
Abstract
We experienced a case involving prolonged cardiopulmonary resuscitation (CPR) during cardiac arrest on Mt. Fuji (3776 m), demanding lengthy exertion by the rescuers performing CPR. Considering the effects of exertion on the rescuers, we examined their percutaneous arterial oxygen saturation during simulated CPR and compared the effects of compression-only and conventional CPR at 3700 m above sea level. The effects of CPR on the physical condition of rescuers were examined at the summit of Mt. Fuji: three rescue staff equipped with pulse-oximeters performed CPR with or without breaths using a CPR mannequin. At 3700 m, the rescuers’ heart rate increased during CPR regardless of the presence or absence of rescue breathing. Percutaneous arterial oxygen saturation measured in such an environment was reduced only when CPR without rescue breathing was performed. Scores on the Borg scale, a subjective score of fatigue, after CPR in a 3700 m environment were 13 to 15 of 20 (somewhat hard to hard). Performing CPR at high altitude exerts a significant physical effect upon the condition of rescuers. Compression-only CPR at high altitude may cause a deterioration in rescuer oxygenation, whereas CPR with rescue breathing might ameliorate such deterioration.
Introduction
A growing number of individuals with cardiovascular disease are ascending to high altitude, 1 thus increasing the potential for cardiac arrest in the field. Immediate cardiopulmonary resuscitation (CPR) is required in patients with cardiac arrest.2,3 However, the performance of CPR is effort-intensive even at sea level, and CPR at altitude is even more strenous. 4 –6
We previously described the application of prolonged CPR in a wilderness setting at high altitude on a trekker who developed cardiac arrest. The rescuer, who continued CPR during steep mountain transportation even though CPR in the lopsided, narrow carriage was very difficult, became exhausted after the work. 6 Following the aforementioned actions, we investigated the physical status of rescuers who provide CPR at high altitudes and found a significant impact on physiological parameters. 6 The Wilderness Medical Society practice guidelines for the out-of-hospital evaluation and treatment of accidental hypothermia advise that CPR can be stopped if it is futile. Additionally, CPR can be interrupted to facilitate evacuation and can be stopped due to rescuer exhaustion. 7
The most recent American Heart Association (AHA) guidelines state that compression-only CPR is simpler for lay providers to learn than conventional CPR (compressions with rescue breathing) and can even be coached by a dispatcher during an emergency. The AHA also determined that public education on compression-only CPR promoted the use of both overall CPR and compression-only CPR by bystanders. 8 Conversely, the opinion has been put forward that compression-only CPR is more exhausting than conventional CPR. It is reported that chest compressions to an appropriate depth decrease more rapidly during chest compression-only CPR owing to rescuer fatigue. 9 We also suspected that compression-only CPR and conventional CPR would have different physiological effects on rescuers, especially at high altitudes. Taking deep breaths prior to exhaling into a victim and the action of blowing against expiratory resistance (resistance of the airways and lungs of victims) seem to significantly affect the respiratory and circulatory status of would-be rescuers.
Methods
Data were obtained from trainees who voluntarily practice CPR under hypobaric conditions, in the expectation of a need for basic life support action when planning high altitude treks. Approval of the local human ethics committee (Gunma University research ethics committee for human studies no. 20-20) was obtained prior to analysis, and the protocol was registered in an internationally accessible clinical research database (UMIN; UMIN000020659) as an observational case study.
At the summit hut of Mt. Fuji, located at 3700 m, 3 male volunteers participated in this study. Participants had completed a basic life support and CPR training course (adapted according to international liaison committee on resuscitation guidelines) 3 before the field activity. All participants were office workers with no regular physical exercise regimen, and none had been exposed to altitudes over 2000 m during the half-year before the CPR practice. They passed prestudy health checkups, including chest x-ray, electrocardiography, and laboratory blood tests, and none had medical ailments such as cardiovascular or pulmonary disease.
Barometric pressure at altitude was 630 hPa, according to the local meteorological center at the time of field work. For measurements at 3700 m, participants were transported to an altitude of 2400 m by car and then ascended the last 1300 m on foot, while carrying a load of approximately 5 kg. Transportation by car from sea level to an altitude of 2400 m took approximately 4 h. The total duration required for the ascent from sea level to 3700 m was approximately 6 to 8 h. All measurements were obtained in wind-sealed constructions, and the temperature was maintained at 18°C. After arrival at the new altitude, participants were permitted 30 min of rest before performing CPR.
These 3 volunteers, who were training to be efficient high altitude rescuers, had arterial oxygen saturation and heart rate (HR) measured during practice of CPR at 3700 m. In the field work, the volunteers performed CPR after climbing, as expected in a real accident. They practiced both compression-only CPR and CPR with breath. At the summit of Mt. Fuji, we used a handheld oximeter designed for portability and durability (TuffSat; GE Healthcare, Helsinki, Finland). A probe for measuring percutaneous arterial oxygen saturation (SpO2) was always positioned on a finger because an earlier pilot test had shown that measurement during CPR was more stable with the probe on the index or middle finger than on an ear or toe. HR and arterial blood oxygen saturation were recorded every 15 s.
Borg scale scores were collected immediately after each CPR activity. 10 This simple scale of perceived exertion has often been used to regulate exercise intensity. A higher Borg scale score indicates a subjective feeling of greater physical intensity.
CPR was performed continuously as a single-operator procedure using a transportable CPR trainer (MiniAnne; Laerdal Japan, Tokyo, Japan) and according to the 2015 AHA Guidelines. 8 The mannequin was not wearing outdoor clothing, but the rescuers were clothed. The simulator was placed on a flat, wooden floor in the mountain hut. Compression-only and conventional CPR procedures were sequentially repeated twice without break, and the duration of each mode was 2 min. The rescuers then performed CPR for 8 min without resting. The rate of chest compressions was kept constant at 100 compressions·min-1 using a digital quartz metronome (CN89; Yamaha Musical Trading, Tokyo, Japan). The adequacy of chest compressions was monitored by measuring chest balloon pressures using a pressure gauge (CE0123; VBM, Sulz, Germany) connected to the balloon inflation valve. Study participants were advised to attain a peak chest balloon pressure of 30 to 50 cm H2O with each compression. This pressure value was determined by observing that a 4- to 5-cm chest compression on the simulator model produced results within this pressure range on the gauge (the depth of chest compression recommended in the 2015 AHA Guidelines is 5-6 cm). 8 During CPR with breaths, the adequacy of breathing was monitored by observing full inflation of the simulated lung. A compression:ventilation ratio of 30:2 was used, in accordance with the 2015 AHA guidelines. 8
The obtained data were given to the high altitude data analysis group working on “Health survey of the hypobaric hypoxic environment visitors,” an academic research project collecting biometric data from alpine tourists, to propose adequate health care during alpine hikes. Data are presented as mean±SD with range, as appropriate.
Results
Participants were 43±8 (36–54) y in age, 168±2 cm in height, and 59±1 kg in mass. They performed CPR for 8 minutes continuously. HR and SpO2 measured before and during CPR by the 3 participants are shown in Figure 1. HR immediately before the CPR was 95, 85, 123 beats·min-1 in Rescuers 1, 2, and 3, respectively. The maximal HR value was 128, 142, and 193 beats·min-1 in Rescuers 1, 2, and 3, respectively. HR increased during CPR in all 3 participants. The difference between maximal and minimal HR was 34, 57, and 94 beats·min-1 in Rescuers 1, 2, and 3, respectively. The HR in Rescuer 3 was extremely elevated during the early half of CPR practice; the maximum HR recommended for the age (220 − 36) was exceeded in Rescuer 3. However, the mode of CPR (compression-only or with breaths) did not affect changes in HR. The value in Rescuer 1 and Rescuer 2 increased during the second, compression-only CPR.
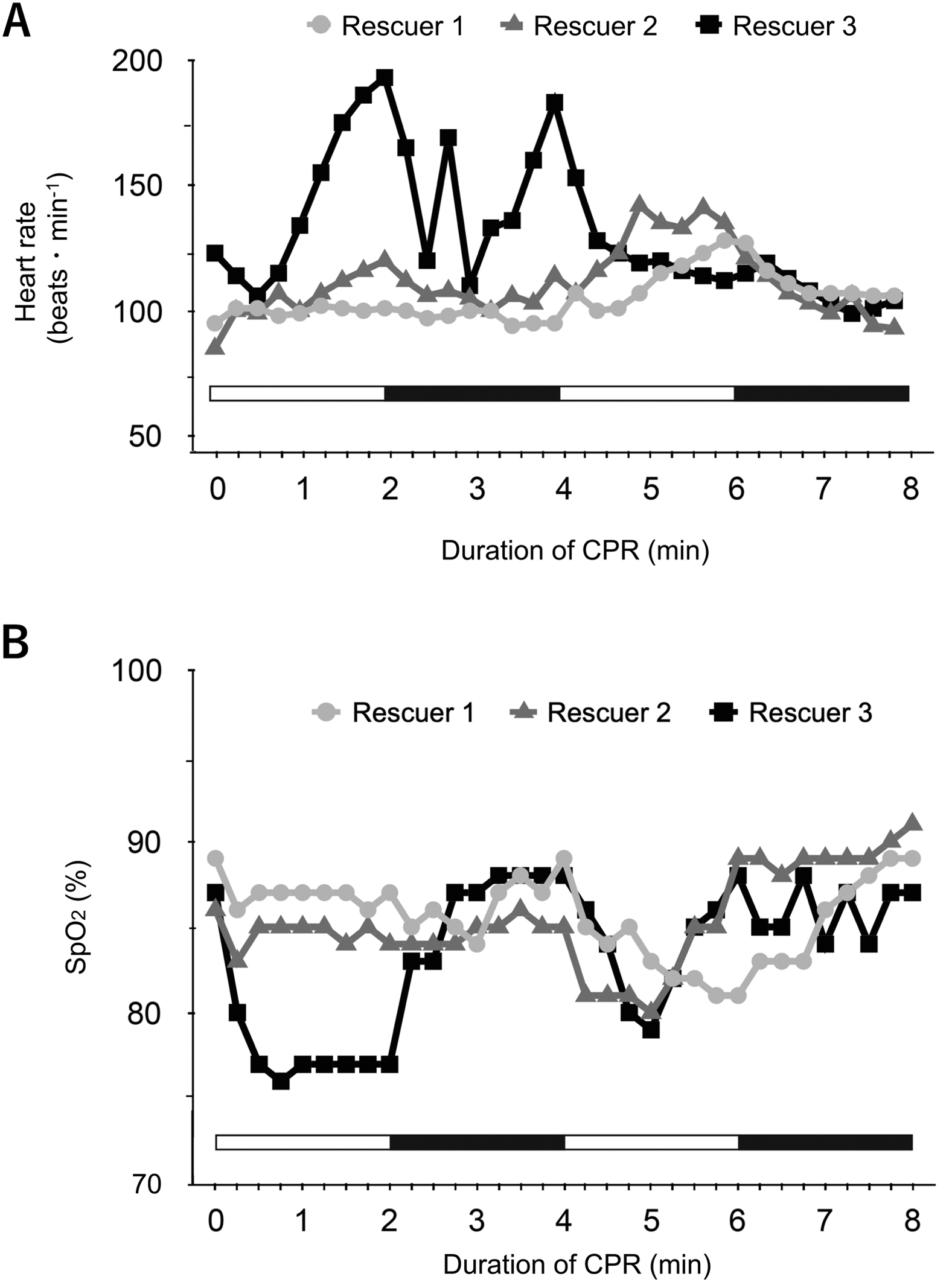
Changes in heart rate (A) and percutaneous arterial oxygen saturation (B) in 3 participants performing cardiopulmonary resuscitation at an altitude of 3700 m, on the summit of Mt. Fuji. White and black bars indicate periods for which cardiopulmonary resuscitation was performed in compression-only and with-breaths modes, respectively.
SpO2 immediately before the CPR was 89, 86, and 87% in Rescuers 1, 2, and 3, respectively. The lowest value was 81, 80, and 77% in Rescuers 1, 2, and 3, respectively. SpO2 was reduced during compression-only CPR in all participants, and the trend was most obvious in Rescuer 3. The difference between maximal SpO2 and minimal SpO2 was 8, 11, and 12% in Rescuers 1, 2, and 3, respectively.
The Borg scale score was 13 in Rescuer 1 and Rescuer 2, regardless of CPR mode. In Rescuer 3, scores during compression-only CPR and CPR with breaths were 15 (meaning hard or heavy) and 13 (meaning somewhat hard), respectively.
Because compression pressure was continuously monitored and the rhythm was indicated by metronome, the quality of the CPR in terms of adequacy of compression depth and frequency was confirmed by the rescuers and the attending observer. The 3 rescuers followed advanced cardiovascular life support (ACLS) guidelines, and quality did not decrease with time. The rescuers could meet the 30:2 compression ratio and ensured the chest rose and fell adequately with breaths. Rescuer 3’s CPR quality did not decrease during profound desaturations into the mid-70s.
Discussion
The present findings indicate that CPR in a hypoxic environment significantly affects the physiological parameters of providers. In particular, compression-only CPR seems likely to decrease oxygenation among rescuers.
We previously showed that applying CPR places major demands on the body at high altitude. 6 The degree of reduction in SpO2 observed in the present study was comparable to the values measured at an altitude of 3700 m in our previous study. 6 The relatively wide deviation in SpO2 among CPR providers was also comparable. Values for SpO2 vary among hikers at any given altitude.1,5,6 The frequency and mean of breathing both affect SpO2, more so at high altitude than at sea level, according to the degree alveolar CO2 partial pressure and positive end-expiratory pressure. When the breathing frequency is relatively low, CO2 partial pressure increases and alveolar O2 partial pressure decreases, which induces lower SpO2. When the positive end-expiratory pressure effect is intentionally or unintentionally provoked by each participant via pursed-lips expiration, O2 passes through the alveolar membrane more effectively, is loaded on hemoglobin, and induces higher SpO2 levels. These phenomena are not apparent at sea level, where ambient O2 pressure is not low. Furthermore, when O2 consumption and CO2 production increase during exercise, the reduction in SpO2 becomes more obvious. The information derived from the present study in the field is consistent with our hypothesis that CPR with breath might improve oxygenation in rescuers when compared with compression-only CPR at high altitude. The increase in HR among rescuers must be derived from an increase in oxygen demand from CPR.
Applying CPR has both physiological and mental effects, including feelings of fatigue. Scores on the Borg scale were high at 3700 m, where SpO2 decreased and HR increased. This is consistent with previous findings. 4 The latest guidelines recommend switching the personnel applying chest compressions every 2 min, based on findings of fatigue and an accompanying loss of CPR quality. 8 In particular, rescuers should switch every minute to maintain the quality of chest compression during compression-only CPR. 9 In remote, high altitude, out-of-hospital environments, few passers-by or colleagues might be able to apply CPR. Therefore, CPR is unlikely to be applied according to recommendations in such environments.
Limitations
This study had limitations. The small number of participants limited generalizability.
The mannequin simulator might not represent a person in cardiac arrest at altitude. The sheltered environment might not reflect actual evacuation circumstances. The participants rested before CPR, which may not reflect real-life circumstances. This report is intended to be hypothesis-generating, and the authors are not aiming to change ACLS protocols. Further research is recommended. Although our experimental conditions differed from a real rescue scene, a recent publication does describe the development of apparent hypoxia among CPR practitioners applying compression-only CPR in a hypobaric simulation chamber. 11
Conclusions
We compared the effects of CPR with or without breaths on cardiorespiratory dynamics at 3700 m. The work of CPR had a significant impact on the physiological parameters of participants. Compression-only CPR at high altitude may deteriorate rescuer oxygenation, whereas CPR with breaths might ameliorate such deterioration. Because CPR demands high exertion, especially at high altitude, CPR with breaths may be the preferred method. Because this is a case report with simulation, further research is required before CPR recommendations can be made.
Footnotes
Acknowledgements
Author Contributions: Data acquisition (TS, SS, MT, MK, YM); data analysis (TS, SS, MT); manuscript writing (TS, SS); critical review (TS, SS, MT, MK, YM).
Disclosures: None.
Funding
Financial/Material Support: This work was funded by the Japanese Ministry of Education and Science with JSPS grants to Shigeru Saito (Nos. 16H02678, 16K15673).