
Abstract
During home health care (HHC) admissions, nurses provide input into decisions regarding the skilled nursing visit frequency and episode duration. This important clinical decision can impact patient outcomes including hospitalization. Episode duration has recently gained greater importance due to the Centers for Medicare and Medicaid Services (CMS) decrease in reimbursable episode length from 60 to 30 days. We examined admissions nurses’ visit pattern decision-making and whether it is influenced by documentation available before and during the first home visit, agency standards, other disciplines being scheduled, and electronic health record (EHR) use. This observational mixed-methods study included admission document analysis, structured interviews, and a think-aloud protocol with 18 nurses from 3 diverse HHC agencies (6 at each) admitting 2 patients each (36 patients). Findings show that prior to entering the home, nurses had an information deficit; they either did not predict the patient’s visit frequency and episode duration or stated them based on experience with similar patients. Following patient interaction in the home, nurses were able to make this decision. Completion of documentation using the EHR did not appear to influence visit pattern decisions. Patient condition and insurance restrictions were influential on both frequency and duration. Given the information deficit at admission, and the delay in visit pattern decision making, we offer health information technology recommendations on electronic communication of structured information, and EHR documentation and decision support.
Keywords
The skilled nursing (SN) visit pattern frequency and duration for the episode is an important home health care (HHC) clinical decision that can impact patient outcomes, including hospitalization.1,2 This decision, made to address the patient’s needed level of attention (eg, monitoring condition change) and care intensity, has 3 components: timing of the first visit, subsequent visit frequency (ie, visits per week), and episode duration (ie, weeks in episode).
Visit pattern frequency and duration were associated with hospitalization risk in a national sample, where patients with fewer than 4 SN visits or episodes shorter than 22 days were more likely to be hospitalized. 3 Half of their unplanned hospitalizations occurred within the 2 weeks following HHC admission. 4 Early and intensive SN visits (frontloading) for high risk patients may reduce hospitalization risk 1 by enabling earlier medication issues identification, close patient condition monitoring, and teaching opportunity enhancement. Recognized as an evidence-based best practice,5-9 frontloading provides in the first 14 days either 60% of planned visits, 1 or 5 or more visits. 3
Insurer reimbursement for agency services impact frequency and duration. During the study, the Centers for Medicare and Medicaid Services (CMS) reimbursed at a lower rate when agencies did not meet the threshold of 5 visits for a 60-day episode, Low Utilization Payment Adjustment (LUPA). Visit duration is of heightened interest due to the recent CMS reimbursable episode length reduction from 60 to 30 days, 10 and LUPA threshold of 2 to 6 visits under the Patient Driven Groupings Model. 11
The importance of the planned visit pattern decision has stimulated recent development of qualitative evidence about how HHC nurses make these decisions. Knowledge about what information items nurses use in their decision making at different times during the admission process would be informative in the consideration of health information technology to support the nurse in this decision-making. The admission entails a patient home visit and completion of the documentation and care plan containing the patient’s needs and future care provision.
Two objectives of the current study are to examine: (1) HHC admission nurses’ visit pattern decisions and (2) how they were influenced by documentation available before and during the patient visit, agency standards, coordination with other disciplines, and electronic health record (EHR) use. Our third objective was to offer health information technology (HIT) recommendations to improve information transfer from referrer to the HHC nurse admitting the patient.
Methods
This mixed-methods observational study included document analysis and structured interviews. The Drexel University Institutional Review Board approved the study. All nurse participants volunteered and provided consent. Patients also consented. The study reimbursed the agencies for the nurses’ time.
This study is part of a larger study to characterize HHC nurses’ information and decision practices at admission and to assess EHR impact on these practices, conducted in 2016 to 2018. The overarching goal is to advance HIT standards recommendations for HHC EHR systems and to enhance the HHC admission process.
Setting and Participants
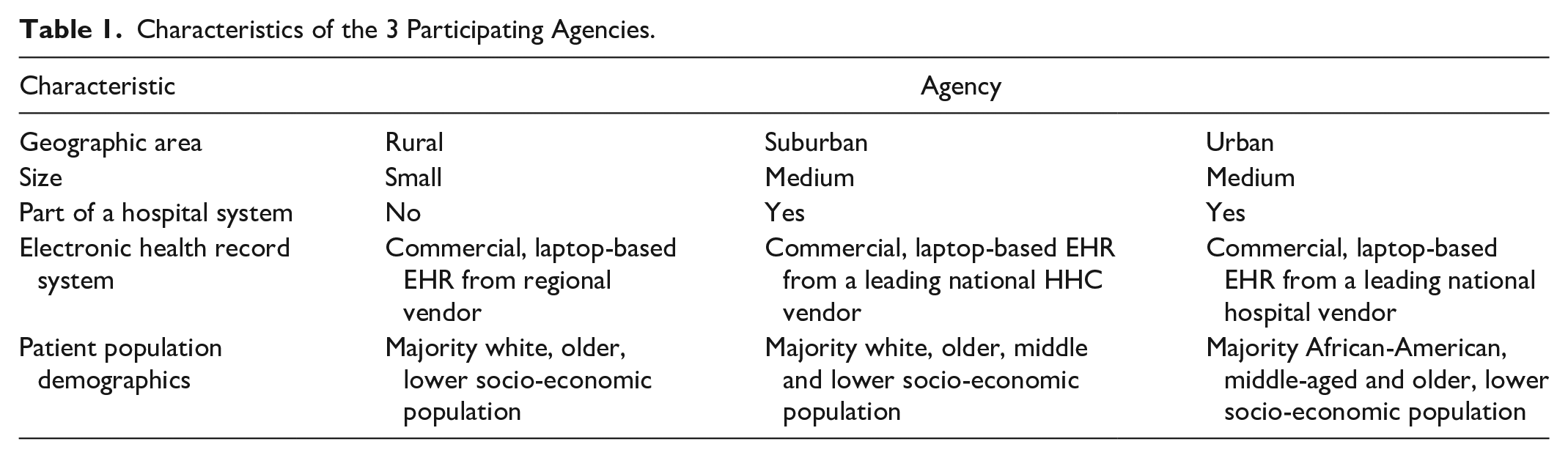
Three geographically diverse (ie, urban, suburban, rural) Pennsylvania agencies participated (Table 1). Each used different point-of-care EHRs.
Characteristics of the 3 Participating Agencies.
Six nurses per agency were observed admitting 2 patients each. At each agency, the first visit timing decision was made by agency staff and is not included in the study scope.
No agency EHR had structured referral data nor a structured data field for recording the planned visit pattern. The urban agency nurses were able to view EHRs of patients referred from tertiary care hospitals and physicians within the same health system.
Data Collection
Two or 3 researchers conducted each observation. The 2 observers always present were a health informatician knowledgeable in HHC and a human factors scientist with health care expertise. The third observer was either o human factors post-doctoral fellow or a research assistant familiar with HHC. Documents specified below were obtained after the observations. Nurses were audio-recorded, and planned SN visit pattern decisions and associated rationale noted. Data collection occurred across 3 phases.
Documentation and information availability
In the Pre-Visit phase, the rural agency nurses had paper referral documents; the others had electronic documents. Referral documents were not designed to have visit pattern information. The rural 12 and urban agencies used intake documents which contained patient information from the referral site.
In the Visit phase in the patient’s home, the researchers observed the admission, including assessing the patient and home environment, and gathering information from the patient and caregiver, if present. Transition documents (ie, discharge summary, progress note) in the Visit phase are designed for patient use (not the visit pattern decision). Thus, we anticipated that the patient and possibly informal caregivers may provide more relevant data including patient preferences.
In the Post-Visit phase, nurses returned to the office to complete the care plan documentation, including the visit pattern plan, and related information in the EHR
Decision response
Before the Pre-Visit phase and after the Visit and Post-Visit phases, the nurse was asked for the then current visit pattern decision. If the nurse changed the decision in the Visit or Post-Visit phase, the nurse was asked what made him/her change his/her mind.
Data Analysis
Data were stored on a secure, password-protected server. Transcription was completed by study team members.
Quantitative analysis of documentation and decision responses
Researchers analyzed the availability of visit pattern information in the documents accessible to the nurses. Nurses provided visit pattern information in the form of 1 or more visits for a set of weeks. For example, 1-2W1 2W2-3 1-2W4 means 1 to 2 visits for the first week, 2 visits per week for the next 2 to 3 weeks, and 1 to 2 visits for the following 4 weeks. Researchers used the maximum value (eg, 1-2W4 was coded as 2 visits*4 weeks = 8 visits). Changes in maximum value between phases were identified for frequency and in duration.
Qualitative analysis of decision responses
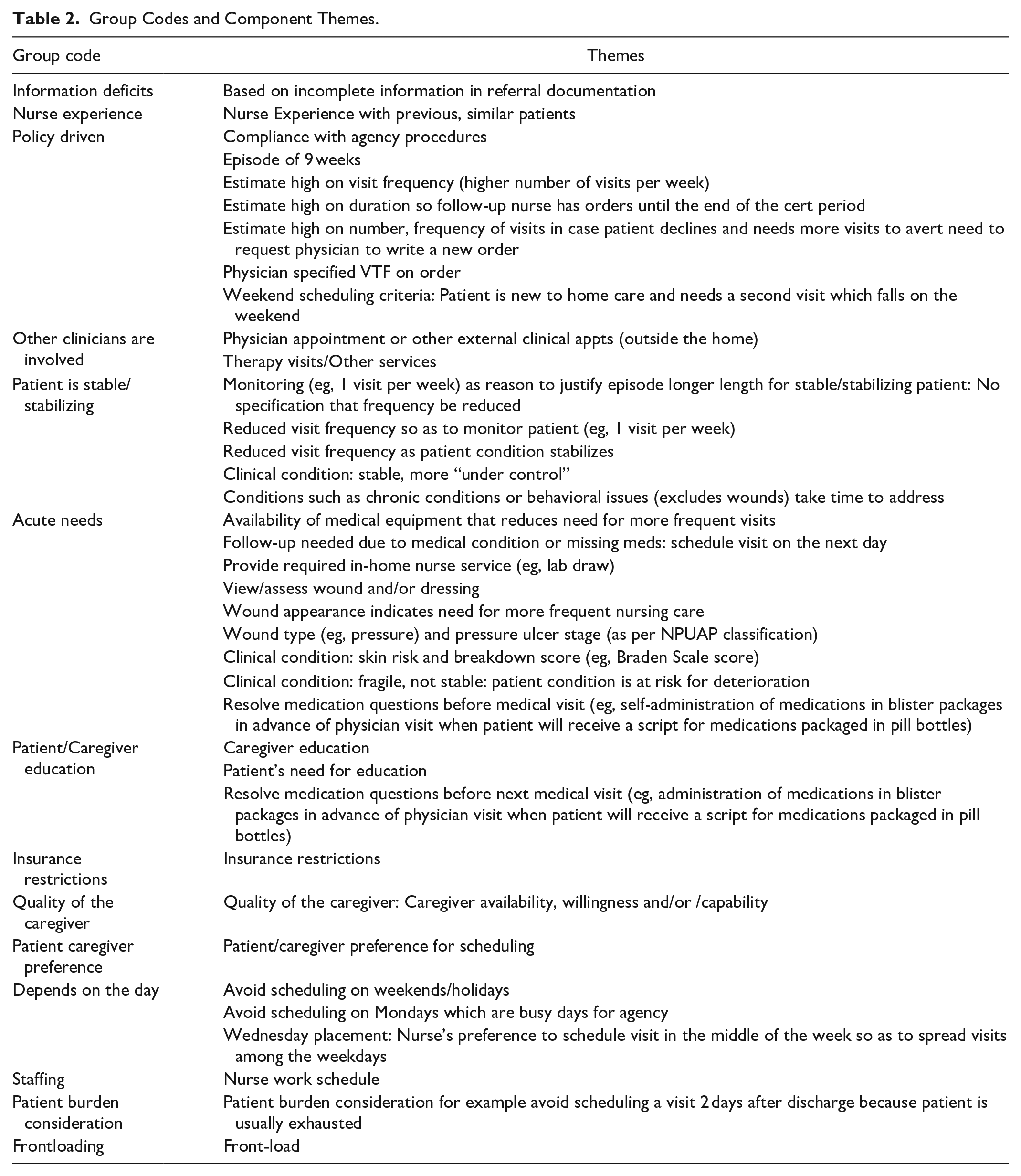
Researchers identified rationale for the visit pattern decisions using conceptual content analysis, a method used to quantify the occurrence of a word, phrase, or text in a document. 13 Quotes were systematically extracted to identify and interpret concepts within the responses. Three researchers codified the quotes into broader themes 14 using discussion to reach consensus. A fourth researcher subsequently independently reviewed and grouped themes to produce group codes (Table 2). Further group code organization produced patient-specific themes, agency-specific themes, and health system themes which the team reviewed and agreed upon.
Group Codes and Component Themes.
Mixed methods analysis of decision responses
This analysis incorporated document and information availability findings, and matched by phase quantitative data (ie, nurse response counts) with qualitative data (ie, interview quotes). The latter provided context for the quantitative data.
Results
The majority of nurses were female. The mean age was 40.4 years old with a mean of 15.6 years of healthcare experience.
Documentation and Information Availability
Future visit pattern order information was rarely available in the Pre-Visit and Visit phase documentation. The exception was for 2 patients at the rural agency, where 2 SN facilities (SNF) included quantitative visit frequency information in referral documentation.
Decision Response
The presence or absence of nurses’ visit pattern responses, organized by phase and HHC agency, are shown in Figure 1. Some nurses would not provide a definitive visit pattern in the Pre-Visit phase. Some stated they were unable to make a decision (coded as no response in Figure 1) while others chose not to answer the question (missing values in Figure 1). In the Visit and Post-Visit interviews, all gave definitive visit pattern responses.
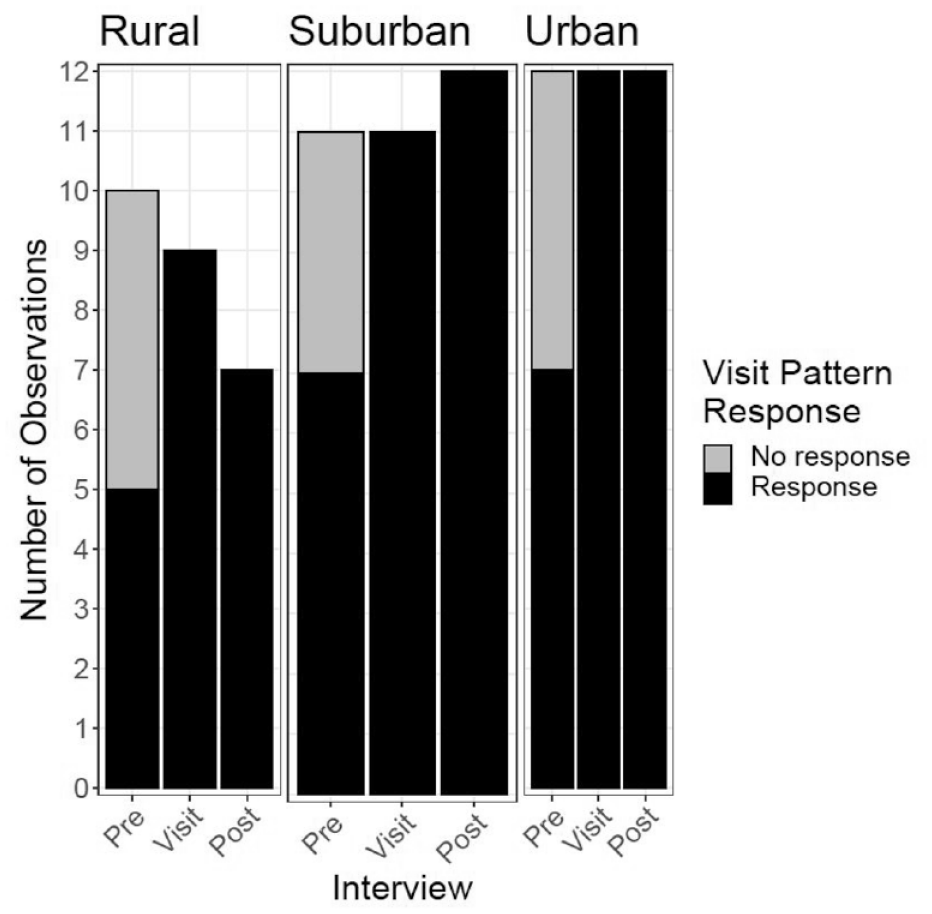
Visit pattern decision response by phase by agency*.
Frequency decision
The median number of visits planned for each phase shows variation. The Pre-Visit phase median response for planned visits was 10 (range: 3, 63). The upper range was an urban agency nurse’s response of daily visits for the episode. The Visit and Post-Visit median responses were both 12 (2, 27) visits planned.
The change in nurses’ visit pattern responses related to frequency and duration, organized by phase and HHC agency, are shown in Figures 2 and 3, respectively. Fifteen out of 19 nurse decisions (79%) changed between the Pre-Visit and Visit phases (Figure 2). From the Visit to the Post-Visit phase, no rural or urban agency nurse modified any decisions, while over half the suburban nurse decisions (6 of 11) changed. One suburban nurse offered rationale: “when you’re actually writing the order it makes you think a little bit more sharply about what you really mean” (S08). This rationale appears to describe a work process involving synthesis of information and/or the desire to provide accurate documentation.
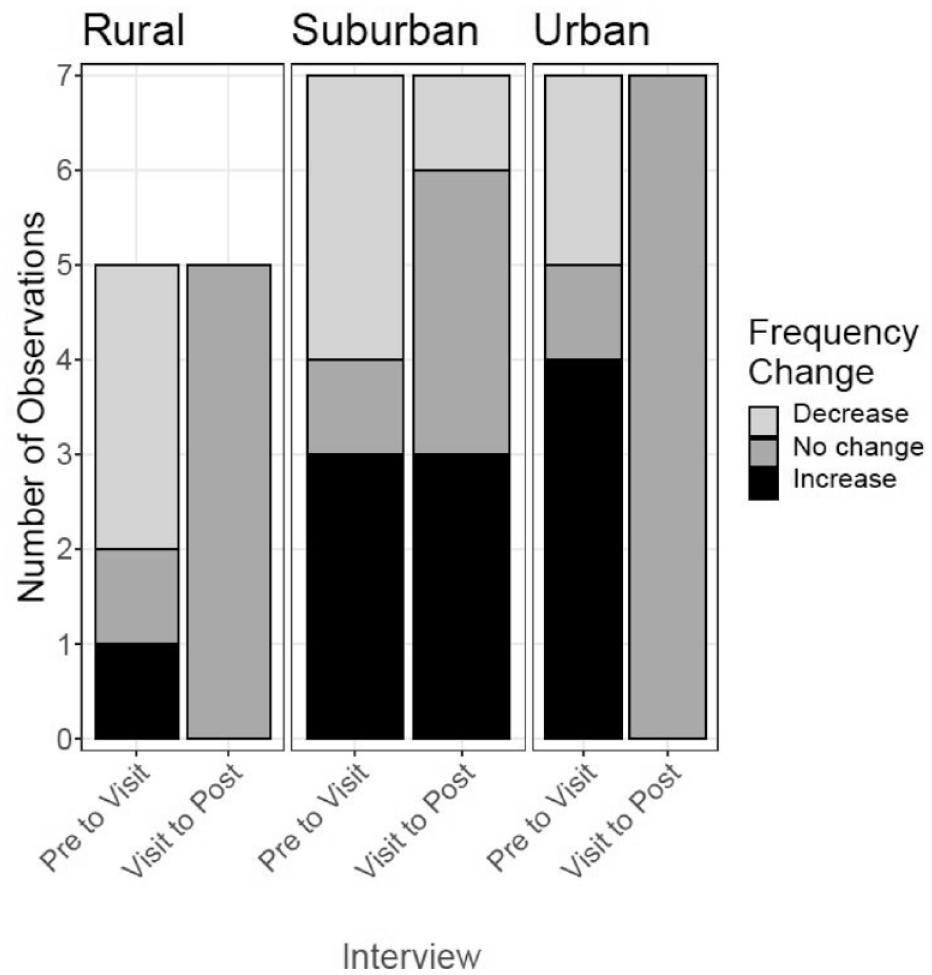
Visit pattern frequency cross-phase changes by agency.*
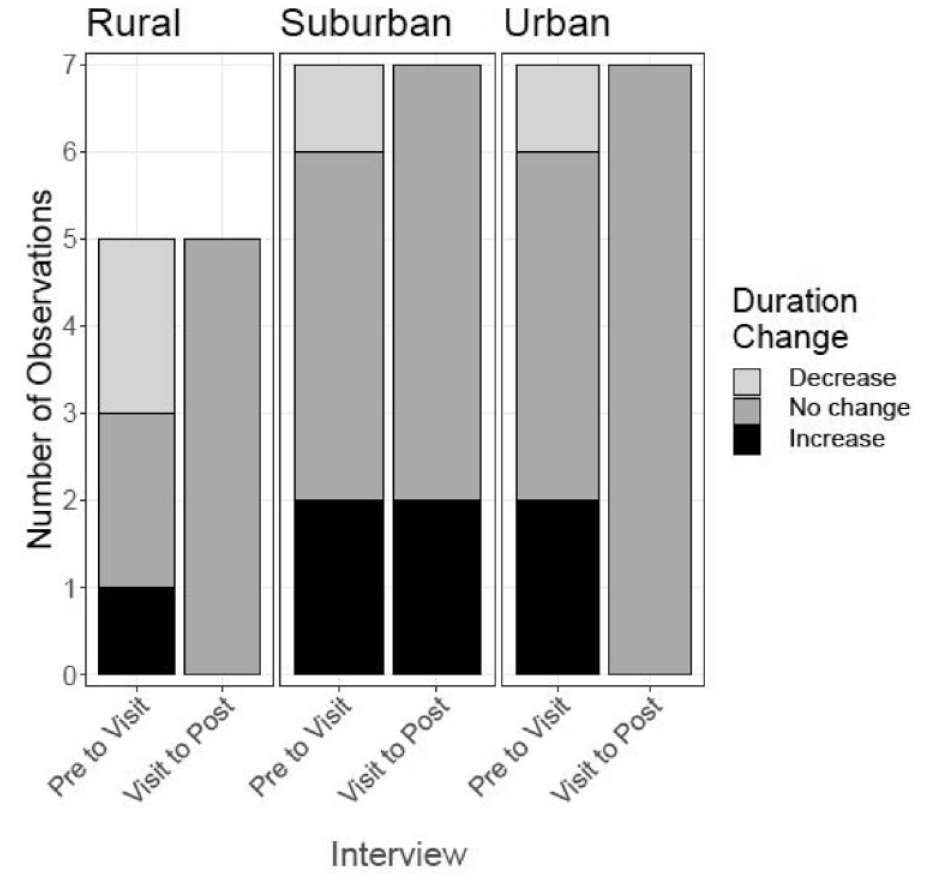
Visit pattern duration cross-phase changes by agency.*
Duration decision
The median number of planned weeks in an episode in Pre-Visit, Visit, and Post-Visit phases were 4 (range: 1, 9), 5.5 (1, 9), and 8 weeks (1, 9 planned) respectively.
Duration decision changes were more frequent from Pre-Visit to Visit (10 of 19 observations, 53%), than from Visit to Post-Visit (3 of 29 observations, 10%) (Figure 3). Only suburban agency nurses changed their decisions from Visit to Post-Visit.
Five of the six urban agency nurses had similar planned visit patterns: 1 to 2, or 2 to 3 visits per week for each week. All nurses replied with the maximum duration. The sixth nurse was a specialized nurse whose responses indicated a set pattern of daily visits.
Decision rationale
Fourteen groups of qualitative themes emerged to elucidate nurses’ rationales for visit pattern changes (each group is indicated with a group code: see group codes in Table 2). We present 7 exemplar grouped themes (group code) by phase with the referenced quotes in Table 3. No nurses mentioned documents or the EHR as a source of patient information.
Study Themes Organized by Phase of Occurrence and Group Code, with Illustrative Quotes (with U for Urban Agency, S for Suburban, and R for Rural).
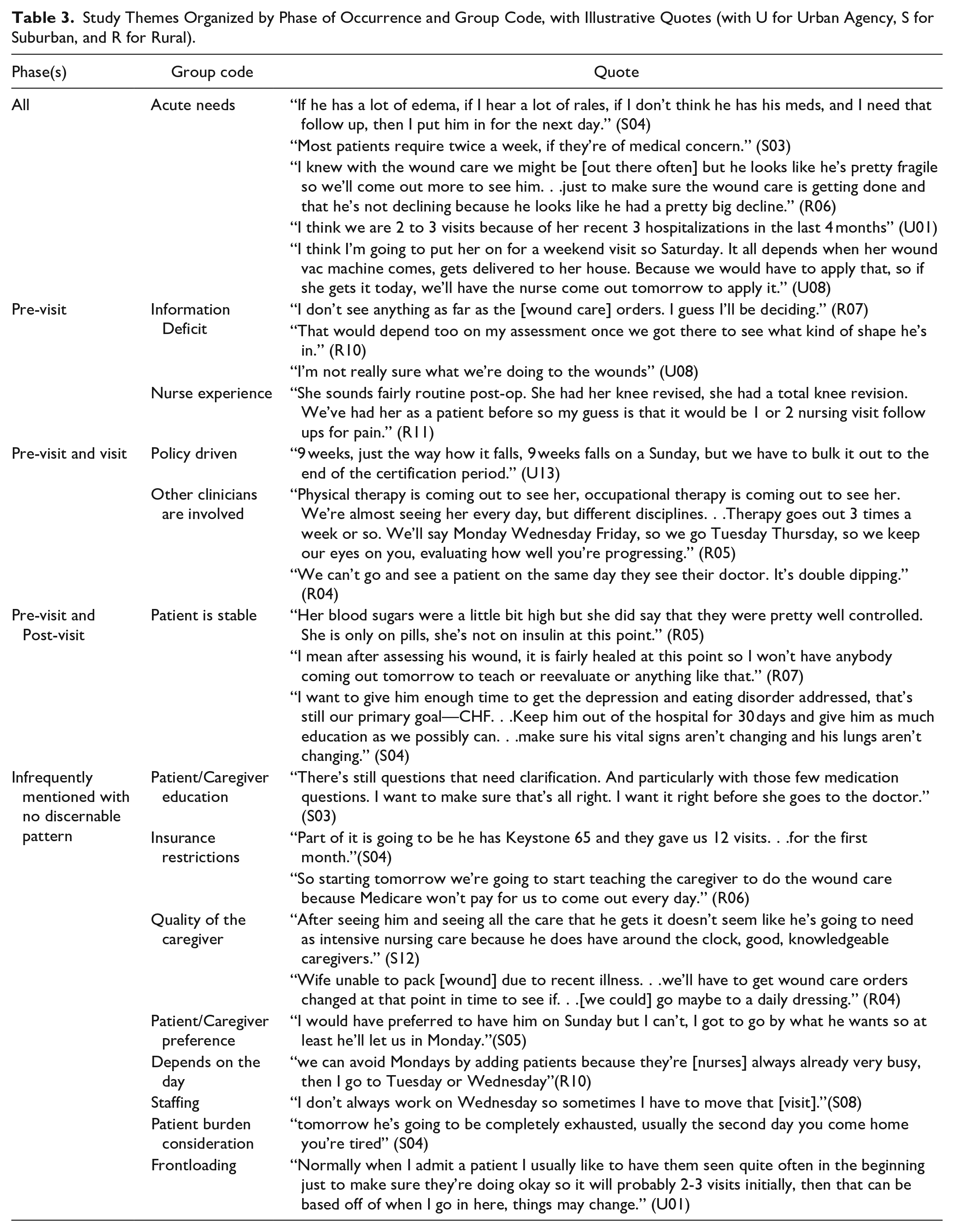
The Acute Needs theme was mentioned in all phases. Acute Needs refers to patient conditions (eg, multiple recent hospitalizations (U01), wounds (R06)) that typically require increased time, attention, and equipment (U08) and therefore increased frequency (S04, R06) and duration.
Two themes were mentioned during the Pre-Visit phase. Information Deficits refers to a lack of sufficient information to make a determination prior to the Visit phase, for example, lack of wound care orders (R07, U08). Nurses preferred to physically assess the patient before making this decision (R10). The lack of occurrence of Information Deficits in subsequent phases suggests that nurses collected what information they needed. The second theme, Nurse Experience, refers to reliance on clinical judgment after the Visit phase. Nurses conceptualized an image of the patient based on the information provided and past experiences with similar patients, conditions, or problems (R11).
The Pre-Visit and Visit phases shared 2 themes. Decisions were Policy Driven, referring to policies (eg, Insurance Restrictions such as CMS reimbursement (U13)) or agency guidelines. The theme Other Clinicians are Involved considered visits scheduled to accommodate a patient’s clinical appointments. These appointments offer additional clinical “eyes on the patient” between nurse visits (R05). Nurses schedule visits when there is no other clinician surveillance (R04). When nurses had information about other clinicians’ schedules, they shifted visit days within the week.
The sole rationale during the Post-Visit, Patient is Stable, incorporated information from the physical assessment and information gathering, including medication self-administration (R05). Visits to a stable patient were to monitor recovery rather than perform teaching or treatments, thereby justifying reduced visit frequency (R07). Furthermore, shifting the focus of care from acute to chronic management influences duration decisions (S04).
Mixed Methods Contextualization
During the Pre-Visit over one-third of nurses did not provide the visit pattern. The theme Information Deficit gives context to the high occurrence of changes after this phase. During the Visit phase, the nurse relied heavily on patient and caregiver information disclosures. Nurses changed the majority of decisions between the Pre-Visit and Visit phases, as supported by the occurrence of patient condition themes in the Visit phase. In the Post-Visit phase, in approximately four-fifths of cases, nurses did not change the decision, indicating visit pattern decisions tended not to change during the EHR documentation activity.
The visit pattern theme, Frontloading was infrequently raised, either explicitly or implicitly. Nurses scheduled 2 or more visits per week for medically fragile patients (Acute Needs). Some suburban and urban agency nurses indicated frontloading (3 visits the first week, and at least twice for the following weeks). If the patient had a physician appointment the first week, the nurse planned to visit twice in that week which supports the theme, Other Clinicians are Involved. Wound care patients were excluded from this analysis as the wound care regimen determines the visit pattern. The rural agency’s medically fragile patients also received wound care.
Nurses scheduled 1 visit per week for medically stable patients (Patient is Stable). Four of 10 rural patients had planned episodes with only 2 or 4 visits, which would be a LUPA– less than 5 visits in an episode. No nurse’s reason mentioned managed care. One suburban patient had between 3 and 6 visits, a possible LUPA. The urban agency’s planned visits had a pattern of at least 1 visit per week for the maximum episode duration, which avoided LUPAs. Across agencies, the mention of Insurance Restrictions did not refer to LUPAs; instead, the reference was to a constraint on providing more visits.
Discussion
We examined how HHC nurses’ visit pattern decisions were made and modified in relation to available documentation, and the rationale for decision changes. Based on the findings we recommend HIT improvements regarding information transfer to support nurse visit pattern planning. This study is part of a growing body of research that recognizes the need to advance visit planning practices, potentially leading to additional coordination and decision support.
Documentation and Information Availability
Regarding available documentation, there was no information for the nurses before entering the patient home about the recommended visit frequency or duration, despite variation in the content, medium, and availability of referral and transition documents.” Patient information relevant to visit planning, such as medication self-management capability, and clinical problems including wounds, was unavailable in referral documents.12,15,16
Due to information unavailability, nurses were hampered in making visit pattern decisions before assessing the patient. Based on an emerging picture of the patient at the home visit, the nurses’ decisions evolved to identify a visit pattern that reflected the patient’s condition and care needs.
Following patient assessment, in 81% of cases the decision was unchanged during post visit documentation. All changes were made by the suburban agency nurses. Further research is needed to determine what was specifically useful in supporting the nurses’ reflection on the care plan during documentation, including the act of writing the order, the opportunity to review the information, particular features of the EHR, or other factors.
Frequency Decisions
Frontloading seldom was offered as a rationale or indicated in the decision responses. This finding was unexpected considering the emphasis on this approach to reduce hospitalizations,1,2,17 and that frontloading is an evidence-based best practice.5-9 Consistent with our results, frontloading has not been universally applied as indicated in recent national studies of heart failure and sepsis patients (only 23% and 44.7% respectively received early nursing visits).17,18 The infrequent occurrence of a frontloaded visit decision may be attributable to patients having physician appointments the first week and associated difficulty scheduling nursing visits. As a physician often sees the patient in the first week, perhaps the definition of frontloading should consider other disciplines in addition to nursing.
For episodes with Medicare as the primary insurer, LUPAs are an agency concern because of reduced reimbursement. For 2 agencies, possible LUPAs were observed. However, the EHR did not provide any feedback (eg, warning).
Duration Decisions
Nurses were constrained by agency policy which reflects CMS policy (Insurance Restrictions): Nurses at 1 agency tended to plan for the then maximum 60-day duration. The impact of recent CMS changes for reduced episode duration on visit pattern decisions is unknown and warrants study. Results could be compared to the hospitalization risk related to visit frequency and duration before the policy change. 3
At 1 agency, most nurses planned for the maximum episode duration, suggesting the visit pattern plan was not meaningful. The plans seemed to lack individualization, nurse decision-making, and communication about intensity of care. Having identified this pattern, future research should extend the investigation scope to examine actual visit patterns, to obtain rationale, and to compare planned and actual visit patterns.
Decision Rationale
Similar to Irani et al’s prior research,19,20 the study’s thematic analysis identified 10 themes. Irani’s theme, “Identify patient needs for visit prioritization,” maps to 3 themes from this study: Acute needs, Patient is Stable and Frontloading. Irani’s theme “Partner with patients for preferences identification” maps to 2 themes here: Patient Burden Consideration and Patient/Caregiver Preference. Irani’s theme “Coordinate with other providers visit timing to avoid overwhelming patients” maps to Other Clinicians are Involved here. Both Irani’s work and this study include “Nurse experience” as a critical component. The “Agency protocols” factor of Irani’s work maps to Policy driven in this study. The Policy/Payer level factor of Irani’s research maps to Insurance Restrictions here. The “Caregiver availability and willingness to participate factor” of Irani’s work maps to Quality of the Caregiver here.
We extend Irani et al’s work with 4 themes: Information Deficit, Patient/Caregiver Education, Depends on the Day, and Staffing. These additional themes need to be validated in future work. Note that 3 themes from Irani’s research did not emerge in our study: “Working within agency standards to meet productivity requirements,” “social factors,” and “identification of patients who were prescribed high risk medications.” This outcome was unexpected as most patients had high risk medications. 21 While patient education was included in the care plan, it was not mentioned as critical to the decision, perhaps because nurses did not fully articulate his/her thinking process.
Recommendations for HIT Changes
Electronic communication of information from referral source EHRs to HHC EHRs could increase availability of needed patient information and thereby reduce the information deficit. Examples include patient information related to orders, conditions (eg, wounds, symptoms), and durable medical equipment availability.
Electronic patient information could support identifying patients with risk characteristics that would benefit from frontloading. Coupled with decision support algorithms, agencies would be in a better position to schedule the first visit as well as the rest of the episode.22,23
Frequency of scheduling could be facilitated with HIT supported HHC updates on clinician appointments external to the agency (eg, physician). Electronic updates would supplant asking the patient or caregiver. For example, if HHC clinicians knew patients’ next outpatient provider visit was further in the future, they may schedule more timely and frequent visits in the interim: an efficiency improvement.
We also suggest that EHRs enable nurses to enter visit patterns that lack precision as structured data, for example, visit frequency as a numerical range (such as the current one- or 2-weeks approach). Having structured data would enable computations necessary to detect LUPAs and compliance with insurers’ regulations.
Information resulting from the above enhancements should be synthesized and presented in the EHR as guidance during the admission, rather than as alerts which may be distracting. 24
Strengths and Limitations
Study strengths include the 3 diverse HHC agencies with a mixed methods approach. Limitations include a 36-observation sample size which may constrain generalizability. This study explored planned visit patterns while actual visits conducted were out of scope, thus preventing determining how visit patterns changed during the episode.
Conclusion
HHC nurses during patient admission made important decisions about future nurse visit patterns in the absence of needed information, which creates challenges for timely decision-making. Nurses tended to rethink care and plan the visit pattern when they assessed the patient and home. Given the information deficit at admission and the delay in visit pattern decision making, HIT recommendations on electronic communication of structured information, and EHR documentation and decision support warrant further consideration.
Footnotes
Acknowledgements
The authors thank the participants and the home care agencies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the Agency for Healthcare Research and Quality (AHRQ) Grant # R01 HS024537. The content is solely the responsibility of the authors and does not necessarily represent the official views of AHRQ.