
Abstract
Teamwork is considered something positive. While there is much research on teamwork in healthcare, research on teamwork in home care nursing is limited. As the need for home care nursing is likely to increase in the future, it is of great interest to investigate the circumstances associated with the implementation of teamwork in home care nursing. The present study compares the results from a large change initiative intended to foster inter-organizational teamwork between municipal home care nurses and doctors employed by the region, with success factors identified by forerunners and contemporary team theory. Eighteen participants representing the organizations involved in the change initiative, and 6 participants from the forerunners, were interviewed, and 3 success factors were identified: fixed doctors in team, co-location of staff, and a shared team identity. However, for the studied change initiative, few of the success factors were present. Since the success factors are similar to factors associated with effective teamwork in the literature, this is problematic. The results indicate that there was a focus on the division of labor between the municipalities and the region rather than on interdisciplinary cooperation. They also suggest that the change initiative, as it worked in practice, did not always make sense from the perspective of the nurses and doctors involved. Thus, we suggest that measures are taken to ensure that change initiatives, like the 1 studied, also make sense on the local level in the organization where most of the implementation takes place.
Keywords
Introduction
In healthcare, the interest in teamwork has increased in recent years.1,2 Among other things, teamwork is associated with improved patient safety, a better work environment and more effective care.3 -6 In the literature, teams and teamwork is almost always considered to be something positive. 7 While there is a considerable body of research on teamwork in healthcare,3,6,8,9 research on teamwork in home care nursing is a limited research field. 10
As the population grows older and more people are cared for at home for longer periods of time, with more complex comorbidities requiring more advanced care, it is likely that the need for teamwork in home care nursing will increase. 10 While the actual care and technology used can be less advanced than the care provided by health care teams in the hospital, the home care context comes with other challenges. When working in the patients’ home, the home care nurse often works alone. Thus, compared to nurses working in hospitals and primary care centers, they usually lack both colleagues and doctors that they can consult with. Thus, there is a spatial barrier. However, there can also be organizational barriers. In Sweden, for example, the care provided in the patients’ home is provided by several different organizations, with nurses and nurse aides being employed by the municipalities and the doctors by the region. In fact, in Sweden, municipalities are not allowed to employ doctors. Thus, when a home care nurse employed in a municipality needs a doctor for a patient, it requires inter-organizational contacts and collaboration. For this reason, several initiatives to foster this type of collaboration, or as it often called, teamwork, exists in Sweden.
In the present study, we aim to compare the results from a large region-wide implementation intended to foster mobile inter-organizational teamwork between municipal nurses and doctors employed by the region, with success factors identified by forerunners who have already implemented this type of teamwork on a smaller scale and with contemporary team theory.
Theoretical Framework: Organizing for Teamwork
Theory on teamwork identifies several organizational characteristics that could support the process of organizing for effective teamwork. For example, Rydenfält et al. 6 argue that (1) more stable teams, (2) where team members have sufficient opportunities to communicate, and (3) participate in the leadership of the team in an adaptive way, could improve teamwork. In the same vein, Stewart 11 points out the importance of autonomy and increased intra-team coordination for team performance. Rydenfält et al. 6 also states that coordination is a factor that enables effective teamwork and that, in turn, more stable teams and occasions for communication facilitate coordination. Schilling et al. 8 argue that “. . .minimizing pre-existing occupational identities and power-dynamics by emphasizing skill mix, establishing combined workspaces and break areas” (p. 17) is important, and they also highlight the importance of informal opportunities for communication. It has previously been pointed out that group cohesion is a trait associated with effective teams.5,12,13 Hence, de-emphasizing pre-existing occupational identities, as suggested by Schilling, 8 can be a way to move the emphasis in a way that encourages the members to identify with the team instead, thereby fostering cohesion in the team. Thus, there are several organizational characteristics identified in the literature that constitute a viable foundation for teamwork. There are also several traits associated with the work itself that characterizes effective teamwork, for example, group cohesion or identification with the team, coordination within the team and autonomy and team members’ participation in team leadership.
Method
Design
The study followed a single case study logic with a single main case, the region-wide change initiative, and several embedded units of analysis in the form of 4 different participating municipalities. 14 Each municipality was paired with 1 primary care center recommended by the municipalities to consider the conditions from the perspective of the organizations providing the doctors. In addition, using contemporary team theory, we compared the main case with success factors identified by 3 organizations that we considered to be forerunners and an inspiration to the change initiative under study. Data related to the main case consisted of interviews with representatives from municipal home care nursing organizations and regional primary care centers as well as documents describing the region-wide change initiative, including the forms for cooperation between the municipalities and the region. Data related to the forerunners consisted of interviews.
Participants and Data Collection
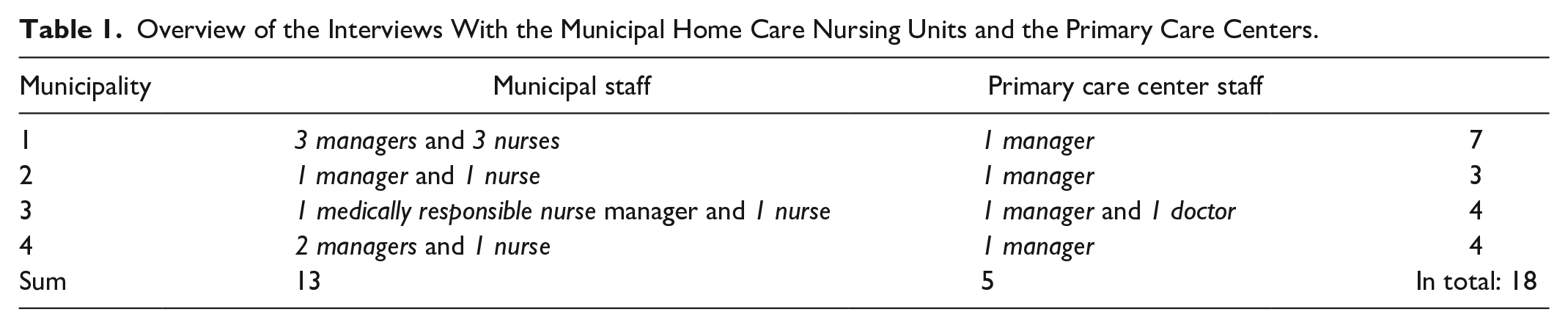
In each participating municipality, we interviewed representatives from the municipal home care nursing unit and the primary care center that they were paired with. All participating primary care centers were considered to have a significant number of patients enrolled in each associated home care nursing unit. As we were interested in the organizational aspects of the change initiative, these interviews mainly targeted participants in management positions. However, we also interviewed a few nurses in the municipalities and a doctor at one of the primary care centers. These participants were recruited upon recommendation from management based on the assumption that they could provide additional information related to the implementation of the studied change initiative. Depending on the opportunities that arose, we conducted both individual and group interviews.
Both interviews with municipal home care nursing units and with primary care centers followed a predefined interview guide. For the municipalities, questions concerned the following topics: the current organization of work, the organization of the mobile team intervention at the moment, how the mobile teams are intended to be developed in the future, which patient groups that are affected by the teamwork, and experiences of how the mobile team intervention actually work in practice, were included.
The interviews with the primary care centers, the questions concerned these topics: the current situation regarding the organization of doctor support in the form of mobile home care nursing teams, how the mobile teams are intended to be developed in the future, which patient groups that are affected by the teamwork, experiences of how the mobile team intervention actually works in practice and expectations for the teams in the future.
An overview of the interviews conducted with the municipal home care nursing units and the primary care centers is found in Table 1.
Overview of the Interviews With the Municipal Home Care Nursing Units and the Primary Care Centers.
We also interviewed representatives from 3 different organizations that could be considered forerunners. In the first forerunner organization, we interviewed 2 managers; in the second, 1 manager, 1 nurse, and 1 doctor; and in the third, a coordinator that was also one of the initiators. In total, we interviewed 6 participants representing the forerunners.
All interviews with home care nursing organizations and primary care centers were audio recorded in combination with notetaking. Afterwards, the research group listened through the recording and either supplemented the notes or transcribed the entire interview. In 2 of the cases, interviews with the forerunners were documented in a similar way with audio recording and notetaking. The third forerunner organization was interviewed over the telephone and documented with notes only. The interviews were conducted between December 2018 and November 2019.
Analysis
All notes and transcripts were imported into QSR Nvivo and analyzed thematically using the process proposed by Braun and Clarke. 15 The first author read through all the data and generated initial codes; then a number of themes were generated from the data. Thereafter, the themes were discussed and reviewed by the first and second author. Lastly, when the first and second author had reached an agreement regarding the themes, the themes, and the description of them were finalized.
Findings
In the following sections, we will first present the findings concerning success factors as seen by the forerunners. We will then proceed and present the main case, that is, the home care nursing units’ and primary care centers’ perceptions of the state of studied mobile inter-organizational teamwork intervention.
The Forerunners and Success Factors
The forerunners encompassed 3 different initiatives concerned with mobile inter-organizational teamwork between municipal nurses and doctors employed by the region. One of the initiatives was implemented in a part of a larger region, covering 15 municipalities with several primary care centers that provided the doctors. One of the initiatives was implemented around 1 hospital and involved teamwork with nearby municipalities. The last initiative was implemented in a larger city and consisted of cooperation between the region and home care nursing staff from the municipality.
The participants emphasized 3 success factors concerned with the organization of mobile inter-organizational teamwork between municipal nurses and doctors employed by the region. The first success factor was to have fixed doctors assigned to the team. The nurses employed by the municipality commonly are the same for the patient over time. However, the forerunners also strived to have as many fixed doctors as possible, that is, they wanted the nurse-doctor team constellation to remain as stable as possible.
The second success factor was to co-locate, to the largest extent possible, the municipal nurses and doctors assigned to the team by the region. In practice, this meant that doctors either had their workplace located together with the nurses from the municipalities or regularly visited the municipality for rounds and consultation.
The third success factor was to foster a shared team identity, that is, that both nurses from the municipality and doctors from the region identified themselves with the same team. One way to do this was to give the inter-organizational team a joint budget; another was to try to create a joint organizational culture.
The Mobile Inter-Organizational Teamwork Initiative in the 4 Municipalities
The implementation process for the region-wide initiative to foster mobile inter-organizational teamwork between municipal nurses and doctors employed by the region was intended to span over several years. When the data was collected, approximately half of the implementation time remained (2 years). The implementation plan emphasized that doctors and nurses from the municipalities should develop common team-based ways of working. There was also an emphasis on team continuity, that is, that the team should consist of the same people over time. A striking and ambitious goal for the initiative was that doctors should be able to conduct emergency visits to patients in their home within 2 hours around the clock. During these emergency visits, the municipal nurse should also be present as part of the team, and the responsibility to provide doctors for these visits was placed on the primary care centers.
In some primary care centers in some of the participating municipalities, there was an ambition to have specific doctors assigned to home care nursing. However, if the assigned doctor was not available, another doctor had to take care of the issue. In other words, there was an ambition to maintain continuity in the nurse–doctor relation. However, it could be difficult to live up to this in practice. None of the municipalities and primary care centers had co-located doctors and nurses assigned to home care nursing. On the contrary, all the forerunners had at least partly co-located doctors and nurses. However, in some cases, there was designated time for home care nursing rounds on a weekly basis. Thus, it is apparent that the prerequisites for the studied municipalities and their associated primary care centers were quite different when compared to the prerequisites for the forerunners.
In the following sections, we will present 3 themes describing how the change was perceived in practice by the organizations: initiative not living up to expectations, divided responsibility, and existing structures the key to success.
Initiative Not Living Up to Expectations
There was a widespread view among the municipal home care nursing organizations that the mobile inter-organizational teamwork initiative did not live up to expectations. Among other things, they did not feel that their expectations on an increased continuity in the relations between municipal nurses and doctors from the region’s primary care centers were fulfilled. It was also acknowledged that being enrolled in the mobile inter-organizational teamwork initiative did not change much in practice for the patients. There was even a fear that the enrollment could result in a decreased access to doctors for the patient. Previously, the home care nurses had the option to call a private mobile doctor service that the region had procured from a private company as a complement. With the implementation of the mobile inter-organizational teamwork initiative, the plan was that this service should be discontinued. However, since there was a fear that the private mobile doctor service would not be available for those enrolled in the mobile inter-organizational teamwork initiative, some doctors were even hesitant to enroll patients at all.
From the municipal home care nursing organization’s perspective, it was also clear that the lack of resources at the primary care centers affected the mobile inter-organizational teamwork in a negative way. The perception was that, at the time of the data collection, it was hard for the primary care centers to provide doctors for patient visits as part of the mobile team during daytime. However, the planning and agreement between municipalities and the region stated that there should be doctors available for home visits as part of the team around the clock, that is, even during nighttime. Thus, there appeared to be a large discrepancy between what was promised and agreed at a higher organizational level and the actual circumstances under which the work was performed in practice. Also, the primary care centers highlighted that they believed that the region would have to keep the private mobile doctor service in order to be able to provide support to the municipalities’ home care nursing organizations. It was also stated by the primary care centers that they did not feel that the region had provided them with the resources required to fulfill their part of the agreement. In 2 of the municipalities, the region had, in the months prior to the data collection, implemented a hospital-based mobile backup team consisting of a doctor and a nurse. When the primary care centers did not have available doctors, they could then choose to route the errand to the backup team. However, where no such team was available, the responsibility to provide doctors lay solely on the primary care centers.
Divided Responsibility
The primary care centers were clear with the fact that the responsibility to provide personnel for the mobile team up to the level of registered nurse lay with the municipality. The region’s responsibility was to provide doctors. However, at the same time, it was stated by one of the municipalities that the responsibility for the mobile team in fact lay with the region and the primary care center. For one thing, the doctors at the primary care center had the power to decide which patients to enroll in the mobile team; they also had the final say regarding whether there was, in fact, going to be a home visit for a patient when the nurse from the municipality asked for it. It was also the case that much of the preparation work related to the enrollment of patients was conducted by the nurse from the municipality. Thus, there did not seem to be someone taking overall responsibility for the mobile team.
Existing Structures the Key to Success
The municipalities highlighted the importance of having 1 dedicated doctor at the primary care center that worked with the nurses from the municipality. In 2 of the municipalities, they stated that they had that kind of relation to some of the primary care centers they worked with. However, it was also stated that this was nothing new that had been introduced as part of the mobile inter-organizational teamwork initiative. Rather, it was something that had been going on for years and something that the municipality together with the specific primary care center, had organized themselves, that is, when the mobile inter-organizational teamwork initiative worked well, it could be attributed to existing relations and structures, rather than due to changes imposed from above on municipal home care nursing or the primary care centers.
Discussion
While the ambition with the region-wide initiative to foster mobile inter-organizational teamwork between municipal nurses and doctors employed by the region was on level with the studied forerunners, or even more ambitious given that it implied that doctors should be available for home visits around the clock, it was clear that those ambitions were not met. To fix the intervention, the region introduced a backup team available to some of the municipalities. While this type of action increases the access to doctors for home care nursing, it also deceases team stability from the perspective of the home care nurse. 6 The backup team comes with a doctor, but it is not the patients’ ordinary doctor, and it could be a different doctor every time. Compared to the forerunners, few of the success factors identified above were in place. Furthermore, since the perception was that there was a strict division of responsibility for the work related to the mobile teams, the personnel from home care nursing and the primary care centers did not see the team as a joint organizational entity with which they identified themselves. While this perceived division of responsibility was probably in part a symptom of the lack of resources experienced by the primary care centers, it is also something that could stand in the way of a pure joint commitment to the idea of creating interprofessional teams involving personnel from both organizations.
While the forerunners seem to have aimed for what often is called interdisciplinary teamwork, that is “. . .a team whose members work together closely and communicate frequently to optimize care. . .” 16 (p. 868), the studied organization in the municipalities appeared to aim at multidisciplinary teamwork. With multidisciplinary teamwork, we mean that the team members work more or less independently with the provision of care for the patient from their own professional point of view. 16 Compared to interdisciplinary teamwork, multidisciplinary teamwork allows for an emphasis on the division of labor and responsibility between different actors in the team.
Furthermore, the ways of work studied could also be considered inter-organizational teamwork since it involves 2 different organizations. 17 In inter-organizational teams, too strong an identification with the home organization is suggested as something that could be problematic. It has also been suggested, in line with the team theory presented above, and the forerunners’ organization of work, that the co-location of personnel from organizations involved in an inter-organizational team could help foster identification with the team.6,8,17
To sum up, the constraints that the prerequisites for work put on the ability to implement the mobile inter-organizational teams resulted in an organization of work that emphasized function and the division of labor in the team rather than the establishment of effective work relations within the team. This is unfortunate since the process of becoming an effective team involves the establishment of relations and agreement regarding effective ways of working. 18
It could be beneficial to lift the gaze from the team itself and the actual ways of working described by the participants, and scrutinize the region-wide initiative to foster mobile inter-organizational teamwork between municipal nurses and doctors employed by the region from a change management perspective.19,20 When doing so, it is also important to acknowledge that it is not a change initiative that affects only 1 organization; rather, it is a change initiative involving several organizations of 2 different types, each with different priorities and responsibilities. Traditional change models, for example, those by Lewin 21 or Kotter, 22 emphasize the importance of a sense of urgency or events that clearly motivate organizational change. However, with more than 1 organization involved, it is probably much harder to rally around a joint motivation for change. While the mobile interprofessional teams make sense on the healthcare system level, our results indicate that their implementation is not perceived as very urgent on the level of the local organizations involved in the team, and it could be argued that the gains for the organizations are quite limited on the local level, especially for the primary care centers. Hence, the gains are expected to emerge elsewhere, that is, in the form of less pressure on the hospitals and the emergency departments. Thus, there seems to be a framing problem, both when it comes to the actual inter-organizational mobile teams and the organizational change initiative that should establish them as a way of working. Given the current framing, they simply do not appear to make enough sense in light of the different organizations priorities and perceptions of purpose. As pointed out by Tsoukas and Chia 23 “Organizational categories and rules are constantly adjusted, modified, or even ignored in the carrying out of actual organizational tasks” (p. 577). In other words, the perceived tasks of the organization take precedence and might not always involve inter-organizational teams together with municipal home care nursing.
Conclusion
The studied change initiative did not work as intended, and the commitment to it differed between the participating organizations. The lack of perceived benefits for the patients appears to have decreased the doctors’ commitment. The prerequisites for the studied change initiative were quite different from the forerunners; consequently, it appears to have been hard to achieve the organizational characteristics identified as success factors by the forerunners. The focus on function and division of labor could be a consequence of a lack of resources, that is, a way for the organizations to protect their resources. While the change initiative makes sense on the system level, it is unclear whether it really made sense on the local level. Together with a lack of resources, this could be a possible explanation for the apparent shallow interest in committing to it. In future initiatives intended to result in inter-organizational teamwork, we suggest that more emphasis be placed on the actual organizational prerequisites for teamwork to ensure team stability. Moreover, there should be opportunities for communication within the team, and occupational and organizational identities should be downplayed to make room for a team identity. We also suggest that measures are taken to ensure that the new ways of working also make sense on the local level in the organization where most of the implementation takes place.
Footnotes
Acknowledgements
The authors would like to thank AFA Insurance (Grant DNR: 170278) for financing the research project in which this research has been carried out.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was funded by AFA Insurance (Grant DNR: 170278) for financing the research project in which this research has been carried out.