
Abstract
The problem of overburdening is increasing among informal caregivers. Some attention has been paid to relationship factors, positive effects of caregiving, and coping strategies in relation to caregivers’ perceived burdens, as these factors might make valuable contributions. The aim of this study was to thoroughly explore the views, experiences, and interpretations of informal caregivers with regard to these factors, who lived in the southernmost part of the Netherlands. In this qualitative case study design, 26 informal caregivers were interviewed using a semistructured questionnaire. The respondents indicated that having a good relationship with the care recipient, experiencing positive effects of providing care, and using coping strategies reduced their burden. In the future, longitudinal research is warranted to determine the actual contribution of these factors.
Introduction
Recent changes in society, such as the objective of developing a “participatory society” to reduce citizens’ dependence on the government, have led to a greater emphasis on the possibilities for citizens to support each other.1,2 A good example of this trend is informal care. Informal caregivers are unpaid nonprofessionals, such as family members, friends, or neighbors, who support chronically ill, disabled, and other people in need in their immediate environment over a lengthy period of time.3-5 Although positive effects of caregiving have been described, negative effects on the physical and mental health and the quality of life of informal caregivers are known to occur as the intensity of the provided care increases.6-11 Caregivers are increasingly perceiving a high burden, which is an important indicator of future health decline. 12
Understanding this trend requires more insight into the determinants of a high perceived burden. It has been assumed that the perceived burden and possibly the physical and mental health outcomes of informal caregivers can be explained by the specific combination of a caregiver’s background characteristics, for example, context and personal characteristics; their stressors, for example, role strains, relationship factors, and psychological strains; and any mediating factors, for example, coping resources. 13 Recently, more information has become available about most of these characteristics of caregivers in relation to the level of perceived burden. 14 Although the importance of relationship factors, positive effects of caregiving, and coping strategies has been reported,7,8,14 few studies have examined the possible influence of these factors on the perceived burdens.
Regarding the fact that informal care becomes more important nowadays and that the problem of overburdening among informal caregivers has been increasing, 16 more research is needed to explore the importance of these less studied factors in relation of perceived burdens. This way essential factors can be defined, that may serve as screening criteria to discover burdens and prevent overburdening among informal caregivers. This requires in-depth explorative research to assess caregivers’ views, feelings, and thoughts. The aim of our qualitative case study was to explore information about relationship factors, positive effects of caregiving, and coping strategies as factors influencing the physical or mental burden that caregivers perceive.
Methods
Study Design
A qualitative case study design with semistructured interviews was used to facilitate the understanding of the influence of relationship factors, positive effects of caregiving, and coping strategies on the perceived burden of caregivers within their context. The emic perspective, using an insider focus on the participants’ views, experiences, and interpretations as the starting point, was used to gain in-depth insight about relationship variables, defined as the way in which the caregiver and care recipient regard and act toward each other; positive effects of caregiving, for example, things related to the caregiver role that were perceived as favorable; and coping strategies, for example, techniques that caregivers used to handle the informal care, in relation to perceived burdens. 17
Study Participants, Recruitment, and Data Collection Procedure
A purposive sampling procedure was used to include a variety of informal caregivers. Information regarding the characteristics and care recipients of informal caregivers willing to participate was used to include them in the study and obtain a complete overview. The recruitment of participants was facilitated by cooperation between Maastricht University, the Municipal Health Service Southern Limburg, and the Expertisecentrum Mantelzorg (Dutch Expertise Centre for Informal Care). An advertisement was placed in the newsletter of the platform Mantelzorg (Platform Informal Care); emails were sent to informal caregivers by these three support agencies for informal care and by municipal authorities in Southern Limburg to recruit adult or elderly informal caregivers who were providing care or had provided care within the last year. Telephone and email contacts were used to schedule 26 individual interviews, at the participants’ home or at a public location, between the end of April and mid-May 2016. Before each interview, an informed consent form was signed after the researcher had introduced herself and explained the purpose, content, and procedure of the interview. During the data collection process, the interviews were summarized to highlight the most important findings. Based on this information, it was decided that the data saturation point had been reached after 26 interviews, as no new information was being put forward and participants started to repeat information. Ethical approval for this study was not required under Dutch law (Central Committee on Research inv. Human Subjects). For this study, analyses of anonymous data were used according to the Code of Conduct for Health Research of the Dutch Federation of Biomedical Scientific Societies. 18
Content of the Interviews
The interviews were semistructured, individual, with open-ended questions (Appendix A). After explaining the content and procedure of the interview and signing the informed consent, the interviewer started by collecting background information, for example, age, gender, household composition, education level, and work. Next, the four main components explored in this study were discussed: relationship factors, perceived burdens, positive effects, and coping strategies. First, participants were asked to describe their relationship with the care recipient. They were asked for whom they were providing care, the condition of the care recipient, the duration of the care and the number of hours per week, whether they were living with the recipient, the actual activities they provided, and their relationship with the care recipient. The second group of questions concerned the perceived physical and mental burdens in daily life resulting from the informal care provision task. The third group examined the positive effects of providing informal care on the life of the respondent. Finally, the respondents were asked about their coping strategies to reduce their perceived burdens.
Data Processing and Analysis
The notes and recordings of the interviews were analyzed using an interpretative phenomenological analysis approach. This approach was used because the providing informal care was defined as a starting point. The information caregivers provided with regard to their relationship with the care recipient, the positive effects of caregiving they experienced, and the coping strategies they used offered insight into the way caregivers made sense of their perceived burden in a given context.19,20 The data were analyzed using an Excel file. The analysis started with open coding to identify, name, and categorize the predefined components or subcomponents of the semistructured questionnaire into main themes (Appendix B). These codes were used to discover similarities and differences. Based on this information, all components discussed in the interviews were related to the perceived burdens of caregivers to find patterns in the data.
Results
Description of the Sample
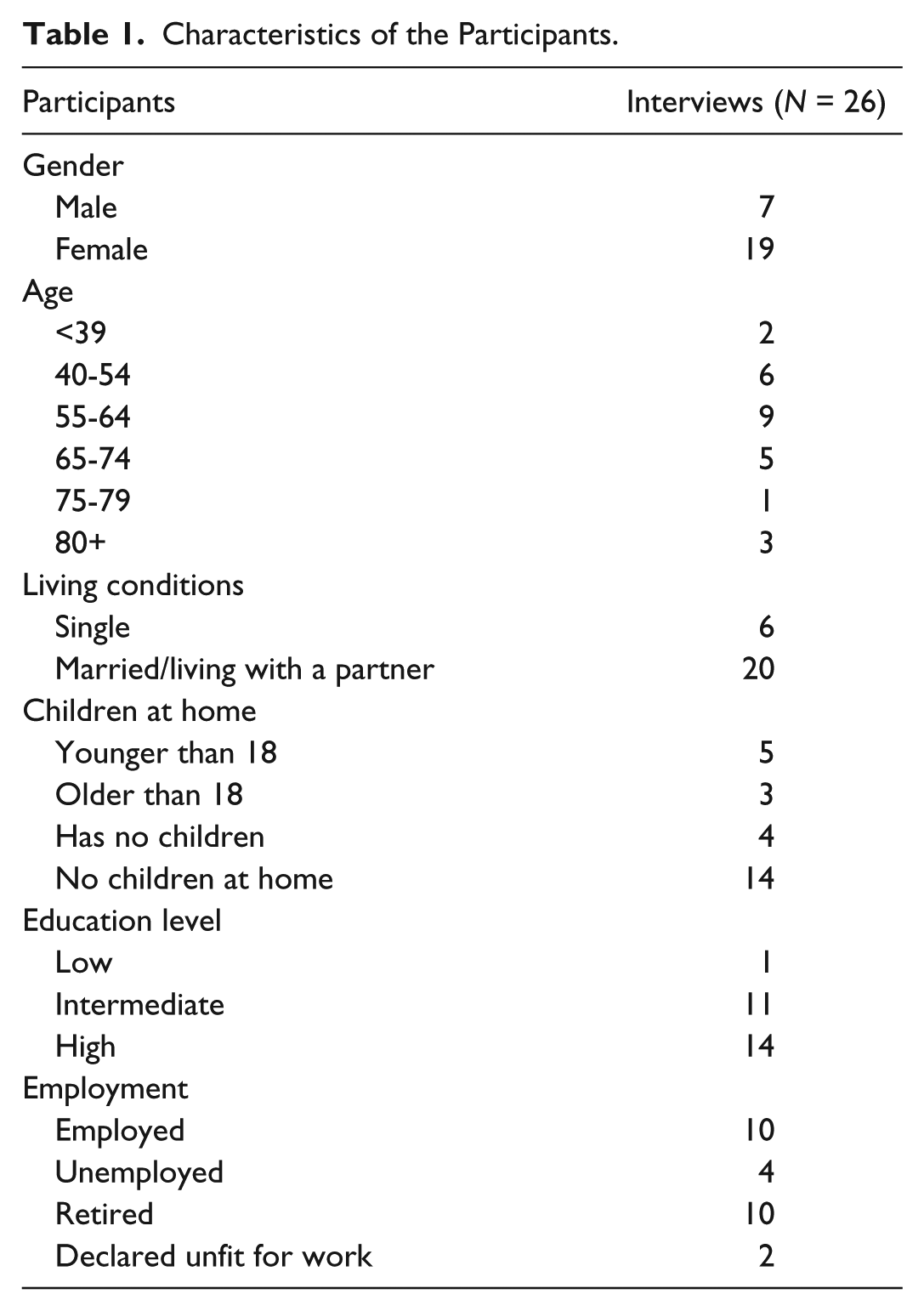
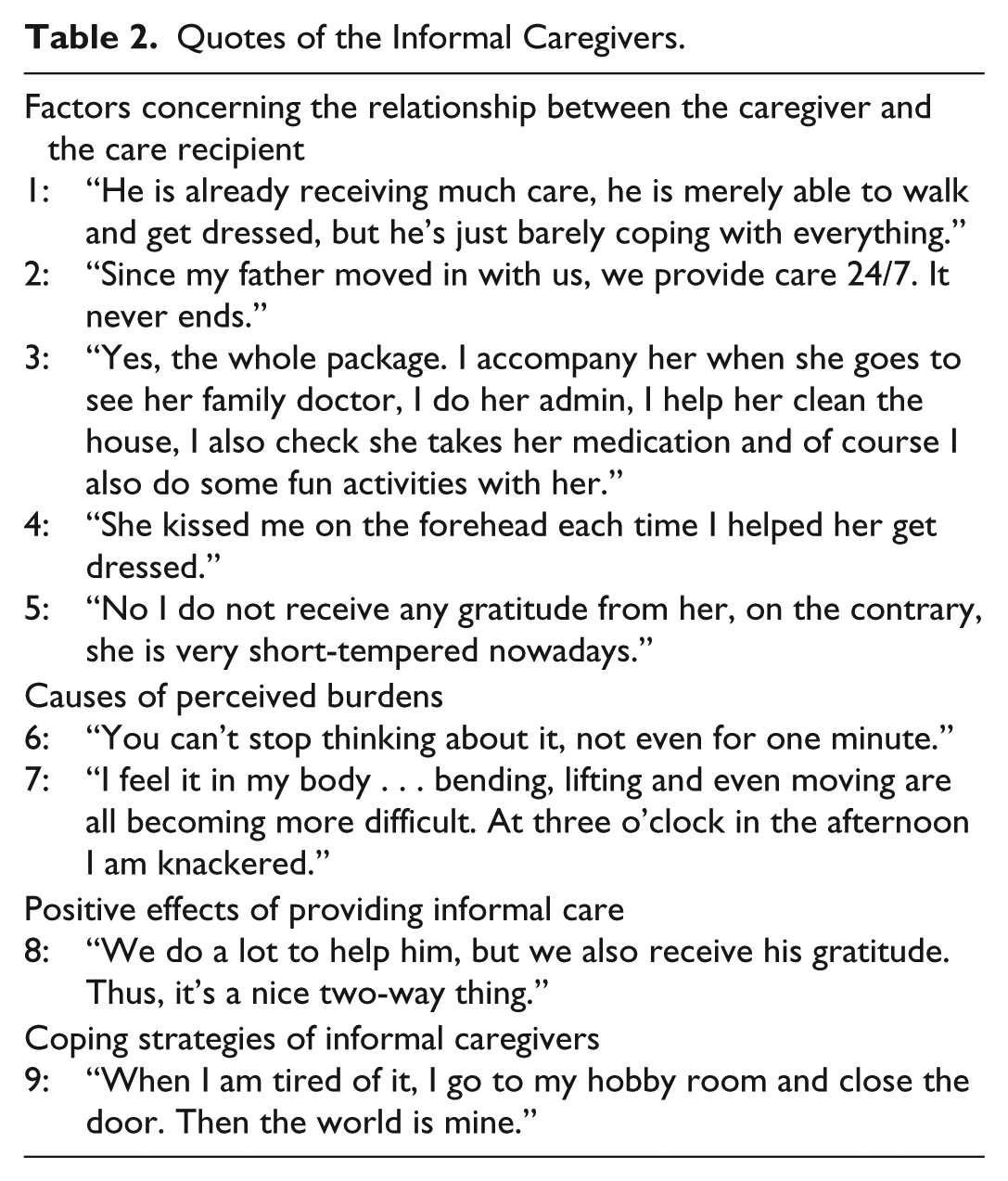
The majority of the participants was female and had an average age of 60 years (range, 29-83). Caregivers who perceived the highest burdens were aged between 40 and 54 years. Most of the informal caregivers were living together with a partner and had no children living at home. The majority of the respondents had a high educational level, and ten participants currently had a paid job (see Table 1). Table 2 provides an overview of the quotes belonging to the main themes.
Characteristics of the Participants.
Quotes of the Informal Caregivers.
Factors Concerning the Relationship Between the Caregiver and the Care Recipient
Most respondents were providing care to a family member, especially immediate family like parent, partner, or child. Others provided care to more distant family members, friends, or neighbors. Four of the respondents were supporting multiple people in need. Most care recipients were aged 60 or over, with twelve recipients aged above 80. Six care recipients were younger, with only four children under the age of 16. Three respondents reported that their care recipient had recently died. Most respondents were supporting a recipient with a physical condition, for example, cancer, cardiovascular diseases, lung diseases, physical disability, or limitations due to advanced age (quote 1). Twelve respondents provided care to people with a mental condition, mostly recipients with a form of dementia.
Most caregivers had provided care for a lengthy period of time, with sixteen respondents having provided care for more than 5 years. Only two respondents had provided care for less than half a year. About half of the respondents were providing care for more than 16 hours a week (quote 2), while only two were providing care for less than 5 hours a week. Half of the respondents were living together with their care recipient, while in other cases, the care recipient lived independently with professional support, or in sheltered housing or a care or nursing home.
All respondents provided practical support for the care recipient, for example, groceries, housekeeping, chores at home or in the garden, laundry, preparing meals, taking care of administration, and coordination of care and transport. All caregivers provided emotional support. They visited or called the recipient, kept them company, and undertook pleasurable activities with them. Six participants who provided care to persons with physical limitations or decreased independence reported that they were having to deal with depressive symptoms of the recipient. Finally, twelve respondents were providing some personal and medical care (quote 3). Four participants helped with medication intake, while others provided full care, including help with bathing and getting dressed. Fifteen respondents shared the care activities with a partner, parent, brother, sister, child, or cousin.
Twenty respondents mentioned that the care recipients showed appreciation for their support, by saying they were grateful or that they would not know what to do if the caregiver did not help them. Participants mentioned that their care recipients enjoyed their presence and gratitude was expressed by a hug or a kiss (quote 4).
Six respondents, including the caregivers who supported a person with dementia, one caregiver of a chronic obstructive pulmonary disease (COPD) patient and the caregiver of a recipient with a slipped disc, reported that they were not receiving any appreciation from their recipient (quote 5). Some of them explained that the care recipient found this a normal thing to do, but most said that the patient was too ill or their personality had changed due to their disease.
Causes of Perceived Burdens
Nineteen respondents reported some form of mental burden, four of whom perceived extremely high burden and explicitly mentioned that not being able to share the burden and not being supported by family, friends, colleagues, or professionals increased their burden. Other potential causes mentioned were a lot of planning and coordination activities, constantly thinking about the care for the recipient, being afraid that something might happen when they left the recipient alone, frequently keeping an eye on the recipient, and worries about how to move on if the care recipient should die (quote 6). Seven participants stated that they did not perceive a mental burden, as they were able to take their mind off the care activities, made strict appointments for their support, visited the recipient in a care center where everything was arranged for them, and had got used to the situation and accepted it.
In addition to perceived mental burdens, twelve participants perceived a physical burden from their care providing tasks. They reported feeling tired because of the intensity of the care. Some participants reported health complaints, such as fibromyalgia, dizziness, headache, pain during care activities, muscle tension, or exacerbation of existing disease (e.g., eye disease, tinnitus, bowel disorder, and cardiovascular disease) (quote 7). Fourteen participants perceived no physical burdens due to the caregiving task.
Positive Effects of Providing Informal Care
The respondents reported not only negative consequences of informal care provision; twenty-one of them reported some positive effects of providing informal care on their lives. Three main influences were mentioned. The first was that it had improved their self-image. They described a learning process that enriched their lives, including enhanced self-confidence, self-knowledge, empathy for others, and a more realistic view of life. The second influence was that the care provision tasks gave meaning to their lives. They felt that they contributed to the quality of life of the recipient. Finally, respondents reported improved social cohesion. They often mentioned a closer relationship with the care recipient, family, friends, and/or neighbors, but also appreciated the new social contacts they built up through their care provision tasks (quote 8). Only five participants did not indicate any positive effects.
Coping Strategies of Informal Caregivers
Twenty-four respondents used coping strategies to alleviate their perceived burdens. The most commonly mentioned strategy was seeking some form of diversion, for instance, through short holiday trips, hobbies or relaxation techniques, volunteer activities, work, and babysitting the grandchildren (quote 9). Five participants received support from their own existing social network, which relieved their burden, while five others had obtained help from professionals. Six caregivers insisted on a living situation with supervision, alarm, and professional support for the recipient, which made them feel more at ease and made it possible to set specific appointments for care provision and to prevent anticipated problems. Two respondents used no coping strategies, as they mentioned that no support from others was available and leaving the care recipient alone was no option.
Discussion
This study explored informal caregivers’ opinions, feelings, and thoughts about relationship factors, coping strategies, and positive effects of caregiving, to assess the relevance of these factors regarding perceived burdens.
The relationship factors we explored were those which appear to be important to explain the perceived burdens of informal caregivers, as reported by Pinquart and Sörensen 6 and Schulz & Sherwood. 7 Part of the burdens perceived by the caregivers might be explained by variables of the care recipients, such as their condition. Caregivers supporting recipients with mental conditions, for example, dementia in a relatively advanced stage, and recipients with serious physical conditions and in need of palliative care, seemed to perceive a higher burden. Pinquart and Sörensen 6 explained this by inspecting three aspects of the care recipient’s impairment, namely, the levels of physical impairment, cognitive impairment, and behavioral problems. The described care recipients often have a relatively high level of these impairments, and the increasing behavioral problems in particular are difficult to deal with for caregivers.7,9,21 The caregivers we interviewed who spent more hours per week providing care and did more tasks for the care recipient reported perceiving a higher burden. This was more common when caring for recipients with mental conditions and serious physical conditions, because they need more intensive care. Andrieu et al 22 explained that it might be especially the content of the task which is important in explaining the perceived burdens, as caregivers providing personal/medical care may feel uncomfortable or unable to do this, which we also noticed in our interviews with the caregivers. Furthermore, caregivers who provided the care on their own and caregivers coresiding with the care recipient reported a higher burden, probably because they reported providing care 24/7 without having a break. 14 Finally, the gratitude received for their support from the care recipient, family and friends might be a very salient relationship factor. In line with what was found by Cormac and Tihanyi 9 and Ratcliffe et al, 23 caregivers of recipients expressing no gratitude reported a higher perceived burden in the interviews. This was most common among caregivers supporting recipients with dementia or serious physical conditions.
Positive effects of caregiving seemed to be helpful in reducing the perceived burdens. In accordance with what has been reported by the Expertise Centrum Mantelzorg, 8 our participants mentioned a sense of meaningfulness and satisfaction in their lives, and rated themselves more positively. 24 In addition, the caregivers appreciated the close relationship with the recipient and described a learning process that enriched their lives, where they experienced pride and efficiency in their abilities to handle difficult situations and crises. This was also reported by Pinquart and Sörensen 6 and Schulz and Sherwood 7 who found that caregivers learned new skills and found out more about themselves and their capacities. Caregivers who notice these new insights into their own capabilities and perceived an enrichment of social cohesion might be better able to cope with the more stressful aspects of their informal care provision. 25
Coping strategies seemed to reduce perceived burdens. The caregivers with a confrontive coping style, those who found ways to take their mind off their caregiving tasks, those who received social support from their own contacts or professional contacts, and those who insisted on a supervised living situation for their recipients expressed a lower perceived burden which is in line with the findings of different studies.13,14,26,27 Caregivers said that coping strategies gave them some time to relax and stop thinking about the care they provided for a while. Thus, it seems to be important for caregivers to have some breaks from their caregiving tasks.
Altogether, it should be indicated that having a good relationship with the care recipient, experiencing positive effects of providing care, and using coping strategies are important to reduce the caregiver burden.
Strengths and Limitations
A major strength of this study is the relatively large number of informal caregivers we interviewed, which yielded a representative picture with a high level of data saturation. 28 The open character of the interviews yielded more in-depth insights into the underlying causes of the importance of relationship factors, positive effects, and coping strategies regarding their perceived burdens. 29
Besides these strengths, some limitations should be acknowledged. First, the sample was based on a purposive sampling procedure among voluntary informal caregivers. The possibility of selection bias may have meant that some categories of caregivers, in terms of characteristics like age, gender, or education level, were underrepresented. However, the group of caregivers we interviewed was sufficient for this explorative study, as the aim was to examine the possible importance of relationship factors, coping strategies, and positive effects of caregiving. Second, the data source consisted of self-reports by the informal caregivers, which is attended by an increased risk of information bias. Caregivers might not be willing to share the burden they perceive, which may have led to inaccurate or socially desirable answers, and probably to an underestimation of the actually perceived burden among caregivers.30,31
Recommendations for Future Research and Practice
All variables we examined might be important to explain the perceived burden of caregivers. The study by Prevo et al 15 already found some associations between characteristics and the perceived burdens. Substantiating those findings and the results from the present study requires a longitudinal study to determine the contributions of characteristics to the perceived burdens. If the importance of some characteristics can be confirmed, these may serve as screening criteria to prevent high perceived burdens and to identify opportunities to provide tailored support to informal caregivers.
Conclusion
This study showed that relationship factors, positive effects of caregiving, and coping strategies should be taken into account when determining the burden perceived by informal caregivers. A first step is presented by exploring these factors, but in the future, longitudinal research is warranted to determine the actual contribution of these variables to the perceived burdens of informal caregivers.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.