
Abstract
Introduction
Some experts recommend that ambulant hypothermic patients should be rewarmed, fed, and not permitted to exercise for 30 min because of concerns that afterdrop can cause cardiac instability. We investigated the outcome of ambulant hypothermic patients in a case series from mountain rescue teams in Great Britain.
Methods
A questionnaire was used to collect information on a series of adult patients with a clinical diagnosis of mild hypothermia. All patients were alert on the AVPU scale and evacuated by walking from the mountain. The outcome measures were survival or a change in management because of medical deterioration during evacuation.
Results
A series of 108 eligible cases were reported over a 5-year period. When rescuers arrived on the scene, 98 (91%) patients were stationary, and 10 (9%) were still mobile. Thirty-eight (39%) of the stationary cases were walked immediately off the mountain without any on-scene delay. In the remaining 60 (61%) stationary cases, the decision was taken to delay evacuation to provide food, drinks, and additional clothing. In 3 cases, the use of heat packs indicated an intention to actively rewarm. In cases where the on-scene time was reported, 27 (79%) were known to be mobile again within 20 min. All patients survived, and no adverse medical events occurred in all 108 cases.
Conclusions
In this study, no adverse events occurred because of immediate mobilization, suggesting that in these cases, there appears to be minimal risk of early activity.
Introduction
Hypothermia is an involuntary fall in the body's core temperature to <35°. The International Commission for Alpine Rescue (ICAR) endorses the use of the Swiss Staging System for accidental hypothermia, which bases out-of-hospital decisions on clinical observations rather than core body temperature.1,2 This is because noninvasive measurement of core temperature in the field is difficult and unreliable.3,4 Conscious level is a good clinical sign in hypothermic patients to identify the risk of cardiac arrest and is used in this way in the Revised Swiss System, adopted by ICAR in 2021. 5 A subsequent retrospective study confirmed the validity of this assumption. 6 The ICAR-endorsed guidelines recommend that patients who are fully conscious and who may be mildly hypothermic can be mobilized promptly if this will help the rescue. 1 However, this practice is controversial. The Wilderness Medical Society (2019) guidelines recommend that patients with mild hypothermia should avoid standing or walking for 30 min once they have been protected from further heat loss and been given food to replenish energy stores.7,8
The concern was that early mobilization may increase afterdrop, thereby bringing the temperature down into the range of hypothermia-induced cardiac instability and potential cardiac arrest. Afterdrop is the continued fall in core temperature observed when a hypothermic casualty has been removed from the cold environment. It is due to a combination of direct heat loss from the warmer core to cooler peripheral tissues and cooling of the blood due to increased flow to cold muscles and subsequent return to the heart. The recommendation to limit activity was generalized from a small study of mildly hypothermic volunteers rewarmed by shivering alone, exercise, or exercise after an afterdrop period; those who exercised immediately experienced the greatest amount of afterdrop measured as 1.1 ± SD 0.4 °C. 9 However, other experts argue that this guidance could cause harm because a delay in mobilization can result in a prolonged rescue and unnecessary cooling. They suggest that the clinical significance of afterdrop in such cases is unknown and that early mobilization of a mildly hypothermic patient with no co-morbidities is safe. 9
The Mountain Rescue England and Wales (MREW) database 2019–2021 (not open to public access) shows that 4% of all casualties were considered to be hypothermic. In a report from Scottish Mountain Rescue (SMR), 14% of casualties were identified as suffering from the effects of cold or exhaustion. 10 The frequency of adverse events in ambulant hypothermic patients is unknown but is of significance to rescuers in the field. This study identifies a series of clinically cold and potentially mildly hypothermic patients who have been assessed by rescue team members and walked to safety.
Methods
All mountain rescue (MR) teams in England, Wales, and Scotland were asked to provide retrospective details about patients with mild hypothermia rescued between January 2018 and November 2023. Patients were excluded if the cause of hypothermia was cold water immersion. Otherwise, the entry criteria for the study were:
The incident was attended by a mountain rescue team. The subject was an adult aged ≥18 years. The weather conditions were compatible with causing hypothermia (eg, cold, wet, windy). The incident was in a location that could not be accessed by a normal road ambulance. The patient had a normal conscious level (AVPU = A) on initial assessment. The patient was initially evacuated by walking unaided from the scene (assistance to cross difficult or steep terrain safely was permitted). Patients were accepted into the study if either the temperature was measured and hypothermia confirmed, or they had clinical features suggesting mild hypothermia (eg, cold, possibly shivering, exhausted, normal cerebral function). Rescue team details and contact information When and where the incident occurred Patient's age, gender, and medical co-morbidities The activity that was being undertaken (walking, climbing, mountain running, etc) The type of incident (lost, injury, illness, exhaustion, etc) Conscious level of the patient (AVPU) on initial assessment Whether body temperature was recorded, and if so, by what route Whether the patient had been stationary before the rescue team arrived Whether the patient was able to walk unaided Whether evacuation was deliberately delayed to refuel and rewarm the patient If so, the length of time evacuation was delayed and actions taken Whether the patient was initially evacuated by walking and the evacuation time Adverse medical events during evacuation Outcome at handover (survived or died) Destination after rescue
An electronic questionnaire was designed to collect the following information:
A pilot questionnaire was sent to four MR medical officers and revised based on their feedback. The amended questionnaire was emailed to all rescue teams in England and Wales (47 teams) and Scotland (32 teams).
All patients were assessed clinically by MR first aiders who hold a current MR Casualty Care Certificate or MR healthcare professionals. Patients were considered suitable for inclusion if there was an appropriate history; the casualty felt or looked cold, was shivering (or had been), was wet, had been sitting on a hillside, especially in adverse weather conditions; or body temperature was measured. The clinical stage of hypothermia was assessed using the Revised Swiss System to assess the risk of hypothermic cardiac arrest based on conscious level. 5 Shivering is no longer used as a stage-defining sign, as it is known to be an unreliable indicator of hypothermia severity, so we did not ask if this was present. The evacuation time was used as an indicator of the amount of energy used by the patient during evacuation. It depends on multiple factors, such as distance, height ascended, nature of the terrain, and fitness. To maximize the number of questionnaires returned, the details of the study were described to the teams during training events, face-to-face meetings of the medical committees, an article published in the national mountain rescue magazine, and recruiting leaflets sent to all the teams. The databases in participating organizations were also searched for suitable cases, and the teams requested to review their suitability for the study. All teams were sent reminders 3 times during the study period. To verify that each case was suitable, the entry criteria were included in the questionnaire. The teams were instructed to use data from incident reports, casualty report forms, and electronic records to complete the returns and ensure that the data was accurate. The returns were automatically entered into a spreadsheet. Noncompliant cases were removed, and the cleaned data set was analyzed using descriptive statistics and a narrative review of the data.
Results
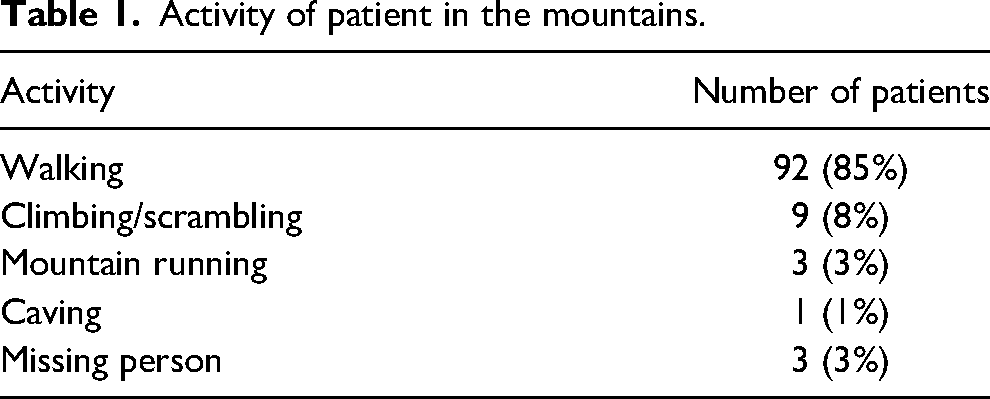
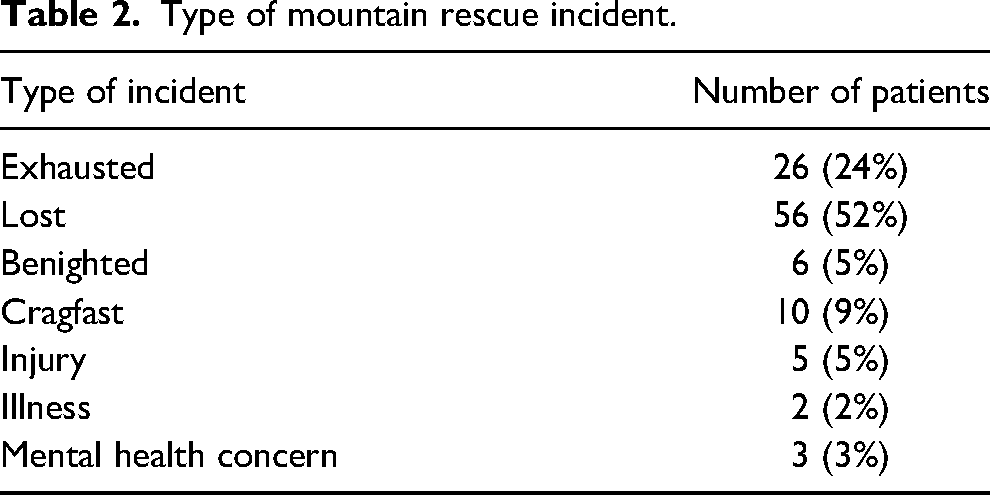
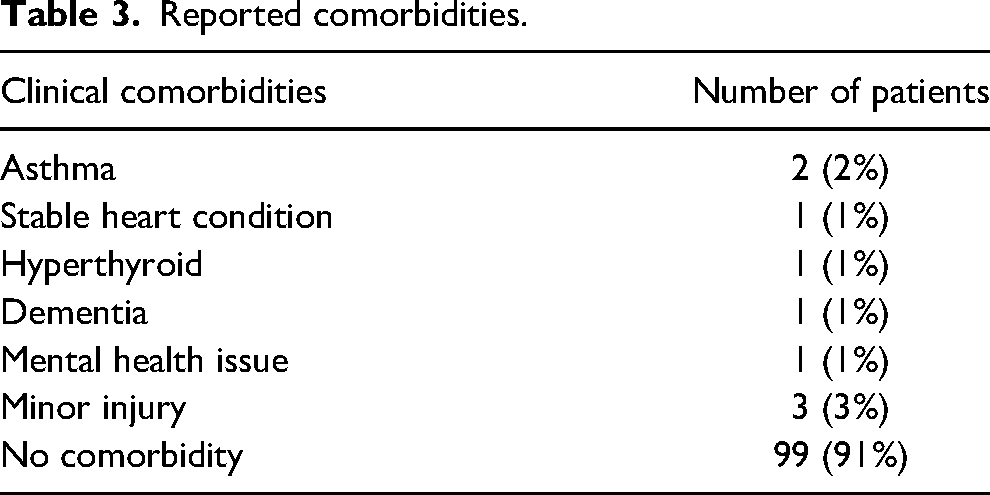
There were 118 cases submitted. Ten cases did not meet the entry criteria and were removed. The analysis was completed on 108 cases. Cases were submitted from all 3 participating countries: England (23%), Wales (43%), and Scotland (34%). The number of different teams submitting cases was 7 in England, 4 in Wales, and 9 in Scotland. Teams used several contemporary sources to report the cases, including the incident log, the patient report form, and other sources. Over half of the reported cases—64 (60%)—took place before January 2022, with 44 (40%) after January 2022. There were 63 (58%) males and 45 (42%) females. The age range was 18–80 year old. There were 79 (73%) patients in the 18 to 40 year age group, 21 (19%) in the 41 to 60 year age group, and 5 (5%) over 60 years. Age was not recorded for 3 (3%) patients. Tables 1 and 2, respectively, show the activity of the patient and type of rescue incident. Patients were mainly walkers and either exhausted or lost in the mountains. There were 9 patients with comorbidities (Table 3).
Activity of patient in the mountains.
Type of mountain rescue incident.
Reported comorbidities.
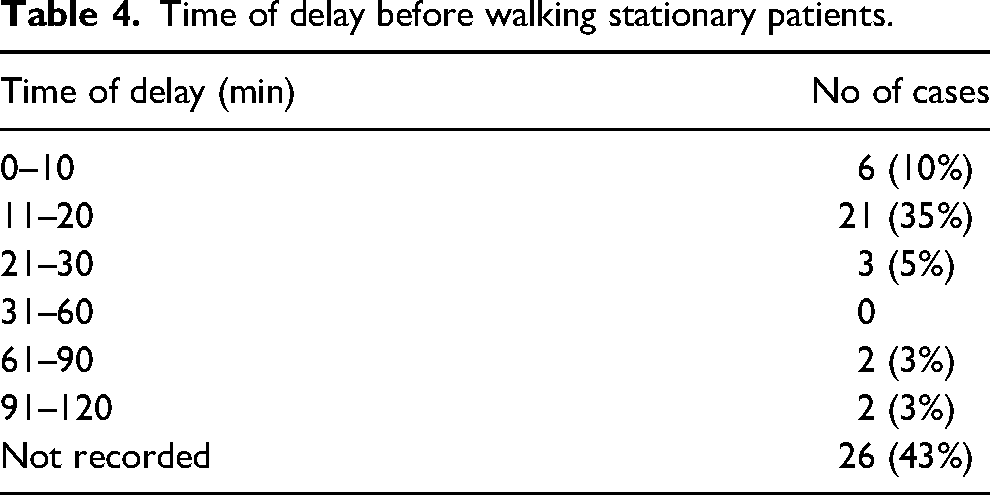
All patients were assessed using external clinical observations. One patient had their temperature taken during their assessment using an oral thermometer, which was 34.4 °C. Ten patients (9%) were still mobile when the rescue team arrived. Of these, 2 were given food, fluid, and clothing and then evacuated without delay by foot, and the other 8 continued without on-scene delay. All 10 were evacuated without adverse events. Ninety-eight (91%) patients were stationary when the rescuers arrived on the scene. In 60 (61%) of these, rescuers delayed evacuation, and 38 (39%) were walked immediately off the mountain without delay. For the 60 stationary patients, when there was a delay on-scene, the action taken during the delay was recorded in 44 (73%). In all cases, it was to provide additional clothing, food, and drinks. In 3 cases, rewarming with a chemical heat pack was specifically mentioned. Two patients required a delay for treatment to minor injuries not affecting mobility. The time taken to complete these actions prior to evacuation was recorded in 34 (57% of the 60 stationary cases). For the cases reporting a time for the on-scene delay, 27 (79% of the 34) were mobile again within 20 min (Table 4). Evacuation times for this group (stationary when found and the evacuation was delayed) were reliably available in 48 of the 60 cases (80%). The time ranged from 15–300 min, with a median time of 60 min.
Time of delay before walking stationary patients.
There were no adverse medical events recorded during any evacuation. In 103 (95%) of the cases, evacuation was completed on foot. There were 5 (5%) cases in which there was a change in the evacuation method. In 4 (4%) of these cases, the rescue team met a rescue vehicle on a track, and the patient finished their journey in this vehicle. One patient was transferred to a helicopter. No change was made because of a deterioration in the patient's clinical condition. After evacuation, 66 (61%) people were discharged home without any further treatment, 3 (3%) people were discharged into the care of the police, and 7 (6%) went to the hospital; in 32 (30%) cases, there was no destination discharge information available. In the hospitalized group, there were concerns about 1 over-ingestion of drugs and alcohol, 3 had minor injuries, and 3 had no information available. No adverse medical events were reported during the evacuation, and all patients survived the evacuation.
Discussion
All 108 patients were in environmental conditions likely to cause hypothermia and had clinical features supporting this diagnosis. One patient had their temperature measured to confirm the diagnosis, but because an oral thermometer was used, the accuracy is doubtful. This case series probably contains patients with different core temperatures. Rescuers followed the recommendation that if there is doubt about the temperature in such patients, they should be assumed to be hypothermic and managed accordingly. 8 The majority were healthy people. Only 9 (9%) had comorbidities, and none had conditions causing secondary hypothermia, so all of these were cases of primary accidental hypothermia. 11 The majority were walkers who became lost or exhausted. They grew cold slowly and would have had depleted energy stores. This contrasts with the laboratory research concerning afterdrop that prompted this study and that investigated the effects of rewarming mildly hypothermic, well-nourished, not exhausted subjects who were cooled quickly in cold water.
The rescue teams reported that most victims—98 (91%)—were stationary when they arrived. Of these, 38 (39%) patients were walked off immediately. These stationary cases are considered by some experts to be at greater risk of rescue collapse because their muscles are likely to have cooled. 12 Nevertheless, they were mobilized immediately, and none in our series had any adverse outcome. There were 60 (61%) who were stationary when found and had a delayed evacuation. Most of these—44 (73%)—were given fuel and clothing without a deliberate attempt to rewarm. For the cases where the time of on-scene delay was reported, the majority, 27 (79%), were mobilized within 20 min. They exercised for a median time of 60 min without adverse outcomes. This exceeds the 45 min by which normothermia was restored in the laboratory experiment that prompted the Wilderness Medical Society guidance. 8 The initial evacuation decision for all patients was to be walked to safety from the mountain. Although there was a change of evacuation in 5 cases, none of these were due to medical reasons. Despite concerns that early increased activity might precipitate a deterioration in the patient's condition, no such cases occurred. These findings contrast with the WMS guidance that suggests that there is a significant risk that immediate activity might precipitate a deterioration in the patient's physical condition. One explanation for this finding could be that the afterdrop observed in the previous study was caused by all subjects being virtually motionless during the experiment. 13 In that situation, the muscles would cool so that when exercise commenced, blood was passing through cold leg muscles and would, therefore, be cooled before returning to the heart, causing the afterdrop. By contrast, mountain rescue patients have been exercising. This means that residual heat will be present deep in the muscles, particularly if the legs are dry. This is supported by postexercise studies that have found that deep muscle temperature and perfusion only fall slowly after exercise unless a deliberate effort is made to cool the muscles.14–18 Another explanation is that the core temperature of people with mild hypothermia who are alert and well enough to walk would not be low enough so that a 1–1.5 °C fall would bring the body temperature into the range of cardiac instability. The critical temperature for cardiac instability is 28 °C, and the temperature range for Swiss Stage 1 hypothermia is 35 to 32 °C.2,19 Therefore, even those patients with a temperature at the lower end of Stage 1 would not be expected to be at risk of cardiac instability, even with an afterdrop of 1 °C. Finally, these observations are in keeping with the Revised Swiss Scoring system that suggests that fully alert hypothermic patients have a low risk of cardiac arrest.5,6
Limitations
We used a case series, which is a qualitative method that provides insight into practice in a specific setting. 20 The findings cannot be generalized to all situations. 21 MR databases can suffer from inaccuracy; therefore, we used a purposely designed questionnaire and asked teams to use several contemporary sources in order to obtain data that was as accurate as possible. Although there are a total of 75 MR teams in England, Scotland, and Wales, reports were only submitted by 20 teams. The location of participating teams and the nature of UK terrain and weather means it is likely that these cases are representative of the mildly hypothermic patients seen each year in the United Kingdom. All decisions were made by trained rescuers using the same method of assessment and management. These results may not apply to other groups of rescuers or laypersons providing first aid using different assessment systems. The study excluded children and cold-water immersion, and results should not be transferred to these groups. The Revised Swiss Staging system introduced an additional category on the AVPU scale described as “alert and having no confusion.” This category had not appeared in the literature before the publication of the Revised Swiss Staging in 2021. 5 Our study spans this period, and we have included all cases reported as “Alert.” Some of those (64 cases) prior to January 2022 could have had confusion. If so, they would be expected to be at higher risk of adverse events. 6 However, no adverse events were reported, and we, therefore, did not perform a subgroup analysis according to the date of the incident to see if those who ran into trouble were confused. There was no measurement of core temperature, and only clinical indicators of hypothermia were used. We were unable to measure afterdrop for the same reason. However, the aim of this study is to provide insight into the situation in which rescuers must work in the field, and at present, there is no reliable method of measuring core body temperature noninvasively.
Conclusions
This case series confirms that rescue team members in England, Wales, and Scotland regularly mobilize cold, potentially hypothermic casualties and walk them off the mountains. There were no reports of cardiovascular problems, suggesting that, in our case series, there appears to be minimal risk of immediate ambulation without a delay to rewarm.
Footnotes
Acknowledgments
We gratefully acknowledge the assistance of the participating Mountain Rescue Teams in this study.
Author Contribution(s)
Disclosure
MG and LG are members of MREW, and ND is a member of SMR.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.