
Abstract
A full century has passed since George Leigh-Mallory and Andrew (Sandy) Irvine disappeared on the upper reaches of Mount Everest in June 1924. Theodore Howard Somervell (April 16, 1890–January 23, 1975), mountaineer, surgeon, and medical missionary, also was a key player in the 1924 expedition—as well as the 1922 Everest expedition where he was a member of the first ever team of climbers to break the 8000-m barrier. More commonly known as Howard or T.H., Somervell was one of those rare individuals whose multiple talents qualified him as nothing short of a polymath while simultaneously providing an example of outstanding humanitarian qualities. British born, he was resident in India for nearly 40 y while working there as a medical missionary. He bore witness as a battlefield surgeon to the horrors of the First World War after receiving his medical training at University College, London. An active climber for much of his early life, he made notable ascents not only in the Himalaya but also closer to home in the mountains of the United Kingdom and mainland Europe. Somervell contributed numerous articles to the medical literature, but he is perhaps best known for 3 books published between 1936 and 1947 that touch largely on his experiences as a medical missionary. His decades of practice as a medical missionary in service to the poor of India allowed him to save lives on a scale approaching that of the slaughter he witnessed years earlier as an Army medical officer.
Introduction
Finally, as we approached the level of 28,000 feet [8534 m], the summit being only half a mile away or less, I felt that, as far as I was concerned, it was hopeless to continue. I told Norton that he had no chance of the summit with me. My throat was not only extremely painful, but was getting almost blocked up—why, I knew not. . . . Somewhere about 25,000 feet [7620 m] high [on the descent], when darkness was gathering, I had one of my fits of coughing and dislodged something in my throat which stuck so that I could breathe neither in nor out. I could not, of course, make a sign to Norton, or stop him, for the rope was off now; so I sat in the snow to die while he walked on, little knowing that his companion was awaiting the end only a few yards behind him. I made one or two attempts to breathe, but nothing happened. Finally, I pressed my chest with both hands, gave one last almighty push—and the obstruction came up. What a relief! Coughing up a little blood, I once more breathed really freely—more freely than I had done for some days. 1
This passage, written by T. Howard Somervell (April 16, 1890–January 23, 1975), shortly after his attempt on Everest's summit in 1924 with Edward Norton, provides one of the earliest graphically written illustrations of how any damage to the respiratory tract is potentially life threatening at extreme altitude (Figure 1). The phenomenon, today often referred to as high altitude pharyngitis and prompted by airway mucociliary dysfunction, may progress from a dry hacking cough to a very dry crusting of the larynx. This can cause serious airway blockage, as described by Somervell.
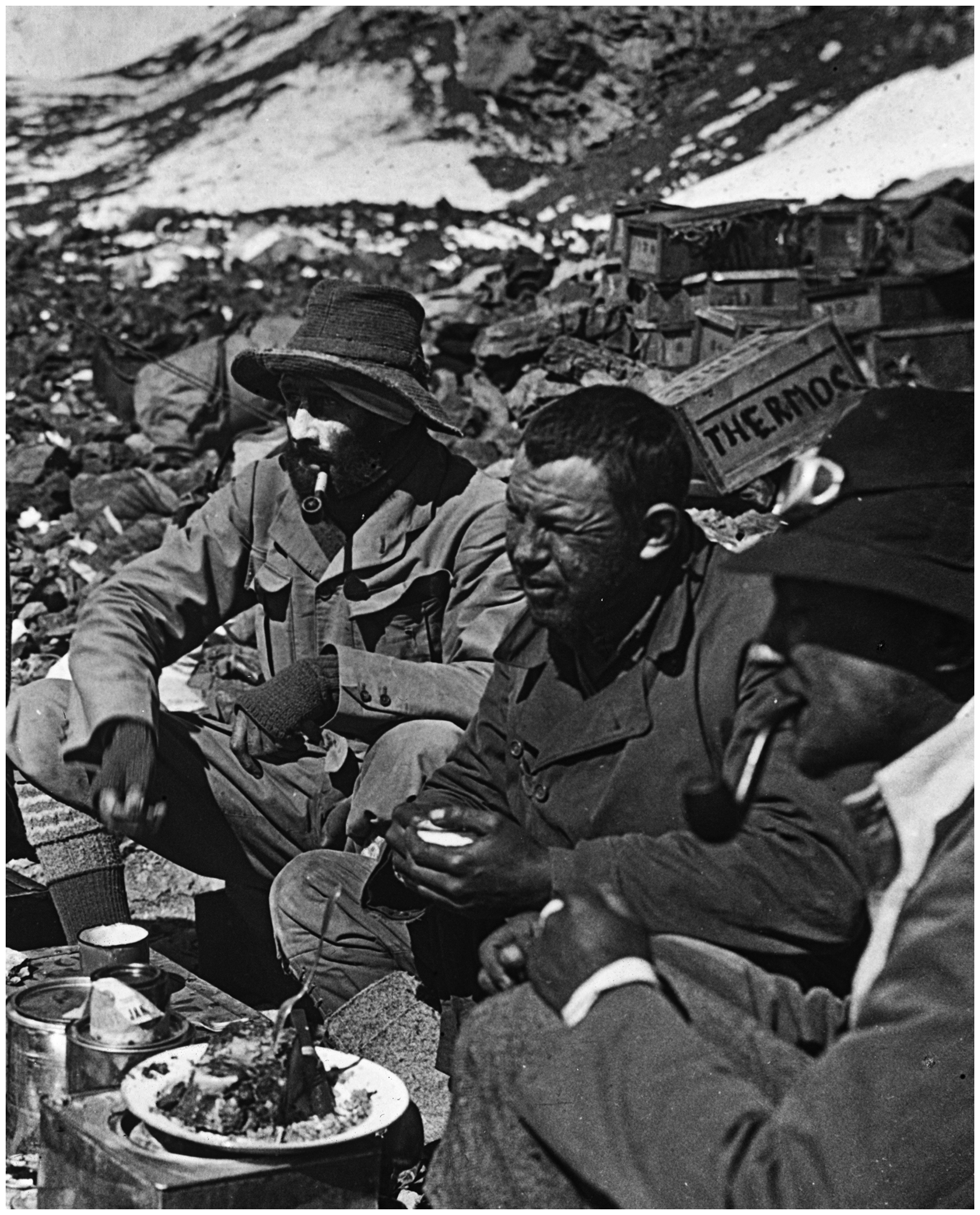
Somervell (center) with Edward Norton (left) and George Mallory at advanced base camp on the north side of Everest in 1922 shortly after their descent from >8000 m. Reproduced with permission of the family of Anne Russell.
As of 2024, a full century has passed since the above-described episode transpired on Everest, on the same expedition where George Leigh-Mallory and Andrew (Sandy) Irvine disappeared on the upper reaches of the peak during a well-known summit attempt—just a few days after Somervell's near-death experience.
More commonly known as Howard or T.H. Somervell, this man was one of those rare individuals whose multiple talents qualified him as nothing short of a polymath while simultaneously providing an example of outstanding humanitarian qualities. British born but a resident of India for nearly 40 years while working as a medical missionary, this surgeon, mountaineer, painter, and humanist was a member of first 2 expeditions to Mount Everest (in 1922 and 1924) that pioneered extreme altitude climbing above 8000 m. This short essay touches on a few of his life's more prominent experiences. (A book-length examination of Somervell's life for a general audience can be found in First on Everest: The Life of Howard Somervell, written by the coauthor of this essay and scheduled to be released in 2025 by The History Press, Cheltenham, UK.)
Youth
Born in Kendal, Westmorland, England, Somervell could have followed his father into the successful family shoe-manufacturing business. After Rugby School, though, he read natural sciences at Gonville and Caius College, University of Cambridge. He graduated with a double first in the Natural Sciences Tripos in 1912. Somervell's talent for natural science led him to the study of medicine at University College, London, from which he graduated in 1915 as the First World War was gathering momentum.
His legendary climbing and mountaineering pursuits began in the Lake District of northern England when he was a young adult, and his first experience with alpine climbing occurred in the Alps of Europe in 1913.
War Years
Early Days
When war in Europe broke out in August 1914, Somervell considered enlistment in the Army as a line officer but eventually joined the Officer Training Corps to gain experience in the Royal Army Medical Corps. He was commissioned as a captain in the Territorial Army on June 19, 1915, the year he qualified as a physician. 2 He began training as a general surgeon at University College Hospital that same year, eventually qualifying in 1921 after his training was interrupted by war service. However, he received training of a less formal sort, although likely more intensive, as a medical officer posted to casualty clearing stations (CCSs) during the years 1915–18. In 1915, 34 CCSs comprised 8 officers and 80 men together with operating tables, portable generators, electric lighting, and collapsible huts as operating theaters. The role of a CCS was threefold. Lightly wounded men were treated and returned to their units. The more seriously wounded who were well enough to be evacuated by train were transferred to base hospitals for further treatment. Those needing immediate surgery were operated on at the CCS itself. Somervell's unit, 34 CCS, was in France by November 1915.
Battlefield Surgeon
By spring 1916, Somervell's CCS was some 10 miles behind the front line, attending some of the casualties that resulted in the leadup to the Battle of the Somme. Once the hostilities started in earnest on the Somme on July 1, 1916, the medical services were overwhelmed. In the first 24 h, 3000 wounded soldiers were brought to 34 CCSs. Three days later, the total increased to a staggering 10,000. Somervell was to write Never in the whole war did we see such a terrible sight. Streams of motor ambulance a mile long waited to be unloaded. Though many ambulance trains went out at one side of our camp, the wounded had to lie not merely in our tents and shelters and in the adjacent farm buildings, but the whole area of the camp, a field of five or six acres, was completely covered with stretchers placed side by side, each with its suffering or dying man upon it. . . . We surgeons were hard at it in the operating theatre, a good hut holding four tables. Occasionally we made a brief look around to select from the thousands of patients those few fortunate ones whose life or limbs we had time to save. It was a terrible business. Even now I am haunted by the touching look of the young, bright, anxious eyes as we passed along the rows of sufferers. Hardly ever did any of them say a word, except to ask for water or relief from pain. I don’t remember a single man in all those thousands who even suggested we should save him and not the fellow next to him. Silently beseeching they lay, as we rapidly surveyed them to see who was worth saving. Abdominal cases and others requiring long operations simply had to be left to die. Saving a life by amputation, which can be done in a few minutes, or saving of limbs by the wide opening of wounds had to be thought of first. There, all around us, lying maimed and battered and dying was the flower of Britain's youth.
1
The major issues that faced the Army medical services in France were complex and grossly contaminated wounds, rapidly spreading gas gangrene, and the challenge of preventing and arresting infection. One major consequence of this was that >41,000 amputations were performed on soldiers during the First World War. 3
In the winter of 1916–17, 34 CCS was treating many hundreds of soldiers with trench foot (ie, nonfreezing cold injury). Somervell subsequently authored an article on his experiences with this malady, observing that tetanus often would complicate the condition. 4 This paper on trench foot was the only peer-reviewed publication to result from his surgical experiences during the First World War.
Not unlike many physicians in the Royal Army Medical Corps stationed near the front lines, Somervell gained immense operative experience during his time at 34 CCS. Many years later he devoted a few pages to the technical aspects of the surgery of gunshot wounds to the stomach. He wrote Diagnosis is not difficult; a wound in a suitable position, with vomiting and a little haematemesis and signs of peritonitis—or even the wound alone without marked physical signs—indicates that the stomach has been damaged. . . . If there is an entrance wound only, the missile must first be localized by means of X-rays, for it is important to visualize the probable track of the missile before opening the abdomen. . . . If the chest portion of the wound seems to be relatively unimportant, and the abdomen is clamouring for treatment, the abdominal operation must first be performed. If the chest is severely injured with open pneumothorax, the chest must first be dealt with.
5
These quoted passages are interesting. In the early phases of the war, wounds of the chest and abdomen usually were considered too time-consuming to operate on, with the result that most soldiers wounded in this way died. Later in the war, attitudes shifted regarding such wounds, and innovative surgeons such as Somervell would often operate. With a transfusion of blood before and after surgery, some patients would survive.
Return to Civilian Life
After 3 y and 9 mo of service, Somervell finished the war with the rank cf Captain. He remained in the Royal Army Medical Corps until September 30, 1921. 6 He was in the army of occupation until February 1919, subsequently working as an orthopedic surgeon in 2 military hospitals in the United Kingdom. As much as Somervell had been horrified at the death and maiming caused by the war, he acknowledged that his skills as a surgeon and skills in the use and interpretation of x-rays had benefited enormously. In 1920, he became house surgeon and then house physician at University College Hospital, London, and also in that year he was awarded fellowship of the Royal College of Surgeons. 7
The Mountain World
Rediscovering the Alpine Realm
After the First World War, Somervell returned to the Alps in 1919 during the period of time he was transitioning from being a military surgeon to a soon-to-be house surgeon at University College Hospital, London. The following year, he achieved an enviable record of hard ascents in the Alps over the course of the climbing season. Despite this not-unreasonable tally of peaks, his application to join the first-ever expedition to Everest, the 1921 reconnaissance, was turned down. Undeterred, Somervell tackled numerous difficult mountain routes in Britain and continental Europe over the next 2 y. When the British decided in late 1921 to return to Everest in 1922 for a full-on summit attempt, Somervell was then working at University College Hospital in London. His interest in Everest had not been forgotten, and he received an invitation to join the 1922 expedition. His salary at the time was £150 per year (roughly £10,000 or US$13,000 in 2024). Because he came from a family of some means, however, he was able to agree to the terms of joining the expedition, which required that he pay for transportation to and from the expedition's launching point of Darjeeling in the West Bengal state of India. Once in Darjeeling, all further costs were to be met by the expedition committee.
Everest 1922
Somervell, with fellow-climbers George Mallory and Edward Norton, achieved an altitude record on May 21 1922, reaching nearly 27,000 ft (∼8229 m) on Everest's north ridge without supplementary oxygen. The men suffered some frostbite on this attempt (Norton later having part of his ear amputated) and were in need of rest and recovery. The expedition regrouped at base camp on the Rongbuk Glacier, but several of the group, including Somervell and Mallory, eventually decided to return to the mountain for one last effort. On June 7, they were enroute to the North Col Camp at 7000 m with a group of Sherpa porters when an avalanche overwhelmed them. Several days of wind-driven snowfall had accumulated in the days prior to June 7, and the climbers were apparently aware of the avalanche potential. Once on the slopes below the North Col, they had excavated trenches to see if they could trigger an avalanche. They were unable to do so, and feeling somewhat more secure, they proceeded with their ascent. Less than 600 vertical ft (∼183 m) from their camp on the col, Somervell later recounted, “With a subdued report ominous in the softness of its violence, a crack suddenly appeared about 20 feet above me. The snow on which I was standing began to move, slowly at first then faster.” 1
Although Somervell and his ropemates were lucky enough to be able to extricate themselves from the avalanche debris, 13 Sherpa porters below were less fortunate. The avalanche swept 9 of them over an ice cliff and into a crevasse. Seven were killed. This tragedy brought an end to any further progress on Everest that year.
After the 1922 Everest expedition, Somervell traveled through India before returning home to Britain. In India, as discussed in the next section, Somervell discovered what was to become in the following year his vocational purpose and home for the remainder of his working life.
Everest 1924
The British also had permission to attempt Everest in 1924, and little time was lost in planning another expedition with the aim of successfully ascending the peak. Somervell was selected for this journey as well and was widely considered to be one of the ablest climbers in the party. Although already working on the Indian subcontinent by the end of 1923, he obtained permission to take leave from his surgical duties for the planned 1924 expedition to Everest.
Before the expedition had a chance to come to grips with the upper mountain, the party experienced weather worse than anything seen in 1922. Four porters became marooned at the North Col Camp on May 23 and needed rescue assistance. 8 The slopes leading up to the col must have been full of foreboding for porters and British climbers alike, with the 1922 disaster fresh in everyone's mind. The expedition leader, Norton, chose his most capable climbers, Mallory and Somervell, for the rescue attempt. 9 This dramatic mission ultimately was successful in safely bringing down the 4 frostbitten men. Of course, this expedition is remembered for the loss of Mallory and Irvine on June 8 and not for the rescue of the porters on May 24. But it was appreciated by all that if a fatal accident had occurred during the course of the rescue, the expedition certainly would have been finished and, furthermore, open to censure on its return.
Seven days later, on June 1, Somervell moved up to the North Col Camp with several other climbers and porters. Subsequently occupying 2 higher camps as they ascended above the North Col, Somervell and Norton reached an altitude of >28,000 ft (∼8534 m), sans supplementary oxygen, on June 4. Norton managed to climb slightly higher than Somervell, reaching a high point of 28,120 ft (8570 m) in what is now known as the Great Couloir on the north face of Everest. 10 This established a world record climbing altitude that was not surpassed for another 28 years—until Lambert and Tenzing reached 28,251 ft (8611 m) on the south side of Everest during the 1952 Swiss expedition. Somervell and Norton then descended ∼5000 ft (1524 m) to camp at the North Col during the afternoon and evening after their record-breaking effort, which was punctuated shortly after the descent began by the episode recounted in the opening quotation of this article. While they were engaged in their summit attempt, more personnel and loads, including oxygen equipment, were moved up to the North Col. Mallory and Irvine left for their summit attempt aided by supplementary oxygen on June 6 and climbed into history a couple of days later on June 8 when they were spotted for the last time at around 800 vertical ft (∼240 m) below the summit on Everest's northeast ridge.
A final note to Somervell's Everest saga is worthy of brief mention because it is relevant in the annals of the history of high altitude physiology. During the Everest expedition of 1924, Somervell made observations on the composition of alveolar air of several members of the climbing party at 3 different altitudes, the highest being on the North Col at 7010 m. The samples were collected and stored in rubber football bladders, and analysis of the alveolar air was done at base camp. 11 Unfortunately, gas rapidly diffused through the bladders during transport to base camp. Therefore, these samples yielded, for example, a very low alveolar PCO2 of ∼8 mm Hg (the correct value is actually about double this). 12 Later pre-World War II British Everest expeditions in 1933 and 1938 collected alveolar gas samples at as high as 7830 m in pre-evacuated glass tubes that were heat sealed at altitude and analyzed back in the United Kingdom.13,14 These measurements produced results much more in keeping with modern accepted high altitude alveolar gas values. 12
After Everest
Following the 1924 Everest attempt, Somervell was not involved in any further major Himalayan mountaineering expeditions. However, during his many years working in India after 1924, he continued to explore and climb in the Indian Himalaya and Europe with family and friends when he was able to take short leaves from his healthcare-related duties. As with many aging mountaineers, Somervell found his relationship with the mountains changing with the passing of the years. Sketching and painting mountain landscapes became a passionate outlet for him, and his “maturing” attitude toward the hills is evident in a quote from a 1933 journey to one of the world's highest peaks, Nanga Parbat (8126 m). He wrote that his intent was to “enjoy Nanga Parbat, not to climb it—to paint it, not to struggle with it.” 15 His mountain landscape artwork has become much sought after, and many of Somervell's paintings fetch princely sums today whenever his art is sold.
Life and Work in India
Committing to an Unconventional Path
As mentioned earlier, Somervell had traveled around India after the 1922 Everest expedition, where he eventually arrived at the town of Neyyoor in the southern tip of the subcontinent. He had arranged to meet a surgeon there, Stephen Horatio Pugh, whom he had first met in England. Pugh had transformed the Neyyoor hospital into the largest surgical center south of Madras. At Neyyoor for just 10 days in 1922, Somervell took on some of Pugh's workload and was struck by the appalling poverty and need for medical care. On his return to Britain, and despite being offered a senior post at University College Hospital in London, Somervell decided that his life's work should be at Neyyoor. He applied to join the London Missionary Society in March 1923, sailing for India in October of that year.
More Than a Surgeon
From the early 1920s to 1945 and then again from 1948–53 and 1955–56, Somervell's professional life was dominated by his medical missionary work in India. His work at Neyyoor General Hospital is described in 3 books, and these provide some insight into the culture and complexities of life in southern India at a time when Home Rule for India was inevitable.1,16,17 The Partition of India in 1947 marked the dissolution of the British Raj and the creation of 2 independent dominions: India and Pakistan. Somervell admitted that when he started at Neyyoor, the British community was “respected,” but 20 y or so later, the British were “suspected.” Those who knew him well, such as friend and famous academic geologist and mountaineer Noel Odell, saw Somervell as a very gifted and unique character. In an obituary that Odell penned for the British Alpine Journal in 1976, he mentioned Somervell holding very broad and practical Christian principles. . . . He was determined not to drive those principles down the throats of Hindu or other devotees, as he declared was so often the tendency of missionaries. Somervell's great advantage proved to be his ability to identify himself with the Indian people, treating them as brothers and sisters, and the hospital patients not merely as cases, not even as “interesting cases.”
18
As Somervell described in After Everest, 1 the revulsion of his sensitive nature to the carnage of the Great War of 1914–18 had a profound influence on his future professional path. This early experience of major surgery and radiography was to stand him in very good stead in his career in India as a pioneering medical missionary. But suffice to say that he was not just a general surgeon. His responsibilities extended to orthopedic surgery, anesthesia, obstetrics, general medicine, and pathology (and occasionally public health). However, surgery was where Somervell's expertise lay.
The great range of surgical procedures he could deploy would be beyond the experience of any single surgeon today. His procedures included anything from amputation of the leg for sarcoma, to dissection of the neck or removal of half the jaw due to carcinoma, to drilling holes in the femur to drain infection from osteomyelitis. Somervell developed a particular expertise in the management of duodenal ulcer and other gastric procedures because such problems were (and remain) extremely common in South India.19–22 Medical issues such as tuberculosis, cholera, malaria, and hookworm also were maladies that Somervell had to commonly manage, and epidemics of cholera and malaria could develop with frightening rapidity. Some of his ideas were not always popular with the local community, such as the purpose-built complex for clinical management of leprosy. By 1931, Somervell was looking after some 90 patients with this malady. He reported in 1935 that opposition to his assessment and treatment of leprosy ended when one of the leaders of those resisting Somervell's efforts was found to be suffering from leprosy himself!
In late 1948, Somervell moved to Christian Medical College at Vellore, India, where he worked until 1953. He then returned to Vellore from 1955 to 1956 to cover the leave of a colleague, thereafter going into retirement in England.
Summary
Although T. Howard Somervell is perhaps best known today for his participation in the 1922 and 1924 British Everest expeditions, his record of achievement extends well beyond his mountaineering exploits. In the aforementioned obituary of Somervell,
18
Odell concluded his eulogy with the mention that The Times [of London] of 25 January ‘75 in their considerable obituary notice described Somervell as a “Visionary on Everest”. But surely, he was more than that. . . . Apart from anything else, the character and extent of his work especially in S [South] India was unequalled. . . . It will be long before the world sees again the like of this many-sided and accomplished man: perhaps fortuna multis dat nimium [fortune gives too much to many], but as Howard Somervell himself would no doubt have added, nulli satis [not enough for anyone].
Although there are those who might question his motivations as a Christian missionary, the level of public service rendered by Somervell during his years in India is difficult to comprehend today, He sacrificed his wealth, and often his health, in service to the poor of India for decades. Perhaps, as Davis has asserted, Somervell's service in the First World War had a marked influence on his later professional life: “On that horrible first morning [on the Somme] he walked alone through six acres of stretchers bearing the wounded and the dying. It was the most terrible experience of his life, but it led only deeper into . . . devotion and compassion, which in the end freed him from trauma.” 23
The authors of this work maintain that it is certainly within the realm of reason that Somervell's work in India was an opportunity for him to sweep away memories of the massive butchery of the First World War by saving the living on a rather grand scale. In our present-day world that never seems to be without a plethora of trauma, perhaps Somervell's life experience can offer thought-provoking considerations to many of us.
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.