
Abstract
Patient Support Programs (PSPs) reinforce patients’ care provided by health care professionals with the aim to improve adherence and patient empowerment. PSPs may include interventions such as home-based care, individualized medication counseling, support, training, and home delivery of medicines and/or devices. This study described these services and its impact on patient-reported outcomes and health care savings. We conducted an integrative literature review which was limited to publications from the last 10 years (2009-2019) and focused on diseases that require special support and/or parenteral administration. From 7040 total citations, we identified 64 home-based care services performed worldwide. Among the home-based care services, most were provided by nurses (n = 47/64; 73.4%) and addressed to cancer patients (n = 22/64; 34.4%); 23 out of 64 services (35.9%) incorporated telepharmacy. In general, home-based services and PSPs showed a positive impact on patients’ adherence to medication, patient satisfaction, and health-related quality of life. In addition, 14 (21.9%) services reported economic results, most of which showed that home therapy led to substantial cost savings.
Keywords
Introduction
The world population reached 7.7 billion in mid-2019 and is expected to increase to 8.5 billion in 2030. 1 By then, the percentage of people aged 60 years and older will increase by 34%, from 1 billion in 2019 2 to 1.4 billion. Some conditions are more prevalent among the elderly, such as chronic diseases, frailty, mental disorders, and physical disability; these conditions impose a substantial care burden on hospitals and primary care centers, 3 as they require complex disease-specific management. 4 Additionally, older patients often experience mobility difficulties that affect their physical and functional status and hinder their access to inpatient care; consequently, they may benefit from home-based care services. 5
Patients with cancer 6 or progressive diseases 7 may also require additional support. They have unmet needs that negatively affect their well-being and health-related quality of life (HRQoL), including learning about their disease and treatment, acquiring coping skills, 8 assistance with daily living activities, and psychological support. 6 In addition, patients with chronic diseases frequently require multiple, long-term medications to prevent disease progression. However, their adherence to medication is poor, leading to treatment failure and an increase in economic and societal disease burden.9,10 In this regard, some strategies that include home-based care have demonstrated a substantial improvement in medication adherence 11 in addition to patients’ HRQoL. 12
The World Health Organization (WHO) 13 defines home-based care as “any form of care given to ill people in their homes, including physical, psychosocial and palliative activities.” Home-based care may cover everything from 24-hour support to periodic assistance with relatively simple tasks such as domestic aid for frail older adults and adults with a disability 14 or post-discharge care. 15 The provision of services at patients’ homes can be more cost-effective than institutional care, mainly if the available home health care is used effectively. 5
More recently, patient support programs (PSPs) have emerged as patient assistance programs that include interventions -such as individualized medication counseling, training support, or virtual reminders, among others- to improve patients’ HRQoL, help them manage their disease and complex medication regimens, improve medication adherence and reduce complications and related costs. 16 Previous studies have shown that PSPs increase patients’ adherence, especially when they combine different interventions, such as home-based care with educational programs. 17
Despite the rapid increase in the number of home-based care and PSPs initiatives, the evidence available so far has some limitations. The first limitation is that prior studies were restricted to specific populations (e.g., patients with a particular disease18-20 or frail patients) and locations (e.g., in certain countries21,22). Therefore, they cannot be generalized to other settings. For example, results in the U.S. context cannot be extrapolated to European settings due to a significant difference between the 2 in terms of their health systems, financial resources, and co-payment systems. Therefore, the second limitation is related to the lack of understanding of the home-based care impact on clinical, adherence, humanistic, and economic outcomes.
To fill these limitations, we designed this integrative review aimed to gather and summarize publications about home care services or home delivery systems initiatives conducted worldwide and focused on certain chronic or rare conditions that might require complex management and additional support. Whereas the specific objectives were: (1) to outline the characteristics of the home care services or home delivery systems collected; (2) to describe the effect of the home care services or home delivery systems on adherence to medication, humanistic (patient-reported outcomes [PROs]), and economic outcomes.
Methods
Study Design and Data Sources
We conducted a targeted integrative literature review following the “Preferred Reporting Items for Systematic Reviews and Meta-analysis: The PRISMA Statement” guidelines (Supplemental Table 1). 23 For this purpose, we used international databases (Medline/PubMed, Web of Science [WoS], SCOPUS) and Spanish national databases (Medicina en Español [MEDES], Índice Bibliográfico Español en Ciencias de la Salud [IBECS]) and a broad search in the gray literature. The search was limited to original research articles, reviews, meta-analyses, and guidelines published between 2009 and 2019, in English or Spanish, focusing on home care initiatives of specific drugs or medical devices and in patients with: multiple sclerosis, human immunodeficiency virus (HIV) infection, cystic fibrosis, diabetes mellitus, rare diseases, Parkinson’s disease, cancer, pulmonary arterial hypertension, rheumatoid arthritis, psoriasis and psoriatic arthritis, inflammatory bowel diseases (IBD), and blood coagulation disorders or patients that require parenteral administration (including parenteral nutrition and parenteral administration of treatment through medical devices such as pumps).
Search Strategy and Search Terms
Our search strategy combined the terms for home care services with those related to the diseases. We used a similar search strategy for all of the databases consulted: Pubmed/Medline, WoS, SCOPUS, Cochrane Library, IBECS, and MEDES, adapting the search terms to the requirements of each one. See Supplemental Tables 2 and 3 for more details about the terms and the search strategy.
Search of the Gray Literature
We carried out a search of the gray literature using the advanced search capabilities of the search engines Google Scholar and Google (Supplemental Table 4). The search strategy included terms in English and in Spanish such as “home care initiative,” “home nursing,” “medicine home delivery,” and “telepharmacy”. Additionally, we performed a manual search of the reference lists of relevant articles. We reviewed the websites and press releases of major pharmaceutical companies for additional publications meeting the inclusion criteria.
Data Abstraction
Two researchers independently screened each of the identified publications based on titles, abstracts, and full texts for inclusion criteria. Any discrepancies between reviewers were resolved through consensus and, if necessary, by consulting a third reviewer.
Table 1 shows the inclusion criteria following the PICOS (population, intervention, comparator, outcomes, and study design) definition.
Eligibility Criteria Defined by PICOS.
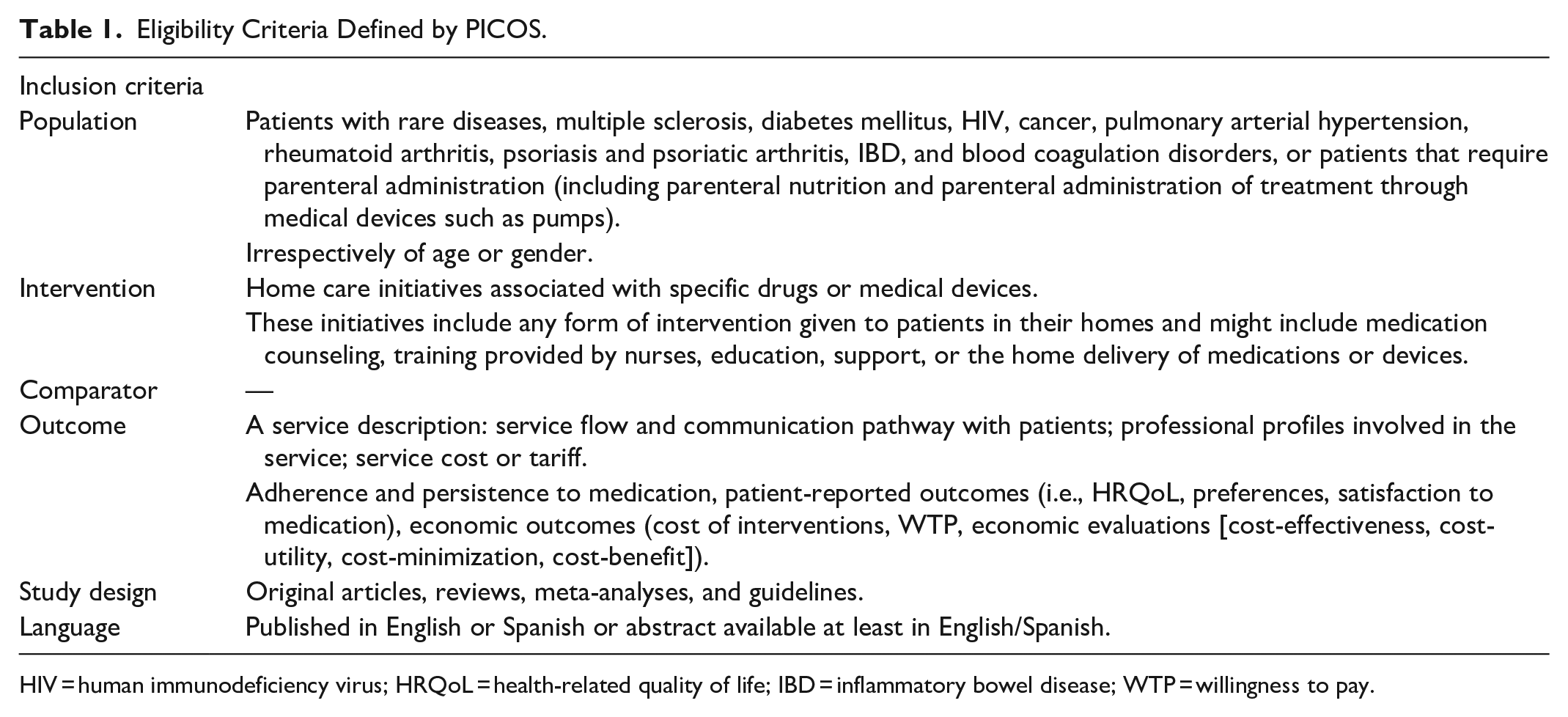
HIV = human immunodeficiency virus; HRQoL = health-related quality of life; IBD = inflammatory bowel disease; WTP = willingness to pay.
From the final included articles, the following variables -used to describe home care initiatives- were extracted: the region (country) where the initiative was implemented; the study design (e.g., observational study or clinical trial); the pathology for which the initiative was implemented; the route of administration of the medication (e.g., parenteral, inhaled, or oral administration); the type of home service included (e.g., telepharmacy, home delivery, or home nurse service); the sponsor of the initiative (pharmaceutical company, health services, or health care company), and the outcomes measured to evaluate the intervention if any (e.g., adherence and persistence, PROs [HRQoL, satisfaction, preferences] and/or economic outcomes). To compare the economic results between them, all the costs were converted into Spanish euros (2020) using the CCEMG-EPPI centre Cost Converter tool. 24 We examined the evidence based on the designs of included studies: a randomized clinical trial (RCT) or a systematic review of RCT methodology were considered the highest quality. Quasi-experimental, prospective observational cohort studies were deemed as medium quality; retrospective, cross-sectional, and other designs (i.e., case series) studies as lower quality.
Results
We first identified a total of 7040 studies: most of them (n = 7037) were from international (Medline/PubMed, Cochrane Library, WoS, and SCOPUS) and Spanish databases (IBECS and MEDES), and 3 studies were from sources identified via Google Scholar advanced and Google advanced search. Of these, a total of 3775 remained after removing duplicates, of which 3636 were excluded as they did not provide relevant information for the purposes of the review. Next, we assessed 139 full-text articles for eligibility (Figure 1) and identified 54 publications that discussed 47 home care services or home delivery systems (Table 2). Also, we identified a further 17 care services or home delivery systems using company websites or press releases (Table 3).
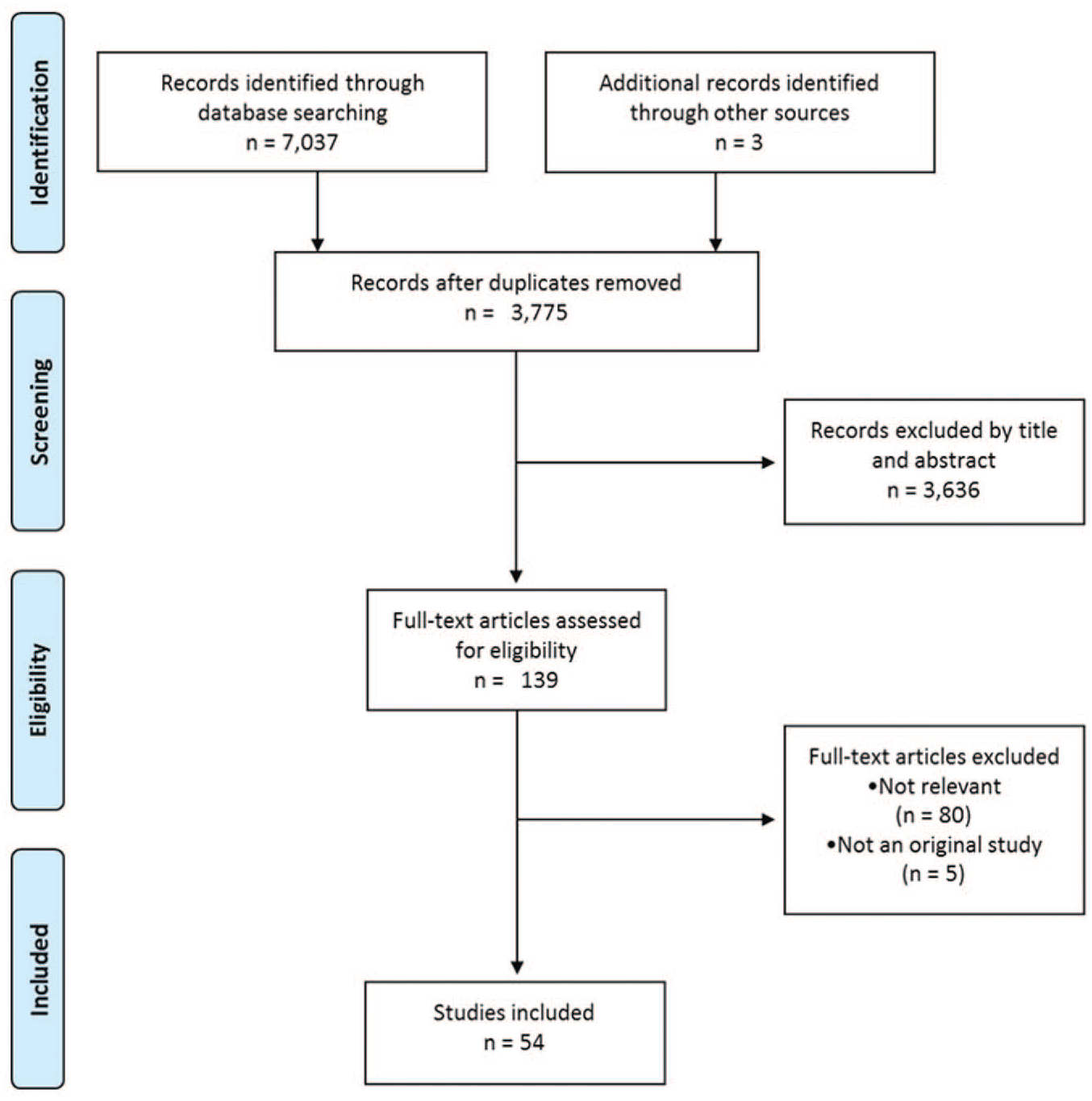
PRISMA flow diagram.
Summary of the Identified Home Services.

HRQoL = Health-related Quality of Life; IBD = Inflammatory Bowel Disease; NHS = National Health Service; OPAT = Outpatient Parenteral Antimicrobial Therapy; PSP = patient support program; NA = not available; UK = United Kingdom; VAD = Vascular Access Device.
Summary of the Home Services Identified in the Gray Literature.
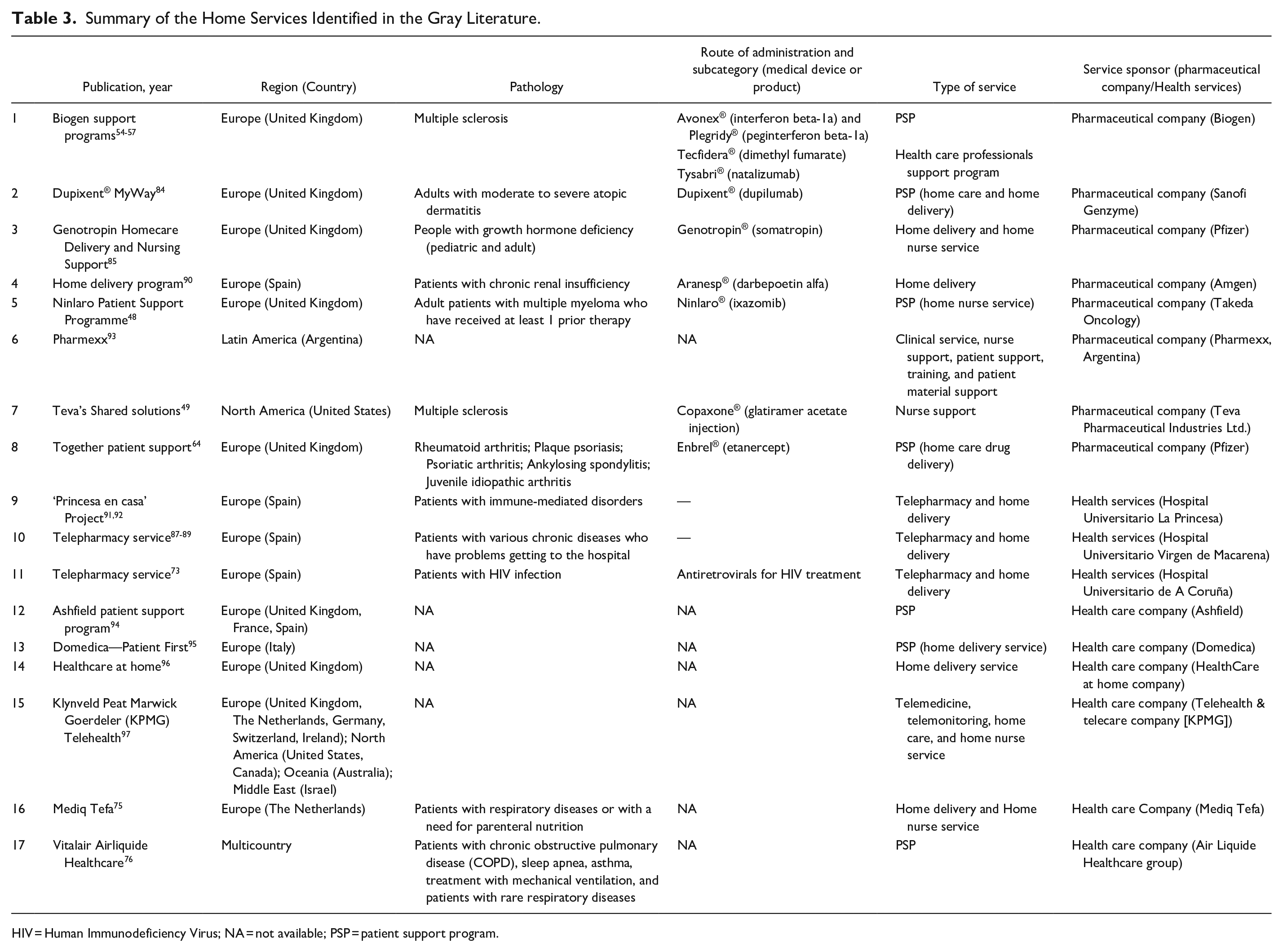
HIV = Human Immunodeficiency Virus; NA = not available; PSP = patient support program.
Characteristics of Published Home Care Services or Home Delivery Systems
In total, we identified 64 home-based care initiatives carried out in various parts of the world. Tables 2 and 3 show the composition of home care initiatives. In short, most home services were implemented in Europe and North America (n = 58; 90.6%), while initiatives in other parts of the world were particularly scarce. Most services involved health care professionals, in most cases nurses (n = 47; 73.4%). More than one-third of home services involved telepharmacy and home delivery of medicines (n = 23; 35.9%). Around 40% of the interventions (n = 26; 40.6%) were directly linked to a specific medicine or medical device. Of the 54 studies identified: three (5.6%) had the highest quality design, whereas 24 (44.4%) and 27 (50.0%) had the medium and lower-quality designs, respectively.
Home care initiatives addressed a wide variety of diseases:
- Cancer (n = 22; 34.4%): Twelve (54.5%) home care services were designed for patients with solid tumors,25-38 while the rest (n = 10; 45.5%) were aimed at patients with lymphoproliferative disorders (leukemia, multiple myeloma, and lymphoma).39-48
- Multiple sclerosis (n = 7; 10.9%),8,21,49-57 5 (71.4%) home care initiatives were aimed at the home administration and monitoring of multiple sclerosis therapies.8,21,51-54
- Rheumatoid arthritis, IBD, and psoriasis (n = 5; 7.8%): two (40%) home care initiatives that supported home-based infusions of biological agents in adult patients with Crohn’s disease.58,59 A further, 2 (40%) PSPs were aimed at adult patients with adalimumab-approved indications.18,60-63 Additionally, a PSP (20%) based on home drug delivery was indicated for patients with rheumatoid arthritis, psoriatic plaques, psoriatic arthritis, ankylosing spondylitis, and/or juvenile idiopathic arthritis. 64
- Rare diseases (n = 4; 6.3%): The identified home care services were based on the management of patients with hereditary angioedema, 65 cystic fibrosis, 66 Fabry disease, 67 and idiopathic pulmonary fibrosis. 68
- Diabetes mellitus (n = 3; 4.7%): two (66.7%) home care initiatives consisted of PSPs aimed at diabetes mellitus patients who were starting insulin treatment.69-71 One home care service was aimed at the telemonitoring and home-based nursing management of patients with diabetes and other chronic diseases (heart failure, chronic obstructive pulmonary disease, and hypertension). 72
- HIV infection (n = 2; 3.1%): These home care services73,74 were aimed at the home delivery of antiretroviral drugs.
- Respiratory diseases (n = 2; 3.1%): one (50%) home care initiative was aimed at patients with respiratory diseases with a need for parenteral nutrition. 75 The other (50%) was a PSP aimed at patients with different respiratory diseases (such as chronic obstructive pulmonary disease [COPD] or asthma) under treatment with mechanical ventilation. 76
- Other pathologies with parenteral administration (through medical devices like pumps) (n = 8; 12.5%): These home care services were aimed at the parenteral administration of various therapies through infusion pumps.20,77-83 Six (75.0%) home care initiatives were developed to enable the administration of parenteral antimicrobial therapy at home.20,79-83
- Other pathologies were associated with a single intervention or associated home care service (all of them are listed in Tables 2 and 3), such as dermatitis, 84 growth hormone deficiency, 85 blood clotting diseases, 86 various chronic diseases that lead to problems getting to the hospital,87-89 chronic renal insufficiency, 90 or immune-mediated disorders.91,92 Five (7.8%) home care services were not aimed at a specific disease; they were based on nursing support or home delivery programs.93-97
Effect of Home Care Services or Home Delivery Systems on Adherence to Medication, Humanistic (Patient-Reported Outcomes), and Economic Outcomes
Of the 64 initiatives identified, 31 (48.4%) had studies that evaluated their impact on treatment adherence, in addition to humanistic (PROs such us satisfaction, HRQoL, and preferences) and economic outcomes.
Adherence and persistence
Of the 31 home-based care services for which studies were assessing the impact of the initiatives, 9 (29.0%) focused on the effects of home care services on medication adherence and persistence.18,26,51-53,59,60,63,67,69,70 Most were aimed at addressing the impact of PSPs on adherence to and persistence with a specific medication.
Six (66.7%) studies showed significant improvements associated with the intervention on the adherence and/or persistence rates for medication for diabetes mellitus,69,70 IBD, 59 and psoriasis, psoriatic arthritis, and rheumatic arthritis.18,60,63 For multiple sclerosis, 3 (33.3%) studies reported improved adherence to a medication through the use of a self-injector device, but further studies are needed to corroborate the findings.51-53
Patient-reported outcomes
HRQoL
Eight studies (25.8%) aimed at evaluating the impact of home care interventions on HRQoL.26,31,37,43,46,47,74,78 The questionnaires used to assess HRQoL were generic: the EuroQol 5-Dimensional Scale (EQ-5D) or the Short Form-36 Health Survey (SF-36);26,31,78 disease-specific -the Lung Cancer Symptom Scale (LCSS)-26,37,46 and the Mini International Neuropsychiatric Interview (MINI); 74 not specified 47 , and an ad hoc questionnaire adapted from a previous study. 43 The majority demonstrated how the interventions improved HRQoL, however, 3 (37.5%) of them showed that patients’ HRQoL remained unchanged, regardless of whether the patient was at home or with the standard of care.26,37,78
Preferences
Two studies -one aimed at breast cancer patients and the other at children with infection- included the assessment of preferences regarding home services. Preferences were evaluated using ad hoc questionnaires. In both studies, patients and caregivers reported a preference for the home administration of treatment over administration in other settings.30,83
Satisfaction
Sixteen studies (51.6%) rated patients’ levels of satisfaction with the interventions.8,21,25,26,28,32,34,38,43,58,62,68,72,74,78,86 In general, these studies used an ad hoc approach to measure satisfaction. Only Van den Bosch et al, 62 applied the Treatment Satisfaction Questionnaire for Medication (TSQM) to assess patient satisfaction.
Most of the services assessed involved nurse-led programs (n = 11; 68.8%),8,21,25,26,28,32,34,38,43,58,62,72 and home medication delivery (n = 5; 31.2%).25,26,28,62,74,86
Patients with various pathologies expressed their satisfaction with the interventions. Specifically, patients with multiple sclerosis indicated a very high level of satisfaction with home treatment,8,21 and 98% decided to receive future infusions at home. 21 Oncologic patients also expressed very high levels of satisfaction with home-based chemotherapy provided by nurses.25,28,32 Several interventions were linked to a specific product, such as pemetrexed,25,26 zoledronic acid, 32 or bortezomib. 43 Likewise, patients with diabetes mellitus, 72 HIV infection, 74 or hemophilia 86 were satisfied with these interventions.
The most common reasons for satisfaction were: personalized care,25,26 the absence of difficulties with transport to the hospital,25,32,43,86 no waiting for treatment,26,32,43 and increased well-being, 43 among others.
Economic outcomes
Of the 31 home-based care services for which there were studies assessing the impact of the initiatives, 14 (45.2%) focused on the effects on their economic costs of these services.18,20,21,39,41,43,47,54,58-60,74,80,83,86
Cost evaluations were usually from the perspective of the company or the health care entity and included direct medical costs. Among these studies, 8 (57.1%) showed that home therapy led to substantial health care cost savings in comparison to the administration of therapy in the infusion clinic. Savings ranged from €47.7 to €9,146.8 per service. Below, we sum up the results of the different studies according to the different diseases:
- Multiple sclerosis: the total cost of home administration was €306,293.9, and the cost savings per treatment with methylprednisolone were €1,215.4 when administered at home. 21
- Multiple myeloma: a combined outpatient and bortezomib home administration yielded €162 cost reduction compared with the model of daily hospital care. 41 Another study compared the total cost of bortezomib injections on an outpatient basis to the administration at home, with home administration being more cost-effective (€1,292.9 vs €1,048.2). 43
- Leukemia: the analysis demonstrated home care-associated savings of €1,925.7/cycle of azacitidine and €9,146.8 per patient. 47
- Crohn’s disease: median total health care cost per patient with nursing assistance was lower compared to the non-assistance group (€27,344.7 vs €29,693.7). 59 Another study also highlighted that administering infliximab at home (€198.6) was more cost-effective than administration at the clinic (€246.3). 58
- Patients with infections that require parenteral administration of antibiotics 20 : the average cost of outpatient parenteral antimicrobial therapy (OPAT) administered at home versus the cost of an in-patient bed for medical patients was €99.5/day versus €379.1/day. 20
- Rheumatoid arthritis, IBD, and psoriasis: two studies showed that the mean costs associated with patients included in the PSPs were lower compared with those for non-PSP patients. The associated medical cost was 22% lower for patients in the PSP than for those not in the PSP (€5,466 vs €6,969.65, p = .045), and the total cost was also 10% lower (€24,417 vs €27,130.5, p = .030). 60 Brixner et al 18 also found reduced costs when comparing PSP and non-PSP patients; savings were associated with medical expenses (€6,670.6 vs €10,181.4, p = .005) and total costs (€40,974.8 vs €45,100.5, p = .056).
Discussion
This integrative literature review is, to the best of our knowledge, the first attempt to describe the characteristics of home-based care initiatives, as well as their humanistic and economic impact, without limiting the type of intervention (PSP, nursing support service, medication delivery, etc.), or the region involved. In this review, we focused on the pathologies that could benefit the most from PSPs or home-based services as they may be associated with restricted mobility, disability, pain, or long-term, complex or intravenous treatment regimes.
Many home-based interventions were aimed at supporting patients with cancer -either solid tumors or lymphoproliferative diseases- during treatment. This is not surprising considering that these patients often need complex long-term treatments that require close monitoring. Home administration of chemotherapy has demonstrated to be a safe and cost-effective alternative that provides patients with some advantages over in-patient administration: it allows for more significant family support. It helps patients to better balance their lives with treatment by avoiding admission or traveling to the hospital.21,25,26,28,30,32,40,43,47,54,78 Nurses led most of the home administration services with specific training in the different pathologies and extensive experience in the home administration of intravenous treatment.21,31 Nurses were mainly responsible for administering the medication at home or teaching patients how to self-administer it, as well as monitoring symptoms and adverse events related to the medication.
Some home care initiatives, such as PSPs, may contribute to increased patient adherence to or persistence with specific therapies. Home visits, particularly in association with educational components, seem to have a positive impact on patients’ medication adherence.18,50,59,60,63,68-70 Previous studies corroborate the idea that PSPs yield beneficial results in terms of adherence and persistence,16,98 and patients’ education was the key to improve their adherence to medication. 16 One possible explanation is that patients who enroll in a PSP are more aware of their disease and treatment. 99 The services included in the PSPs vary among studies. They include training on the home administration of treatments, education on illnesses and treatments, and reminders to take medication, which can affect adherence in different ways.
In general, home-based services had a positive impact on humanistic outcomes such as HRQoL, which is a good indicator of their success. Home-based interventions improved patients’ knowledge of treatment and disease and increased their sense of control and confidence.Some studies showed that HRQoL was unchanged when comparing home interventions with hospital care. The reasons for the lack of improvement may, for example, be due to low sensitivity for detecting HRQoL changes in a short time, low specificity to the target diseases, or that the timing was not controlled as patients self-completed the survey at home. Nevertheless, these results can be considered a positive outcome, as they indicate that treating the patient at home, rather than in the hospital, does not worsen their HRQoL.26,37,78 Furthermore, when asked, patients expressed a preference for treatment at home over treatment in other settings.25,26,74,78
Similarly, most of the patients were highly satisfied with the home services evaluated. Reasons for satisfaction included: no exhaustion from traveling to or waiting in the hospital, less disruption to their daily routine, and greater family support.25,26,32,43,86 These results are in line with those obtained by Martinez-Sesmero, 100 in which the implementation of a PSP for immune-mediated chronic diseases produced high degrees of satisfaction among patients and health care professionals.
Most of the studies showed that home therapy led to substantial health care cost savings when compared to the administration of therapy in the infusion clinic.18,20,21,41,43,47,58,59 Besides, the medical costs associated with patients included in PSPs were lower than those for non-PSP patients. Health care cost savings were mainly associated with a significant decrease in disease-related medical costs, more specifically, with a reduction in hospital admissions18,59 and all-cause emergency department costs. 18 PSPs are thought to be cost-saving strategies that also increase the effectiveness of health interventions; this may be mainly attributable to higher treatment adherence. 101 These findings are supported by other studies in which home-based programs led to a reduction in health care costs. 102
One of the keys to the programs’ success is that patients find them useful, convenient, and that they somehow improve their lives or make them more accessible. Future plans should, therefore, focus on making them more attractive to users. The digitalization of PSP interventions through apps or websites will permit a more personalized and adaptable experience for each type of patient. However, the implementation of home-based care initiatives is not without complications. In Europe, public home-based services regulation and legislation vary widely from country to country, whereas private home-based initiatives are poorly regulated compared to the public sector. This results in great inequalities in the degree of implementation of these initiatives, especially those sponsored by private providers. 14 The regulation of mail-order or home delivery of medicines is also heterogeneous across countries; but, in general, online sales are only permitted for over-the-counter medication, though there are some exceptions, such as The Netherlands and Brazil.103,104
In recent months, the importance of home-based care and delivery services has increased substantially due to the outbreak of the crisis caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Home-based services could play an essential role in reducing contact between individuals and in preventing them from making unnecessary visits to the hospital or the pharmacy, driving telehealth care to grow exponentially. At the same time, home services may allow hospitals and clinics to reduce the number of non-essential health care workers on-site, where they are at high risk of infection. This new scenario makes it urgent to improve and standardize the current regulation of home-based services to facilitate their proper implementation.
Limitations
An integrative review examines and synthesizes the information on a subject that is available in the literature, and, therefore, has some associated publication bias. Not all existing databases have been searched, leading to the omission of some critical databases, such as Embase. The study’s inclusion criteria are limited to English/Spanish publications, which may result in the omission of home interventions discussed in other languages. Also, most of the studies that evaluate home care interventions do not include control arms, so no conclusion may be drawn about whether these interventions were more effective than the standard of care.
Many studies do not provide sufficient detail to understand the quality of the interventions. For instance, PROs and economic outcomes are assessed in several studies. However, the extrapolation of these findings to the general population may be risky due to the variability of the people, interventions, and settings involved. It should also be noted that PROs themselves are inherently biased. Thus, this approach may limit the accuracy and validity of the results presented.
Conclusions
In this review, we have synthesized recent evidence on home care initiatives, with a great variety of services, target populations, and locations. However, despite their heterogeneity, in general, home-based services and PSPs showed a positive impact on patients’ adherence to medication, patient satisfaction, and HRQoL. Additionally, some of the evaluations demonstrate that home-based care leads to substantial health care cost savings in comparison with care in a hospital setting. In summary, the findings of this integrative review imply that home-based initiatives are valuable not only to patients but also to public health care systems and their professionals. They are potential tools to assist the management of patients, especially those that require additional support -such as those with cancer or progressive diseases- and improve their well-being and satisfaction with medications. Additionally, further implementation of home-based initiatives on health care systems may potentially ease the care burden of chronic diseases that require multiple, long-term medications, and save health care costs. The positive impact of home interventions on patient and economic outcomes makes it necessary to improve and standardize the current regulation of home-based services to facilitate their proper implementation.
Supplemental Material
sj-docx-1-hhc-10.1177_10848223211038305 – Supplemental material for Impact of Home Care Services on Patient and Economic Outcomes: A Targeted Review
Supplemental material, sj-docx-1-hhc-10.1177_10848223211038305 for Impact of Home Care Services on Patient and Economic Outcomes: A Targeted Review by Irene Lizano-Díez, Sonia Amaral-Rohter, Lucía Pérez-Carbonell and Susana Aceituno in Home Health Care Management & Practice
Footnotes
Acknowledgements
The authors would like to thank Elena Viciano at Outcomes’10 (Castellón de la Plana, Spain) for medical writing assistance.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Irene Lizano-Díez and Sonia Amaral-Rohter are employees of Ferrer; Lucía Pérez-Carbonell and Susana Aceituno have nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ferrer (Barcelona, Spain) provided financial support for the conduct of the research and publication of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.