
Abstract
This article investigates business models innovation for delivering health care at the base of the pyramid (BoP). The examination of six health care organizational cases suggests that co-creation of patient needs, community engagement, continuous involvement of customers, innovative medical technology, focus on human resources for health, strategic partnerships, economies of scale, and cross-subsidization are business model innovation strategies that enable inclusive health care delivery. Based on these findings, we propose a four-dimensional framework. A process of value discovery, leading BoP patients and communities to recognize a health need and seek for an acceptable treatment, precedes the identification of a successful value proposition. Value creation and value appropriation then follow to warrant patient affordability and organizational sustainability. A “business model mechanism” for BoP health care hence emerges, where interdependencies among these dimensions are highlighted. This article sheds new light on how market-based approaches can improve equitable health care access and hence contribute to poverty alleviation.
Introduction
Under-optimal access to health care is a widespread phenomenon among disenfranchised individuals in economic resource-poor areas of the worlds, also known as base-of-the-pyramid (BoP) settings (George, Rao-Nicholson, Corbishley, & Bansal, 2015; Kim, Farmer, & Porter, 2013). Limited health care access, in tandem with poor living conditions, enhanced exposure to disease-prone environments and unhealthy dietary habits, contributes to reduced life expectancy, poverty, and depleted quality of life for BoP communities (Marmot, Friel, Bell, Houweling, & Taylor, 2008). One root cause undermining timely and effective health care access is the cost of medical treatments and the risk of catastrophic health care expenditures, which may cause sudden impoverishment of the low income households and push them further below the poverty line (Balarajan, Selvaraj, & Subramanian, 2011).
In order to increase access to health care at the BoP, and hence to ensure a healthier as well as wealthier population, new business models of health care delivery are necessary (Bhattacharyya et al., 2010; George et al., 2015; Kim et al., 2013; Simanis, Hart, & Duke, 2008). Extant literature defines a business model as “a structural template describing how a focal firm transacts with customers, partners, and suppliers, that is how it chooses to connect with the factor and product markets” (Zott & Amit, 2008, p. 3), which ultimately portrays “how an organization creates, delivers and captures value” (Osterwalder & Pigneur, 2010). Innovative business models have been described across a variety of industries, from the new business creation facilitated by the world wide web (Amit & Zott, 2001), to new approaches to urban mobility (Cohen & Kietzmann, 2014), to microcredit (Yunus, Moingeon, & Lehmann-Ortega, 2010). With reference to the latter, social business models, in particular, are conceptualized to include in the profit equation not only financial returns but also welfare-enhancing outcomes (Haigh & Hoffman, 2014; Prahalad & Hart, 2002; Yunus et al., 2010).
Despite its relevance, studies addressing business model innovation for ensuring more effective and efficient health care delivery at the BoP are rare. The few exceptions focus on single case study design (e.g., George et al., 2015) or lack a business focus (Bhattacharyya et al., 2010) and, while providing rich, in-depth insights, still fall short in offering a broader systematization of how to develop business models innovation strategies for delivering health care in these settings. Also, the existing conceptualizations of business models do not adequately guide in designing business models specific to health care and BoP markets. The fundamental human right to have access to basic health care for hundreds of millions of poor provides an unmatched motivation for economic actors to conceive, design, implement, and support innovative health care solutions.
In this study, we particularly examine how business model innovations can enable the delivery of inclusive health care. To define inclusive health care we draw on the concept of “inclusiveness”, which points to “the development and implementation of new ideas which aspire to create opportunities that enhance social and economic wellbeing for disenfranchised members of society” (George, McGahan, & Prabhu, 2012). Business models adopting market-based approach—as opposed to corporate social responsibility strategies (Montiel & Delgado-Ceballos, 2014)—are crucial to ensure viability, scaling up, and hence, continuity of the supply of the welfare-enhancing product and service. Inclusive health care—rather than only affordable—promotes health service delivery that is not only financially but also socially and culturally acceptable to BoP patients. With the help of six case studies from India, we identify innovation strategies enabling successful and sustainable business models for health care delivery to low-income patients. The research question underpinning this study is, therefore: Which business model innovation strategies allow for the delivery of inclusive health care at the BoP?
BoP Health Care Markets
Health care delivery at the BoP provides a novel standpoint for observing how specific business models can be tailored to the need of low-income markets. BoP markets inherently differ from higher tier markets, as an institutional theory lens reveals (Angeli & Jaiswal, 2015; Rivera-Santos, Rufín, & Kolk, 2012). It is well known that economic resource-poor communities are characterized by institutional isolation and by an idiosyncratic structure of beliefs, sociocultural traditions, values, and norms (Angeli & Jaiswal, 2015; De Soto, 2000; London, 2009; Rivera-Santos et al., 2012) and that informal institutions, rather than formal ones, have a prominent role in governing social life in these contexts (Rivera-Santos & Rufín, 2010). An institutional divide exists between BoP and developed markets—which manifests into different meanings and values attached to products and services (Angeli & Jaiswal, 2015; Rivera-Santos et al., 2012).
Challenges to delivering products and services at the BoP become magnified in the case of health care delivery. Health care services are characterized by high information asymmetry between patients and physicians (Lako & Rosenau, 2009). This information asymmetry is even higher in the BoP settings owing to the low degree of education and health literacy of the population. The customer need itself often goes unrecognized, and idiosyncratic beliefs, traditions, norms, and institutional isolation may hamper the very process of health need recognition (Marmot et al., 2008). BoP patients are often not able to identify their ailments (Bhattacharyya et al., 2010) and they rely on local communities and social networks to determine and deal with their health conditions and to take decisions in relation to when and which type of health care services to seek. A number of social and cultural factors intervene in health-related behavior patterns, such as gender, family constraints, mistrust toward modern medicine infrastructure, potential stigma (Bagley, Angel, Dilworth-Anderson, Liu, & Schinke, 1995; Kumar, Goel, Kalia, Swami, & Singh, 2008). The strong influence of sociocultural beliefs, values, and traditions often undermine health-seeking behavior and adherence to treatments, particularly for women (Bhanderi & Kannan, 2010). Even when seeking treatment, unqualified traditional healers or chemists’ shops constitute the first consultation point, rather than regular physicians (Sudhinaraset, Ingram, Lofthouse, & Montagu, 2013). Allopathic health care services are considered only when the ailment has become very serious, and when the costs of the necessary treatment might be prohibitive. Individual and social barriers, even when facilities are present and could be utilized, undermine the health status of BoP communities, directly contributing to a spiral of poverty increase.
On the provider side, delivering health care in low-income setting is complicated by the extreme affordability requirements, the infrastructural voids such as poor availability of electricity and transportation, lack of government support (Khanna & Palepu, 1999), shortage of trained resources (Rao, Rao, Kumar, Chatterjee, & Sundararaman, 2011), and the lack of formal market institutions.
The heavy sociocultural connotation of health and health-seeking behavior makes the health market at the BoP markedly different from BoP markets for other products and services such as consumer goods where needs are fairly straightforward and more easily detectable (Angeli & Jaiswal, 2015). Affordability for BoP consumers is of extreme importance, however particularly difficult to achieve in health care delivery, where the quality of treatment cannot be compromised. To add complexity, affordability and availability alone seem to be insufficient to ensure success to low-cost models. New business models designed for BoP consumers need to achieve awareness and acceptability in the target market, which may display highly complex and idiosyncratic characteristics and be reluctant to access products or services even when infrastructures are available (Anderson & Markides, 2007; Angeli & Jaiswal, 2015). And in fact, awareness and acceptability of health treatments at the BoP are particularly critical, because of the challenges posed by patients’ limited health literacy and exposure to traditional dissemination channels devoted to publicize socioculturally acceptable solutions.
The theory of disruptive innovation portrays how low-cost, simpler, and more functional products or services emerge, in response to the needs of more resource-constrained customers (Hwang & Christensen, 2008). Low-income health care markets pose peculiar challenges to business model innovation, and as such constitute fertile settings where business model disruption can occur (Christensen, Bohmer, & Kenagy, 2000).
Conceptualizing Inclusive Business Models for Health Care
In the extant literature, the definition of a business model and its dimensionality vary significantly. Zott and Amit (2008) emphasize the way through which the focal firm handles its relationships with suppliers, customers, and partners within its value network as a salient aspect of a business model. Johnson, Christensen, and Kagermann (2008) elaborate and conceptualize a business model into four main elements: the customer value proposition, the primary resources, the main processes, and the profit equation. Yunus et al. (2010) suggested a four-dimensional conceptualization of business model. They argue that business model presents a consistent and integrated view of how an organization generates revenues and profits, through a specific combination of value proposition and value constellation (Yunus et al., 2010). The third dimension is the economic profit equation, which financially translates the value proposition and value constellation to ensure that revenues outweigh costs and hence that the enterprise is sustainable. The fourth dimension is the social profit equation, which is exclusive to and an important cornerstone for organizations that are born with an important socially oriented mandate while aiming at being financially self-sustainable. The so-called “social businesses” are particularly close to what modern health care organizations strive for—an often difficult—balance between social and financial outcomes.
Drawing on previous literature, a generic conceptualization of a business model can be presented, that hinges on three dimensions of value: value proposition, value creation, and value appropriation. Value proposition points to the solution offered to a particular problem or customer need (Yunus et al., 2010; Zott & Amit, 2008) or “a job to be done” (Johnson et al., 2008); value creation, which considers the internal and external value chain resources, processes, and actors that create and deliver the value in the form of offered products and services, in line with the concept of value constellation (Yunus et al., 2010), value network (Zott & Amit, 2008), and use of resources and processes (Johnson et al., 2008); value appropriation, which highlights the ways through which part of the value created flows back to the organization and how it is shared with other stakeholders. The last dimension considers not only the profit equation (Johnson et al., 2008; Yunus et al., 2010) but also social outcomes (Yunus et al., 2010).
Method
Our research focuses on business models for inclusive health care in the BoP population, a field characterized by the paucity of scholarly research. Owing to the lack of adequate theoretical basis and emerging nature of the field, we opted for an exploratory and inductive research approach (Eisenhardt, 1989; Eisenhardt & Graebner, 2007). Qualitative rather than quantitative research is often recommended in the early stage of theory development in a given field of inquiry. Similar research approach has been used in the extant literature to study the strategies for low-income markets in developing countries (London & Hart, 2004), innovation (Galunic & Eisenhardt, 2001), health care in developing contexts (Bhattacharyya et al., 2010; George et al., 2015), and linkages between proactive environmental strategy and organization capability development (Sharma & Vredenburg, 1998).
We selected a multiple case study methodology (Eisenhardt, 1989) as part of which we carried out an in-depth investigation of selected cases of inclusive health care initiatives. This method allowed us to conduct a systematic analysis of the selected cases in order to develop theory on how organizations undertake business model innovation for inclusive health care. Qualitative research also enabled us to identify possible constructs and explore the relationships among them. This in turn would help in the formulation and empirical examination of hypotheses in future studies. Comparison of multiple cases also allows examination of “What” and “How” questions relevant to our research objectives (Yin, 1989) such as what are the different business model innovation strategies that health care organization adopt for delivering inclusive health care and how exactly they reduce the health care costs.
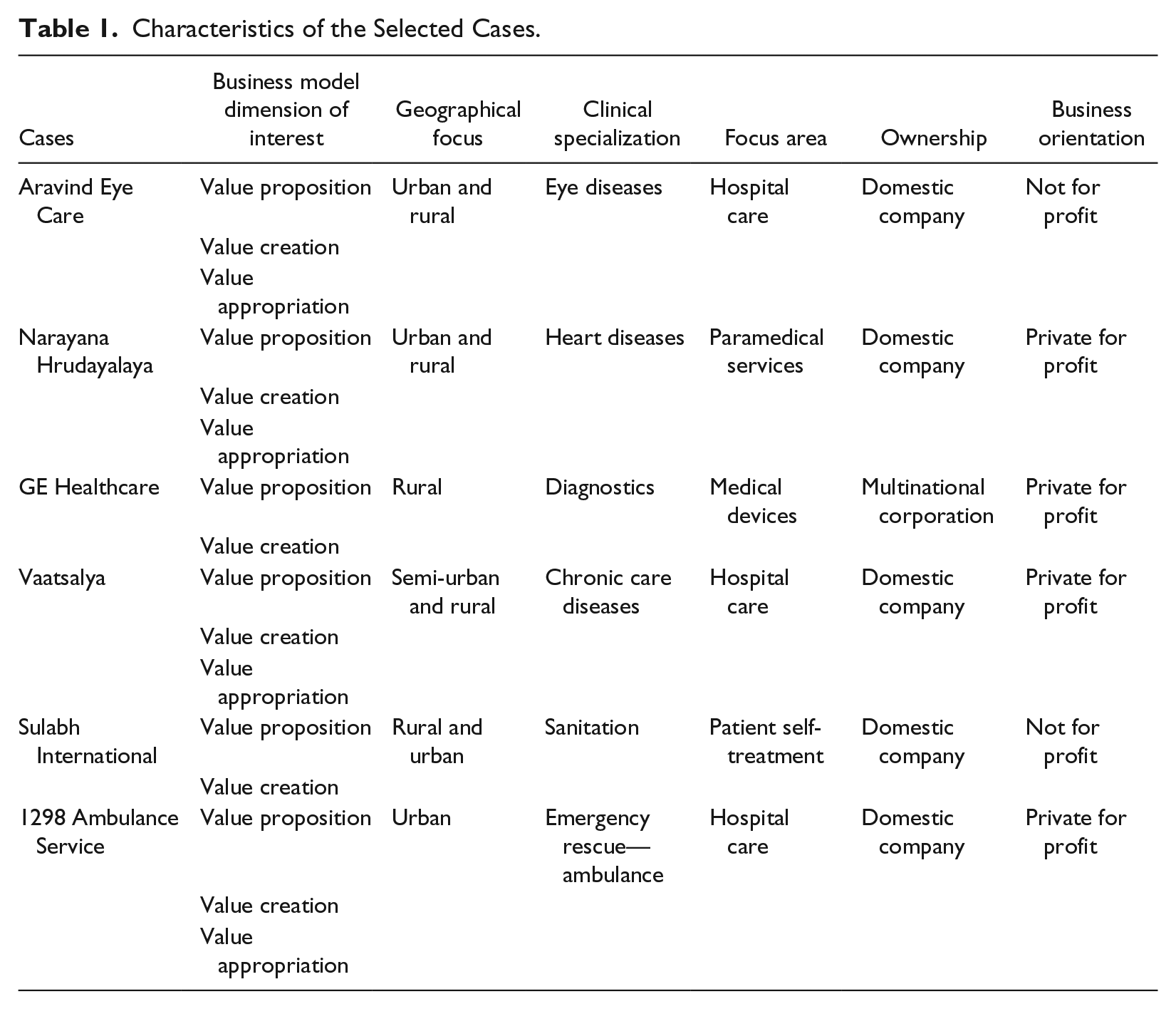
We followed three steps as part of our research methodology. In the first stage, we selected health care ventures to be examined in our research. The cases exemplify different kind of approaches toward innovation across the three different dimensions of business model—value proposition, value creation, value appropriation. The selected cases involved major innovations on at least one value dimension of the business model. The cases cover all the key constituents in the health care delivery value chain, such as hospital care, medical devices, and medical support services. The selected organizations vary in terms of clinical specialization, ranging from heart diseases, to ophthalmology, to chronic conditions. Differences in terms of geographical focus are also taken into account, as the selected cases operate in urban, semiurban, and rural areas, both exclusively or in combination. These cases also pertain to spearheading major improvements in behavioral practices that have a direct and immediate impact on health care such as those related to drinking water and sanitation. The selected cases involved ventures of domestic companies as well as local arms of multinational corporations. The cases of both for-profit and not-for-profit organizations were considered as the latter played a significant role in the delivery of inclusive health care in India. We initially selected seven cases; however, as one of these ventures closed down during the data collection, we decided to exclude it from the study. Table 1 summarizes the characteristics of the selected cases in relation to the selection criteria as well as their business model dimension of relevance.
Characteristics of the Selected Cases.
All the selected health care initiatives were from India. There were many reasons for focusing on health care organizations from India and selecting the country as our data collection site. First, out of the total worldwide BoP population of 4 billion, measured as people earning less than US$3,000 annually in local purchasing power, almost one-fourth (925 million) live in India making it a country with largest BoP population (Hammond, Kramer, Katz, Tran, & Walker, 2007). Furthermore, BoP spending on health in India is $35 billion, making it an important constituent of worldwide BoP health care market that is estimated to be of $158.4 billion (Hammond et al., 2007). Second, in general, the existing BoP literature has a key focus on India and is interspersed with Indian success stories and examples (Kolk, Rivera-Santos, & Rufín, 2014). Third, one of the authors resides in India, which offered certain added advantages in field work and data collection.
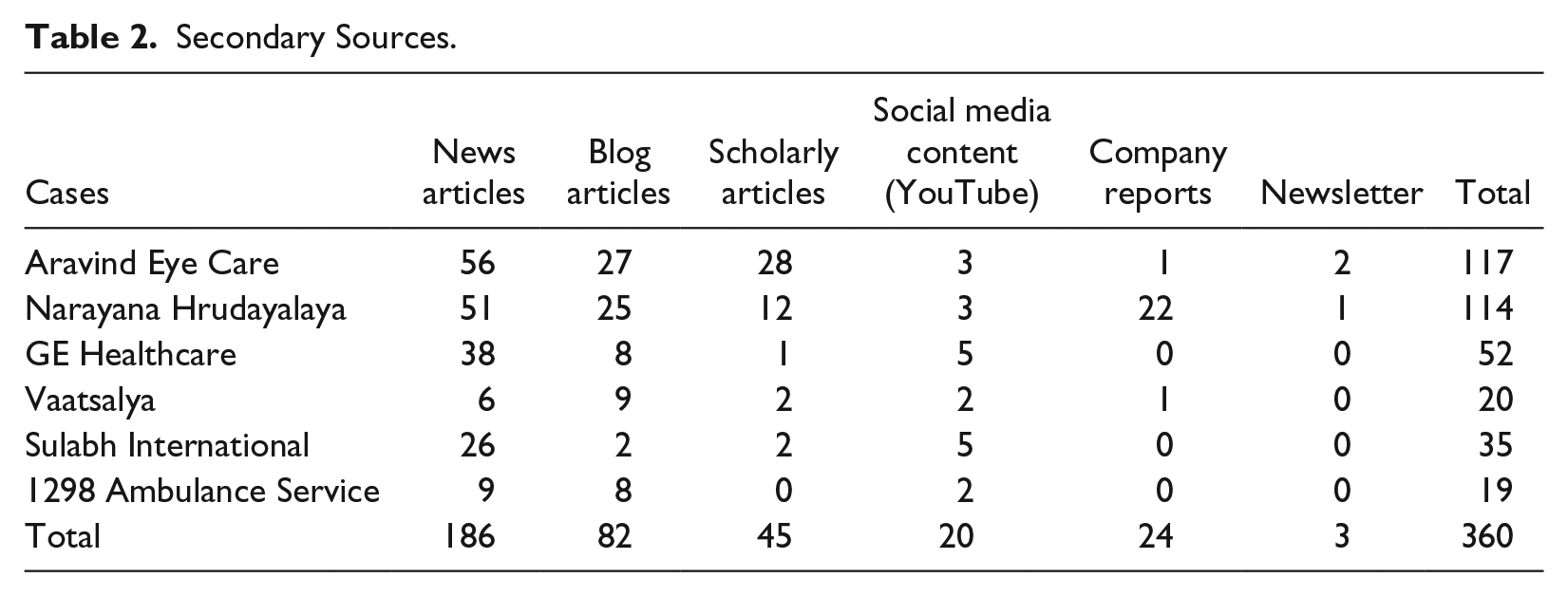
In the second stage, we collected data iteratively from multiple secondary sources such as peer-reviewed scholarly articles, published teaching and research case studies, newspapers articles, business periodicals, annual reports, industry analysis reports, and organizations’ websites. Data available through social media such as YouTube videos and blogs were also collected. Essentially our data sources included both academic articles and grey literature (Bhattacharyya et al., 2010). The authors, with the help of a research assistant, conducted an extensive search of the aforementioned archival material on the selected six health care ventures. The search was carried out using different databases such as EBSCO, ABI-INFORM, ISI Emerging Markets. Google and Google Scholar were also searched to ensure that no relevant archival information had been missed out. The search was conducted using keywords related to the research objectives, such as innovation, different types and aspects of innovation strategies, and names of the selected health care initiatives. A total of 360 secondary sources were consulted (Table 2).
Secondary Sources.
Parallel to the process of collecting and analyzing the archival information, formal and informal interviews with managers of the health care ventures were conducted. A total of 15 interviews were conducted by the authors and their research staff. Senior executives of three organizations: GE Healthcare (5 interviews), Narayana Hrudayalaya (6 interviews), and Aravind Eye Hospital (4 interviews) were interviewed. These three organizations allowed access to authors for the data collection over a period of time. The first author conducted five field visits to Narayana Hrudayalaya, as it has been a key setting of research on inclusive health care undertaken and supervised by the first author. In order to favor openness of the respondents, the interviews have been kept informal. The data collected through interviews were compared, contrasted, and triangulated with the archival material through case studies and other sources.
It is important to highlight here that primary information was accessible for only three ventures out of six selected cases, due to access constraints. BoP contexts pose special challenges in collecting reliable primary data due to difficulties to access the empirical sites (Kolk et al., 2014) and many studies relied on secondary data wholly or partially (Angeli & Jaiswal, 2015; Karnani, 2007; London & Hart, 2004). We believe the potential bias deriving from this methodological limitation to be small, for three main reasons. First, direct interviews have been used to gather insights into the most complex, large organizations, in which business model innovation touched upon multiple dimensions. Instead, the innovative aspects of the smaller, younger ventures of our sample could be adequately portrayed through the use of secondary data only. Second, secondary data also included transcripts of interviews conducted with firms’ managers, so the subjective recounting of the respondents has been taken into account also when primary data were missing. Third, secondary data collection has been conducted systematically and thoroughly, especially for those cases in which only secondary data were available.
In the third stage, we analyzed the collected data by identifying the emerging themes that were common and recurring (Miles & Huberman, 1984). Following the methodological approach used for case-based qualitative research (Eisenhardt, 1989), the emerging themes were constantly analyzed in light of conceptualizations of business models (e.g., Johnson et al., 2008; Osterwalder & Pigneur, 2010; Yunus et al., 2010), and particularly in relation to the value dimensions highlighted by previous literature (value proposition—creation—appropriation). We followed an iterative process of back-and-forth refining between the three business model value dimensions and the themes emerging from the data (Miles & Huberman, 1994). This process led to the identification of eight main themes, or business model innovation strategies, which denoted the strategic approaches that an organization chose to innovate the value proposition, value creation, and value appropriation aspect of their business models. The results of our analysis are presented in the next section.
Business Model Innovation Strategies for Inclusive Health Care
Eight main themes emerged, each corresponding to a particular strategy for business model innovation. It is worth noting here that we name these themes as “strategies” because they denote courses of action, activities, and deliberate organizational choices aimed at establishing and maintaining the firms’ competitive advantage. As organizational choices supporting the realization of innovative business models, we thus describe them as strategies in a more generic sense, which is also consistent with the traditional definitions of the term (Chandler, 1962; Porter, 1996), the common terminology used in BoP literature (e.g., Yunus et al., 2010), and the lexical practice in popular press (Handy, 2014).
We discuss each of these strategies adopted by the selected health care ventures. In the subsequent section, we relate these strategies to different dimensions of the business model framework.
Co-creation of Patient Needs
Health-seeking behavior at the bottom of the pyramid is likely to differ substantially from the average wealthy patient’s behavior. When formulating a value proposition for delivering health care to low-income individuals, a fundamental first step is to ensure that patients are aware of their health needs and recognize the health-enhancing potential of the proposed solution. The fact that health-enhancing services or technologies may not be seen as immediately valuable by patients is interestingly illustrated by the case of sanitation through toilets. A 2014 World Health Organization report estimated that over 2.5 billion individuals do not have access to basic sanitation facilities, including toilets. In India, the problem affects about half of the population; adequate sanitation would spare 600,000 lives annually lost to bacterial-driven diarrheal conditions, enhance dignity and spur safety, by especially avoiding women’s exposure to chances of molestation and abuse. However, the majority of households in urban slums and rural areas, even when the government has installed a toilet, do not use it. This is because the population is not clearly aware that open defecation and inappropriate disposal of human waste directly contribute to bacteriological infections and deaths. Instead, evidence highlights how slum dwellers and rural inhabitants do not want to be exposed to excrements in closed space and certainly not under the same roof where they eat and sleep, a behavior that some associate with lower castes (Mehrotra, 2014). Empirical findings also highlight that the public toilets are often uncleaned and unhygienic and this results in them not being used. Reports document that if common toilets would be kept in hygienic state and offer facilities for bathing and washing clothes, then people would be much more keen on using them and paying for their use (Jha, 2003).
Against this backdrop, Sulabh International developed a successful business model to install toilets after carefully understanding the value that consumers could attach to the product (Kothandaraman & Vishwanathan, 2007). Sulabh understood why previous governmental solutions promoting home-based toilets failed and had been rejected by BoP consumers. Sulabh developed the new model of public pay-per-use toilets for slum dwellers and urban poor, which addressed their resistance to having to deal with human excreta at home. The user charge was extremely affordable and recognized that even the very poor are willing to pay a small amount for a clean toilet. Particularly important was the creation of a service experience in public toilets, where also bath, laundry, and accommodation were offered. Even more salient are the health promotion and education activities promoted by Sulabh, as illustrated by the Sulabh International Institute of Health and Hygiene and the Sulabh International Museum of Toilets. Both were specifically created to raise the awareness of sanitation and hygiene by training teachers, school children, volunteers, and associates involved in promoting hygiene. Sulabh International Institute of Health and Hygiene imparted training to more than 8,000 female associates to work toward creating awareness about sanitation and health (Kumar Rastogi, 2013).
The Sulabh example illustrates how health needs and their solutions are co-defined in a dynamic interaction between patients (consumers) and providers. Health promotion and health awareness are only a necessary but not sufficient precondition; the following step is a patient’s understanding that a specific solution is available, at an affordable price and offered by a trusted provider.
Community Engagement
While the individual consumer is the traditional target for orthodox business models, delivering health care to patients in low-income markets requires a stronger focus on communities of patients, for two main reasons. First, the underprivileged are often strongly geographically scattered, and their levels of literacy, language, access to traditional media, technological skills, beliefs toward new technology widely vary across communities (Hammond et al., 2007; London, 2008; Sachs & Bono, 2005; Sanchez, Ricart, & Rodriguez, 2007; Webb, Kistruck, Ireland, & Ketchen, 2010). Such cultural, psychological, and linguistic differences often require entirely different solutions when moving from a community to another, frequently hampering scale economies and wide success of BoP endeavors (Angeli & Jaiswal, 2015). Second, because of their isolation and because of institutional voids, low-income patients are predominantly influenced in their behavior and choices by informal institutions; hence, those social norms, beliefs, cultures, and ethics are idiosyncratically developed within the social groups and communities (Angeli & Jaiswal, 2015; De Soto, 2000; Rivera-Santos & Rufín, 2010). It follows that to sharpen need awareness and to ensure the successful acceptance of proposed solutions, particularly in the case of health care delivery, a process of trust creation through community bonding is important.
For the poor and the underprivileged, the relationship to the community often has much higher relevance than for economically well-off patients. That is why Vaatsalya, a Karnataka-based budget hospital chain started in 2004 continuously attempts to gain patients’ trust and build a long term relationships with them. Vaatsalya primarily provides treatment for chronic ailments in rural and semi-urban areas. People suffering from chronic diseases develop a special long-term relationship with a doctor, after overcoming all fears and psychological barriers due to unfamiliarity. Initially, when Vaatsalya was established, the management realized that patients were reluctant to visit its hospitals, partly because private healthcare providers such as Vaatsalya were perceived to be providing costly treatment. However, patients also feared that seeking treatment at Vaatsalya would negatively affect their relationships with local physicians, who were mostly unqualified doctors. This risk could result in losing the possibility to be cured, if Vaatsalya would stop its operation after a while. Therefore, it was critical for Vaatsalya to gain the trust of its patients by ensuring long-term commitment to the local community (Mukherji, 2010).
Another salient illustration of the relevance of community-oriented approaches can be drawn from India-based Aravind Eye Hospital (AEH). Blindness is one of the major epidemics in India, affecting millions of people (Dandona & Dandona, 2003). Combining the philosophies of mass marketing, Dr. Venkataswamy founded AEH in 1976 in Madurai, India. AEH was established for providing finest quality eye care to a maximum number of patients at minimum cost. While India has a large population suffering from cataract, it was not easy for AEH to bring patients to the hospital. Research conducted by AEH documented that even when free treatment was available, a mere 15% of patients diagnosed with cataract visited the hospital to undergo surgery. Such low rate can be explained by patients’ not being able to afford expenses for food and travel, fear of surgical operations, family obligations and unavailability of family members to travel with the patients and support them through the treatment. AEH overcame these constraints through a well-planned outreach program that centred on the use of eye camps, organized with the help of local business or social organizations. Bus travel was planned in a way so that patients from the same region could be clubbed together and could naturally support each other before and after surgery (Mukherji, 2010).
By understanding the relevance of the community in the lifestyle and in the health-related behavior of low-income patients, organizations like Vaatsalya and AEH have developed successful business models, which increase the patients’ awareness and trust toward their health interventions and, thus, enhance patients’ acceptability of the same.
Continuous Involvement of Customers
The development of low-cost medical devices for rural areas was full of challenges for GE in India given its traditional focus on premium products. GE product teams spend enormous time to develop in-depth understanding of its customers’ requirements. Teams continuously interact with different users of medical devices such as doctors and medical staff. Their objective is to collect relevant insights about the extent of use of medical devices, how they are being used, problems and difficulties faced in using them, issues related to maintenance of these devices, and the overall experience of the users. In many cases, team members faced severe difficulty in interacting with users of medical devices, because the medical staff in a government hospital and in primary health care centers thought that they were officials who had come there for inspection. To address this problem, the product team sought the help of MART, a marketing research organization having a strong presence in the rural areas. Through the help of MART, product teams comprising product managers and engineers visited the large number of villages in different parts of India (Malodia & Jaiswal, 2015).
GE teams found that doctors and small clinics in rural areas cannot afford the existing premium electrocardiography (ECG) machines as their patients have low paying capacity. Besides these machines are heavy and bulky, need trained operators, and require extensive service support. The team realized that rural doctors need affordable devices that can be battery-operated and thus can run even without electricity, are easy-to-use, robust, and do not need much maintenance. For instance, the team realized that the devices should be operable by somebody who is aware of traffic signals, a “green” switch to start and a “red” button to stop (Govindarajan & Trimble, 2012). The continuous engagement with the customers helped the team develop products that are affordable, suitable for local needs, and can be used on a regular basis.
Medical Technology Innovation
The introduction of technological innovation is one of the fundamental ways to lower production and delivery costs of clinical interventions. Global electronic manufacturer GE launched low-cost medical equipment in the form of Tejas XR and Mac 400 series for Indian consumers. GE redesigned two of its products to suit the largely scattered poor population in Indian villages. With half the cost of imported machines, Tejas XR 6000 X-ray machines provide high-resolution digital images for superior radiology diagnosis (Express Healthcare, 2008). The battery-operated portable Mac 400 ECG machines manufactured by GE cost less than a fifth of conventional machines available in the market, and produce ECG reports at less than US$1.00 (INR 66, as per currency exchange rates in 2016). With important features like 1.1 kg weight and a rechargeable lithium-ion battery, Mac series was designed for power-starved areas in a country like India. With a capacity to perform 100 ECGs on a single battery charge, Mac 400 comprises easy-to-use software applications, making it convenient to use even for the less specialized medical professionals (Business Week, 2008). GE Healthcare also developed several other low-cost medical devices in India such as Discovery IQ PET/CT scanner and Lullaby baby warmer (Globalhealth.care, 2014).
Another important example of technology-enabled health care is the case of telemedicine in Narayana Hrudalayala (NH). Dr. Devi Prasad Shetty established NH Hospital in 2001 in Bangalore with the aim of providing low-cost quality cardiac care to all. By 2014, NH had 26 hospitals in 16 cities with 6,900 beds, 13,000 employees and 1,500 doctors (Madhavan, 2014). Dr. Shetty felt that doctors do not need to be physically present with the patients to diagnose heart problems, and that technology could be exploited to provide treatment to poor patents living in remote villages. NH established cardiac care units (CCUs) which were connected with the main hospital through video conferencing. NH provided beds for patients, medicines, computing devices, and ECG machines in CCUs. CCUs were managed by medical staff who were given technical training to operate medical devices (Mukherji, 2010). Till 2008, NH analyzed distantly generated over 144,000 ECG outputs and 33,000 angiograms making this initiative the world’s largest telemedicine project on cardiac care (Suresh, 2012). NH also developed standardized processes to reduce morbidity and minimize complications. Following a new protocol, it achieved the target of zero incidence of bed sore post–heart surgery against the 8% to 40% incidences worldwide. NH’s protocol was adopted by the American Nursing Association to decrease the bed sore cases in the United States (Kachhap, 2015).
New medical devices can also replace some crucial components with indigenously produced similar components. This approach can be termed as import substitution and constitutes a second use of product innovation to rethink health care business model. For example, through its division “Aurolab,” AEH started indigenous production of intraocular lenses (IOLs), a popular component used in eye surgeries. Previously, IOLs were predominantly imported in India from the United States at an average unit price of US$100 to 150, making the surgery too costly for poor patients. AEH brought down the price of the IOL at nearly US$ 6 per each without any compromise in quality. At present, AEH serves 10% of the World’s IOL requirement, supplying to 120 countries across the world (Bhattacharyya et al., 2010; Madhavan, 2013).
Focus on Human Resources for Health
Among the reasons why health care delivery is expensive is the wide deployment of specialized knowledge and labor in most phases of care and treatment (Christensen et al., 2000). Developing business models for inclusive health care delivery demands innovative solutions that enable the use of the same human resources at lower costs or the use of less expensive resources.
One way to maintain the same resources but at lower expenses is to provide medical professionals, or human resources for health (HRHs) with reasons other than financial incentives to offer their services. This approach focuses on leveraging the intrinsic motivation of health professionals (Mathauer & Imhoff, 2006). Adopting the no-frills approach, Vaatsalya focuses on patients in semi-urban and rural areas and charges around INR 100 to 300 (US$2-7) per bed for basic health care treatments to patients who need hospitalization. Its founders set up a model of incentives to attract doctors who grew up in rural and semi-urban area but had moved to large towns for completing their medical studies. A good number of them appeared to be inclined to return to their home towns and set up a medical practice there. A doctor can gain recognition much faster in small towns, which are typically characterized by acute shortage of trained doctors. To further increase incentives, Vaatsalya provided them salary and monetary benefits that were 20% to 25% higher than the compensation offered by hospitals in the major cities, in addition to comparatively higher designations and positions of responsibility (Mukherji, 2010).
A second way to decrease the costs related to medical personnel is to use task reallocation practices (Niezen & Mathijssen, 2014). The disruptive innovation perspective calls for a shift of caregiving from higher skilled to lesser skilled professionals, as part of the necessary transition to enable low-cost business models in health care (Christensen et al., 2000). NH has made task reallocation a core point of its strategy. Dr. Shetty identifies the scarcity of qualified doctors as one of the most critical hurdles in making quality cardiac care accessible to a large section of Indian population. For instance, in India over 18,000 doctors graduate from medical schools annually, however merely 1% of them specialize in cardiology and cardiac surgeries. NH’s founder planned to reduce this gap by setting up training programs to create an intermediate level of expertise to deal with emergency and nonintervention heart procedures. NH launched 19 postgraduate programs in different areas of cardiac care for doctors and other healthcare professionals (Mukherji, 2010).
Strategic Partnerships
Medical technology innovation and adequate medical personnel can be considered the two most important internal resources that need to be developed in order to support business models at the BoP. With the aim of sustaining the quick and effective acquisition of such internal resources most of the selected cases make use of an extensive network of strategic partners. For example, together with Indian Space Research Organization (ISRO), NH started the world’s largest telemedicine program to reach the rural areas while containing the costs. ISRO had supported telemedicine as part of its social mission and offered connectivity to the CCUs without any charges. Similarly, in 2005, NH partnered with Indira Gandhi National Open University to provide India’s first diploma in cardiac care as part of which doctors with MBBS degree complete 2 years of training at NH or at 50 other reputed cardiac care centres in India (Mukherji, 2010). On the training side, 1298 Ambulance service offers programs in collaboration with the American Heart Association and New York, Presbyterian Hospital, which allows it to provide high-quality, internationally recognized certificates.
Economies of Scale
Given the imperative of cost reduction and low customer margins, business models for inclusive health care often achieve profitability and sustainability primarily through the scale effect. For instance, NH is by far the finest example of health care organization effectively exploiting scale benefit, and providing quality cardiac treatment to all strata of the population.
Globally Indians account for 45% of total coronary artery disease patients (Kohn, 2008). One-third or nearly 2 million people in India die each year because of heart-related diseases (Gaziano, 2007), and among them, the poor are the worst victims of it due to lack of paying abilities. To treat a maximum number of patients, Dr. Shetty created NH with a very large bed capacity. Today, NH is a 1,000 bed hospital in Bangalore that conducts on average 35 major heart surgeries per day and a maximum of 60 per day in its 24 operation theaters, making it one of the largest cardiac hospitals in the world. By contrast, the largest heart hospital in the United Kingdom has 270 beds, 5 operating theaters, and conducts 58 operations a week (Cawston, 2014).
NH adopts assembly line model in conducting heart surgeries, as part of which junior doctors do all the early stage tasks while the specialist surgeon performs only the core part of the surgical process. This enables specialist surgeons to conduct three operations per day in comparison to just one surgery conducted by surgeons per day in the developed countries (Ganguly, 2013). Assembly line model not only reduces costs but also improves quality as conducting surgeries repetitively enhances doctors’ skill and minimizes errors. NH’s mortality and infection rates are 1.27% and 1%, respectively, for coronary artery bypass graft operations, which are comparable to U.S. hospitals. However, the average cost of a bypass surgery at NH is $1,500 (INR 99,000) in comparison with US$144,000 in the United States (Madhavan, 2014).
Another example of economies of scale is AEH’s entire surgical process, which is also designed as per the assembly line model. AEH realized the capacity constraints in the form of shortage of qualified ophthalmologists in India. At AEH, trained support staff and nurses perform all the activities before and after the operations. This allows surgeons to devote their time only to the core activity of surgical operation. In the preoperative stage, patients in groups are readied by staff. All the AEH’s operation theaters have two or three surgical tables. Once a surgeon finishes the surgery on the first table, after doing necessary sterilization, he shifts his attention to the next patient waiting in the second table already prepared by the staff. The treated patient is quickly moved to the recovery ward for the postoperative care, the surgical supplies are quickly replenished and the first table is ready to receive the next patient (Rangan & Thulasiraj, 2007). On an average an ophthalmologist at AEH performs 2,000 cataract surgeries in a year, which is 4 times more than the average number of surgeries normally conducted by an ophthalmologist in India. Every year, AEH alone performs 60% of the total eye surgeries carried out by the United Kingdom’s National Health Service, at 1/1,000 of the cost (Rangan & Thulasiraj, 2007). At the same time, the surgical complications arising at AEH are half the complications occurring within the National Health Service in the United Kingdom (Rosenberg, 2013).
Cross-Subsidization
Ensuring a suitable mix of wealthy and low-income patients is often crucial, in order to achieve cross-subsidization. A cross-subsidization model promotes the organizational mechanism wherein affluent consumers pay relatively higher price for a product or service compared to their underprivileged counterpart, who pays lower prices for a similar product or service. The earlier discussed example of AEH also makes use of a cross-subsidization philosophy. AEH’s 40% patients are affluent and pay for eye surgeries, while the remaining 60% of patients are charged negligible or no fees. Affluent or paying patients receive better support service such as beds against floor mats for poor patients, choice of air-conditioned rooms and separate or partially shared bathrooms. However, the hospital provides the same surgical facilities to every single patient and periodically rotates doctors between paid and free sections of the hospital. Furthermore, the criticality of serving affluent patients forces AEH to keep stringent control over the quality (Rangan & Thulasiraj, 2007).
Another example of cross-subsidization is offered by a paramedical service Dial 1298 ambulance. Started in 2005 in Mumbai, India, Dial 1298 provides well-equipped fine quality ambulance services in the city. Despite Mumbai being a metro city, it abysmally lacked efficient, reliable, and up-to-the-mark ambulance service. In particular, the poor were deprived of timely medication, owing to the expensive ambulance service. Keeping in mind this access gap, Ziqitza Healthcare in association with the London Ambulance Service, started Dial 1298 for Ambulance in Mumbai (Acumen Fund, 2009). Ziqitza designed its pricing on a “sliding price scale” model where patients were charged as per their ability to pay, providing an opportunity to poor people to access quality ambulance service. Nearly 20% of all Ziqitza Healthcare patients use the ambulances for free or pay at a lower rate to the company. The company charges its patients on the basis of their hospital selection. Patients deciding to seek treatment in a government hospital are categorized as “poor” and provided free service, while patients opting for luxury hospitals are charged comparatively more. The company owns two types of ambulances—full-service ambulances equipped with advanced equipment and Basic Life Support ambulances. Recently the model has scaled up and evolved and is currently operated by dial 108 for free services and 1298 for paid services (Choudhury, 2014).
Discussion
This article used six cases to unravel business model innovation strategies for inclusive health care. Our evidence highlights that co-creation of patient needs, community engagement, continuous involvement of customers, medical technology innovation, focus on human resources for health (HRHs), strategic partnerships, economies of scale, and cross-subsidization are the core strategies that underpin the success of the selected business models.
Our findings suggest the need for refining and extending the existing conceptualization of business models in the context of inclusive health care at BoP. In fact, the traditional triadic framework of value proposition–value creation–value appropriation proposed in the existing literature (e.g., Yunus et al., 2010) only partially encompasses the innovation strategies that emerge from our empirical evidence. Processes of value creation—which recombine internal and external resources to create value—are clearly employed in health care ventures studied by us through the use of strategic partnerships, development, and procurement of innovative medical technologies and focused development of human resources. In line with existing literature, value creation involves the utilization of not only the key internal processes, systems, and organizational resources but also the resources and capabilities pertaining to the external network or value chain (Johnson et al., 2008; Yunus et al., 2010). Likewise, economies of scale and cross-subsidization well exemplify innovative strategies on the value appropriation dimension of business models, which must ensure financial returns. Delivering health care services to underprivileged masses requires also that a share of the created value be appropriated by the providers, and shared with suppliers, distributors, alliance members, and other value chain partners. In the context of inclusive health care, value appropriation models should be sensitive to the extreme affordability demands of the BoP consumers and socially responsible pricing (Vachani & Smith, 2004). At the same time, sustainability of business models should be ensured, as in the case of social businesses (Yunus et al., 2010) and in some cases acceptable surplus to the actor(s) instrumental in design and execution of the business model. Low-income patients in emerging economies are most often uninsured, and they mainly rely on out-of-pocket payments to finance health care. Successful business models for inclusive health care rely on innovative ways to lower production costs, and push internal efficiency.
On the value proposition side, the strategy of continuous consumer involvement enables the development of strong value propositions, and in defining product/service solutions that adequately respond to consumers’ needs. In both Johnson et al.’s (2008) and Osterwalder and Pigneur’s (2010) conceptualizations, the customer value proposition triggers the creation of a business model, as it directly responds to the need to satisfy a specific customer by “getting a job done,” and provide a solution to a problem (Johnson et al., 2008). An implicit assumption of these studies is that, once the innovation is coupled with an appropriate business model and has overcome stakeholders’ resistance, the customer acceptance will follow. The value proposition concept in the existing conceptualizations of business model (Johnson et al., 2008; Osterwalder & Pigneur, 2010; Zott & Amit, 2008) and even those designed for understanding social businesses (Yunus et al., 2010) appears however to lack in-depth elaboration of the acceptability and awareness dimensions of a product or service, which is instead salient to the delivery of health care services at the BoP. When providing product and service solutions to BoP consumers, however, the formulation of a customer value proposition is only but the end point of a much longer process. The identification of the problem is far from straightforward, and issues of cognitive resistance to a solution that seems to be perfectly in line with the problem are to be taken into account. The cognitive gap—or institutional divide—between producers and customers is a known challenge when serving BoP markets (Angeli & Jaiswal, 2015; Hart & Sharma, 2004; Rivera-Santos et al., 2012). The cognitive gap between providers and consumers becomes even more accentuated in the case of health care delivered to low-income patients in developing countries. Our organizational cases, in fact, show how strategies such as co-creation of patient needs and community engagement enable the process of increasing need awareness in the patients, in a way that is socially acceptable to both individuals and communities.
Our findings hence suggest an additional element that previous systematization of (social) business model has not taken into account: the value discovery. Value discovery denotes here a co-creation process through which the health care need is identified by the patient and the organization together. The concept of value discovery stems from the traditional value proposition dimension, but expands it and adapts it to BoP settings. In particular, our evidence documents that such process precedes the formulation of a value proposition, which instead takes for granted both the presence and recognition of a preexisting need. A process of value discovery is fundamental to business models that aim to effectively and efficiently deliver health care, because the health care need often goes unrecognized or deliberately neglected. This is even more critical in BoP settings, where a large number of conditions go untreated. Business models that incorporate strategies of need co-creation and community engagement prove successful as the value propositions rest on a bottom-up assessment of what BoP patients know, want, trust, and are willing to pay for.
Against this backdrop, a first contribution of this work proposes an important extension of the existing business model conceptualization by incorporating value discovery as a fundamental antecedent to value proposition, value creation, and value appropriation dimensions. The resulting extended framework for BoP business models is hence represented in Figure 1. Table 3 presents the salient empirical evidence related to each case and draws the link between the cases, the innovation strategies, and the four business model dimensions represented in our extended framework. Also, Table 3 clarifies the distinction between value proposition and value discovery, and highlights which cases present relevant evidence on the two separate dimensions.
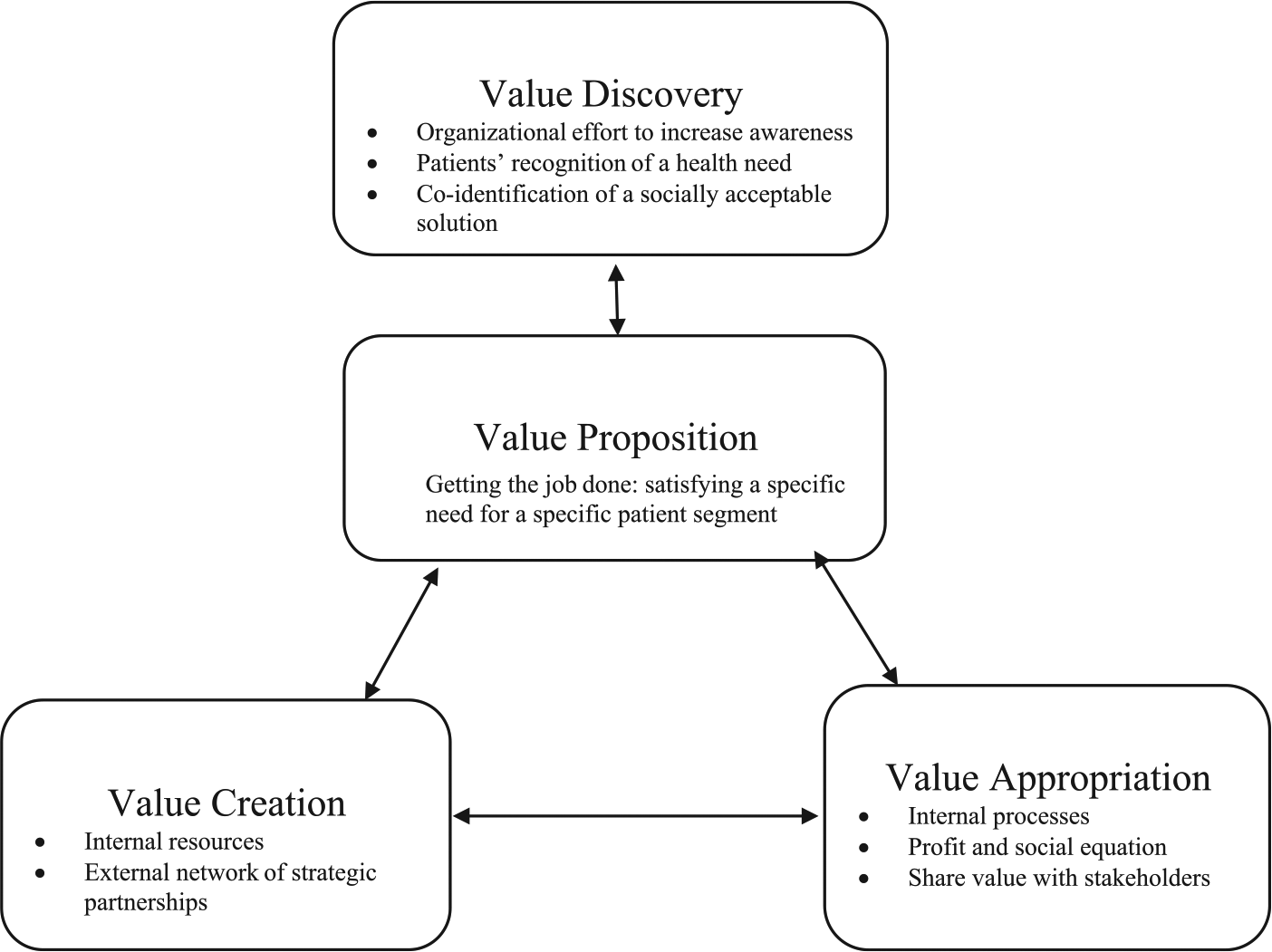
Business model conceptualization for delivering health care at the base of the pyramid (BoP).
Innovative Business Model Strategies Illustrated by the Six Cases.
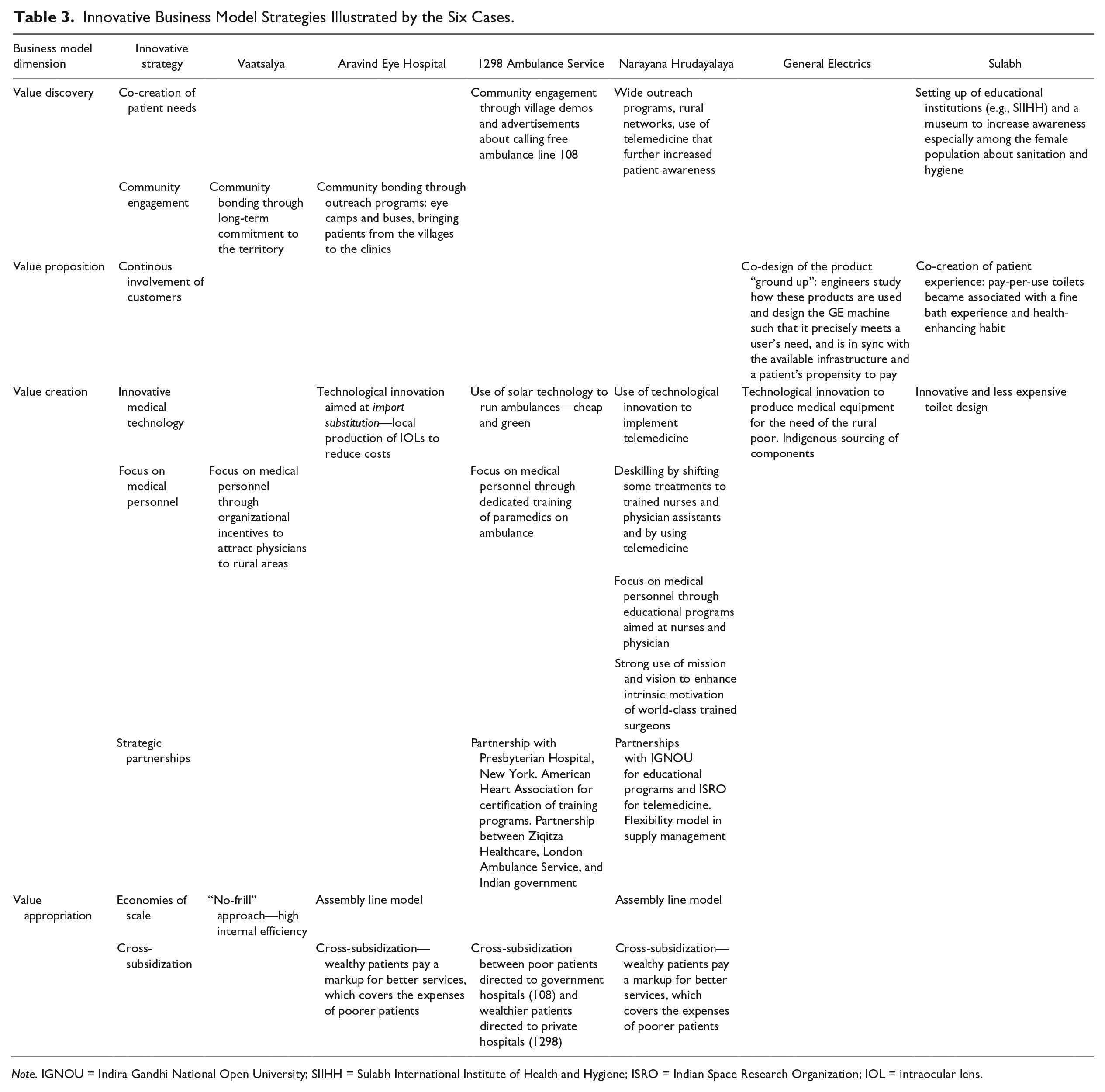
Note. IGNOU = Indira Gandhi National Open University; SIIHH = Sulabh International Institute of Health and Hygiene; ISRO = Indian Space Research Organization; IOL = intraocular lens.
The relevance of value discovery in delivering health care at the BoP strongly emphasizes how in resource-constrained contexts, customers’ and communities’ needs must constitute the starting point of sustainable business models. Rather than being a mere building block in a larger business model representation, engaging patients and communities through need co-creation seems to be the generative trigger for successful BoP business models to emerge and prosper. This first “gear” works as a starting point for what we can define as a business model mechanism for health service delivery at the BoP (Figure 2). After patients and communities have been successfully involved in the health need recognition and development of acceptable solutions and at the same time made aware of available treatments, local supply can be motivated to enter the business at favorable conditions. This is the case for example of suppliers of medical technologies, who commit to technology development or import substitution for the BoP once there is evidence of a market opportunity. After the demand is ascertained, the cost of the core suppliers (technology and medical professionals) has been agreed upon, and strategic partnership is forged, financial mechanisms such as cross-subsidization and economies of scales can further help price reductions for BoP segments and allow for adequate financial returns. The three foundational gears of the mechanism are therefore value discovery and value proposition, which leverage engagement of patients and communities, through need co-creation and community approaches; value creation, which hinges on suppliers of medical technology and of educational and training programs, in order to develop adequate internal resources; and finally value appropriation, through strategies such as cross-subsidization and economies of scale. The business model mechanism for health delivery at the BoP, represented in Figure 2, is hence activated by and through the patients and communities, which then triggers the development of internal resources through external partnerships and further proceeds with the adjustments of the financial cost/revenue equation. Although developed in the context of health care delivery, this dynamic model can be applied to other segments of BoP markets, where conditions might be less critical and far less complex.
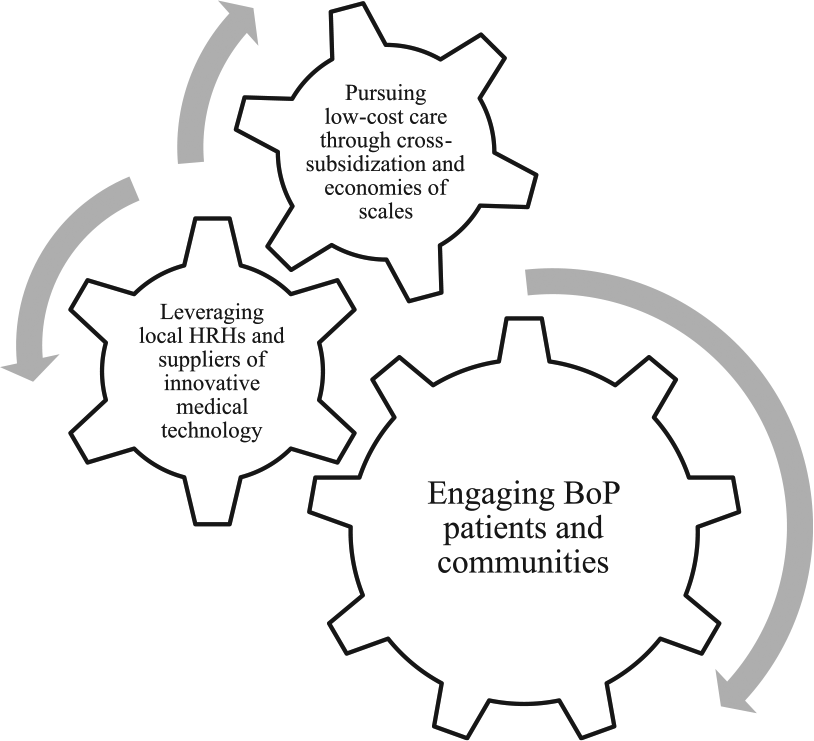
Base-of-pyramid (BoP) business model mechanism.
The BoP business model mechanism as represented in Figure 2 provides a second important contribution to business model conceptualization for BoP markets. Business models have been so far represented through a collection of building blocks; however, the interdependencies and hierarchies among the salient dimensions have been left widely underexplored. Through the examination of BoP business model for inclusive health care, this study highlights that the essential approach for the successful business model at the BoP is the customer engagement and community involvement. This result goes in line with recent work that highlights the superiority of “open business models” in resource-constrained environments (George et al., 2015), which incorporate ideas and stimuli that originate both internally and externally to the organization. Open innovation as intended here hinges on co-creation approaches, which promote early and deep involvement of end (BoP) consumers in the design of product or service solutions (Alexy & George, 2013; George et al., 2015). This work advances this line of conceptualization by highlighting that before solutions can be co-designed, needs have to be co-created, through community engagement and health education and promotion. Need co-creation constitutes the very primary gear that is able to activate a successful model, particularly evident in the health care domain.
Implications
There are many practical implications of our study for poverty alleviation in resource-constrained settings. The new conceptualization advanced in this paper provides an encompassing and more accurate lens for understanding the innovativeness of the business models presented in our cases. While providing evidence that market-based approach can work (Bhattacharyya et al., 2010; George et al., 2015), such insights can directly inform nascent public as well as private sector initiatives aimed at improving health care access, which is a critical and complex issue in BoP domains. Eight main strategic mechanisms emerge that underpin successful inclusive health care delivery, and they lend themselves for direct use by practitioners. By focusing on a specific industry (health care) in a specific segment (BoP), this article to our knowledge is the first attempt to provide practical guidelines on how traditional business models can be disrupted to serve new needs. While existing literature has developed widely generalizable frameworks, the goal here instead has been to detail the specific strategies that guide a business model shift toward higher affordability and inclusiveness.
The empirical cases and the theoretical framework offered here can be useful in guiding policy interventions. Health measures are among the first agenda items of policy makers not only in developing but also in developed countries, increasingly facing the urge to contain the rising costs of health care without compromising the foundational principle of universal health coverage. It is important to consider that, although health care is one of the fastest growing economic sector, absorbing up to 16.4% of U.S. GDP and 8.9% of OECD countries’ GDP in 2013 (OECD, 2015), it is also strikingly one of the least innovative field (Berwick, 2003; Herzlinger, 2006). Care provision is rooted in well-established, expensive, and inaccessible-to-many business models, which create substantial institutional and professional resistance to the conception and implementation of new, low-cost solutions (Christensen et al., 2000). It is obvious that public expenditure devoted to health care is destined to rise, in the absence of low-cost private sector alternatives. Based on these success stories and business model innovation strategies, specific measures and policy tools targeting health care organizations can be developed, with a clear view to decrease costs while maintaining high quality standards.
These findings should be considered in light of two main limitations, which provide directions for future research. First, the use of six case studies has provided broad and varied understanding at the expense of in-depth insights into organizational mechanisms enabling the success of specific strategies instead of others. Qualitative in-depth inquiries into a smaller sample may bridge this gap. Second, our main focus on India may raise concerns regarding the existing context-specific factors that may limit the disruptive potential of the strategies in other geographies. Future studies in other countries or world regions can corroborate the extendibility of such strategies or enhance the understanding of how health care can be made accessible to BoP patients with innovative approaches successfully developed and adopted in different contexts.
Footnotes
Acknowledgements
Authors are thankful to Harit Palan for providing research assistance in the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The second author acknowledges the Research and Publication unit at Indian Institute of Management, Ahmedabad for financial support for the project.