
Abstract
At-home respite services seem too rigid to meet the needs of older adults and their caregivers. It is critical to develop service flexibility, as it allows for personalized care, adapted to health conditions, preferences, and evolving needs. While no prior studies used coconstruction methods to increase flexibility, this study could offer a better understanding of flexible respite for stakeholders. Using a living lab approach, this article aimed to (1) empirically determine the characteristics of this type of respite model and (2) document the levers and obstacles to consider for its implementation. Starting from a pre-existing flexible respite model named ANAAIS, the research team led workshops and interviews. First, the team carried out 2 workshops (TRIAGE and persona-scenario) with a total of 3 caregivers and 8 homecare professionals or managers. Second, a team member conducted interviews with 3 caregivers and 6 homecare professionals or managers. Content analysis was used on the data. The stakeholders coconstructed a Québec version of ANAAIS, a web application allowing caregivers to request an affordable respite, at the time wanted, and offered by a qualified care worker, through a simple application. Levers and barriers to its deployment are linked to the model’s characteristics as well as its internal and external context. For example, relations and connexions were perceived as a lever to deployment, while the lack of resources was considered an obstacle. This living lab project showed the feasibility and pragmatism of coconstructing a flexible and applicable respite service model.
Introduction
Caregivers play a crucial role in allowing older adults to age in their home. A caregiver is “a person who provides some type of unpaid, ongoing assistance with activities of daily living or instrumental activities of daily living.” 1 Caregivers of older adults are responsible for a considerable amount of homecare, 2 potentially leading to physical and psychological burden. 3 To support them, private and public organizations offer various services, including respite. Respite is “the temporary provision of care for a person, at-home or in an institution, by people other than the primary caregiver.” 4 Widely recognized as necessary support,5,6 many studies identify the need and use for at-home respite.6 -9
Although respite is deemed necessary, it is seldom used.10 -13 Despite their burden, as little as 6% of all Canadian caregivers use it. 11 This worldwide under-usage 14 can be explained in part by a lack of flexibility.15,16 Caregivers often feel that they are being prescribed services according to organizational criteria rather than their needs.17,18 At-home respite seems too rigid to meet the caregivers’ needs. It is crucial to enhance flexibility for personalized care that adapts to health conditions, preferences, and evolving needs.
Although respite best practices are rooted in person-centeredness, 19 few studies involve stakeholders, such as caregivers and respite providers, to develop respite models and to document the factors linked to their implementation. Stakeholders tend to agree that flexibility is critical: The challenge lies in the coconstruction of an applicable model, effectively leveraging the strengths, and overcoming the obstacles of implementing flexible respite. 14 To address this challenge, stakeholders must come together to coconstruct a solution,6,20 -24 considering specific circumstances and perspectives. 14 This holistic approach is crucial, since existing research indicates that the implementation of flexible respite models can be challenging.25,26
Objective
Through a living lab approach, the article’s objectives are to: (1) Empirically determine the characteristics of a flexible at-home respite model and (2) document the perceived levers and obstacles to consider for its implementation.
Methods
Research Approach
This study was embedded in a larger living lab project27,28 (Figure 1) that began with a scoping review 29 and a consultation with 12 stakeholders to identify the core characteristics of flexible respite. This first phase allowed to identify ANAAIS 30 as a potential model; Figure 2 contains a detailed description of ANAAIS. This article presents phase 2 of the project: The coconstruction of the Québec version of ANAAIS (ANAAIS-QC) and the documentation of the levers and obstacles to consider for its implementation in the Eastern Townships. The Research Ethics Committee of the Eastern Townships Integrated University Health and Social Services Centre approved this project (project number 2022–4492). All participants provided written informed consent.
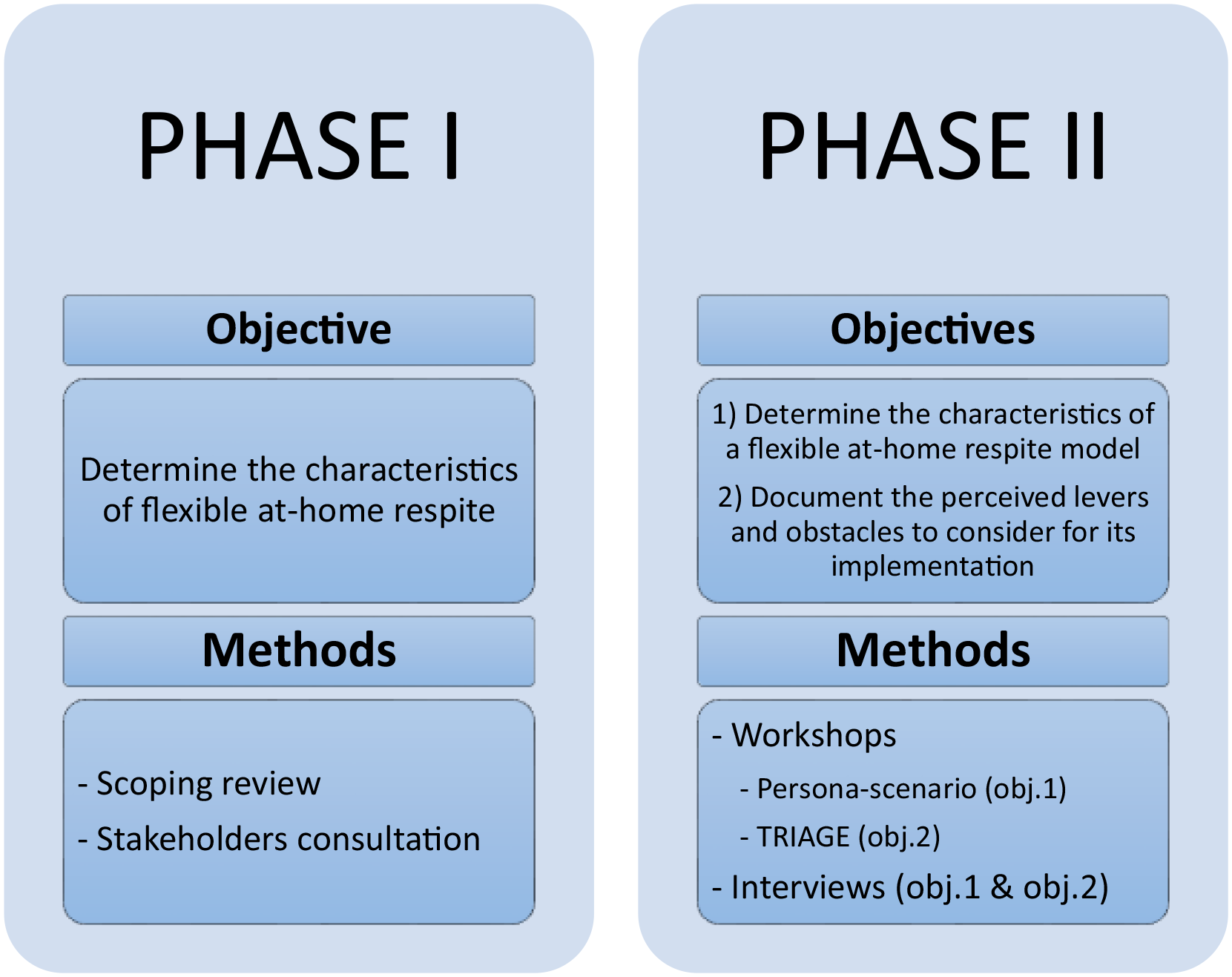
Project phases.
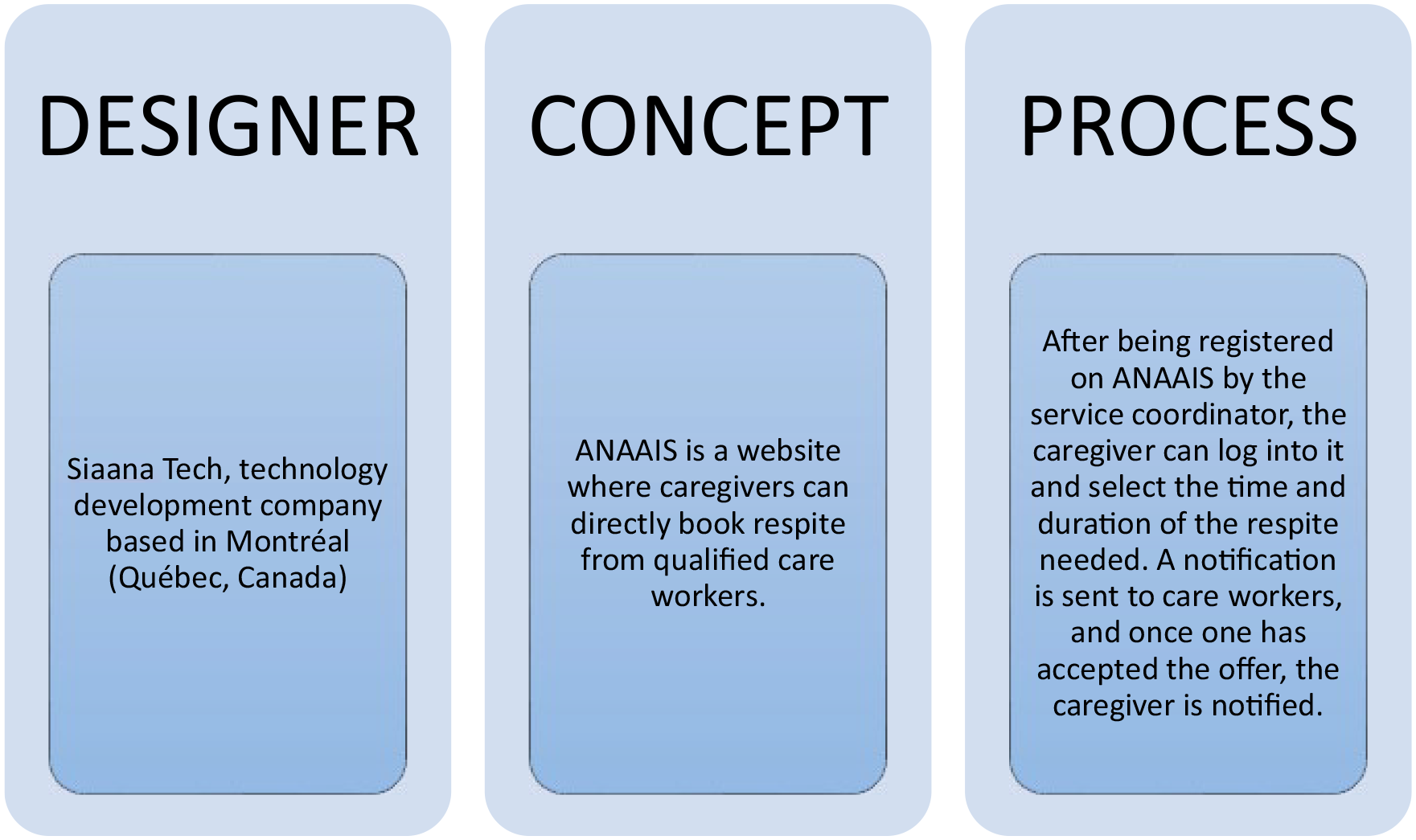
ANAAIS’s characteristics.
Method 1: Coconstruction Workshops
Sampling and recruitment
The research team used a convenience sampling approach by sending emails to all homecare organizations and concertation tables in the region to constitute the targeted sample of 12 participants.31,32 The targeted stakeholders were equal parts caregivers, care workers, as well as representatives of public homecare services and community homecare organizations (CHCO) from the Eastern Townships.
Data collection methods and tools
The research team held 2 workshops. The first, to determine the characteristics of ANAAIS-QC (obj. 1), used persona-scenario. Persona-scenario involves the creation or validation of scenarios from a user points of view. 33 Specifically, participants were presented with one step-by-step scenario of a caregiver using ANAAIS. The participants then validated each step or suggested modifications to create the desired “path” from registration on the application to the end of respite.
In the second workshop, the research team used the TRIAGE method,31,34 an animation technique used to reach consensus within a group. Participants were invited to write, sort, and prioritize, in sub-groups, statements that describe perceived levers and obstacles to ANAAIS-QC’s implementation (obj. 2). Plenary concertation allowed to reach consensus.
Method 2: Interviews
Sampling and recruitment
Through a convenience sampling approach, administrators from 2 CHCO who took part in the workshops approached caregivers and care workers, individually. 34 The participants had (1) a smart mobile phone or a tablet and (2) access to the Internet. A sample of 7 participants per CHCO was targeted, based on their administrators’ knowledge of the available sample: 2 to 3 caregivers, 2 to 3 care workers, plus the administrator.
Data collection methods and tools
In the first CHCO, participants used ANAAIS for 6 months (July-December 2022) and were interviewed before the trial, at mid-point and at the end. In the second CHCO, the participants simulated the use of ANAAIS prior to a single individual interview. The research team developed 1 interview guide adapted from the Consolidated Framework for Implementation Research (CFIR) 35 and co-validated it with 1 researcher and one of the CHCO administrators. The questions included: What aspects did you like the least about ANAAIS? How could we improve these aspects? What resources would be needed to implement it?
Data Analysis
The research team based the content analysis 36 on the audio-taped interviews and workshops notes. The WHO, WHEN, HOW framework 29 served as a starting point to characterize ANAAIS-QC (obj. 1). To define the levers and obstacles for its implementation (obj. 2), 3 dimensions of the CFIR were used 35 : Innovation, inner setting, and outer setting domains. A student-researcher categorized the extracts in the different categories, in either framework, and then defined them. The analysis was reviewed by one of the co-authors, ensuring that all categories were discussed until a consensus was achieved. 37
Results
Descriptions of Workshops and Participant Interviews
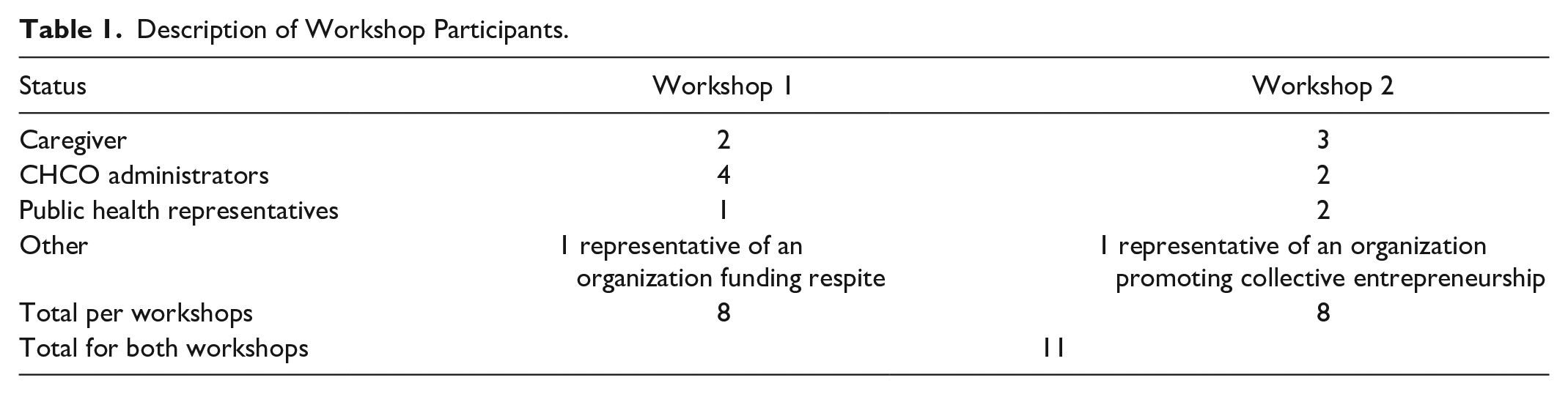
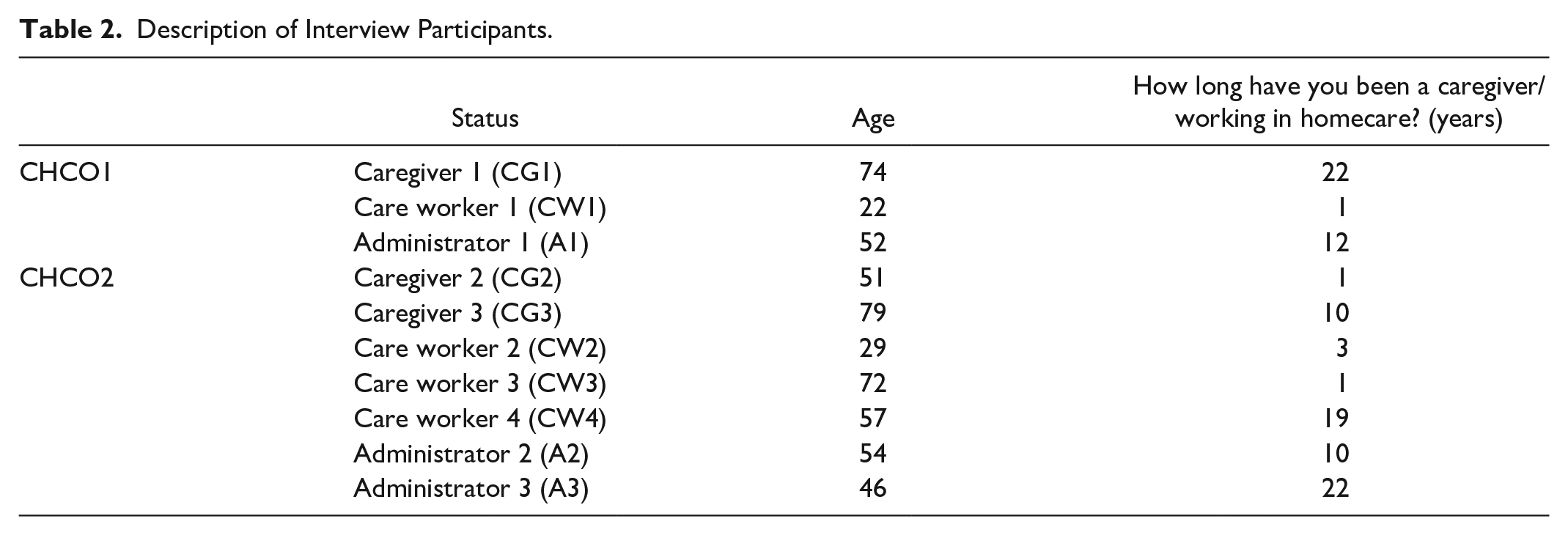
The workshop participants are described in Table 1. In the first CHCO, a student-researcher interviewed 1 caregiver, 1 care worker, and 1 administrator (Table 2). For the second CHCO, 3 care workers, 2 caregivers, 1 administrator, and 1 service coordinator were interviewed (Table 2).
Description of Workshop Participants.
Description of Interview Participants.
Characteristics of ANAAIS-QC
The characteristics of a prospective ANAAIS-QC version can be classified into 3 categories (Table 3): Who is tendering respite; When can it be tendered; and finally, How is it tendered.
Characteristics of ANAAIS-QC.
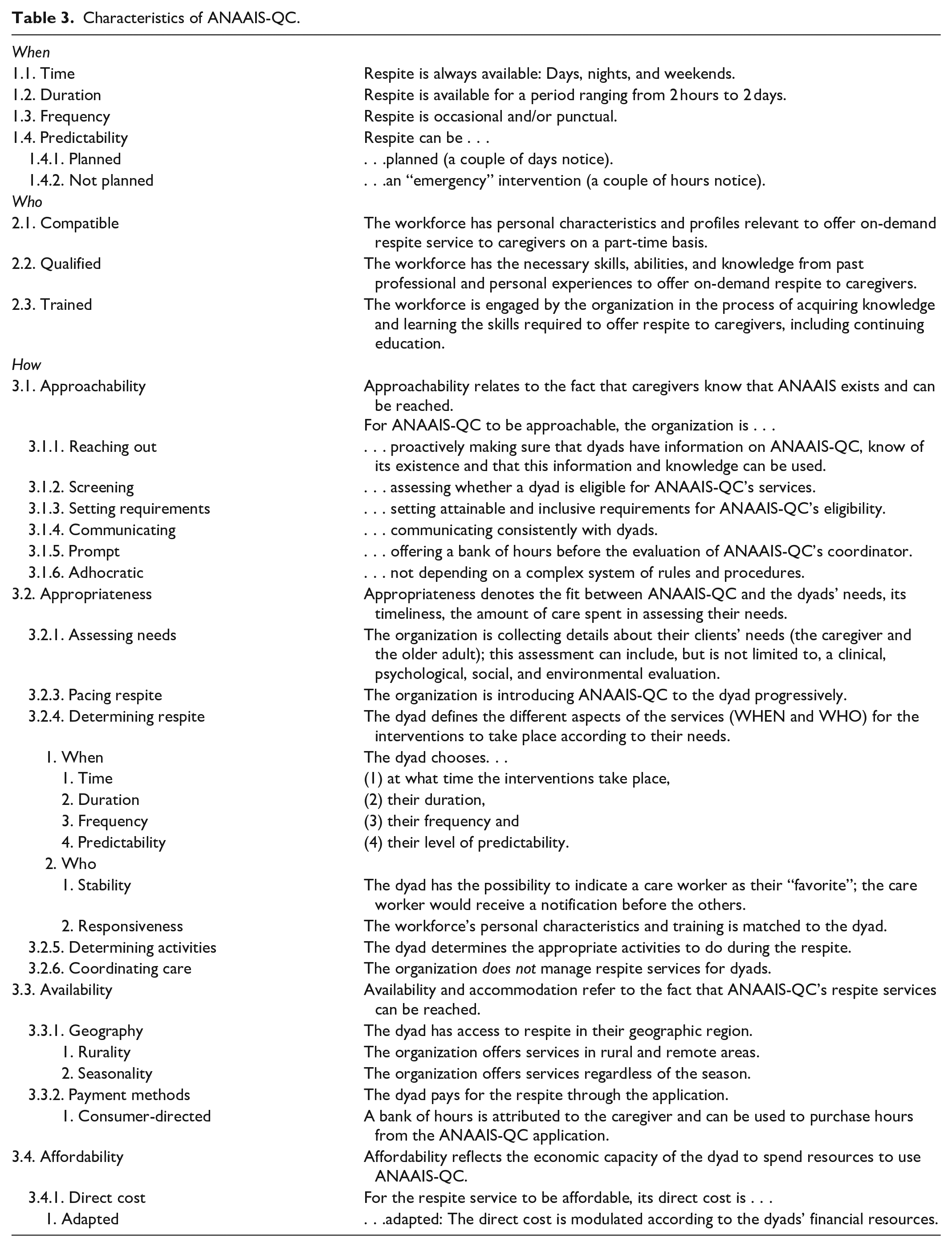
WHO
For ANAAIS-QC, the workforce must be compatible, qualified, and trained. First, care workers would be compatible: This model, where a caregiver can request respite at all times, requires care workers that are comfortable not having a stable schedule and guaranteed hours. As A1 explains, “if you have employees who only work for the application, then it works because they only work part-time, and they only want to work with [ANAAIS].” Second, care workers should be qualified, from professional and personal experiences, for instance, former nurses. Finally, the care workers would be trained by the organization administrating ANAAIS-QC (a CHCO); for example, on neurocognitive disorders.
WHEN
Through ANAAIS-QC, the caregivers would have access to respite at all times, at any frequency, punctually and for different durations. Respite would be available for a period ranging from 2 hours to 2 days. ANAAIS-QC, through its reactive on demand offer, would be specialized in offering punctual respite. As CG1 explained, “punctual requests are important, because even if the schedule is atypical . . . it becomes typical if it’s always the same atypical schedule.” Finally, the respite’s predictability could vary; from days to only a couple hours’ notice.
HOW
As ANAAIS-QC would offer flexible respite, it should be approachable, appropriate, available, and affordable.
First, approachability relates to the fact that caregivers would know that ANAAIS-QC exists and could be reached. The organization would be reaching out, as to proactively ensure that caregivers have information on ANAAIS-QC. As CW2 suggests, a snowball approach could be used: “When a care worker goes to someone’s home for a service, they can talk about [ANAAIS-QC]: ‘Did you know that you can request such and such a service?’” The organization would screen the caregivers to assess if they are eligible for ANAAIS-QC’s services, but with inclusive eligibility criterias. For example, participants explained that, currently, caregivers cannot obtain respite if they are not living with the person supported. Also, the organization would communicate consistently with the caregivers, using instant messaging between the care workers and caregivers and posting care workers’ availability on ANAAIS-QC. As CG1 puts it: “If I know there are possibly 5 people available, then I would be more inclined to ask; not only that, but I will hurry to make sure they are not taken.” The organization should be offering prompt services by setting up an emergency bank of hours available before formal registration. Finally, the organization should be adhocratic; after a coordinator registers the dyad (caregiver and supported person) on ANAAIS-QC, the services would be ready to use with no further bureaucracy needed.
Second, the appropriateness of ANAAIS-QC is denoted by the fit between the respite and the dyads’ needs. To begin, the organization would collect details about the dyads’ needs. The organization would pace the service, introducing ANAAIS-QC as a trial to the dyad to progressively build trust between them and the care workers. The caregiver would then define the different aspects of the service (WHEN and WHO). In addition to indicating a favored care worker, their personal characteristics and training would be matched to the dyad. For example, the presence of animals in the home must be acceptable to the care worker. Finally, the caregiver would determine the activities to do during the respite by leaving a note on their request. For example, a caregiver could suggest going for a walk. A particularity of ANAAIS-QC is that the organization would not manage services; this responsibility is upon the caregivers and the care workers.
Thirdly, ANAAIS-QC should have availability; caregivers could reach services whenever needed and wherever their location. First, services should reach rural and remote areas. As explained by A2: “A person on the border of a county should be able to obtain services from the nearest city. Currently, services are organized around counties, which can cause challenges with emergency respite on large territories.” Also, the organization should offer services year-round; in Québec, caregivers can face service interruption because of the harshness of winter. Lastly, caregivers could pay through ANAAIS-QC using a bank of hours modulated in function of the dyads’ financial resources (affordability). For example, a caregiver could have a bank of 200 hours at the modulated cost of 7 dollars per hours.
Levers and Obstacles to ANAAIS-QC’s Implementation
The participants pinpointed levers and obstacles for ANAAIS-QC’s implementation (Figure 3). These factors were associated with ANAAIS-QC itself (innovation), the CHCO that would be created to administer ANAAIS-QC (inner setting), and the environment in which this organization would operate (outer setting).
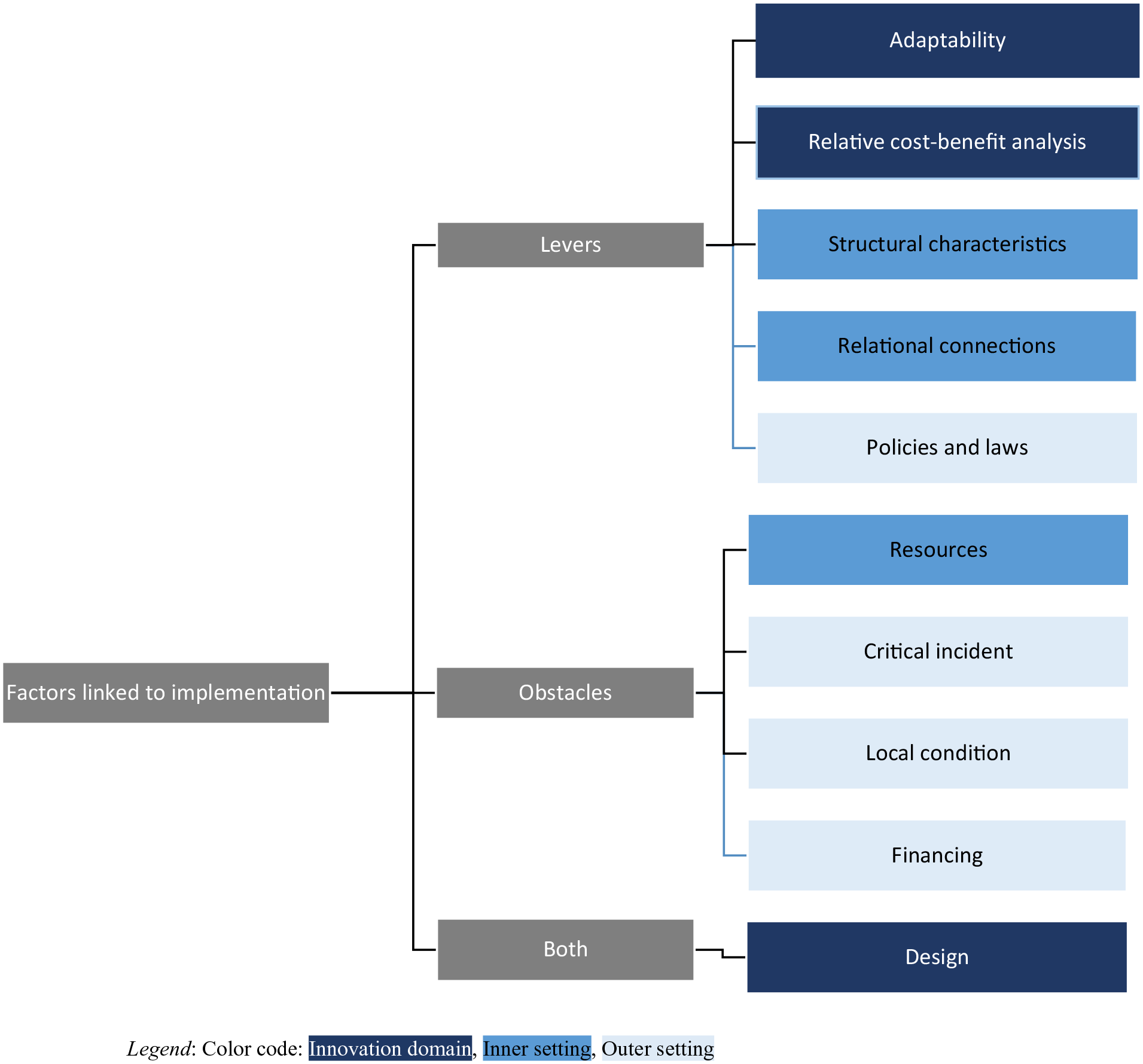
Synthesis of levers and obstacles to consider for the implementation of ANAAIS-QC.
Innovation domain
Participants reported that ANAAIS-QC’s design is both a lever and a barrier to implementation, while its adaptability and relative cost-benefit are levers.
First, design refers to the way in which ANAAIS-QC is packaged, assembled, and presented. The application is user-friendly with its simple color-coded design. As A3 puts it: “For a short time, we are searching around, but quickly, we find our way.” Yet, its use requires a certain level of digital literacy; at least being comfortable using a smartphone or tablet. As A1 explains, “people are ‘in between’: Either people are very much digitally competent, or they don’t want to know anything about it and don’t have the resources.” Participants noted that there are various ways to assist users, such as providing tutorials, establishing a support phone line, and involving family members during ANAAIS-QC’s introduction. That way, people “feel less abandoned to a system” (CG3). ANAAIS-QC’s adaptability would allow it to be customized to the community’s needs and local context. It can also be extended to other on-demand services, as highlighted by CW4: “[ANAAIS-QC] could also offer a relay to care workers in nursing homes, for instance, with time-consuming tasks like managing wandering residents.” Finally, the “relative cost-benefit analysis” made by care workers by dressing the pros and cons of the model indicates that ANAAIS-QC could offer advantages over traditional respite models, giving them more autonomy, as noted by CW3: “The care workers hold power, whereas normally, they do not have a say.”
Inner setting domain
While resources are a barrier to ANAAIS-QC’s implementation, the CHCO’s structural characteristics and relational connections are levers.
Resources available to implement and deliver respite through ANAAIS-QC can influence its implementation. Offering on demand respite requires a considerable pool of available care workers. Addressing the labor shortage in the homecare sector is a top concern, as highlighted by CG2: “The problem: It’s the staff!” Resources are needed to recruit care workers from different sources, including retired or semi-retired professionals willing to provide part-time, on-demand respite.
Structural characteristics of a CHCO encompass both work infrastructure (tasks, responsibilities, and staffing levels) and information technology infrastructure. The organizational features of the CHCO, such as service structure, spare staff capacity, and minimal bureaucracy, would promote flexibility. For instance, being an independent organization allows for unique policies on on-demand respite. As CW1 explained: “We are not allowed to finish at midnight because it falls on another day and causes a system error.” Participants proposed that care workers could have a self-employed status, which liberates them from operational constraints. Lastly, information technology infrastructure would enhance the fluidity of communication and coordination through the ANAAIS-QC application.
Finally, the CHCO’s relationships and connections would allow to optimize resources. For example, partnerships with other community organizations, public health services, and retirement homes can contribute to better knowledge of needs and context.
Outer setting domain
While policies and laws are levers to ANAAIS-QC’s implementation, critical incidents, local conditions, and funding are barriers.
Policies and laws are the legislations, regulations, professional group guidelines, and recommendations around the implementation of ANAAIS-QC. Policies and laws drive the ways in which homecare is funded and managed; “There has to be political pressure put on deputies” (CG2). They also frame the flexibility of services by setting the legal requirements for homecare organization management and professional practices. Orienting policies and laws in favor of flexibility would facilitate implantation.
Critical incidents are large-scale events that would disrupt the implementation and delivery of ANAAIS-QC. For example, A1 reported that during the COVID-19 pandemic, she noticed an overall reduction of participation in services or activities.
Local conditions refer to the different economic, environmental, geographical, political, or technological obstacles in each area. In Québec, winter brings challenges for transportation; caregivers living in more rural areas are sometimes secluded during the winter, because snow removal reaches them later or is insufficient. Also, as CW1 explains, “Some smaller villages barely have mobile phone reception, so there is no mobile phone Internet.”
Finally, financing refers to the funding from external entities available to implement ANAAIS-QC and deliver on demand respite. The lack of established funding mechanisms can be a challenge for this novel models’ implementation.
Discussion
This article aimed to determine the characteristics of a flexible at-home respite model and to document the levers and obstacles to consider for its implementation. Through workshops and interviews, the stakeholders coconstructed a Québec version of ANAAIS; this web application would enable caregivers to easily request affordable respite care, provided by qualified care workers at their preferred time. Successful implementation hinges on various factors, such as the organization’s connections and ability to secure funding.
These results build on existing evidence that flexibility is key in respite services.12,38 -41 Respite requires flexibility in time; caregivers have to be able to request service whenever they want, for the time and duration needed.19,40,42 However, our results show that flexibility goes beyond; it also means obtaining respite from a preferred resource (someone qualified and that they favor) and how they want (easily and quickly). Existing studies point out the challenges related to obtaining respite, such as long wait lists, which can limit flexibility.16,17 Our results emphasize that access (HOW) is a central component of respite flexibility.
Participants highlighted the need for a restructuring of community and public services to enable greater flexibility. This aligns with person-centered care in care culture, policies, and practice guidelines, and reducing bureaucratic barriers.18,43,44 Homecare service financing and the organization of the care worker profession need to be reconsidered. Currently, a significant portion of respite services is outsourced to CHCO by public health institutions, limiting their ability to adapt to caregivers’ needs.45,46 Both the literature and this project’ findings suggested shifting to a bottom-up approach and decentralizing care to give CHCO more autonomy in service provision, as to promote person-centered care.25,26,46 -48 Additionally, as explained by Fox, 43 participants recognized that a self-employed approach, where care workers manage their own schedules, could enhance flexibility.
The project has significant implications. Scientifically, it contributes to the knowledge on enhancing at-home respite services for caregivers through a collaborative coconstruction approach, a rarely explored topic. From a practical perspective, the project may facilitate the rollout of this flexible respite model in the Eastern Townships and foster inter-organizational communication and information sharing. Through key stakeholder partnerships, it identified a solution acceptable to all: An online respite request application. Ultimately, this local initiative could serve as a model for wider adoption in Québec and beyond.
The project has some limitations. First, we cannot exclude the potential influence of the interactional context during workshops. 49 However, the research team made efforts to create a trustful environment during workshops and to ensure non-judgmental exchanges. Although the analysis was reviewed by one of the authors, it was not formally co-coded, which could have limited it’s confirmability. 37 Also, in coherence with the person-centered approach, interviews could have been conducted with people supported by caregivers, despite potential challenges for participants with neurocognitive disorders. Additionally, implementation factors are highly specific to the local context; the participants lived in rural areas, which can explain their concern for physical access. Nevertheless, this research approach can be useful for other researchers or administrators looking to coconstruct, in context, their own service model. 27 The project’s main strength lies in the collaboration and commitment of caregivers and home service providers, providing valuable insights into the region’s issues and ensuring the model’s validity. Their ongoing involvement throughout the project enhanced the rigor of the conclusions. 50
Conclusion
This living lab approach project showed the feasibility and pragmatism of coconstructing a flexible and applicable respite service model. However, future research could shed light on the application’s real-life usability and its capacity to address the care needs of caregivers and older adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Fonds de la recherche du Québec (#309508) – Santé and the Conseil de recherches en sciences humaines du Canada (#892-2019-3075). L’Appui was also an official partner of the research. Annie Carrier and Véronique Provencher are Fonds de recherche du Québec – Santé Junior 1 and Junior 2 researchers (#296437 and #297008, respectively).