrals. This shows that children presenting with mainly inattentive symptoms experience more difficulties getting referred properly after a first consultation with an HCP.
Family Satisfaction With Their Child’s Care Pathway
Families in six European countries reported that the long delay to diagnosis of ADHD was among the most frequent causes of frustration (Caci et al., 2014). This is consistent with family interviews (Dennis et al., 2008; Dosreis et al., 2003; Johnson & Marsh, 2001; Leslie et al., 2007). Families in our study report the same frustration as being the reason for their dissatisfaction, with a mean of one additional milestone and 14-month delay compared with children from satisfied families. This could be partly explained by the difficulties experienced by HCPs in diagnosing ADHD (Quiviger & Caci, 2014). Children from dissatisfied families not only had their symptoms identified later by the main caregiver and by an adult nonfamily member but also health care professionals diagnosed ADHD less frequently and took more time to recommend specific treatment. More information about differential diagnoses and comorbidities would have been valuable in exploring the characteristics of these children further. In addition, the results support evidence that inadequate access to information, especially in terms of coordination of care and educational adaptation, is a major concern for families. Once again, parents’ lack of concern regarding the costs of health care has to be interpreted in the context of the French health care system, where most of the medications are fully reimbursed. It should also be stated that, in France, it is a legal requirement for schools to be specially adapted for disabled children (Loi pour l’égalité des droits et des chances, French equal rights law, 2005).
Limitations
Several limitations in this study need to be addressed. First, not all views may be represented as participation in the sample was voluntary. Awareness of ADHD and its symptoms may be heightened in this group of respondents compared with in the general population. Moreover, parents retrospectively reported clinical histories in the large majority of cases, which entails a certain level of reporting bias. In an attempt to control this bias, we compared subjective measures of quality of care with objective information (e.g., repeating a grade or the need for special education). Second, because cross-sectional data were used, the time between the milestones should be considered as a rough approximation of the exact duration. Reports of services cited by parents were not confirmed by the provider or administrative records; however, good correlation between parent reports and outpatient department records has been reported in other studies (Ascher, Farmer, Burns, & Angold, 1996; Bussing et al., 2003). Third, the lack of standardized diagnostic procedures could have affected the quality of the results. The questionnaire used to report symptoms and functional impairment in children with ADHD was developed by a group of experts in child psychiatry and by child neurologists. The content was considered to be acceptable by the group of experts; other acceptance criteria were not available. However, all participants were patients of ADHD specialists having made the diagnosis. The lack of data concerning differential diagnoses and psychiatric comorbidities (e.g., learning disorders) is regrettable and may have slightly affected the overall results. Finally, the small sample size may limit generalization of the results.
Clinical and Theoretical Implications
Recently, the French national authority for health (Haute Autorité de Santé [HAS]) published best practice recommendations for practitioners directly concerned (http://www.has-sante.fr/portail/jcms/c_2012647/fr/trouble-deficit-de-l-attention-avec-ou-sans-hyperactivite-tdah-repere-la-souffrance-accompagner-l-enfant-et-la-famille). Unfortunately, this document fell short of national evidence-based guidelines, which clarify the roles of HCPs treating children and adolescents with ADHD. More efficient referral of young people with academic or behavioral problems is clearly needed, especially during the kindergarten and elementary school years. Basic reading, writing skills, and peer-relationship skills that develop concurrently require concentration and a low level of excitability. HCPs should be educated to recognize the main symptoms of ADHD, as well as more atypical forms, in particular the inattentive form. Information about the etiology of the disorder may be also important, as beliefs as to the assumed causes of the disorder affect ADHD management (Quiviger & Caci, 2014). As the family is regarded as a driving force in the mental health care process (Dennis et al., 2008; Dosreis et al., 2003; Johnson & Marsh, 2001; Leslie et al., 2007), more detailed information for parents about the different services and how they relate to one another could improve the chances of young people receiving early treatment.
Conclusion
In this study, the time between observation of the first symptoms and ADHD diagnosis was longer than 4 years. This may result in a loss of opportunities for these patients. We observed various trajectories in terms of duration and type among young people and their families. In particular, the time to diagnosis and treatment was longer in the group containing a higher number of girls and with predominantly inattentive symptoms. Further research is needed to assess our model of the predictors underlying the delay in ADHD diagnosis, and to evaluate the benefit of training HCPs who are not experts in ADHD (e.g., school and family doctors) in the core symptoms of ADHD and less typical forms, in view of reducing the time to diagnosis. In line with this, a consensus protocol on optimal referral for children with ADHD may help reduce the disparities observed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.C. received payment for consultancy activities and/or meetings on behalf of Schering-Plough, Bristol-Myers Squibb, Pfizer, Otsuka, Janssen, Lundbeck, Shire, and Sanofi-Aventis. In addition, over the past 2 years, he received payment for consultancy work, specific assignments, and/or conference participation on behalf of Otsuka, Lundbeck, Shire, and IntegraGe. Over the 5 last years, O.B. received payment for consultancy activities, lectures, and advisory board membership on behalf of Actelion, Orphan Europe, Shire, Otsuka, and Bristol-Myers Squibb. H.C. was a consultant for Shire and principal investigator in several Phase 3 studies in ADHD sponsored by Shire, Lilly, and Boiron. B.K. received payment for interventions on behalf of Shire and Otsuka. J.-P.R was invited by Shire France to the American Academy of Child and Adolescent Psychiatry Congress in 2011 and 2012. He has no other conflicts of interest. S.P. is an employee of Shire. L.V. received payment for consultancy activities, advisory board membership, and conference participation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The survey was supported by Shire France AG. Xavier Benarous, MSc, MD, resident in psychiatry Hopîtal Pitié-Salpêtrière, provided editorial assistance for this publication under the direction of the authors. Editorial assistance in formatting, proofreading, copy editing, and fact checking was provided by Raison De Santé funded by Shire France AG. Statistical analysis was provided by Methodomics.
Supplemental Material
Additional data can be found online only (questionnaire). To view these files, please visit the online journal (http://jad.sagepub.com/; ![]() ).
).