
Abstract
Orthodontic tooth movement allows clinicians to modify tooth position and functionality using a mechanical stimulus, which makes reliable mechanical models highly beneficial for predictive tasks and virtual parameter studies. Several individual advancements over the last few decades have identified challenges within this system of multiple constituents. This work aims at providing a thorough review from the mechanical perspective. It specifically reviews and discusses the mechanical boundary value problem in terms of geometry, loads, and material behavior. Characteristic values of the involved loads and material models are summarized. Clinical key features of the treatment process then highlight the link between the mechanical and the clinical perspective, underlining the relevance of variability in patients and treatment. Future perspectives can be guided by practical assessment of model sensitivity, data uncertainty, and the coupling to non-mechanical fields.
Keywords
1. Introduction: relevance and challenges of orthodontic tooth movement and its modeling
Orthodontic tooth movement (OTM) is a crucial aspect of orthodontic treatment, as it enables the alignment of teeth to achieve an ideal bite and ensure the proper function of the temporomandibular joints. By applying controlled forces through various orthodontic appliances, it is possible to correct malocclusions, improve oral health, and enhance overall facial aesthetics. Beyond cosmetic benefits, effective tooth movement also plays a vital role in restoring optimal chewing function, preventing long-term dental issues, and improving speech and breathing [1–3]. Understanding the mechanical processes involved in OTM is essential for refining treatment strategies and optimizing patient outcomes, making it a fundamental component of modern orthodontics.
Given the requirement for reliable predictions for successful OTM treatments, mechanical models and their numerical (in-silico) simulations can be a promising tool for that task [4,5]. Such model predictions must be both accurate and applicable to provide valuable information to the clinician. Several approaches have explored the potential of computational methods coupled with studies in vivo and in vitro [6–11]. This task naturally involves different disciplines such as medicine, biology, manufacturing, and mathematical modeling. Even more so, the processes appear on different length and time scales. Several studies contributed significantly to the successful modeling of OTM but unanimously underlined the need for a further development on a larger scientific scale. Valuable reviews have been provided for this reason on the behavior of the periodontal ligament (PDL) [12,13], as it constitutes a center for the entire OTM process and poses greater challenges for parameter identification due to its small size and complex in-vivo conditions. A clinical view on OTM modeling is provided, for instance, by Tepedino [14] and on the potential of finite-element simulations by Cattaneo and Cornelis [6].
The present analysis aims at contributing to this goal by reviewing the OTM process from the viewpoint of mechanical modeling. This specifically implies the definition of the boundary value problem that is necessary to setup and to evaluate a model and its numerical simulation. The individual investigations of geometries, load conditions and the material behavior are collected to establish a novel and accessible connection between the mechanical modeling perspective and the clinical conditions of the OTM problem. To be more precise, the highlights of the present review analysis are:
Review of the OTM boundary value problem for mechanical modeling;
Classification by geometry, load, material properties, and methodology;
Analysis of 78 publications from the years 2000–2025 plus further references;
Summary of characteristic values for a representative OTM boundary value problem;
Clinical key properties in the patient treatment process;
Established modeling options and future perspectives.
The review of the OTM boundary value problem starts in Sec. 2 with an introduction to the overall system as well as mechanical descriptions from clinical practice and history. The subsequent tabular classification allows for a detailed comparison of geometries, loads, material properties, and methods before they are discussed quantitatively and qualitatively. Subsequently, Sec. 3 summarizes a characteristic system with established modeling features. Clinical key properties shall moreover provide a link to the patient treatment process and open the discussion on future perspectives, before Sec. 4 concludes with the main findings.
2. The boundary value problem of OTM
2.1. Overview and composition of the OTM system
The system of the OTM process involves three main constituents: the tooth, the surrounding alveolar bone, and the PDL in between (Figure 1). These constituents can be subdivided further, depending on the desired level of detailed functionality and length scale. The tooth, for instance, is composed of its root, crown, and the inner pulp, which are made of different tissues: connective tissue, dentine, enamel, and radicular cementum. The alveolar bone region can be divided into cancellous bone, cortical bone (outside the sketch section), and the socket wall, which is a porous layer of bone that encases the dental root and its PDL. Moreover, the gingiva may be considered on top of the bone. The PDL contains fibers of at least four different types, classified by their spatial orientation: transeptal, horizontal, oblique, and apical.
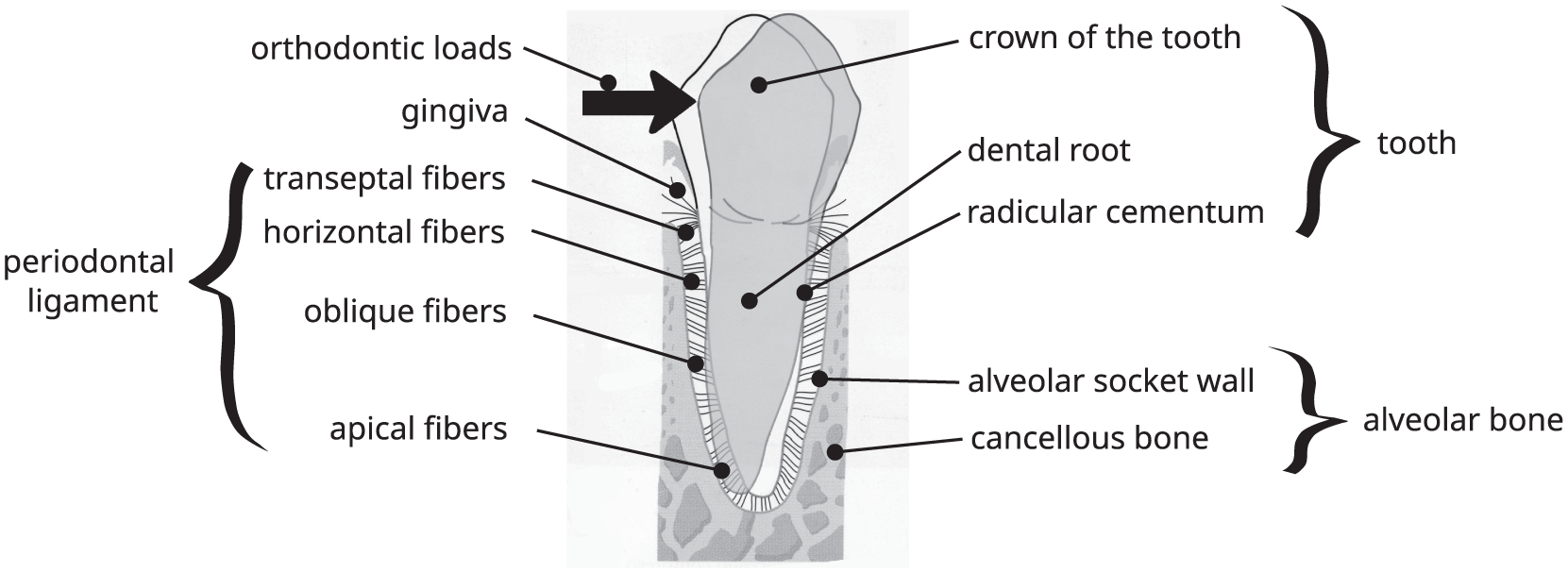
Schematic sketch of the OTM system.
The OTM process typically involves the application of external mechanical loads, e.g., forces and/or angular momentum, via braces, aligners or removable appliances. Its duration can span several weeks [15] with four characteristic phases. During the first phase, the tooth is simply displaced within the alveolar socket due to the damping function of the PDL. During the second phase, strains in the extracellular matrix are transmitted to cells, which are thus triggered and activated. This yields to the ultimate and third phase of tissue remodeling with slow persistent tooth movement. However, a fourth and intermediate lag phase called “hyalinization” should be considered because the initial forces in the clinical setting are usually sub-optimal. Hyalinized (necrotic) tissue can develop due to bloodflow shortage and tissue hypoxia, which is removed by macrophages before further movement can occur. This lag phase, as could be easily anticipated, usually slows down the overall OTM process.
Patient variability should be noticed distinctively when quantitatively evaluating OTM models. The behavior of the involved materials or the geometry [16,17] can highly depend on the individual patient. While correlations are possible, for instance, with age or health status, we cannot fully exclude all uncertainty. For a patient-specific treatment, on one hand, this may be approached as epistemic uncertainty that can be reduced by a preventive medical check-up or online monitoring. For the development of appropriate material descriptions or general risk analysis, on the other hand, patient variability may be accounted for as aleatoric uncertainty [18–20]. Even more so, geometrical and material behavior can depend on many more factors such as the exact location, the time of day, nutrition, hormone level, or medication. Quantitative references must, accordingly, be considered as snapshots for calibration and validation.
2.2. Mechanical descriptions and terms from clinical practice
Before we continue with the mechanical boundary value problem, we find it helpful to summarize some descriptions and terminology that were established during decades of clinical research and treatment. This can be helpful for the remainder in two ways. First, it helps to understand the context of terminology that is not always a rigorous one-to-one mapping between the disciplines involved. Second, descriptions often originate directly from practical observations and hence reflect the parameters that are accessible for observation and treatment in daily practice.
In vivo/in vitro and in silico studies can typically be rephrased as experimental and numerical studies (or simulations), respectively. Special care should just be given to the fact that the medical viewpoint often shows a more granular classification for experimental investigations, e.g., in vivo (on the whole living organism) versus ex vivo (typically isolated cells)/in vitro (in a laboratory environment) or human versus non-human material. In contrast, numerical studies, or in silico ones, are often classified in more detail from the mechanical viewpoint, e.g., mesh-based methods (including finite element simulations) versus mesh-free methods (such as particle-based methods) versus data-driven approaches (such as artificial neural networks).
Bodily movement, tilting, tipping, uprighting, intrusion, extrusion, translation, and rotation are descriptions of the tooth movement that can often be interpreted in a mechanical context. These terms, however, can require a context of the underlying study, because they may be only qualitative descriptions or refer to a specific axis or direction of the system at hand [21].
Center of rotation and center of resistance derive from the simplified tooth motion, see Figure 2. The center of rotation describes the reference point of the tooth that shows only rotation but no translation, assuming a rigid body motion to be well defined. The center of resistance (CR) is difficult to define uniquely in a mechanical context, because its definition can differ among research works [21–24] and does not always derive from a well-defined mechanical context [25,26]. Definitions range from a point of an applied force that allows bodily movement, to the point of the greatest resistance or a geometric definition when idealizing a parabolic tooth geometry and stress distributions [27].
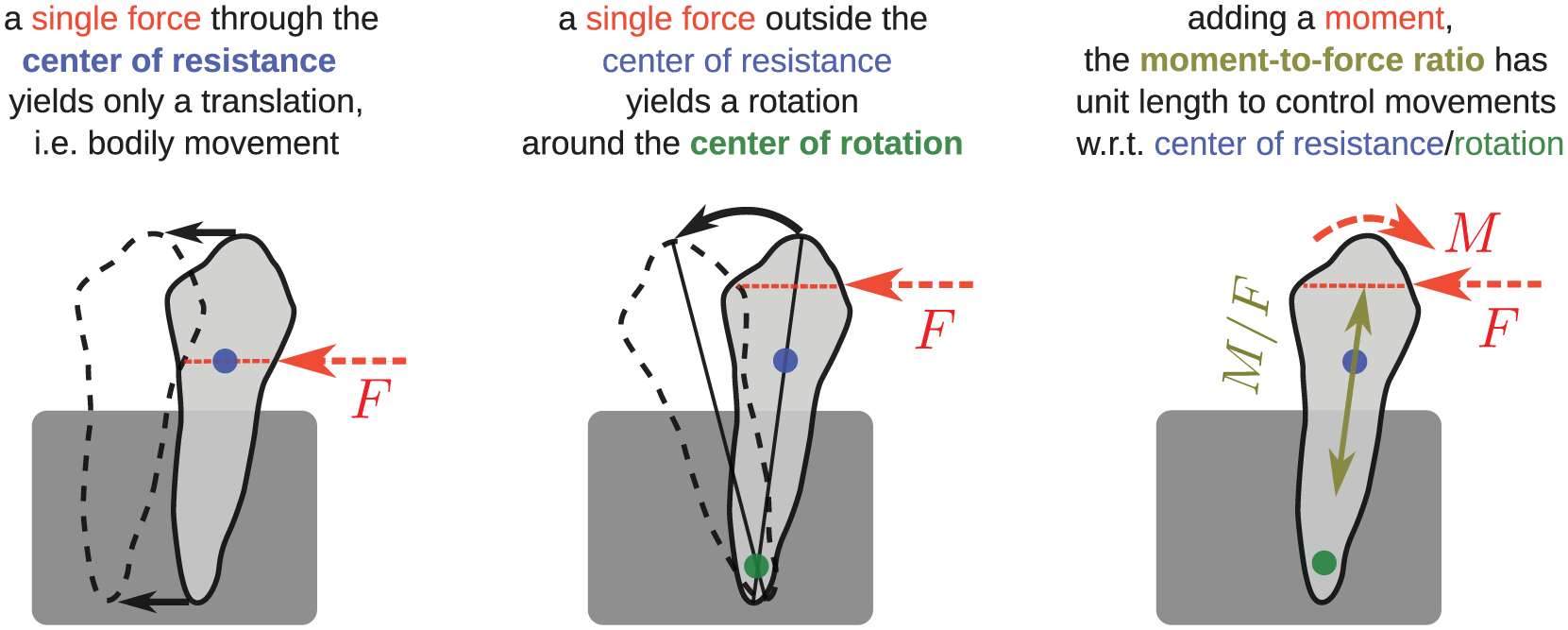
Sketch of the center of resistance (blue dot), center of rotation (green dot), and the moment-to-force ratio (double arrow, olive-green line).
Moment-to-force ratios,
Stresses and strains refine the characterization by forces and angular momentum to a more precise description of fields acting within the entire system. Being second-order tensors, stresses
Historically, several theories have been proposed to describe the major driving factors for OTM. Schwarz proposed in 1932 the so-called “pressure-tension theory” [34] based on the previous work from Sandstedt [35,36] and Oppenheim [37,38]: when a force is applied, the tooth is first displaced within its bony socket, then the tension on the bone exerted by the stretched PDL fibers on the side of force application stimulates bone formation, while the PDL compression on the opposite sides reduces the blood flow and causes hyalinization, necrosis, and bone resorption. Later, this theory was modified by Melsen et al. [39,40] to conform to Frost’s [41] mechanostat theory and to the anisotropic behavior of the PDL fibers: on the same side of force application, stretched PDL fibers load the bone with tension stimulating new bone formation, while on the opposite side, the slack PDL fibers are no longer able to transmit forces to the bone, and this unloading leads to bone resorption. On the other hand, Baumrind [42] proposed a different explanation, suggesting that the main driving factor should be the deformation of the bone structure. Indeed, the alveolar bone can be deformed more easily than the PDL itself and such a strain leads to the formation of “stress lines” that regulate bone remodeling. Other authors [43] and more recent findings [44,45] suggest that also the fluids present in the PDL vessels and extracellular matrix, with their flow secondary to applied pressures, represent an important stimulus for the regulation of bone remodeling during OTM. None of the described theories alone is able to completely explain the phenomenology of OTM, suggesting that further studies are still needed to achieve an in-depth understanding of OTM. This situation is also reflected in the discussion of mechanical modeling features.
2.3. Tabular overview and classification of the BVP
The following Table 1 classifies the main characteristics of OTM models in literature along geometry/object, loads/boundary conditions, material behavior, experimental/numerical methodology, and further notes. The 78 reference works are ordered by ascending year and author name, respectively. From the perspective of mechanical modeling and because of the variety of material models and geometries, we found it helpful to list a brief description in addition to characteristic numbers. The latter are rounded values to serve as a first and concise reference, but variations are possible. Several of them are, moreover, adopted from other sources, and we refer to the textbooks referenced in the introduction above and in the literature sources themselves for more detailed information on the materials. A detailed analysis of tooth or PDL material alone, for instance, would exceed the scope of the present work. We also refer to the brief historical context and termini presented in the previous subsection for a wider range of seminal papers in the past decades. The entries in Table 1 have been chosen on the basis of recent review articles such as Tepedino [14] and Ovy et al. [12], cross-references as well as a web-of-science data base title-search for “OTM model”(s). Without further judgment of individual relevance, purely non-mechanical or non-OTM -related studies have been omitted as well as redundant or only implicitly related publications, which then may have been considered in the notes as possible.
Tabular overview of modeling approaches for the boundary value problem of orthodontic tooth movement.

Characteristic values are provided as first indicators and variations may of course appear. If not otherwise noted: E is Young’s modulus (in MPa), G is shear modulus (in MPa), dito
2.4. Geometry
The geometry of the OTM problem is generally well captured by (µ)CT scans. The resolution reaches voxel sizes between approximately 37 and 600 µm [28,31,49,56,97] with optional information on densities and ongoing technical improvements. In addition, the size of the analyzed section varies from an isolated material point behavior [30,59], to a section of the PDL (few mm), very often a single tooth (few cm), parts of maxilla or the mandible [31] or a greater portion of the skull (order of 10 cm) [94]. The consideration of tooth-tooth contacts and daily operational loads benefits from models that include larger volumes. The importance of a holistic approach in practice was underlined in, e.g., Schmidt et al. [90] and reflected by the natural frequency response by Liao et al. [78]. A challenge remains by the fact that not all data is freely available. Idealized geometries [7,47,71,76], in contrast, allow us to analyze isolated effects or trends for the preparation of more precise guidelines and models. Recent investigations especially focused on the PDL geometry with uniform thickness being a common assumption (median
2.5. Boundary, initial, and contact conditions
The loads used for appliances in OTM are also well documented and based on practical experience. Typical loading scenarios could involve single forces F ranging from 0.3 N to 2 N, with 1 N (
Modeling multiple teeth [84,90] also requires a definition of contact conditions. These are realized by either perfect bonding (e.g., PDL-tooth and PDL-bone by Ammar et al. [53]), frictionless contact (e.g., teeth-aligner by Savignano et al. [9]) or friction coefficients (e.g., 0.2 for occlusal contacts by Ortún-Terrazas et al. [31], 0.2 for bracket slots-archwire by Tominaga et al. [72] and Ozaki et al. [73], 0.3 for tooth-bone and 0.37 for mini-screw bone by Ammar et al. [53]).
2.6. Material behavior
2.6.1. Tooth
The tooth itself is mostly assumed to be linear elastic. It ranks among the materials with the highest elastic moduli of the entire system, which applies to the tooth itself and its components (dentin, enamel, except for pulp). A few studies assumed the tooth to be rigid (< 20 % of cases) for the simulation or in terms of a prescribed deformation with constant shape. Of course, more detailed understanding and models of tooth mechanics are available with connections to orthodontic treatments, for instance, properties on different (multi)scales [121] and anisotropy in finite element simulations [52]. Although the teeth generally show a complex multiscale architecture, it was yet rarely adopted for OTM purposes.
2.6.2. Bone
Bone is also most often considered to be linear elastic, although a viscoelastic model would be more realistic, since it is well known that bone behavior is dependent on loading frequency and timescale. Cortical bone shows larger elastic moduli than trabecular/cancellous bone (by factors of ≈ 10–100) if that distinction is made. A more detailed consideration is found in the form of a heterogeneous elasticity distribution depending on bone density [98]. A rigidity assumption is less common, however, probably because the OTM process involves a remodeling process that alters the bone geometry. Similar to the teeth, bone shows a microstructure that affects its effective mechanical properties, e.g., captured by a second-gradient model in a visco-poro-elastic material with bio-resorbable grafts [122–124]. A consideration of the bone microstructure for OTM processes is found especially by its capability of exchanging viscous fluid with the PDL. Permeability is thus attributed to it in few cases [31,54,99] and allows to capture viscous fluid flow, typically relating to the variables of void ratio or porosity. Similarly, to the material behavior of teeth, bone has been analyzed in great detail outside the OTM context, but we try to concentrate on modeling approaches found against the background of OTM.
2.6.3. PDL
The PDL is located at the origin of the remodeling process and its modeling has been a major focus of recent research. The characterization of the PDL has likely been more challenging than that of teeth and also bones because of its smaller size and rapid change from in-vivo to ex-vivo conditions during handling and unwanted drying. Moreover, the PDL is not necessarily only a thin interface, but a region of finite thickness with a complex microstructure and two adaptive functionally graded interfaces connecting to bone and cementum, respectively [125]. The complex (micro)structure allows for its functionality as a shock absorber, pathogen barrier, and mastication sensor [120] with a variability of the model parameters [126]. A panoply of recent studies therefore focused on mechanical PDL modeling alone.
Linear elastic PDL models are used with a Young’s modulus that is significantly smaller than that of teeth and bones. The reported values cover a wide range between 0.05 MPa (moderate compression), around 0.2–0.7 MPa (moderate tension) and a few MPa (severe tension or compression close to tooth-bone contact) [16,51,52,56,62,64]. When captured as a homogeneous material, the Poisson’s ratio of PDL is often assumed in the range of 0.45–0.49 to mimic incompressibility of this liquid-filled material. Note that this entire range is found as a numerical approximation of incompressibility (especially because near-incompressible behavior poses numerical challenges) and may yield respective variations in derived elastic moduli [107]. Alternatively, it can be modeled by hydromechanical coupling of the poro(visco)elastic PDL matrix and a viscous pore fluid [54,75,99].
Other elastic approaches put effort into employing the PDL’s non-linear behavior. On one hand, the non-linearity is used to capture finite strains, e.g., by hyperelastic potentials [67,70] or Ogden-type descriptions [28,31,61,99,106]. On the other hand, a non-linear elastic description is used to account for the PDL tension-compression asymmetry [48–50,65,74]. This asymmetry is already motivated by the fiber-reinforced structure of the PDL in a few cases [30,31,71]. The pore fluid also motivated the analysis of viscous effects that have been reported on characteristic (relaxation) time scales between the orders of 0.1 and 100 s [17,30,58]. The breakdown of PDL material is also characterized [30] but is usually not assumed for OTM loading scenarios.
2.6.4. OTM appliances
Appliances in OTM such as braces are often made of metals and therefore show a comparable high elastic stiffness. This does not necessarily imply negligible deformations, though, because thin elements such as wires can still show significant bending [11]. Most of their models are restricted to a linear elastic description [64,75]. Another category of orthodontic appliances are clear aligners, removable appliances made of thermoplastic polymers or 3D printable resins. Due to their viscoelastic behavior and the lack of knowledge regarding the boundary conditions between aligner and dental surface, they have been usually described through a simplistic approach [110].
2.6.5. Bone remodeling
The remodeling process is probably the least understood material behavior in the entire OTM process. It is assumed to finally change the bone structure to adapt to tooth movement with the PDL as a mediating element. The complexity of the bone remodeling descriptions increased steadily [127]. Based on the early concepts of OTM and clinical reports, spring-induced
Turning the view towards more sophisticated evolution laws with local driving forces/variables, they allow for a more time-continuous description within a continuum mechanics stetting. PDL strain magnitude was one of the first such variables used to model tooth movement, e.g., by updating the node positions of the finite element mesh according to a relationship between normal PDL strain and tooth velocity or formation/resorption rate [51,83] or by restoring an initial PDL thickness [84]. It was motivated by the assumption that the PDL deformation plays a relevant role in stimulating the bone remodeling process. The strain energy density is another driving force that fits into continuum mechanics frameworks as a stimulus for the apposition and resorption rate [59,60], via iterative node displacement updates of the bone surface [32] or based on the damage-like criterion with energetic overload and underload conditions around a lazy zone [33,80].
2.7. Methodology
Finite element analysis emerged as a promising tool for OTM investigations [128] and was also successfully applied in other clinical scenarios with viscoelastic tissues such as kinetic loading of the jaw system during chewing [129], fracture in endodontically treated teeth [29], or arterial walls [130]. Decades of development yielded numerically efficient commercial and open-source codes that can consider several different material models and OTM-specific requirements. The latter include contact of biological parts and appliances [84], PDL and bone porosity [13], interstitial fluid [31], geometric updates via remeshing or ALE and internal variables to capture changes in biological phases [32,33,80]. The finite element frameworks are complemented by approaches of reduced order [92,93,112], simplified geometries [102], simplified rigid-body equilibria [90,97], or (semi)analytical solutions [68,76,100]. Reducing complexity, for instance, allowed for faster evaluation and a wider range in parameter studies. Another alternative emerges from the recent trend of data-based methods, e.g., in the form of superimposition [131,132], which benefits from an increasing data base of clinical treatments.
Due to the abundance of experimental designs in orthodontics, the present work just distinguishes two main sources for OTM. On one hand, monitored treatments are close to the clinical view on the OTM process and indicate measurements that are available during treatment [55,131]. On the other hand, experiments are especially designed for model calibration and validation [52,54]. The tooth and bone parameters are, moreover, also found outside the OTM context.
2.8. Coupling with non-mechanical fields
It is very likely that a mechanical model is required but is not sufficient to provide a reliable prediction of the OTM process. While the starting problem is driven by mechanics at first sight (input: mechanical stimulus, output: tooth movement), multiple other fields interact during the entire process [133]. Although significant contributions have been made towards their understanding, quantification remains an ongoing challenge. Thus, a connection between the mechanical problem and other involved processes should be established.
George et al. [87] indicated four densities—osteoblasts, osteoclasts, oxygen, and glucose—to govern OTM bone remodeling. This is explained by activation of cell proliferation through oxygen variation in the PDL. Bone remodeling occurs with osteoblast proliferation and an increase in oxygen under ligament tension, while resorption occurs with osteoclast proliferation in hypoxia under ligament compression. Mechanical tension can accordingly induce oxidative stress that could affect cellular behavior during OTM [134]. Fibroblasts in human PDL can adapt to environmental changes and modulate bone remodeling as well as inflammation and regeneration [135]. These processes then affect tooth attachment, loosening, and inflammatory root resorption. Moreover, immune cells such as macrophages can play an additional mediating role in OTM [136]. Mechanical PDL compression during OTM can have a mechanotransductive effect on compressed cells and reduces oxygen supply blood vessel compression, triggering multicellular pseudo-inflammatory processes and their regulation. Mechanical compression can also stimulate pro-inflammatory expression [137], possibly relating the complex biological processes of modulating phosphorylation to an effective mechanical state of damaged cells. The volume-averaged hydrostatic PDL stress is also discussed as an OTM indicator, whereas a universal
3. Established modeling features, clinical key properties, and future perspectives
The previous detailed review shall be summarized in the form of established and extended modeling features. They are sketched in Figure 3 that is based on their frequent occurrence in the literature review. Note that their frequency and commonness are also affected by the evolution of numerical and experimental techniques and do not always necessarily imply a recommended procedure. Clinical key properties will then reflect on their connection to patient treatment strategies and lead to the discussion of future perspectives.
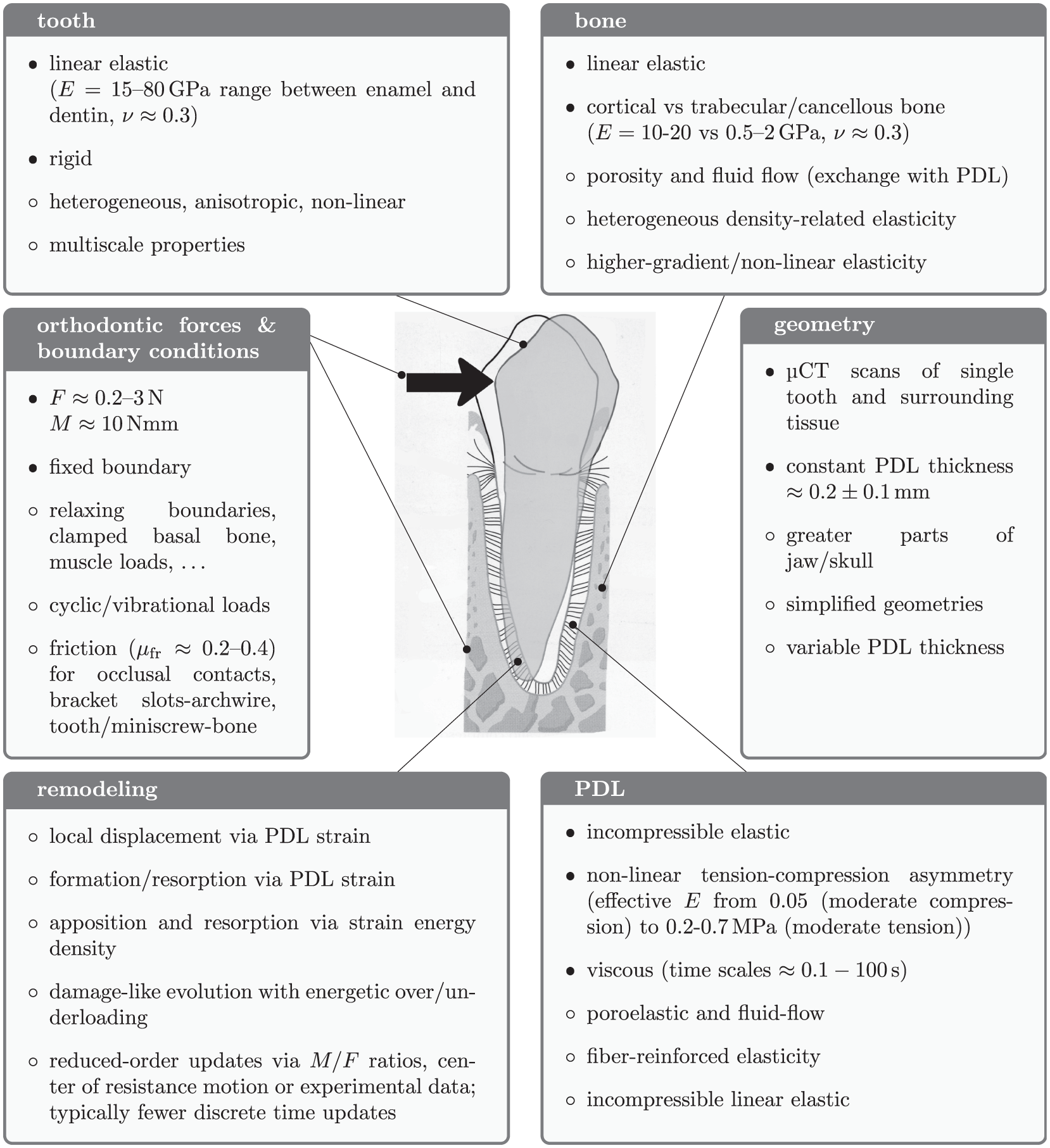
Most common modeling options for the OTM boundary value problem as summarized from the present literature review.
3.1. Established modeling approaches and optional extensions
The individual elastic models for the tooth, bone and PDL are well established. While teeth and bone are often modeled by a linear elastic, isotropic approach, the PDL can also be captured by a tension-compression asymmetry and as an incompressible homogenous material. Also their geometry is reconstructed with resolutions that can approximate the PDL thickness with at least a few voxels. The boundary loads of OTM appliances are also well characterized.
Optional modeling features are a valuable contribution to the mechanical description and may increase its accuracy—their impact on the OTM process is yet unclear. PDL viscosity, poro-elasticity, and interstitial fluid typically affect the mechanical short-term response at the first few seconds to minutes, but the loads in long-term OTM treatments occur over a few days or weeks. All constituents also clearly have a microstructure that yields a scale-dependent and anisotropic response. As the PDL is the most compliant part and its strains are used as one indicator for PDL modeling, it can be relevant to capture this effect by structural information based on fiber direction or a volumetric-deviatoric split [65,106]. The effects of anisotropy or graded properties of tooth and bone yet remain unclear for the low OTM forces. The same applies to their non-elastic behavior [64]. At least locally, however, bone resorption may notably increase bone compliance and thus the deformation state surrounding the OTM process or their natural frequencies.
3.2. Clinical key properties
In addition to the mechanical perspective, the modeling and simulation tools must be usable for clinical practice. A few key clinical properties should therefore be introduced to guide the model design.
After a thorough diagnosis involving skeletal, dental, muscular, and functional parameters, an orthodontic treatment plan with clear objectives is drawn. Then, the biomechanics needed to reach such goals and the design of the required appliance are defined. Furthermore, such treatment goals should be reached in the safest, most effective, and most efficient way. In this regard, two main considerations should be made. First, due to the complexity of the human body, almost every medical procedure is followed by a certain amount of side effects, apart from the intended outcomes, and orthodontic treatment is no exception. Adverse effects directly dependent on force application are root resorption, gingival recession, undesired tooth movement, formation of pulpolitis, and loss of dental vitality [141]. Such effects depend—apart from systemic conditions, genetic predisposition, and other local factors-—on the intensity of applied orthodontic force. Indeed, high forces cause harm to the supporting structures of the tooth mainly because the blood supply becomes severely hindered while applying this force [142]. Roscoe et al. [143], for example, demonstrated that the compressive hydrostatic stress could be a good predictor of inflammatory root resorption, because root resorption was observed in areas where such stress exceeded the maximum capillary pressure of 4.7 kPa. The second consideration is that orthodontic treatment should be as short as possible to reduce the risk of side effects, reduce costs, and take maximum advantage of patient compliance, which is limited over long periods. To obtain such efficiency in OTM, the right force system (i.e. the most efficient combination of single forces and moments on every tooth, in terms of modulus and direction) must be used: this prevents undesired movements on the dental reaction units, which would need additional time to be corrected, and keeps the force within the optimal range for a rapid OTM [144]. However, the previously defined “right force system” is not something that can be easily calculated in advance by the clinician because not all patients respond biologically in the same way [145], the biological effect of the orthodontic force depends on the PDL surface onto which it is applied, and the position of the CR depends on root morphology, bone quality, and bone morphology. Therefore, what a clinician usually does is apply the closest guess to the ideal force system, then monitor the OTM over time, and eventually adjust the force to be closer to the desired outcome, which is not very efficient. As a general indication, usually 1–3 weeks are necessary to observe crown movements (i.e. tipping, rotation), 2 or 3 months are necessary to appreciate radicular movements (i.e. torque, uprighting), while bodily movement can proceed up to a rate of 1 mm per month, but great variations can be observed between patients.
Again regarding the force system and its effects, it is easier for the clinician to predict and adjust when the appliance is in a static configuration that allows to determine all the forces and moments involved and to straightforwardly derive the desired and undesired effects. This applies for situations where the orthodontic wire is engaged only in one bracket (where two points of contact can be recognized) and in one single point (i.e. a button or a simple ligature). However, in many situations, this is not possible and in some cases, especially with clear aligners, the complexity of the interaction between appliance and tooth makes it almost impossible to define a predictable force system while the patient is on the dental chair. The previous considerations become particularly important in patients with special conditions, such as bone pathologies or other systemic conditions that interfere with bone metabolism and therefore OTM, where a personalized clinical approach is necessary to calibrate the adequate force system. In such cases, where clinical trials would be extremely costly and complex due to the low prevalence of such conditions, predictive models could provide valuable information to help customize the orthodontic treatment according to the patient’s needs. Moreover, predictive models could help improve our understanding of the phenomenon of OTM and therefore help determine the ideal force system for different treatment outcomes.
3.3. Future perspectives
Given the availability of several comprehensive mechanical models, the next step is suggested not only for their improvement but more for the assessment of their sensitivity. This will help to estimate the importance and need of individual model components for the overall OTM goal. Another challenge arises from the fact that unknown model parameters may serve well for data fitting but not always on a physically reasonable basis. The non-uniqueness of possible model parameters has already been shown in the early exploration of PDL parameters [69]. A sensitivity study will therefore also help to explore sound parameter ranges. In addition, this issue is particularly relevant in biological models, such as those describing OTM, which can be represented using generalized continuum models (see, e.g., [146–150]). Therefore, special care must be taken in the methods used for parameter identification to ensure their physical relevance (see, e.g., [151–156] for some techniques used in those cases).
The coupling of mechanics with other fields is evidently an open question. The available insights indicate that a possible coupling can start between the PDL deformation and osteoblasts, osteoclasts, oxygen, and glucose fields [87]. Basic studies will be required next to approach the governing equations first qualitatively and then quantitatively.
Turning the view to available data, a realistic definition of complete boundary conditions remains an open task. This firstly implies boundaries of the bone if a mechanical model should be set up for a single or a few teeth and their surroundings. Second, contact conditions must be well defined, especially if the treatment affects multiple teeth. Dynamic loads, either through cyclic/vibrational treatment or chewing, talking, and breathing, are another mechanical impact that will need further clarification [157–159].
Further potential for improvement concerns the numerical (in-silico) methodology. A model prediction will benefit from a fully time-resolved strategy without the need for simplified iterative steps. Dot et al. [10] pointed out the still relevant challenge of tracking the evolution in time and the experimental reference data of the changing geometry. This can be achieved by switching from coarse-grained update schemes to local evolution equations, e.g., in terms of apposition and resorption rates or internal damage-like variables with driving forces based on energy densities [33,59,60,80]. Moreover, given the complexity of the models in question, it is highly practical and effective to employ approaches grounded in a variational formulation, which are especially apt for problems involving tissue growth [160,161], fluid interaction in porous media [162–164], or the progression of damage accumulation [165–170].
Another aspect, in the context of OTM, focuses on the refinement of mathematical frameworks that accurately capture dissipative phenomena during the complex interactions within biological tissues. One promising direction is the use of coupled oscillator chains as approximations for dissipative systems, as suggested by numerical evidence by Bersani et al. [171]. These models have the potential to enhance our comprehension of how forces dynamically transmit through the PDL and alveolar bone. Furthermore, incorporating cohesive interface models [172,173] with degrading friction coefficients [174] may improve the representation of the evolving mechanical properties of the PDL under sustained orthodontic load. Furthermore, advanced models of time evolution for wear contact problems [175] could provide valuable information on the long-term adaptation of bone and soft tissues, leading to improved predictions of tooth movement. These approaches collectively offer a pathway to develop more predictive and physiologically accurate OTM simulations, ultimately optimizing orthodontic treatment strategies.
When combining the mechanical and the clinical view, Cattaneo and Cornelis [6] mention the need for a good compromise between accuracy and applicability (in speed and effort) for clinical applications. A fast and reliable prediction is also required for a clinical decision support platform [112]. While finite element simulations can provide a detailed understanding of the underlying processes, they may not be the best option for daily use in treatment, because the setup and evaluation require background knowledge and are not straightforward. They can hence be used to support fast-access alternatives, for example, in terms of reduced-order surrogate models. If efficiency is achieved once, it can even be combined with uncertainty analysis to account for patient variability [176]. This will also allow to derive a data base for emerging data-based approaches [131,132]. Machine learning strategies capture the governing mechanisms not by an underlying model but via the training data, which are costly to generate and can be achieved by the individual models reviewed in this work. Synergies can then be built with future perspectives on the online monitoring and management of orthodontic treatments [177,178].
4. Conclusion
The present work reviewed and classified the literature with respect to the mechanical boundary value problem of OTM, which is a key to the successful prediction of treatment strategies. A major outcome is the detailed classification in Table 1 with respect to geometry, loads, material models, and methodology. The representative system in Figure 3 summarizes the most common modeling options. A standard minimal system consists of µCT scans of a single tooth, the intermediate PDL and the surrounding bone. Forces and moments are approximately between 0.2–3 N (or 20–300 g) and around 10 Nmm, respectively. Loads, just like material and geometric properties, are patient and treatment specific and thus, of course, vary. Isotropic and linear elasticity is a common assumption for tooth and bone, while the PDL is typically incompressible. The latter is sometimes extended by fiber-induced anisotropy, tension-compression asymmetry, or viscosity. Extensions like poroelasticity, multiscale approaches, and interstitial fluids are possible but not widely adopted. Descriptions in modern continuum mechanics frameworks have yet opened the way for time-continuous and thermo-dynamically consistent settings.
On one hand, the current state of research evolved successfully from the mechanically simplified beginnings such as rigid-body descriptions. On the other hand, several individual extensions remain to be fully explored, such as heterogeneous material distributions or anisotropic properties. Refined time-continuous simulations will also enable a better understanding of the individual process evolution. A guide for future perspectives can be specified by three factors. First, some individual mechanical processes may be relevant for the individual materials or time scales but their impact on the OTM process is yet unclear and must be determined. Second, the interaction with non-mechanical fields will be required for a comprehensive understanding and will depend mutually on the simultaneous development of numerical and experimental techniques in bio-medical and chemical analysis. Finally, uncertainty intervals must be considered for practical application and guidelines. These uncertainties can originate from the patients’ conditions as well as from treatment conditions and will benefit from the combination of detailed individual simulations with large-scale data-based analyses.
Footnotes
Acknowledgements
The authors would like to thank Francesco dell’Isola for the fruitful discussions on the understanding and modeling of the OTM process. P.K. would like to thank Ben Mierswa for the careful review of the data collection from the literature.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.