
Abstract
Introduction
Pregnant individuals benefit both psychologically and physically by participating in outdoor activities.
Methods
The authors conducted a narrative review of the available literature to address unique pregnancy considerations for the wilderness adventurer. There is limited evidence behind many opinion-based recommendations on participation in wilderness activities in pregnancy.
Results
As a result, remote or adventurous activities may be considered unsafe or restricted without significant medical literature to support these opinions. The authors reviewed the literature for the best available evidence, including observational studies, case series, limited controlled trials, and extrapolations from physiological data, as well as evaluating expert consensus statements.
Conclusion
This narrative review discusses pregnancy-specific medical concerns related to participation in outdoor adventure activities.
Introduction
Although the benefits of exercise in pregnancy have been well established, the unique setting of activities in the wilderness poses specific risks and benefits for pregnant individuals, for which evidence is currently lacking.1–9 People of childbearing age account for a considerable proportion of participants in wilderness-related activities such as mountaineering, hiking, trail running, skiing, cycling, and water sports. Many individuals participate in wilderness-related activities throughout pregnancy (Table 1).10,11 Despite pregnant individuals’ interest in continuing activities in wilderness settings, there is a shortage of quality information and recommendations on safe recreation in the wilderness. 12
Outdoor Activities Currently and During First Pregnancy by Trimester.
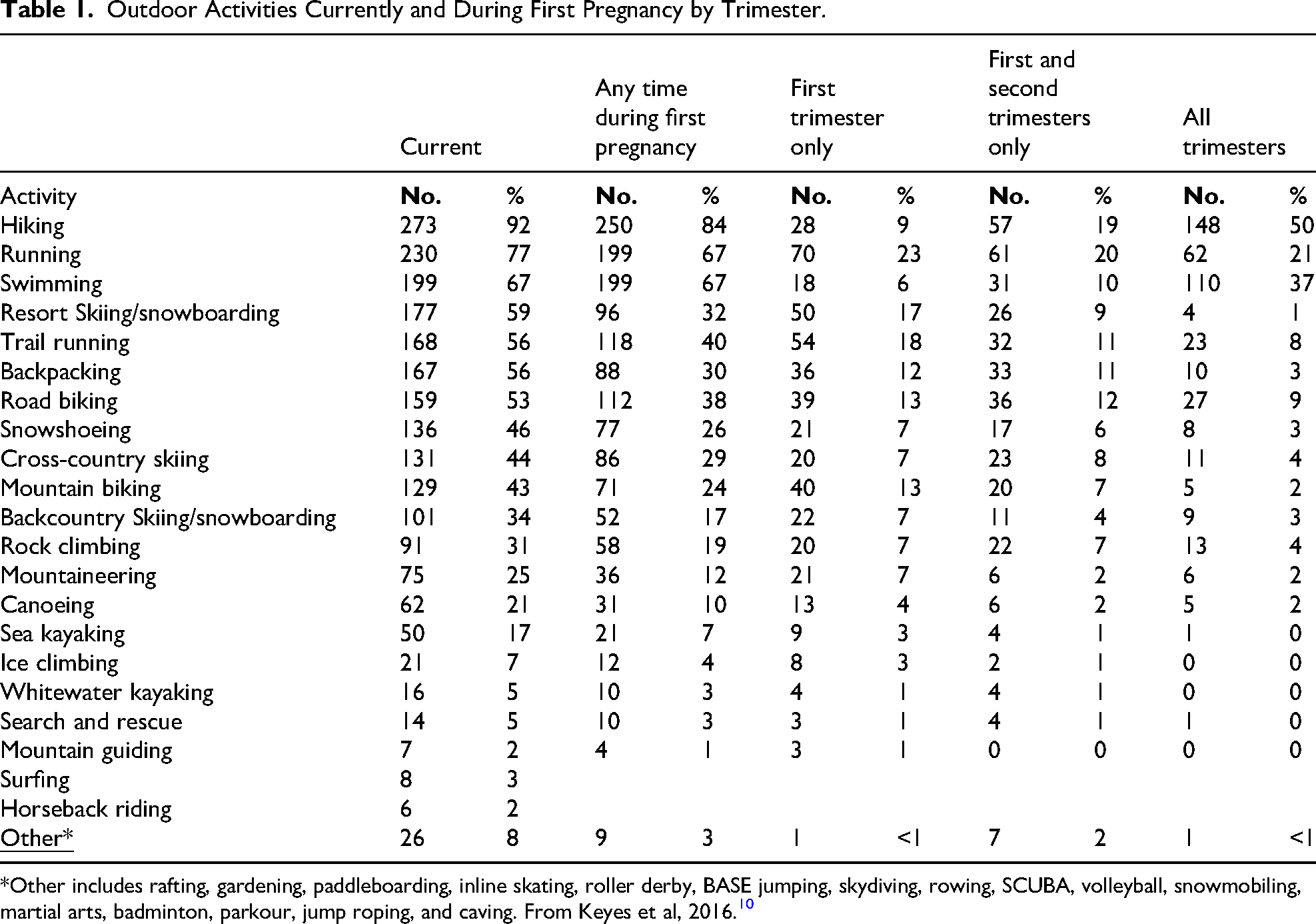
*Other includes rafting, gardening, paddleboarding, inline skating, roller derby, BASE jumping, skydiving, rowing, SCUBA, volleyball, snowmobiling, martial arts, badminton, parkour, jump roping, and caving. From Keyes et al, 2016. 10
The physical and physiological changes in pregnancy and potential effects on the fetus may impact the risk calculation in specific outdoor activities—for example, trail running in the heat, hiking at high altitude, or snowboarding. Pregnant individuals may avoid many wilderness activities due to an abundance of caution. When guidelines are restrictive or unclear, many pregnant individuals forgo a reasonable risk analysis related to individual activity and stage of pregnancy. 13 Likewise, they may unwittingly engage in activities that are higher risk than anticipated.
The American College of Obstetrics and Gynecology (ACOG), American Association of Family Practitioners (AAFP), the American College of Sports Medicine (ACSM), the Canadian guideline for physical activity in pregnancy, and pregnancy-related physical activity guidelines from around the world acknowledge the health benefits of engaging in moderate exercise in uncomplicated pregnancies.1–9 The 1985 guidelines published by the American College of Obstetrics and Gynecology recommended keeping a pregnant patient's heart rate (HR) under 140 and restricting daily exercise to 15 min or less. 14 Subsequently, guidelines have increasingly recognized the benefits of physical activity and recreational pursuits during pregnancy while also advising against exercise and activities that may involve hot or humid conditions, strenuous levels of activity, or activities with a risk of fall or abdominal trauma frequently encountered in outdoor and wilderness settings. Guidelines often encourage more controlled environments such as gyms with air conditioning, stationary equipment, or pools.1–9 These academic society guidelines may discount the physical and emotional health benefits of outdoor exercise in pregnancy.
Recreation in wilderness settings has multiple potential mental health benefits for pregnant people. Pregnancy-associated mood and anxiety disorder has a prevalence rate of 18.2% during pregnancy. 15 Poor mental health in pregnancy is associated with preterm labor, low birth weight, cognitive problems, psychopathology in offspring, and increased risk of maternal postnatal depression. 16 Exercise in pregnancy is associated with improved mental health as well as reduced risk for hypertensive disorders, gestational diabetes, and cesarean sections. 17 Outdoor exercise is associated with improved mental well-being. 18 Hiking and long-distance walking have positive psychological and physiological health effects. 19 Findings suggest that outdoor activities offer some relative advantages and benefits over indoor exercise for psychological health, highlighting the importance of considering outdoor exercise's physical and emotional health benefits.20,21
This narrative review evaluates the existing literature on wilderness-based physical activity recommendations during pregnancy. To enhance understanding of the risks and benefits of outdoor recreation during pregnancy, we conducted a comprehensive review and synthesis of the existing literature, summarized in Table 1. The objective is to offer guidance for healthcare practitioners who oversee the well-being of pregnant individuals who want to participate in diverse outdoor activities.
Methods
We conducted a narrative review of wilderness activities commonly practiced by people of childbearing age. We searched PubMed for relevant articles on pregnancy and specific sports, including climbing, mountaineering, hiking, backpacking, trail running, skiing, cycling, open-water swimming, scuba, water sports, and surfing, and further searched the references of identified articles. We summarized available data on existing recommendations and considerations of risks and benefits for pregnant individuals. We also researched formal guidelines regarding exercise in pregnancy, including activity-specific guidelines from recognized national organizations in the United States and Canada, as well as the International Olympic Committee (IOC), and associated evidence and reference lists.
General Considerations for Exercise During Pregnancy
The 2020 ACOG guidelines recommend that pregnant patients build up to moderate-intensity exercise for at least 20–30 min daily, most days of the week. Guidelines suggest that the activity may be too strenuous if pregnant individuals cannot pass the “talk test,” carrying on a conversation during exercise.1,22
The Canadian guidelines for physical activity in pregnancy emphasize the benefits of exercise in pregnancy for maternal health as well as for reduction in pregnancy complications, stating that pregnant women should accumulate at least 150 min of moderate-intensity physical activity each week, but also note that the safety and efficacy of chronic high-intensity physical activity for the mother, the fetus, and the neonate are not known. 4 Accordingly, the Consensus Panel recommends high-intensity physical activity only in a monitored environment. 4
The IOC expert committee on exercise in pregnancy in recreational and elite athletes reviewed exercise in pregnancy and summarized changes to maternal physiology and anatomy. 23 These include changes in gait, stance, and balance; a 50% increase in cardiac output and maternal blood volume; decreased vascular tone; respiratory changes, including increased tidal volume and minute ventilation; improved maternal thermoregulation; and increased maternal glucose levels and insulin resistance. 23 Screening of athletes during pregnancy can evaluate for risk factors that might limit activities. 3 They caution that warning signs to stop exercising may include vaginal bleeding, regular painful uterine contractions, amniotic fluid leakage, dyspnea prior to exertion, and/or dizziness/syncope. 23 Their recommendations include not performing high-intensity training at >1500–2000 meters for those not acclimatized, avoiding full-contact sports throughout pregnancy, and in the second and third trimester, avoiding sports such as downhill skiing, snowboarding, BMX and mountain cycling, among others, due to risk of direct trauma or falls. 3 They do recommend continuing noncontact training throughout pregnancy in uncomplicated pregnancies. 3
Exercise during pregnancy has shown significant health benefits, including a reduced risk of cesarean delivery, gestational diabetes, and hypertensive disorders of pregnancy. 24 While these guidelines generally recommend up to moderate levels of exercise in pregnancy, data also support the benefit of vigorous exercise. A portion of pregnancies fall into a high-risk category, and restrictions on physical activity may be warranted in those cases. The benefits of aerobic exercise for pregnant and nonpregnant people are well-documented. Without maternal or fetal contraindications, pregnant people should feel comfortable engaging in these physical activities below 90% of their VO2 max.25,26 Studies support exercise up to 90% of the maximum heart rate without adverse effects on the mother or fetus.25,26 These studies suggest providers should not necessarily counsel against higher-intensity activities or decrease exercise intensity during uncomplicated pregnancies in pregnant individuals accustomed to such exercise.
Risks of Trauma
Overall, trauma in pregnancy is the leading cause of nonobstetric maternal death and remains a significant cause of fetal demise.27,28 Pregnant people have twice the mortality of nonpregnant people in the setting of trauma evaluated at a trauma center. 29 In early pregnancy, the uterus is protected from direct trauma. However, by the end of the first trimester, the uterus and fetus rise out of the pelvis and are susceptible to blunt traumatic injury. 30 Some forms of outdoor recreation have a greater risk of falls and injury. High-velocity blunt trauma confers unique complications, including placental abruption, pelvic fracture, uterine rupture, premature labor, premature rupture of membranes, fetal demise, and amniotic fluid embolism. 30 Pregnant patients should be aware that falling in the later parts of pregnancy confers an increased risk to the fetus over falls in the first trimester, when considering the risks of engaging in particular outdoor endeavors.
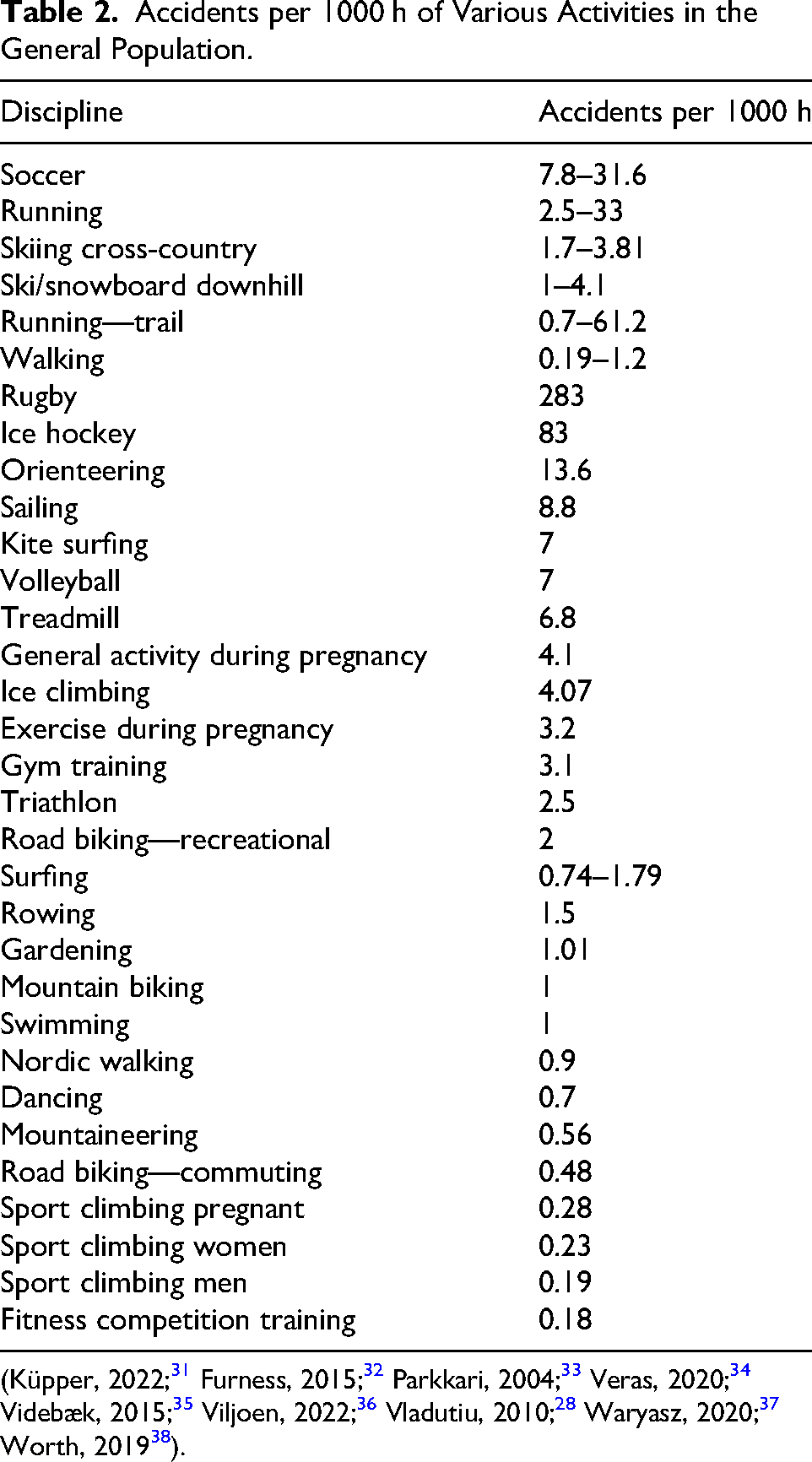
Injury rates related to nonexercise physical activity, such as walking, as well as occupational, gardening, and home activities, during pregnancy (3.2 per 1000 h) are slightly lower than injury rates related to exercise during pregnancy (4.1 per 1000 h). 26 However, the majority of injuries occur while not exercising. 28 Some activities carry greater inherent risk than others. For comparison, we provide the trauma risk for wilderness and common nonwilderness activities in nonpregnant patients (Table 2). The table illustrates that some activities that may be considered “dangerous,” such as sport climbing, carry lower risks than “safe” activities like dancing and gardening. Such data may help clinicians and pregnant individuals with risk assessment. Individual skill and comfort level should also inform decision-making around sports activities during pregnancy. Potential activity-specific dangers of falls and trauma are discussed separately in the following sections.
Accidents per 1000 h of Various Activities in the General Population.
Mountaineering and Climbing
Mountaineering and climbing raise unique considerations in pregnancy and are often perceived as being high-risk activities by medical professionals. A more nuanced understanding and appreciation of mountaineering and climbing can guide best practices to manage the risks. Sport climbing has a low incidence of injury compared to many other sports (Table 2), with the majority of injuries minor in severity, such as abrasions. 31 Climbing inside increases the risk of crowds and collisions, whereas outdoors, depending on the rock, rock falls, and scree, may pose risks. 31 Greater than 50% of all severe accidents are related to a significant mistake in belaying. 31 As with any situation, the belay technique is a foundation of safety in climbing. Pregnant climbers tend to self-adjust their climbing habits over pregnancy. Of 32 pregnant sport climbers, half the patients continued to climb until 36 weeks pregnant without complications, and the majority adjusted climbing practices to include decreasing climbing difficulty, time spent climbing, and increasing the proportion of top roping. 39
Given the risk of life-threatening implications from blunt trauma, people who are pregnant and pursuing climbing or mountaineering may consider strategies to mitigate risk should they have a fall. While not studied, the general practice after the first trimester is to transition to a full-body harness to accommodate the growing uterus. Climbing with a belay or top roping will carry less risk for a high-consequence fall than lead climbing, bouldering, or solo climbing. Pregnant climbers can be encouraged to emphasize lower-difficulty top-rope climbing in a full harness in the second and third trimesters. They can ensure their belayer is trustworthy and experienced and can minimize extra slack in the rope. Pregnant climbers should also recognize that other conditions related to pregnancy, such as peripheral edema, can result in poor shoe fit, and repetitive motions often associated with climbing may make pregnancy-related problems, such as carpal tunnel syndrome, worse.
Mountaineering carries different risks than indoor and sport climbing. Some critical considerations are the remoteness, altitude, extremes of temperature, risk of UV exposure and lightning, issues of fatigue and endurance, risks of unroped falls in high-consequence terrain, and the use of sharp crampons and ice axes near gravid abdomens. Despite the lack of existing data and literature describing the risks of mountaineering in pregnancy, the additive dangers inherent in this activity and environment encourage an abundance of caution and situational awareness.
Pregnant climbers can mitigate risk by not pushing their limits, top roping, avoiding ground falls early in a climb, selecting reliable routes, and avoiding climbing roofs and overhangs. It is also recommended to switch to a whole-body harness in the second and third trimesters. 31
Hiking and Backpacking
Hiking is a common pregnancy activity, with one study showing that 84% of survey respondents hiked during their pregnancy. 10 Many of the risks may overlap with those of mountaineering, as described earlier, depending on the terrain and environment. Uneven footing, exercise fatigue, and pack weight could increase fall risk in pregnant and nonpregnant individuals. Precautions that increase stability should be advised, such as wearing sturdy hiking boots and using trekking poles. Trekking poles can improve balance and reduce muscle activity around the lower extremity joints. 40 Pregnant hikers must prepare carefully for potable water procurement, avoiding iodine water treatment systems, and ensuring adequate hydration when far from potable water sources. 41
Trail Running/Running
Individuals who were runners before pregnancy continue to hold firmly to this identity and trust their instincts and knowledge as they adjust to running during pregnancy. 42 Surveyed runners lost trust when their medical providers imposed restrictions without solid evidence that seemed overly restrictive, emphasizing the importance of a partnership model between the pregnant patient and the provider. 42 There is variable data on the risks and benefits of running during pregnancy. In one study of competitive runners, a voluntary decrease in total training time and effort was common, especially in the third trimester. 43 The reasons given for this change include feeling poorly, concerns about the risk of miscarriage, and a desire to gain/maintain weight. Notably, 27% of women stopped running during pregnancy due to physician advice, and although their reasons for stopping were not included, injuries reported due to running were rare. 43 An international study of females who reported running during pregnancy showed no risk of reduced gestational age or birth weight but an increased risk of assisted vaginal delivery. 44 Trail running may increase the risk of falls and injuries, though data comparing casual trail with road running is lacking, and most data are specific to race conditions, which are inherently more intense than recreational exercise. 36
Despite the myth that pregnancy is associated with poor balance and instability, data suggest that differences in balance during pregnancy may reflect positive adaptations to the physical changes experienced during pregnancy. 45 Pregnant individuals who exercise are less likely to experience a fall than those who are sedentary. 46 Thus, fear of poor balance alone should not determine decisions to run in specific terrain. Pregnant individuals who were regular trail runners prepregnancy, likely can continue on trails with awareness of slowing down or transitioning to hiking in technical sections. Pregnant patients should be aware that falling in the later parts of pregnancy confers an increased risk to the fetus. Pregnant patients should consider the role of abdominal and breast support during running; a maternity belt can help provide abdominal support in some cases, and a well-fitting sports bra can enhance comfort and may require a different size than prepregnancy.
Skiing
Nordic Skiing
Nordic skiing is a highly aerobic sport that requires full-body strength and allows participants to achieve a “vigorous” level of activity, defined as >85% of maximal heart rate, which is in contrast to ACOG's general recommendation of moderate levels of activity for most pregnant patients.1,25 Nordic skiing is a low-impact sport that can be a safe mode of exercise for pregnant individuals with prior experience while acknowledging fall risk and heart rate parameters. 47 Multiple publications have shown that female Nordic skiers who exerted themselves at a high level before pregnancy can maintain an elite level of training while pregnant, with no observed detriment to the fetus.48,49
Injuries in nonpregnant Nordic skiers occur at 3.81/1000 h of training.38,50 The most common causes of injury are lower extremity (foot, ankle) and overuse injuries rather than acute trauma. 50 These injuries include medial-tibial stress syndrome, Achilles tendonitis, and ankle ligament sprains.38,50 Nordic skiing has lower rates of injury relative to other endurance sports such as long-distance running, swimming, cycling, and orienteering. 38 Nordic skiing includes the benefits of aerobic exercise and time outdoors in winter, in an activity with a lower risk of significant trauma than many other outdoor activities. Nevertheless, we encourage pregnant individuals to strongly consider their fitness level, skill and comfort on skis, speed, crowding, snow conditions, and trail steepness when calculating their risk.
Downhill/Alpine Skiing/Snowboarding
While there is no research on the risks of alpine skiing and snowboarding for pregnant mothers and fetuses, the data on known risks in the general population can help guide decision-making. Downhill skiing/snowboarding is a high-gravity sport performed at high speeds, resulting in a significant risk of traumatic injuries. Injuries most frequently occur through falls and collisions, with steep slope angles, variable snow/obstacles, and unpredictable visibility increasing the risk of falling. Additionally, snow sports at public resorts increase the risk of skier–skier collisions, independent of the athlete's skill set, putting participants at risk of trauma that is out of their control. Snowboarding has a higher incidence of abdominal trauma than skiing, showing a 6-fold increased risk of splenic injury, 51 although head injuries remain the most common problem. 52 Pregnant individuals should be aware of these significant risks and may prefer alternative outdoor activities to downhill snow sports, particularly in the second and third trimesters. If participating, pregnant individuals should strongly consider their skill and comfort on skis, altitude, snow conditions, slope angle, and resort crowding when deciding whether to partake in downhill skiing or snowboarding.
Cycling
One survey of pregnant people found that 38% participated in road biking during pregnancy, with 9% doing so during all 3 trimesters. 24% participated in mountain biking during pregnancy, with 2% maintaining mountain biking throughout the pregnancy. 10 During the third trimester, maternal and fetal physiologic parameters were similar in upright and semi-recumbent cycling. 53
Mountain Biking
The risk of mountain biking in pregnancy is unknown, but data on known risks in the general population may guide decision-making. Common injuries associated with mountain biking in the general public are traumatic brain injuries, upper extremity fractures/dislocations, and contusions/lacerations. 54 There is an increased risk of injury with downhill mountain biking, steep/technical trails, and slippery riding conditions. 55 As discussed in the downhill skiing section above, the risks of high-velocity trauma have serious consequences in pregnancy. We encourage pregnant individuals to avoid high-risk terrain mountain biking unless they are highly skilled and conditioned, choosing low-risk terrain, controlled speeds, avoiding jumps, and ensuring well-maintained equipment. For most mountain bikers, it may be prudent to avoid mountain biking in the second and third trimesters of pregnancy.
Road Biking
Common injuries associated with road cycling in the general public are abrasions, upper extremity fractures/dislocations, iliotibial band syndrome (overuse), and traumatic brain injuries. 56 Risk factors for injury include downhill slope, technical turns, unprotected bike lanes, and obstacles on the road.56,57 Notably, road cycling injuries may occur at high speeds and in the presence of traffic. Road bicycle accidents have a high mortality rate when requiring hospitalization.57,58 Snap-in pedals can be a source of falls if snapping out is difficult, so pregnant cyclists could consider using pedals without snap-in technology to avoid falling. As with other high-speed sports, we encourage pregnant individuals who road bike to carefully assess the risk of high-traffic roads, riding speeds, bike path crowding, and their skill level because of the serious consequences of blunt trauma in pregnancy.
Water Sports
Open Water Swimming
Water-based exercise, most commonly lap swimming or water aerobics, is considered safe during pregnancy. Immersion in water leads to an experience of weight reduction with less stress on joints and decreased vertical forces. 59
While lap swimming in a pool is a popular and recommended safe choice in pregnancy, pregnant individuals may prefer to enjoy the benefits of being outside in open water. 60 In addition to the risk of trauma from boat traffic, drowning, and gastrointestinal illness from water pollution, open water swimmers also risk temperature dysregulation. Placental blood flow has been found to be unaffected by cold water–mediated peripheral vasoconstriction. 61 Regular cold water exposure is hypothesized to reduce circulating levels of stress hormones, with pregnancy outcomes possibly ameliorated through stress attenuation, as a consequence of long-term cold water swimming. 61 Conversely, hyperthermia is associated with high levels of exertion in water temperatures over 33 °C. Swimming-induced pulmonary edema (SIPE) occurs in the absence of aspiration during swimming, causing shortness of breath and potentially a productive cough with blood-tinged sputum and hypoxia. SIPE is often associated with longer distances, female sex, cold water, and triathletes, but we are unaware of any documented cases in pregnant swimmers. 62 Case reports of acute gastrointestinal illness related to open-water swimming have been described in the literature. 63
Swimming outdoors in open water holds baseline risk regardless of pregnancy status. Pregnant individuals should maintain situational awareness of boat traffic, unseen hazards, water quality, and drowning prevention similar to nonpregnant swimmers, including an open-water swim buoy and not swimming alone. Well-fitted wetsuits that are not too tight as to cause constriction can be considered and can provide added buoyancy; however, there is no data on the use of wetsuits in pregnancy. They also should maintain awareness of the risk of hypothermia, hyperthermia, and pulmonary edema depending on the environment.
Scuba Diving
Women constitute approximately 40% of the 3.5 million active self-contained underwater breathing apparatus (scuba) divers in the United States (DEMA). However, the number of women who dive during pregnancy is unknown.
ACOG recommends avoiding scuba diving in pregnancy 1 due to concerns that fetal pulmonary circulation cannot filter bubble formation, increasing the theoretical risk of arterial gas embolism. 64 Animal data suggest adverse fetal effects due to fetal decompression and hyperbaric oxygen exposure, leading to premature closure of circulatory shunts. 65 While scuba diving is not recommended, there are multiple case reports of women unknowingly diving during pregnancy without adverse outcomes.65,66 Based on these reports, and despite theoretical concerns, fetal harm is not certain and pregnancy termination is not recommended following inadvertent scuba diving. 64 Given known risks, however, we do not recommend scuba diving during known pregnancies.
Water Skiing and Personal Watercrafts
There is no research on the effects of water skiing and use of personal watercrafts in pregnancy. Known risks in the general population can help guide decision-making. For water skiers and jet skiers, falling backward with legs abducted may cause water to strike the perineum. Water can be forced into the vagina, cervix, upper genital tract, and peritoneal cavity. Water skiing is the most commonly reported sport, placing participants at risk for vaginal injuries, including extensive vaginal and cervical lacerations, incomplete abortion, traumatic episiotomy, pelvic abscess, and salpingitis. 67 Passengers on personal watercraft (jet skis) are at particularly high risk due to the fast acceleration. 67 Given such concerns, these sports are not recommended during pregnancy. If a pregnant person sustains a potential water skiing or watercraft injury, a careful pelvic exam including an evaluation of the cervix for necessary repairs should be performed, and antibiotic prophylaxis can be tailored based on the water source. 67
Surfing
While there is no research on the effects of surfing in pregnancy, the known risks of surfing overall can help guide decision-making. Surfing is often continued into pregnancies, although lying prone on a surfboard will become uncomfortable as pregnancy progresses. Surfing is also strongly associated with gastroesophageal reflux disease (GERD), with short-board surfing having a stronger association with GERD than long-board style surfing. 68 The incidence of GERD during pregnancy ranges from 17% to 45%. 69 Theoretically, surfing may compound the baseline increased prevalence of developing or worsening GERD symptoms in pregnancy, but this has not been studied.
In general, surfing is a relatively safe sport, with injury risks cited as 0.74 to 1.79 per 1000 h surfed.70,71 Surfing confers a risk of blunt traumatic injury, most commonly from contact with the board or ocean floor. The most common areas injured are the head and neck and extremities. Injuries include lacerations, contusions, sprains, and fractures. While abdominal and pelvic trauma are uncommon in nonpregnant surfers, 70 pregnancy adds considerably to the stakes if abdominal trauma does occur. Higher wave height and rock or reef ocean floor are both associated with an increased risk of injury. 72 Pregnant individuals who choose to surf during pregnancy can continue as comfort allows, consider using softer boards, rounded noses, and flexible soft edge fins to reduce board-related trauma. Pregnant surfers can choose skill-appropriate settings with minimal crowding that minimize risk for trauma or collisions and be aware of the risk of hypothermia.
There is no data to suggest snorkeling, paddle sports, or boat travel pose an increased risk during pregnancy. Pregnant individuals can consider their level of comfort when engaging in these activities.
Seasickness is a common ailment at sea and shares many clinical features and treatment options with nausea and vomiting in pregnancy. Most medications that are used for nausea and vomiting in pregnancy are also effective for seasickness prophylaxis, except for serotonin antagonists (ondansetron).73,74 Anticholinergics (scopolamine, dicyclomine) used for nausea and vomiting in pregnancy and motion sickness have a good safety record, with no studies supporting an increased risk of malformations or other fetal complications. 75 Patients may consider transdermal scopolamine patches if they are unable to swallow oral antiemetics or if suppositories are not optimal. 76
Counseling the Active Pregnant Patient: Considerations
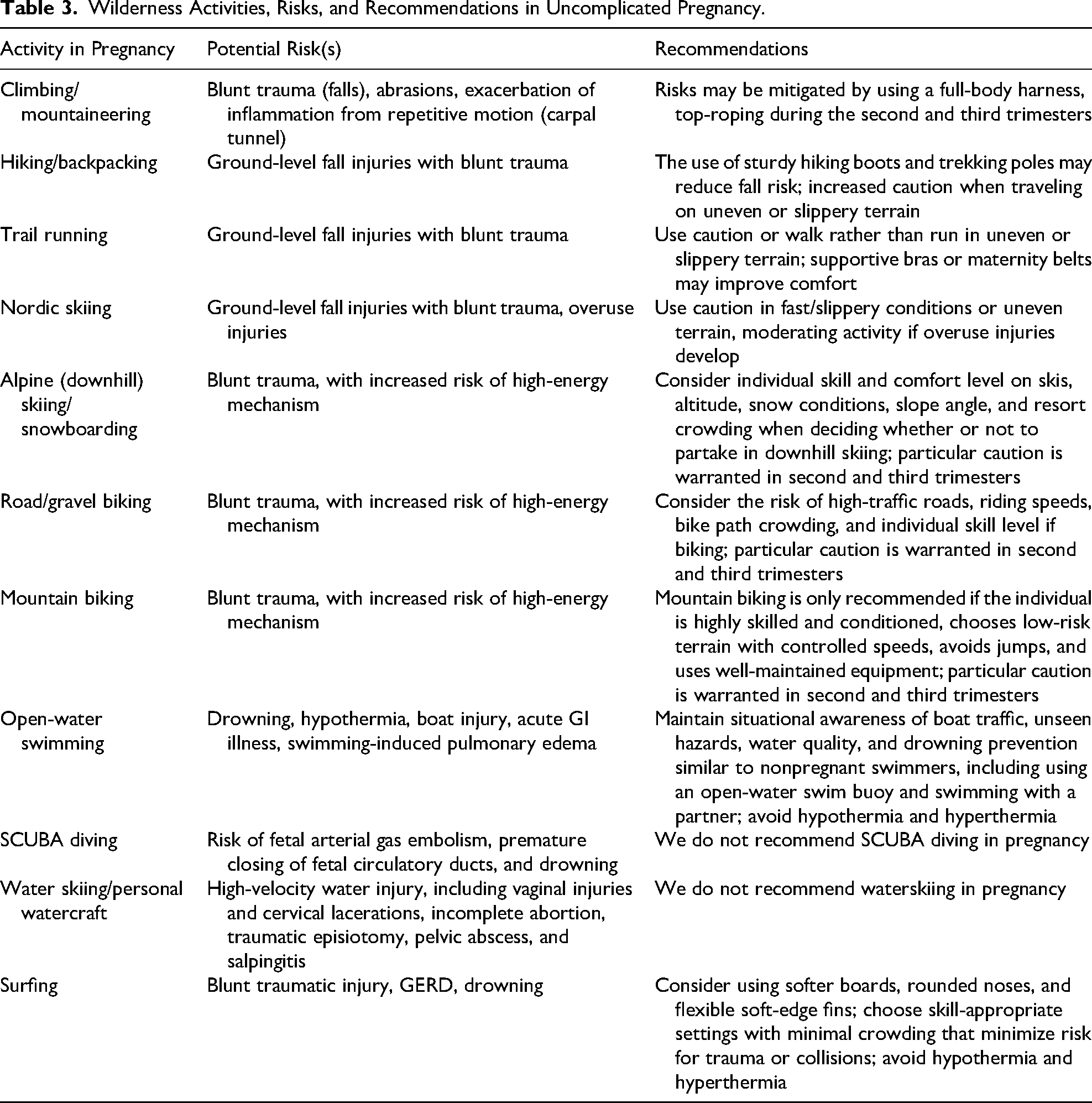
We recommend shared decision-making between the clinician and the patient when evaluating specific activity recommendations. Begin with an assessment of baseline physical fitness and the patient's prior experience with the proposed activity. A questionnaire such as the Canadian Society for Exercise Physiology(CSEP) Get Active For Pregnancy questionnaire can be helpful. Is there a history of obstetrical complications with previous pregnancies, or are there current complications such as intrauterine growth restriction or maternal hypertension? If so, consultation with an obstetrician may be helpful. In which trimester will the activity take place? The fetus is well protected in the pelvis in the first trimester. In the second and third trimesters, blunt trauma, including falls (particularly high velocity), poses risks, including placenta abruption, premature uterine contractions, and maternal fetal hemorrhage, indicating a need for prompt medical evaluation of the pregnant patient and her fetus. Where will the proposed activity take place, including risk factors such as altitude, heat or cold exposure, and remoteness from rescue and medical care? Can precautions, such as equipment modifications, be taken to maximize comfort and minimize risk? An informed discussion of these issues, individualized to the patient, may help promote safer participation in wilderness activities in pregnancy. Table 3 summarizes risks and considerations for specific activities during pregnancy.
Wilderness Activities, Risks, and Recommendations in Uncomplicated Pregnancy.
Limitations
This review is limited by the lack of data specific to wilderness activities in pregnancy. We have employed data on the benefits of exercise in general and on the benefits of exposure to nature during pregnancy, but further research is needed to inform specific recommendations. Additionally, we also extrapolate data on injuries in nonpregnant individuals to guide recommendations for risk assessment. Currently, few studies focus on the risks and benefits of activities in wilderness settings in pregnancy. When available, studies are often limited by small sample sizes.
Conclusions
In light of the limitations of existing research on wilderness activities during pregnancy, we aim to maintain objectivity without making overly lenient recommendations and balance theoretical versus objective risks. The absence of data on activities in wilderness settings does not imply that a given exposure is necessarily harmful or safe. A general starting point should be a pregnant person's fitness and comfort level with the activity prepregnancy. Existing data and literature suggest that many wilderness activities can safely occur during pregnancy. There is a need for further research to better understand the safety profiles of various activities and to develop evidence-based recommendations for pregnant individuals. Prospective studies of pregnant individuals across a range of activities could add value to existing guidelines and reviews. We recommend a tailored and individualized approach, accounting for patient-specific profiles, and balancing the need for safety with the many emotional and physical benefits of access to and activity in wilderness environments.
Footnotes
Author Contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.