
Abstract
The imminent climate crisis has been labeled as the biggest health threat humanity must deal with. Vector-borne disease distribution and transmission as well as the population at risk are influenced to a great degree by environmental and climactic factors affecting both the vectors themselves and the causative pathogens. Paired with an increase in worldwide travel, urbanization, and globalization, along with population displacements and migration, elucidating the effects of anthropogenic climate change on these illnesses is therefore of the essence to stave off potential negative sequelae. Outcomes on different vector-borne diseases will be diverse, but for many of them, these developments will result in a distribution shift or expansion with the possibility of (re-)introduction of vector and pathogen species in previously nonendemic areas. The consequence will be a growing likelihood for novel human, vector, and pathogen interactions with an increased risk for infection, morbidity, and mortality. Wilderness medicine professionals commonly work in close relationship to the natural environment and therefore will experience these alterations most strongly in their practice. Hence, this article attempts to bring awareness to the subject at hand in a wilderness medicine context, with a focus on malaria, the most burdensome of arthropod-borne diseases. For prevention of the potentially dire consequences on human health induced by climate change, concerted and intensified efforts to reduce the burning of fossil fuels and thus greenhouse gas emissions will be imperative on a global scale.
Keywords
Introduction
Worldwide travel has been increasing steadily over the last decades, with especially leisure transportation and tourism expected to make a full recovery after the COVID-19 pandemic. 1 Our globalized planet is bound to become even more connected in the coming years. Of special importance for the field of wilderness medicine is the fact that destinations that were once considered too remote for “ordinary” travelers are now within reach for everyone. Although this may be a fortunate circumstance for many outdoor enthusiasts, it carries with itself a certain risk: Humans, some of them maybe with preexisting medical conditions that prevented them from traveling before or simply of older age,2,3 can now more easily enter areas where they will be exposed to potential dangers to health, be they related to their physical (eg, traumatic injuries, infections, and conditions provoked by unfamiliar environmental conditions) or mental well-being.
Specifically, infectious diseases have long been an important issue in wilderness travelers. 4 Epidemiologically, this pertains commonly to gastrointestinal infections, 5 but vector-borne diseases such as malaria, dengue and other arboviral infections (eg, chikungunya, West Nile, Zika, and yellow fever),6–8 leishmaniasis, 9 and tick-borne diseases 10 are not to be overlooked, particularly when venturing into warmer or even tropical destinations.
Another facet that will certainly have an impact on wilderness medicine is the impending climate crisis. Because of human influence, namely emission of greenhouse gases such as carbon dioxide and methane when burning fossil fuels, temperatures have risen a remarkable 1.1°C from 2011 to 2020 when compared with the period from 1850 to 1900. 11 This increase is only accelerating as we steer closer and closer to crossing the 1.5°C threshold 12 and thus to crucial tipping points in the world's climate. 13 Transportation, including leisure-related travel, especially via air,14,15 is responsible for a substantial amount of greenhouse gas emissions.16,17 Therefore, the question arises as to how leisure travel and tourism can be enjoyed in a sustainable 18 and globally just 19 manner, because human-made climate change universally affects all areas of the natural world; for instance, sea levels will rise, deserts will spread, the polar ice shield will thaw further, and weather extremes such as flooding and wildfires will be more and more common. 11 The world's population is threatened by these circumstances, which may very well result in massive health problems, (forced) migration, and conflicts. Overall, climate change and associated weather events appear to be one of the greatest threats to health we shall face in this century.20,21 Naturally, this is not limited to travelers or the local populace, not even to the human species; instead, global warming will bring massive changes to whole ecosystems, encompassing all flora and fauna.
Attention to the climate crisis is deservedly increasing incessantly. Although it is important not to neglect diseases of direct transmission, vector-borne diseases, especially those passed on by mosquitos, make up the lion's share of investigations with regard to infectious diseases and climate change. 22 A lot of thorough research has been published of late concerning this topic.20,23–26 This article attempts to bring a few of the relevant points into focus for a wilderness medicine audience, with special emphasis on the most pernicious of vector-borne diseases, malaria.
Methods
The intention of this narrative review is to provide a brief overview of the topic of vector-borne diseases, particularly malaria, and their interplay with climate change, stressing their importance for wilderness medicine. Although it is impossible to cover all worldwide changes or illnesses, this review still aspires to present some of the core developments on a global scale because the intricate relationship between climate, health, and disease is being altered not exclusively in certain areas or on certain continents but within this broad geographic scope. To meet this end, the method of selection was designed according to recommended standards and therefore employed a defined time period of query, several keywords and search engines, and report of inclusion and exclusion criteria. 27 Thus, articles were identified through internet search engines (ie, PubMed/MEDLINE, Google Scholar, LIVIVO, Ecosia, and DuckDuckGo) by using keywords as search terms, either independently or in different combinations. These keywords were the following: Anopheles, Aedes, arbovirus, climate, climate change, distribution, ecosystem, environment, expedition, geography, globalization, global warming, highlands, humidity, infectious disease, land use, malaria, migration, mosquito, outdoor recreation, Plasmodium, prevention, rainfall, Rickettsia, season, sustainability, temperature, tick-borne (disease), tourism, travel, urbanization, vector-borne (disease), weather, and wilderness medicine. The online supplemental table provides an overview of the independently searched keywords and their combinations.
Because of the accelerating importance of the topic in recent decades, the study period was limited from 1990 to the present. The articles were then reviewed scientifically regarding their impact and relevance. Emphasis was placed on including peer-reviewed studies, both with positive and negative (ie, failing to confirm the research hypothesis) findings. Articles summarizing the current scientific consensus such as narrative and systematic reviews and meta-analyses also were taken into account. Excluded from review were dispatches, pathologic and clinical case conferences, conference or scientific meeting presentations, poster abstracts, and redundant publications.
Vector-Borne Diseases and Climate Change
Although a complex relationship, it is well known that urbanization, alterations in patterns of land use, and specifically climate change greatly influence the geographic distribution and risk of transmission of infections. 28 These factors are suspected to have led to an aggravation in more than half of all infectious diseases pathogenic to humans. 29 In Europe, for example, two thirds of all relevant infectious diseases are sensitive to changes in climate; these changes may pertain to temperature, humidity, and the amount of fine particulate matter in the air. 30 Most notably affected are vector-, soil-, food- and water-borne infections.
With warming temperatures, the areas of endemicity of many vector-borne diseases will change, especially because many vectors as biting arthropods are ectothermic (ie, relying on external sources of heat to regulate their body temperature). 31 While these areas of endemicity have never been a static concept, environmental changes and especially human interventions have in a multitude of cases brought about a relative confinement of vectors and thus the diseases they bear. Even though some people argue that the extent of the influence of global warming on vector-borne diseases is as of yet uncertain 32 and there is an upper temperature threshold after which suitability of a geographic region for a vector declines, 25 it is most likely that the changes in our planet's climate will lead to a more widespread endemicity and transmission for many of these infections,20,33–35 putting more and more people at risk, both the local populace and travelers, tourists, and migrants.
For a vector-borne infection to occur, pathogen, vector (most often arthropods), and host have to come into close physical contact, paired with the right environmental circumstances, 21 including climate and weather, 32 with the latter referring to day-to-day variations in atmospheric conditions.
The following associations between vector-borne infectious diseases and climate (such as aforementioned temperature, wind, barometric pressure, and extreme weather events) as well as environmental factors (such as increased land use and the fragmentation or destruction of habitats) have to be considered. 25 First, the pathogen itself may experience a heightened or accelerated replication. 36 Second, the distribution of the vector carrying the infectious agent can become more widespread, with the species developing more quickly or exhibiting alterations in biting behavior and in its relationship with humans. Third, humans themselves also can change their activities and conduct, that is, spend more time outdoors or in different environments (eg, closer to areas of high vector population density such as still waters).
As mentioned earlier, the ectothermic nature of most arthropod vectors results in growth, development, survival, and spread being closely linked to environmental air temperature. 37 Commonly, these vector characteristics increase or accelerate with a rise in temperature; moreover, life cycles may speed up, leading to a higher population density. Nevertheless, there is an optimum in temperature. 38 Milder winters and longer summers usually mean a prolonged period of activity and population density for most arthropods,20,39,40 inducing an increased likelihood of meeting of vector and host.
Vector competence, that is, the specific capability for pathogen transmission by the respective arthropod after exposure to this pathogen, 41 is often used interchangeably with vector capacity, which ought to be the more quantitative measure. 42 This capacity is influenced by said competency but also by the local population density of the vector and of pathogen sources, its longevity, host preference, and the extrinsic incubation period, which, in turn, is directly affected by air temperature, where a higher temperature usually shortens the incubation period. 43 This temperature must stay within a certain range to facilitate transmission for a given period of time. 25 For becoming endemic in temperate climate zones, this vector–pathogen temperature threshold plays an important role; similarly, overwintering of infected vectors and vertical transmission (ie, between generations) must be guaranteed. Although this may vary between different vectors and pathogens, 44 it can be surmised that higher temperatures often go hand in hand with an increase in disease transmission,45,46 at least if the aforementioned upper threshold of the temperature optimum for vector competency is not broken.
Apart from these environmental and/or climate aspects, socioeconomic circumstances influence arthropod-borne disease transmission rates. Even though climate change may have multiple effects that may work diametrically (eg, more frequent occurrence of extreme weather events and temperatures), it can be said that warmer (but not extremely high) temperatures usually incentivize humans to spend time outdoors, partaking in warm-weather activities47,48 (which include water-based sports), thus increasing the likelihood of coming into contact with a vector. Moreover, continued urbanization may lead to an increase of breeding sites for some arthropod species (eg, Aedes mosquitos49,50) and a decrease for others depending on location and environmental factors (a good example for the preference of Anopheles for the rural environment 51 is the disappearance of gardens and still waters in Rome when transitioning into a modern city, facilitating a loss in breeding sites and hiding places 52 ).
Globalization, international transfer of goods and products, and tourism or travel may aid or help to accelerate individual vector species expanding their habitat, for instance, from warmer regions toward more temperate areas of the world. 53 Should this arthropod then by chance meet an infected host (eg, a returning traveler infected with the malaria parasite Plasmodium) and take a blood meal, autochthonous transmission could be established in the formerly disease-free area.
In all these ways, it is highly likely that climate change will and already is playing a substantial role when it comes to the distribution and transmission of vector-borne diseases. Of these, many possess particular relevance for wilderness medicine professionals. They include—among others—malaria (Plasmodium parasites transmitted by Anopheles mosquitoes), arboviruses such as chikungunya and Zika virus (transmitted by Aedes mosquitoes), dengue and yellow fever (transmitted by Aedes mosquitoes, chiefly A aegypti 54 ), and West Nile virus (transmitted mostly by Culex mosquitoes); Rocky Mountain spotted fever (Rickettsia ricketsii bacteria) and various other fevers transmitted by ticks, Lyme borreliosis (Borrelia burgdorferi spirochetes, transmitted by ticks, often of the genus Ixodes), and tick-borne encephalitis (a flavivirus usually also transmitted by Ixodes ticks); leishmaniasis (parasites of the Leishmania genus, transmitted by the phlebotomine sandfly genera Phlebotomus and Lutzomyia); African (Trypanosoma brucei gambiense/rhodesiense parasites transmitted by the tsetse fly [Glossina]) and American trypanosomiasis (Trypanosoma cruzi parasites transmitted by the so-called kissing or vampire bugs of the Reduviidae family/subfamily of Triatominae); and murine/endemic (Rickettsia typhi bacteria, transmitted by the flea Xenopsylla cheopis) and epidemic typhus (R prowazekii, transmitted by the human body louse Pediculus humanus corporis).4,55,56 Although this article does not concentrate on vector-borne diseases transmitted by non-arthropods, one would be remiss not to mention infections such as rabies and schistosomiasis as relevant for a wilderness medicine audience. For a more exhaustive list of vector-borne diseases transmitted by biting arthropods, see Table 1.
Overview of infectious diseases transmitted via arthropod bites
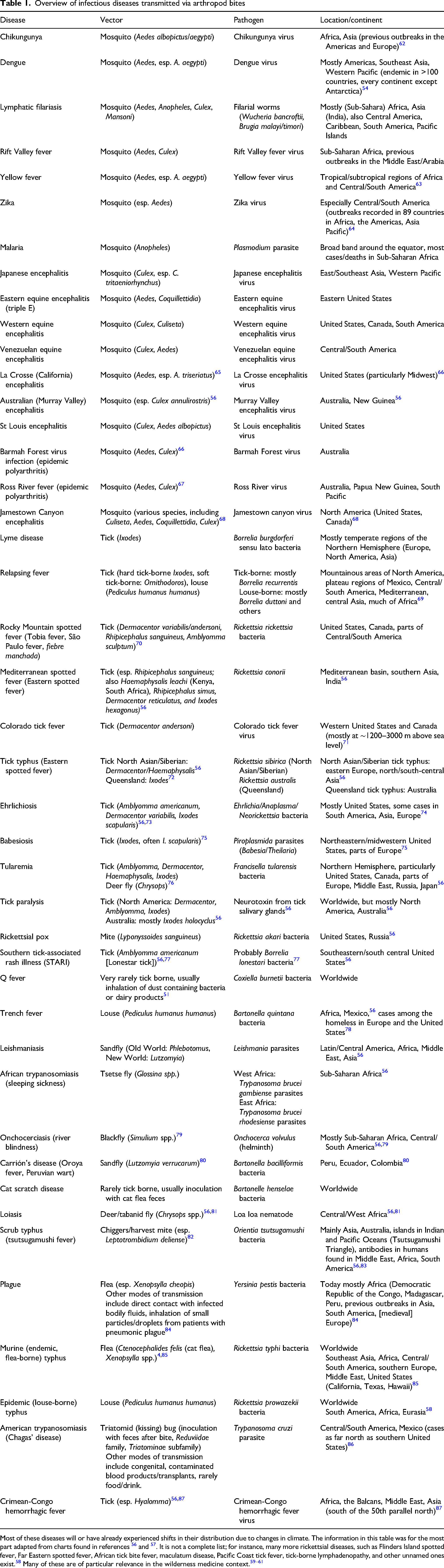
Most of these diseases will or have already experienced shifts in their distribution due to changes in climate. The information in this table was for the most part adapted from charts found in references 56 and 57 . It is not a complete list; for instance, many more rickettsial diseases, such as Flinders Island spotted fever, Far Eastern spotted fever, African tick bite fever, maculatum disease, Pacific Coast tick fever, tick-borne lymphadenopathy, and other unnamed ones exist. 58 Many of these are of particular relevance in the wilderness medicine context.59–61
Malaria in Wilderness Medicine
When it comes to vector-borne diseases, malaria is by far the most important on a global health scale. In 2022, there were 249 million cases in 85 malaria-endemic countries with 608,000 deaths, especially in Sub-Saharan Africa. 88 It is also known to be sensitive to changes in climate.89–92
Vector-borne diseases and especially malaria are of particular concern in travel and wilderness medicine.4,93 Malaria is caused by protozoan parasites of the genus Plasmodium, six of whom are known to infect humans, namely P. falciparum, P. vivax, P. ovale wallikeri, P. ovale curtisi, P. malariae, and the zoonotic P. knowlesi. Of these, P. falciparum is responsible for the majority of morbidity and mortality, especially in the Subsahara, whereas P. vivax remains the species with the largest area of endemicity around the globe. 88 The most vulnerable population for severe disease and death is made up of children under the age of 5 years and pregnant women, with an infection often leading to adverse birth outcomes as well. The Plasmodium parasites are introduced into a human's bloodstream through the saliva of an infected female Anopheles mosquito, which serves as vector. Concerning human malaria transmission, there are currently 41 dominant vector species of Anopheles globally. 94
The disease is not only an enormous health but also a significant socioeconomic burden on endemic regions, 95 causing and being caused by inequalities in both sectors.95,96 Hence, malaria eradication is an integral part of the Sustainable Development Goals of the United Nations (under Goal 3: Ensure healthy lives and promote well-being for all at all ages). 97
Today, malaria is found around the equator in both the Northern and Southern Hemispheres, but its distribution used to be a lot more extensive, reaching so far up north as, for instance, parts of Scandinavia and Russia in Europe.98,99 The disease was endemic on the European continent until the 1970s and has since been eradicated (except for a few cases that continue to arise due to travelers and migrants), particularly through control measures (eg, the draining of swamps, thereby reducing mosquito breeding grounds).
Characteristic for malaria is an intermittent fever, accompanied by (among other symptoms) cold sweats, a general malaise, limb pain, headaches, diarrhea, and organ swelling. Especially P. falciparum infection may result in complicated malaria, bringing about shock, renal insufficiency, seizures, coagulopathy, pulmonary edema, clouded awareness, and ultimately coma and death.
Treatment depends on the type of malaria, with artemisinin-based combination therapies being the first choice in P. falciparum infection, even though by now resistances against all types of antimalarials and major insecticides have appeared, jeopardizing eradication efforts.100–102 Other cornerstones of handling the disease are preventive measures such as vector control, chemoprophylaxis (of special importance in travelers), and, recently, two approved vaccines recommended by the World Health Organization (WHO) for young children in Sub-Saharan Africa. 103
In the wilderness, depending on location, malaria is one of the prime considerations for the cause of fevers4,56 and one of the main health risks when traveling to developing countries where it is endemic. 104 Moreover, it is the most frequently diagnosed disease in febrile migrants and travelers on a global scale, and the import of cases from endemic to malaria-free countries continues to be especially problematic. 105 Malaria thus is one of the most important differential diagnoses in returning travelers in both a wilderness medicine context 59 and in general. For all these reasons, the importance of the disease for travel and wilderness medicine is substantial. The most recent data indicate that 125 million international travelers are at risk for infection because they are visiting one of the more than 80 countries where malaria is endemic. 106 Hence, a lot of emphasis is placed on pre-travel information regarding bite prevention and chemoprophylaxis with medications such as atovaquone/proguanil, doxycycline, and mefloquine, which are advised by most international guidelines. 107
With this article targeting a wilderness medicine audience, it should be kept in mind that—even though regular tourism still may fall under the wing of this subspecialty—it often deals not only with “ordinary” travelers but also with people who may be seeking out especially remote or potentially hazardous environments for adventurous activities—expeditioners to all intents and purposes.108,109 Naturally, this situation brings with it a different risk profile for disease and injury. It can be speculated that such expeditionary travel more often goes hand in hand with travel to malaria-endemic (ie, tropical or subtropical) parts of the world and that the behavior of these travelers more often involves outside activities in areas with higher bite risk, sometimes for prolonged and/or uninterrupted periods of time, or includes outdoor exposures at times of day and night when Anopheles is most active (ie, between dawn and dusk).
Pre-expedition training has emphasized the importance of malaria, 109 and the disease plays an integral role in the wilderness medicine curriculum at different institutions.110,111 Prevention of malaria consisting of counseling (e.g, regarding chemoprophylaxis and personal protective measures) in a wilderness medicine setting is usually part of preparticipation evaluations, of medical planning for expeditions into remote terrain, and of medical clearance for sports, adventure, and endurance events depending on location.56,112–114 Travelers should be educated about the importance of chemoprophylaxis, the side effects of the medication, and symptoms of malaria, because any delay in treatment may incur potentially deadly consequences. 56 Before recommending any prophylactic antimalarial agent, the individual malaria risk (depending on destination, aforementioned activity profile, age, medical history, and duration of voyage) should be gauged while taking into account local resistance patterns and the option of potential self-treatment in case of infection.
Another pillar of malaria prevention in the wilderness traveler is represented by personal protective measures, among them insecticide treatment for bed nets, clothes, shoes, tents, and other equipment; long pants and long-sleeved shirts; skin insect repellents (eg, 10% to 35% N,N-diethyl-3-methylbenzamide [DEET]); and the reduction of activity during dusk and at night. 56 This thorough pre-travel process is especially vital because most travelers lack what is known as partial immunity, acquired through frequent exposure to Plasmodium.115,116 Naive adults acquiring malaria do experience remarkably higher rates of malaria symptoms and severe disease progressions while at the same time exhibiting different clinical presentations.117,118 In this context, special consideration must be given to particularly vulnerable individuals such as pregnant women and young children,119,120 still traveling to highly malarious areas where doing so may be considered unwise in general. 4
When venturing into any malaria-endemic region, every medical kit naturally should contain antimalarial agents, rapid diagnostic tests, and mosquito nets treated with pyrethroids such as permethrin (which, interestingly, are also susceptible to lowering of their efficacy due to ambient temperature changes 121 ). The argument could be made that the typical patient in travel medicine is in most cases not necessarily a sick person but arguably rather a client seeking advice (this is also partly the case in wilderness medicine, of course). With a high probability these humans (eg, tourists and expedition participants) come from affluent (Western) countries, and they are often willing and able to pay for the costs that malaria prevention with medication and equipment incurs. From a climate or global health justice perspective, it would be remiss not to mention that disposable income greatly affects one's ability to protect oneself from and/or treat not only malaria but also many other vector-borne infections. Due to this and many other factors, vector-borne diseases are a leading cause of death and disability in low-income countries. 122
Malaria, its Parasite, Vector, and Climate Change
As was established earlier, it is not uncommon for vector-borne diseases to be influenced massively in their distribution and transmission by climate phenomena. Malaria as a climate-sensitive disease is no exception. Even in their most recent World Malaria Report, the WHO stresses the risk for progress toward malaria eradication posed by climate change. 123 Moreover, the WHO's Global Technical Strategy for malaria was established in 2015, and it aimed for a reduction in incidence and mortality rates by 40% by 2020, 75% by 2025, and 90% by 2030; as of right now, these goals have not and also are not projected to be met. 88 Several extensive review articles exist that deal (at least in part) with the topic of malaria and climate change23,24,26,28,89,124 or with certain areas of malaria endemicity.25,125–128 The following thus can only attempt to provide a brief overview of the subject.
Similar to other ectothermic vectors, several species in the mosquito family are remarkably sensitive to air temperature changes, with numerous studies demonstrating effects on growth and reproduction rates (eg, through fecundity, ie, how many eggs a female lays per day and egg-to-adult survival), metabolism, lifespan, biting behavior, immune system (as well as their capability of pathogen transmission), infection probability, and extrinsic incubation period (ie, the time required for sporogony or until the mosquito becomes infectious) in different genera. 121 Plasmodium spp. complete their sporogonic cycle about twice as fast at 28°C compared with 22°C, although total duration differs between species. 26 With climate change, colder regions most likely will see a rise in suitability for mosquito-borne diseases, whereas those close to the transmission temperature optimum or above this threshold will see this suitability decline. Correspondingly, malaria transmission is defined by limitations in season and geography because of temperature variations. 121
It has been observed that there is additional transmission of mosquito-borne infections after intense rainfall. 121 Precipitation and hydrology, hours of sunshine, and relative humidity strongly affect Anopheles and malaria, albeit with a relative delay.92,129 There has to be an abundance of water (eg, lakes, ponds, containers, or puddles) for the immature aquatic or semiaquatic larval and pupal stages’ optimal growth.38,129 Higher humidity usually results in positive effects on survival, drought resistance, egg production, and development for Anopheles. 25 In Africa, where most of morbidity and mortality for malaria are found, the mean temperature—except a few highland, southern, and northern regions—is above 25°C. 130
The International Panel on Climate Change uses model algorithms for prediction of emissions scenarios to gauge global warming by the end of the century. The rise in temperature spans from a predicted 1.4°C (very unlikely, in the lowest greenhouse gas emissions scenario) to 2.7°C (for an intermediate emissions scenario) and even up to 4.4°C (high greenhouse gas emissions scenario) worldwide until 2100. 11 Some people argue that this most likely will result in more rapid development of the parasite and an increase in a general malaria incidence not only but also in large parts of the continent most afflicted. 131 Others suspect more diverse outcomes depending on the scenario because of the nonlinearity between temperature and transmission and the climax of malaria incidence under laboratory conditions falling at ∼25°C. 124
All this underlines nonetheless that it must be kept in mind that the relationships between climate, parasite, and vector are highly complex and, to a certain degree, volatile. Global warming will not be equal in all regions, serving the malaria vector only as long as the optimal temperature threshold is not broken—in essence, extremely high (and, vice versa, extremely low) temperatures also may hinder mosquito growth and malarial distribution.124,128 Transmission also increases with temperature but reaches a climax at a certain point and then decreases again. 132 On the surface, the rise in temperature incited by climate change, particularly during a long-term high-emissions scenario, might have the appearance of being beneficial for Plasmodium because it would result in temperatures outside the temperature optimum of the vector and/or parasite. The other consequences of this ambient temperature increase, however, would be dire: There is a relationship between various nontransmittable diseases and high temperatures (especially regarding cardiovascular and mental health problems), and the negative effects on agriculture, biodiversity, and whole ecosystems would be extreme, for instance rendering parts of Africa unlivable. 124
In the short term, the aforementioned WHO Global Technical Strategy will be adversely affected by the modeled smaller temperature increases because this will bring the parasite closer to its transmission optimum, particularly in the most vulnerable regions. Nevertheless, efforts to stay within the lowest emissions scenario will help to delay this transmission zenith. 124 Although the tolerated ambient temperature varies among Plasmodium species (the increased tolerance for lower temperatures possibly facilitating the bigger spread of P. vivax), 26 there are also data that indicate differences in climate sensitivity between species.133,134 Moreover, extreme weather events such as floods may flush away larvae initially, decreasing transmission,128,135 but data from Pakistan, where there were extreme weather events that included melting of glaciers, surges in rivers, and extensive flooding, suggest that malaria cases increased fivefold afterwards due to an increase in standing water. 88 As mentioned earlier, local wind conditions and land use and cover (eg, through [de-]forestation) have an influence on mosquito and host populations. 38 Forest ecosystems usually are beneficial for malaria transmission; still, logging may aid larval development through the exposure of still waters to sunshine as well as advantage the mosquito in general through novel formation of habitats and changes in microclimate, precipitation, and wind. 26 Irrigation efforts for agriculture, of increasing priority with global warming and growing populations, have been shown to boost malaria incidence in areas of unstable transmission, where most of the population possesses little to no protective immunity.26,136
Climate change has already caused migration and displacements of human populations. 11 This will only be aggravated in the future and may contribute to emerging unrest, political instability, and even wars, environments in which infectious diseases and malaria in particular are known to thrive for a multitude of reasons (eg, overcrowding, breakdown of healthcare systems and control efforts, infected individuasls carrying the parasite to previously nonendemic areas, etc). Apart from returning travelers, there is evidence that (asymptomatic) malaria prevalence is high in refugees, asylum seekers and during mass population displacements as well as humanitarian emergencies, where the disease may lead to a further breakdown of health services and the general situation.137–139
Malaria transmission is intensified in rural settings, with urbanization facilitating a loss in breeding sites. Nevertheless, in areas where this process occurs rapidly and without structure, poverty, close proximity of humans, and deteriorating infrastructures have to be considered as risks for malaria. 26 Anopheles is also capable of adapting to modifications in its habitat (eg, contaminated waters) and thus also can expand into polluted environments. 26
In total, it is widely speculated that global warming will lead to an increase in the incidence and geographic distribution of malaria; nevertheless, others argue that the evidence is too sparse for a clear attribution of local resurgences or spreads in geographic distribution to changes in climate, warranting further research. 128 The duration of the malaria transmission season is set to increase in the highland regions of the world (eg, some parts of Africa, Central and South America, Australia, and the Indian subcontinent), whereas in tropical areas it will rather decrease. 89 Anopheles distribution in Africa probably will move from the west further east and south, and although this may result in a decrease of disease burden, new populations will be affected, where the public health system is not yet fit to deal with an upsurge of malaria cases and control measures are not in place. 26
In summary, potential direct effects of climate change on malaria in areas below the optimal transmission threshold include an expanse in geographic limit in currently malaria-free territories, an increase in transmission intensity, and a reintroduction of the disease where it was recently eliminated. 88 In regions where the mean temperature is already close to the optimum, a decrease in transmission intensity may be observable because vectorial capacity, survival, biting, and sporogony decrease above 28°C, with temperatures of 36°C usually not survivable for mosquitoes. Aridity further hinders transmission. Where rising temperatures have no influence on vector dynamics, transmission intensity likely will remain constant. Indirect effects of global warming that have an influence on malarial incidence include insecurities in socioeconomics and food—it is well known that malnutrition increases disease susceptibility—human displacement and disruptions in services and healthcare, and more challenging implementation and execution of malaria control programs, at least partly because of a rise in costs. 88
Anopheles distribution in the Northern Hemisphere will expand further northward due to higher temperatures, with accelerated mosquito development and oogenesis, an increase in population density and a shortened incubation period resulting in a heightened vector potential, especially in Europe. 25 Plasmodium parasites have a very high host specificity. 140 Therefore, for upkeep of transmission, apart from female Anopheles acting as competent vectors and fitting environmental conditions (ie, temperature and humidity), untreated, gametocyte-bearing (ie, carrying sexual forms) humans must exist. Hence, for Europe, the risk of a substantial increase in autochthonous malaria cases remains quite low as long as socioeconomic standards and access to health services remain stable. 25 Nevertheless, between May and July 2023, eight locally acquired P. vivax malaria cases were reported in the southern United States, seven in Florida and one in Texas, 141 illustrating the possibility of local propagation even in countries with highly developed health systems. For prevention of autochthonous transmission occurring in previously malaria-free areas, pre-travel counseling and education, chemoprophylaxis, and bite avoidance must be emphasized in travelers.
Implications of Climate Change on Vector-Borne Diseases for Wilderness Medical Practitioners
Our world is faced with a climate emergency, 142 and these changes in climate have been declared by the WHO to be the single biggest health threat for humanity. 88 Accordingly, the ramifications for wilderness medicine will be striking. Delivering care to austere and wild environments or treatment of those who sojourn in these settings will be complicated by the alterations engendered by global warming, and the relevance of this type of medicine arguably will be greater than ever.143,144 Hence, the implications of climate change on wilderness medicine and recreational activities in general (with special reference to vector-borne diseases such as malaria) had been noted by practitioners in the field as early as 1992. 145
With changing—and in most cases expanding—geographic distributions of vector-borne disease incidence and transmission, a larger part of local populations and travelers will be at risk of infection. This, of course, also entails other medical conditions made more likely by climate change, now encountered in areas that were previously thought innocuous (eg, hyperthermia-induced illnesses such as heat exhaustion and increased morbidity and mortality of cardiovascular diseases during extreme heatwaves146,147). Wilderness and travel medicine professionals need to be aware of this increase in risk, in the field, during pre-travel counseling and in returning travelers and people visiting friends and relatives.
Shifting disease and incidence patterns make it necessary to familiarize oneself with the current situation and circumstances. Frequently affected by an incidence increase are territories favored by expeditionary travelers. With malaria, already alluded to earlier, outcomes will be mixed and depend on the region concerned. Areas where there are sufficient data to draw conclusions encompass the Subsahara and (sub-)tropical highland regions.23,35,88,89,144 In Sub-Saharan African children, investigations concluded that anthropogenic climate change has led to a rise in malaria prevalence with 2:1 odds. 88
A well-known fact in the outdoor community is that temperatures decline with increasing altitude. In the troposphere, temperatures drop, on average, 6.5°C for every kilometer of altitude gained.56,148 For many vector-borne diseases, this means that global warming allows them to expand their habitats into higher, more mountainous regions, which are frequently chosen as outdoor recreation destinations by hikers, climbers, and the like. In the case of malaria, in the cooler highlands, for the most part previously malaria-free zones, a slight warming of the climate most likely will lead to higher case numbers, as was shown for the highlands of East Africa,149–157 South America,89,154,157,158 Asia,89,144,159 the Western Pacific region, 35 and the Eastern Mediterranean. 157 Most data are found for the East African highlands, even though some people suggest that attributing malarial incidence increases to climate change alone may be simplifying the issue, 26 not taking into account factors such as resistance patterns and control efforts. 160 Be that as it may, numerous studies have shown an association with a higher malaria case-fatality rate in international travelers for East Africa compared with other regions of the continent. 161
The developments in the more mountainous regions of the world are, of course, of particular relevance to the discipline of wilderness medicine, representing prime destinations for outdoor travel, recreation, and expeditioning and for climbing, hiking, and other activities. For instance, the main malaria vector in the highlands of northern Tanzania, Anopheles arabiensis, has experienced a pronounced range expansion in higher altitudes due to changes in climate and land use, affecting the popular climbing destination of Mount Kilimanjaro. 162 In general, usually little malaria transmission occurs at over 1800 to 2000 m above sea level, even though individual mosquitoes of the Anopheles gambiae complex (to which An. arabiensis belongs) have been observed at altitudes up to 3000 m. Hence, the human population there harbors only a low degree of protective immunity. 26 With the International Panel on Climate Change noting the expanding habitat of malaria into more mountainous regions, there is great potential for epidemics with high morbidity and mortality, an aspect underlined by outbreaks having taken place at higher altitude in Rwanda, Uganda, and Kenya recently. 26
Similarly, this phenomenon of a rise in risk for infectious diseases such as malaria, dengue, Japanese encephalitis, and cholera is projected to occur in the Greater Himalaya region, also affecting the local population in remote villages. 144 Although mentioned earlier, especially from a sustainability and global justice point of view, it needs to be stressed that of course one must not only think of the expeditioner but also of shifting incidences and risk patterns in the local population, in some cases expediting transmission or requiring increased medical attention by a wilderness medical professional when employed abroad. For instance, two thirds of the populations of Ethiopia, Kenya, and Tanzania live in areas with an altitude of 1000 to 2500 m above sea level, the range that is most strongly affected by effects of climate change on malaria incidence. 154 In addition, the East African highlands in general belong to the most populated regions on the continent with one of the highest population growth rates on the planet. 151
Not only may the incidence of a certain illness change with global warming, but whole disease patterns also may be altered. For instance, for Sub-Saharan Africa, climate change may incur a move of the ambient temperature away from the suitability for Anopheles and malaria toward arboviruses such as dengue (Anopheles gambiae malaria transmission reaches its zenith at 25°C compared with Aedes aegypti dengue transmission's optimum at 29°C) or chikungunya. 127
The subject of planetary health or “one health” is closely connected to issues presented here, but overall too comprehensive to not go beyond the scope of this article. However, one interesting aspect must be mentioned on the topic of highly populated mountainous regions: Climate change also will facilitate novel viral sharing among mammal species, with animals and humans collocating especially at higher altitude and in densely populated areas in both Africa and Asia. 163
Tick fevers are one of the most common reasons for evacuation on wilderness expeditions in the United States. 5 Although the incidence of tick-borne illnesses in the field remains low, almost all cases in cohort studies required evacuation, 10 rendering these diseases of special concern for the wilderness medical professional. With a longer life cycle than mosquitoes, ticks are not as affected by changes in weather. 33 Nonetheless, many tick-borne diseases or their vectors have experienced a growth of their geographic range, seasonal activity, and abundance with climate change.10,20,164,165 This is true for the more temperate regions of the Northern Hemisphere, where ticks expand their habitat further northward and—similar to mosquitoes—to higher altitudes, including major wilderness travel and climbing destinations, such as the Alps. 20 Another factor with tick-borne illnesses is not only the distribution of the vector but also the distribution of wild hosts (eg, deer, birds, and rodents) and livestock, which also will change in light of the climate crisis. Because of this, and because numbers of trekkers and other people spending their leisure time outdoors are steadily rising, the exposure to tick-borne pathogens will only be altered further. 20
To prevent the expansion of vector-borne diseases in the face of the climate emergency, reductions of greenhouse gas emissions will be of preeminent importance. Measures to curb these emissions need to be put in place, or if they are already established, they must be intensified on a global scale. Though this may not completely thwart global warming and avert all consequences of the changing climate, it will at least decelerate the occurrence and/or attenuate the severity of negative sequelae. 25 However, such action will necessitate intense interdisciplinary efforts on the political, biological, scientific, and, last but not least, individual scales. Politically, plans need to be made to hamper the import of infected vector species, and local vector control measures should be put in place or intensified, for instance, in (urban) planning, architecture, and land use. 25 Research and development in diverse fields and especially of therapeutic agents and insecticides must be reinforced, for instance, by supporting scientists and investigators. Further research is also needed to elucidate the attributable effects of climate change on diseases such as malaria. There is an inherent necessity for the merger, integration, and analysis of epidemiologic with biological, environmental, climatic, and demographic data. 166 Additional emphasis should be placed on the rapid reporting and treatment of cases, 25 requiring healthcare professionals such as wilderness and travel doctors with experience in the diagnosis of and approach to these diseases.
While mitigation of the effects of climate change is certainly a worthwhile pursuit, it may not always be possible or only to an extent where the effects will still be too pronounced to simply accommodate them without further action. This is where thorough plans for adaptation will be essential, thus proactively reducing the health risks afforded by changing infectious disease distribution and transmission due to the climate crisis. Adaptation assessments represent the first step in this process, evaluating and prioritizing potential measures and policies in light of their effectiveness and resource requirements. 167 Specific guidelines and strategies for such adaptive processes exist in the realm of infectious diseases (eg, by the European Centre for Disease Prevention and Control 168 and the Centers of Disease Control and Prevention of the United States 169 and under the United Nations Framework Convention on Climate Change, 170 to name just a few). Although these assessments of climate change, health vulnerability, and adaptation strategies have at least in part been helpful for authorities and researchers, significant hurdles still abound when it comes to access to relevant data, certainty of climate projections, funding, and implementation of the policies deemed effective. 171 Nevertheless, adaptation options are projected by researchers to significantly reduce the number of cases and in the case of vector-borne illnesses may consist of many factors, some of which overlap with the aforementioned mitigation strategies. These include improved disease and outbreak surveillance, reduction of exposure to vectors (eg, through window screens, 25 adequate clothing and insecticides, and avoidance of habitats), monitoring of air passenger numbers and vectorial capacity as potential early-warning measures, eradication of vector breeding grounds (eg, through wetland management), and the development or implementation of novel vector-control methods and vaccines (where possible). 166
On an individual level, travelers must be educated regarding prophylactic measures (eg, bite avoidance or sleeping under bed nets), made aware of the risk of reintroduction of tropical diseases into their home countries and, depending on the disease, should make use of chemoprophylaxis. Crucially and perhaps most important, one needs to keep in mind how and to what degree one's own behaviors and lifestyle are contributing to climate change. Because of the close association between nature and their line of work, wilderness medicine providers should be especially aware of their exemplary status and therefore act as paragons for environmental protection.
Conclusion
Vector-borne diseases are affected by changes in environment and climate. The repercussions are already noticeable and manifold and will continue to massively alter the distribution, transmission, and size of the population at risk. Among these illnesses, malaria exerts the highest toll on human health—hence, the interplay between climate change and this disease is of great importance. Outcomes of global warming on vector-borne diseases in general and malaria in particular will be diverse and depend on location and time scale. It is essential for wilderness medicine professionals to be mindful of these changes in risk. They will need to provide thorough and concise pre-travel education and counseling and post-travel surveillance and always consider vector-borne diseases when in the field, especially in febrile patients. Future research should attempt to further decode the intricate interactions between vector-borne diseases and climate change to mitigate and decelerate negative consequences. Paramount for this is also a continuous concerted and intensified global endeavor for a reduction of greenhouse gas emissions.
Supplemental Material
sj-docx-1-wem-10.1177_10806032241283704 - Supplemental material for The Influence of Climate Change on Vector-Borne Diseases in a Wilderness Medicine Context
Supplemental material, sj-docx-1-wem-10.1177_10806032241283704 for The Influence of Climate Change on Vector-Borne Diseases in a Wilderness Medicine Context by Jonas E. Mertens in Wilderness & Environmental Medicine
Footnotes
Acknowledgments
The author would like to express his thanks to the anonymous peer reviewers for their helpful comments and corrections.
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental table of used keywords mentioned in the Methods section can be found in the online version at https://doi.org/10.1177/10806032241283704.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.