
Abstract
Heart transplantation is the most important treatment option in end-stage heart failure, and heart transplant recipients should be monitored at home by healthcare professionals in terms of symptoms and self-care requisites. The aim of this study is to examine symptoms and self-care requisites of patients with heart transplantation after discharge. Symptoms and self-care requisites of 81 patients who had heart transplantation between 2015 and 2020 were evaluated retrospectively in this study. Survey data were collected using the telephone interview method. It was determined that 77.8% of the patients were male and their mean age was 41.87 ± 2.51 years. Fatigue (91.4%), pain in the back, neck, and joints (86.4%), restlessness/agitation (81.5%), weight gain (71.6%), and edema in the lower extremities (71.6%) were the first 5 common symptoms experienced at home after heart transplantation. It was also found that the vast majority of patients (80.2%) answered negatively to the question of eliminating the lack of knowledge about the disease, and some of the patients were found not to pay attention to some important issues (e.g., regular blood pressure check, quitting smoking, etc.). Findings revealed that patients with heart transplantation experience a series of symptoms, and their self-care requisites were mostly focused on education and information specific to the disease after discharge. As a part of public health nursing practices, home care concentrating on symptoms and learning needs of patients should be planned and organized with a multidisciplinary approach to decrease rehospitalization and contribute to cost-effectiveness after heart transplantation.
Introduction
End-stage heart failure is a clinical process in which signs and symptoms of heart failure persist despite optimal medical and/or surgical treatments, leading to rehospitalizations, and significantly shortening the survival of patients. 1 Heart transplantation is considered as the gold standard in the treatment of end-stage heart failure. 2 It is reported that the heart transplant rate in the United States in 2020 is 11.2 per million people. 3 In Europe, the highest heart transplant rate in 2019 was in Slovenia, which was 10.5 per million inhabitants, while it was 9.3 per million inhabitants in Croatia. 4 In our country, on the other hand, it is reported that a total of 91 people received heart transplantation in 2018. 5 Survival rates after heart transplantation are well enough, especially when compared to the natural history of end-stage heart failure, 6 and the latest data from the International Heart and Lung Transplantation registries indicate that 1-year survival after heart transplantation is 84.5%, and the 5-year survival is 72.5%. 7
Although heart transplantation is the most important treatment option for irreversible organ failure, physiological symptoms, psychological, and social problems are common in post-transplant patients. 8 It is reported in the literature that heart transplant patients may face with physical, mental, and social problems due to immunosuppressive treatment that should be used after transplantation, and comorbidities may develop in the long-term. 9 In a systematic review, it is stated that patients face with various symptoms such as pain, infection, fatigue, insomnia, and various side effects due to the long-term use of immunosuppressive treatment and medications that prevent organ rejection after organ transplantation. 10 In another study, it was found that patients experience a series of symptoms such as edema in the feet and legs, pain at the surgery site, weakness in the legs, memory problems, difficulty in concentrating, fatigue, insomnia, agitation, and depressive feelings after heart transplantation. 11 Symptoms and psychological and social problems have been reported to increase the needs of patients with heart transplantation, and this necessitates close monitoring of these patients after discharge. 10 The inability to manage or mismanage symptoms increases the health care costs in this patient group 12 along with difficulty in providing symptom management. 10 Therefore, determining symptoms of heart transplant patients after discharge should be considered among the priorities of follow-up care. 13
Although the diseases are the same, the course and recovery process differs in every individual in terms of physiological and psychological aspects after heart transplantation. In this context, evaluation of symptoms and self-care requisites of patients with heart transplantation is of great importance in terms of contributing to symptom management and meeting the needs of patients as soon as possible, as well as planning interventions to prevent and promote health in this patient group. Therefore, the primary aim of this study is to determine symptoms and self-care requisites of patients with heart transplantation and to guide health professionals providing treatment and care services to this patient group.
Methods
This retrospective study used a quantitative descriptive design. The study was conducted in one of the heart transplantation centers in Turkey with 81 patients who received heart transplantation between 2015 and 2020. Three members of the multidisciplinary research team practiced at this center and were influential in subject recruitment. The additional team members conducted the survey with patients. There were 126 patients who had heart transplantation between 2015 and 2020 at the relevant heart transplatation center, and it was determined that 11 patients were dead before the study. Therefore, 115 patients were planned to be included in the study.
Patients who met the inclusion criteria (>18 years old and having transplantation in the last 5 years) and agreed to participate in the study were included in the study. Some patients under 18 years old (12 patients) were excluded from the study, and 22 patients stated that they did not want to participate in the study. Therefore, 81 patients constituted the study sample.
The data were collected between January and April 2021 by using the telephone interview method. Patients’ contact information was obtained from the hospital electronic records, hospital archive, and hospital database. Detailed information about the study was given to the patients on the phone, and informed consent forms were sent by mail. After the signed consent forms were received by the researcher, the patients were called by phone and the “Patient Information Form,” “Symptom Checklist,” and “Self-Care Requisites Form” were applied to the patients.
Patient Information Form consisted of 13 questions including socio-demographic characteristics and information about the disease and the postoperative period (Table 1). Symptom Checklist was prepared by the researchers according to the literature10,11,13 to evaluate the symptoms of patients with heart transplantation and it consists of 21 symptoms (fatigue, pain, restlessness/agitation, shortness of breathing, etc.; Table 2). Self-Care Requisites Form based on Orem’s self-care theory 14 was prepared to evaluate the self-care requisites after heart transplantation. Patients’ self-care requisites were evaluated under 3 subheadings as universal self-care requisites, developmental self-care requisites, and self-care requisites in health deviations. It consists of a total of 34 items (10 items for universal self-care requisites, 6 items for developmental self-care requisites, and 18 items for self-care requisites in health deviations) (Table 3, Table 4, Table 5).
Descriptive Characteristics of the Patients (n = 81).
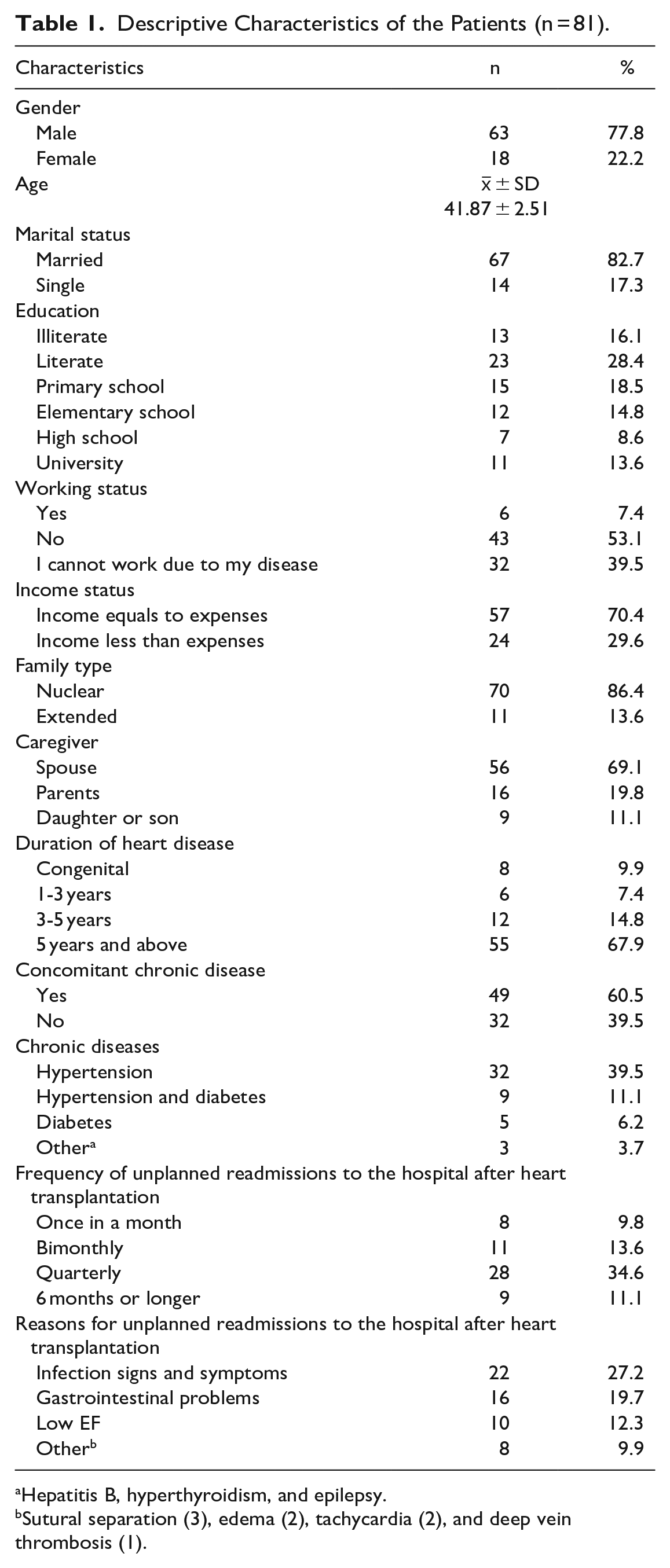
Hepatitis B, hyperthyroidism, and epilepsy.
Sutural separation (3), edema (2), tachycardia (2), and deep vein thrombosis (1).
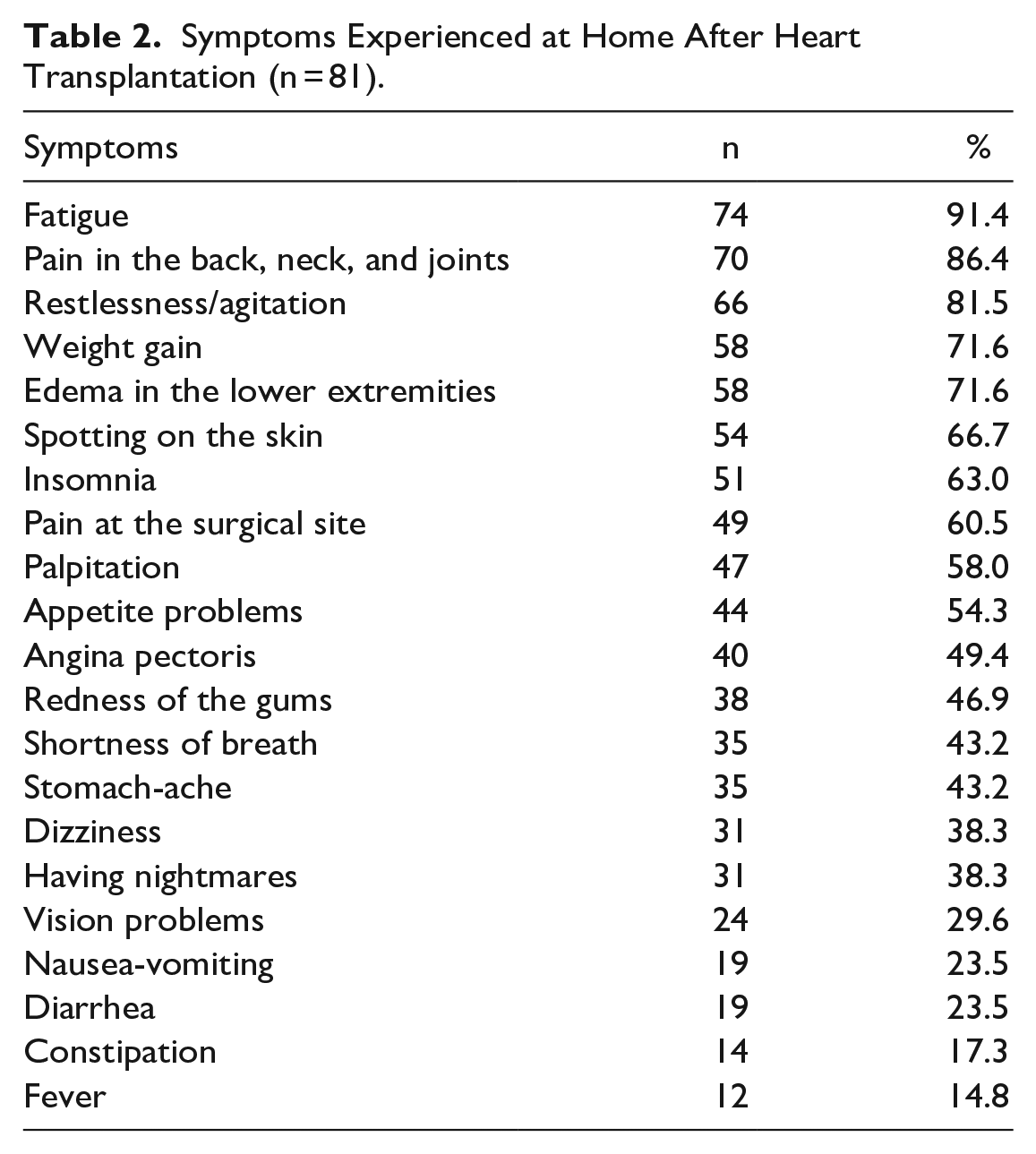
Symptoms Experienced at Home After Heart Transplantation (n = 81).
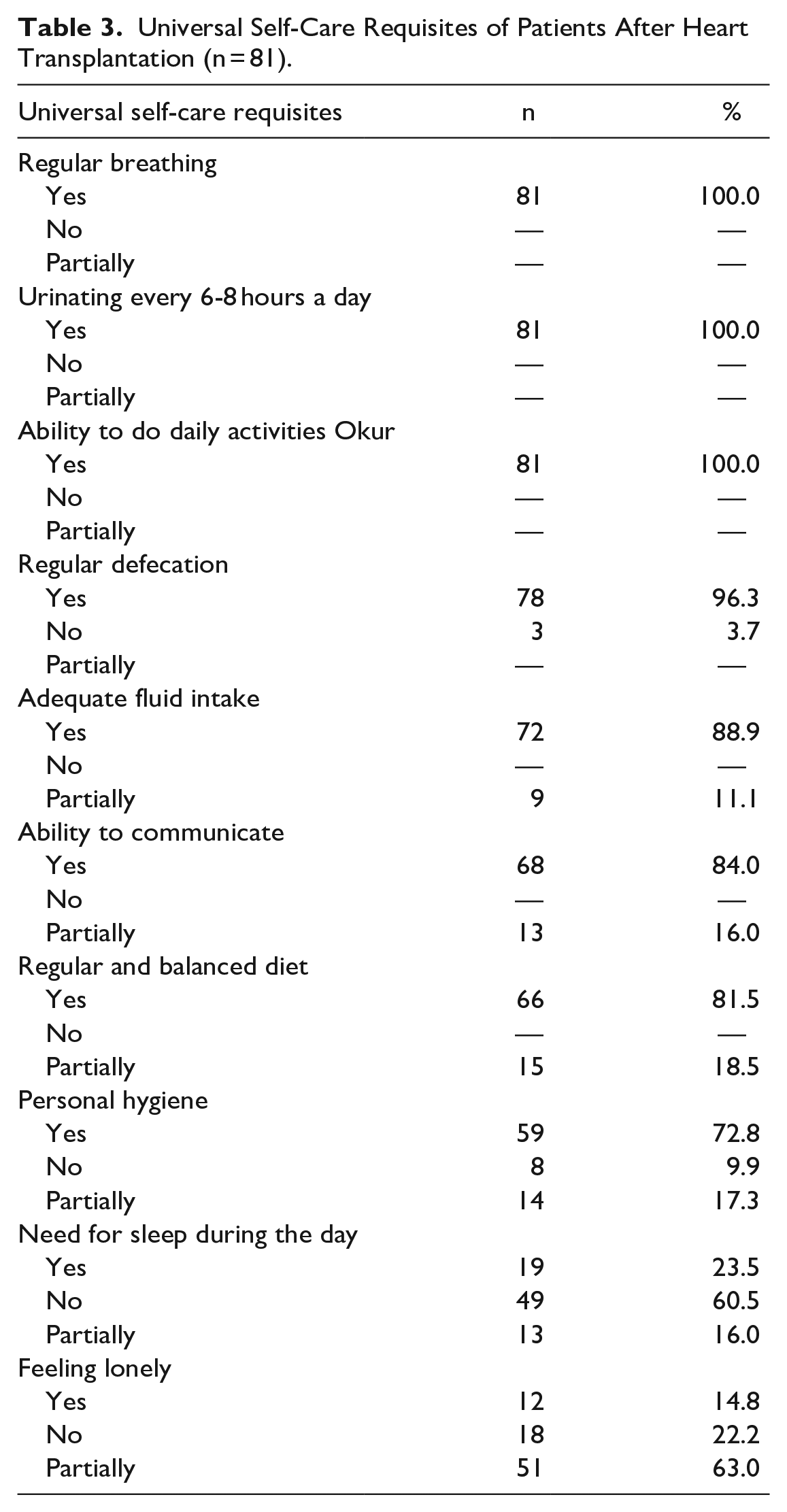
Universal Self-Care Requisites of Patients After Heart Transplantation (n = 81).
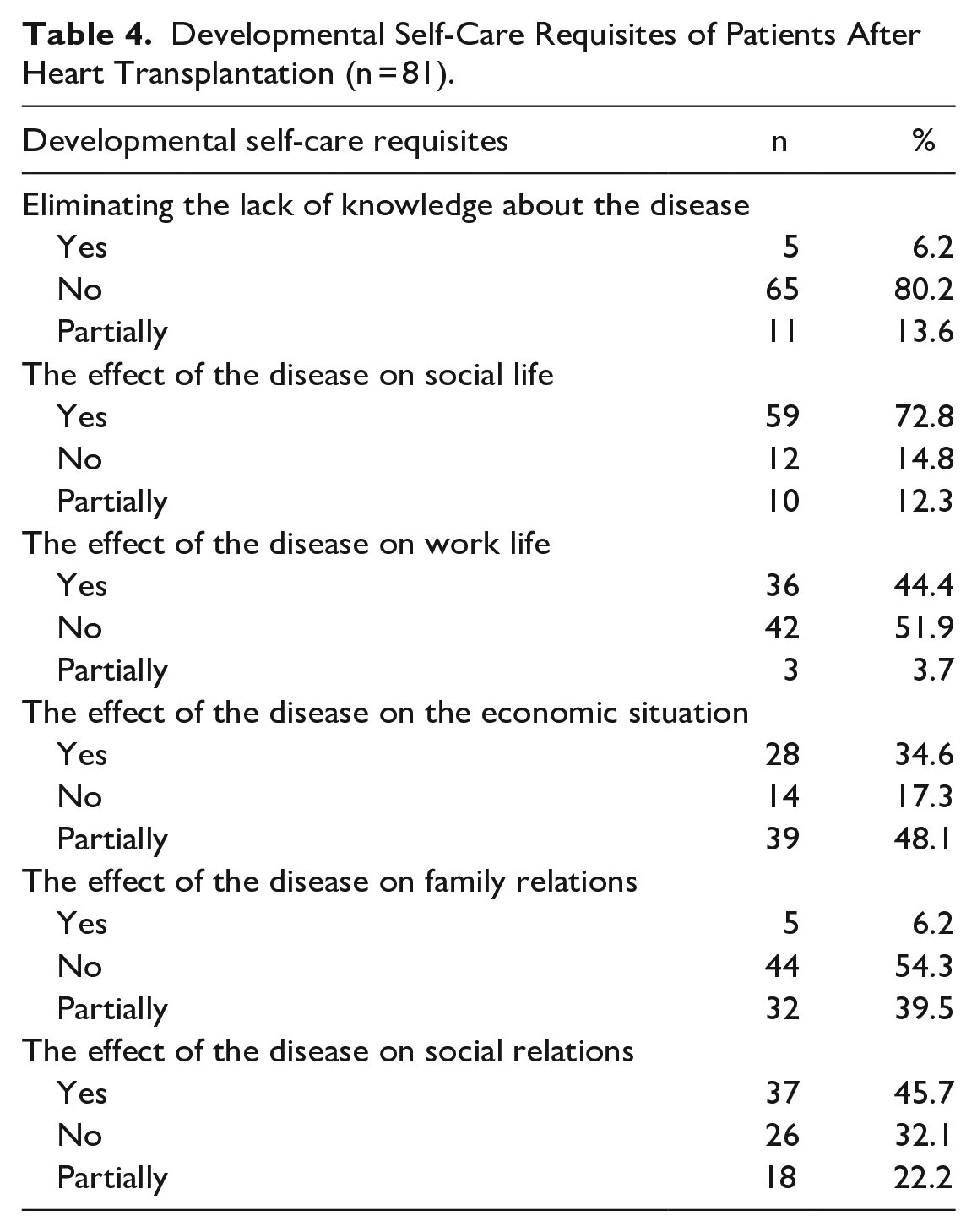
Developmental Self-Care Requisites of Patients After Heart Transplantation (n = 81).
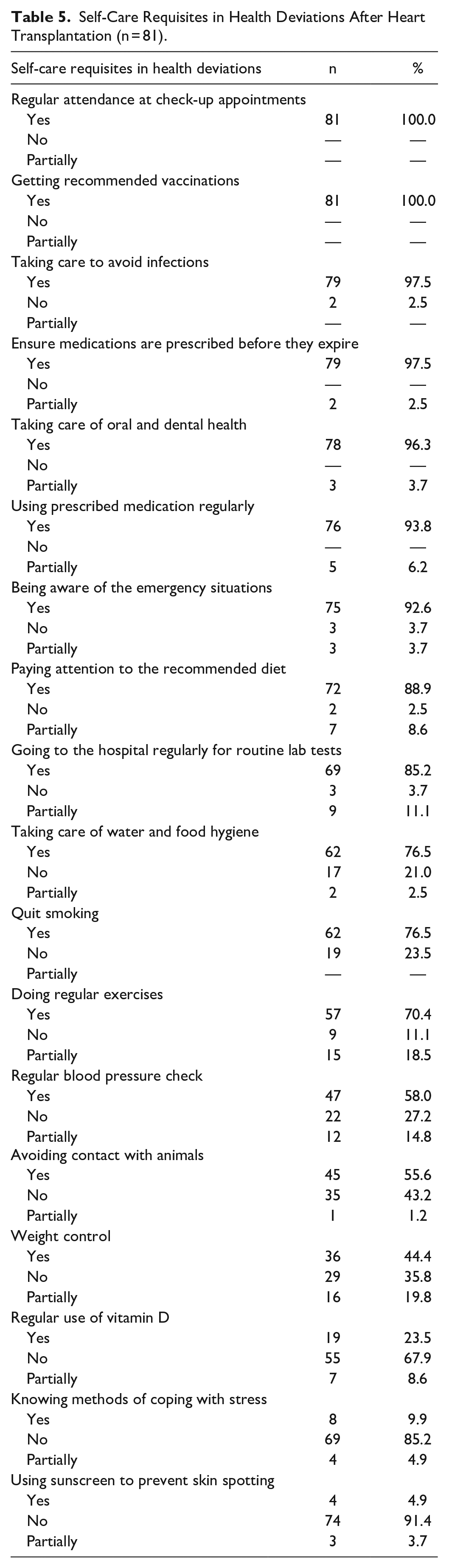
Self-Care Requisites in Health Deviations After Heart Transplantation (n = 81).
Data Analysis
The data of the research were analyzed using the SPSS for Windows 22.0 package program (IBM Corp., Armonk, NY, USA). Numbers, percentages, mean, and standard deviation were used in the evaluation of the data.
Ethical Considerations
This research was approved by the Non-Invasive Clinical Research Ethics Committee of the Hospital with the decision dated 16.01.2020 and numbered 2020.1/01-279. In addition, informed consent forms have been read and signed by all participants included in the study.
Results
The distribution of the descriptive characteristics of patients is given in Table 1. Patients’ ages ranged from 18 to 64 and most of them were male. About 45% of the group had no education, while about 25% had a high school or higher education. More than half of the patients were not working for any reasons and had heart disease for more than 5 years. It was determined that 60.5% of the patients had a concomitant chronic disease, and hypertension was the most common chronic disease. In addition, according to the hospital database, it was determined that more than half of the patients (69.1%) readmitted to the hospital at least once out of their control appointments, and 27.2% of them readmitted for infection signs and symptoms (Table 1).
The distribution of the symptoms is given in Table 2, and it was determined that the first 5 most common symptoms were fatigue, pain in the back, neck, and joints, restlessness/agitation, weight gain, and edema in the lower extremities. In addition, more than half of the patients were found to have skin spots, insomnia, pain at the surgical site, palpitation, and appetite problems (Table 2).
Findings regarding the universal, developmental, and self-care requisites of the patients are presented in Table 3, Table 4 and Table 5. It was determined that heart transplant patients could mostly meet their universal self-care requisites, while they could rarely meet their personal hygiene needs, and almost 2/3 of them felt lonely from time to time. When the developmental self-care requisites were examined; it was found that the vast majority of patients answered negatively to the question of eliminating the lack of knowledge about the disease, and the disease had a negative impact on their social and work life and affected their social relations. It was also found that almost all the patients showed due care to important issues like going regularly to the control appointments, getting recommended vaccinations, avoiding infections, taking care of oral and dental health, using prescribed medications regularly, etc., while some of them were found not to pay attention to some important issues like using sunscreen to prevent skin spotting, knowing how to cope with stress, using vitamin D regularly, taking care to avoid contact with animals, weight control, regular blood pressure check, quitting smoking, etc. (Table 3, Table 4, Table 5)
Discussion
After heart transplantation, symptoms of heart failure leave its place to the problems occurred due to the surgical procedure, complications of transplantation, and the side effects of immunosuppressive treatment. 11 In a systematic review examining the difficulties and needs of organ transplant patients, it is reported that transplant patients experience deterioration in physical comfort, pain, infection, fatigue, sleep problems, various complications, and side effects related to the use of anti-rejection drugs and immunosuppressives. In the same study, it is stated that multiple symptoms negatively affect patients’ quality of life by causing rehospitalization and inability to maintain daily activities. 10 In another study, the most common symptoms in the first 5 to 10 years following the heart transplantation were found to be memory problems, fatigue, cramp-like pain in the hands, feet, and legs, restlessness, skin tenderness, weight gain, edema in the legs and feet, drowsiness, agitation, vision problems, and diarrhea. 11 In another study, it was found that shortness of breath, bloating, nausea-vomiting, appetite problems, diarrhea, itchy skin, headache, pain, tremor in the hands, dizziness, feeling sad, and decreased libido were commonly experienced symptoms in the first 2 years after heart transplantation. 13 Similarly, in our study, in which the symptoms in the first 5 years of heart transplantation were evaluated, it was determined that fatigue, pain in the back, neck, and joints, restlessness/agitation, weight gain, and edema in the lower extremities were the most common symptoms, and skin spotting, insomnia, pain at the surgical site, palpitation, and appetite problems were other symptoms observed in more than half of the patients in this study.
Fatigue is one of the frequently reported symptoms after heart transplantation,15,16 and it is reported in the literature that fatigue should be evaluated in this patient group. 13 Similar to the literature, fatigue was determined to be one of the most frequently reported symptoms in our study. Many factors contribute to the emergence of fatigue after heart transplantation, and it is claimed that fatigue is one of the most common symptoms associated with immunosuppressive treatment in organ transplant patients. 17 Fatigue, which has a complex relationship with many symptoms, is also reported to be associated with sleep problems in organ transplant patients. 18 In our study, it was determined that in addition to fatigue, more than half of the patient experienced insomnia and nearly half of them had nightmares. Therefore, one of the reasons for fatigue may be related to the sleep problems, which may have increased fatigue in this patient group in addition to the side effects of immunosuppressive use. Since fatigue is a multidimensional symptom and associated with many variables, we assume that an in-depth investigation of the determinants of fatigue may contribute to the recovery process of patients with heart transplantation.
Diarrhea and other gastrointestinal system symptoms are frequently seen after solid organ transplantations and it is suggested that 12.6% to 34% of these symptoms occur due to immunosuppressive treatment. 19 All patients included in this study are routinely prescribed cyclosporine, everolimus, mycophenolate mofetil (MMF), and prednisolone after heart transplantation. Although it is suggested in the literature that the use of MMF significantly reduces acute rejection, it is also reported that it causes an increase in gastrointestinal complications. 20 In a study evaluating the efficacy and safety of sirolimus and everolimus, it was reported that symptoms like edema, gastrointestinal symptoms, and infection caused treatment discontinuation in 39% of all patients. 21 In this respect, one of the reasons for gastrointestinal symptoms experienced by patients participating in our study may be due to the side effects of the immunosuppressive treatment routinely prescribed after heart transplantation.
Organ transplantation is a chronic condition that requires patients to have some skills to manage their own health, that is, self-management.13,22,23 The most important part of self-management is symptom management and in patients with heart transplantation individual-oriented symptom management should be provided to cope with the side effects of ongoing medical treatment. 13 In the literature, it is stated that the inability to manage or mismanage symptoms has negative impact on patients and health care costs. 10 In our study, according to the data obtained from the hospital database, it was determined that more than half of the patients made unplanned readmissions to the hospital for various reasons at least once following heart transplantation, leading to an increase in health care costs. In the literature, it is strongly suggested that the transplant team must provide necessary support in the development of symptom management strategies in order to make patients to cope with the side effects of treatment and to enable them to manage their symptoms. 13 Adopting a more holistic approach in the follow-up care, which should be provided at home after heart transplantation, and moving from traditional care to chronic disease management approach, which deals with the patient from multiple perspectives, can improve patient outcomes, and contribute to the cost-effectiveness of health care services.
In the literature, it is stated that in addition to evaluating the problems and symptoms faced by transplant patients, healthcare professionals should also focus on the needs of patients, and this approach increases the quality of life of patients. Home care needs after organ transplantation are defined as psychological needs, educational and information needs, social needs, and other needs (i.e., symptom management, medical needs, coping with stress, social support, etc.). 10 In our study, in which the self-care requisites of patients were evaluated along with the symptoms, it was concluded that the education and information needs come to the forefront in our patient group. We assume that negative answers related to the topics which patients need to be educated and informed are related to the fact that education and information needs of the patients were not adequately met, especially in the post-discharge period. Transplant team members are supposed to identify knowledge gaps and new methods to address learning needs of patients after transplantation. 24 In some study conducted with patients with solid organ transplants, however, patients stated that they did not receive enough information to help them cope with the difficulties they encountered after transplantation.25,26 Therefore, it is obvious that there is a need for educational programs which inform patients about many subjects like symptoms, medical treatment, beneficial lifestyle changes, or emergencies after heart transplantation. In this context, we anticipate that planning individual-specific education programs will contribute to the adaptation process of patients, who try hard to adapt the new situation, as well as symptom management after heart transplantation. We also think that all these interventions will have a positive impact for preventing and promoting health in this patient group.
Limitations
There are some limitations to this study. One of them is that the study was conducted as a single center and retrospectively. Due to the retrospective methodology of our study, we only included patients who had heart transplantation in the last 5 years so that they could remember their symptoms and needs, therefore, including limited number of patients to this study is another limitation. The fact that heart transplantation is performed in fewer numbers than other open-heart surgeries is also a limitation of this study.
Conclusion
Findings obtained from this study reveal that patients with heart transplantation experience a series of symptoms after discharge, and this study provides a roadmap for symptoms and self-care requisites that heart transplant patients may experience in the first 5 years following the transplantation. In addition, it was also determined that the self-care requisites of patients with heart transplantation were mostly focused on getting education and information specific to the disease. Since heart transplantation is invaluable and performed in limited numbers in all countries, home care services after discharge are of significant importance in terms of protecting the transplanted heart. Thanks to home care services, patients may experience fewer symptoms, therefore, unplanned returns to the hospital may decrease along with health care costs. Therefore, nursing interventions concentrating on symptoms and education needs of patients to ensure symptom management and contribute to patients’ quality of life after heart transplantation should be planned and organized with a multidisciplinary approach.
Footnotes
Correction (February 2024):
Article updated to correct an article type from “Review Article” to “Original Article”.
Author’s Note
This research has been presented as oral presentation at the third International Home Care Congress, Istanbul, Turkey (09-12 November, 2021) and has been awarded as the best oral presentation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.