
Abstract
The Himalayan Rescue Association (HRA) has operated high altitude clinics in Nepal for 50 years, with rising visitor numbers, especially from India, China, and Nepal. New roads have eased access and increased the speed of ascent in some areas. Our aim was to provide a description of the activities, clinical problems, and lecture attendees of the HRA aid post in Manang over one season. We also highlight the evolving challenges of providing healthcare and education in the high Himalayan region. We describe the clinical and educational activities of the HRA aid post in Manang from September 24 to December 1, 2023. Prospective clinical data collection included anonymized patient demographics and diagnoses. Lecture data were taken from the attendee register and by daily manual counts of lecture attendees. We saw 376 patients, 62% of whom were Nepalis. Infectious diseases (42%) and altitude illness (16%) were the most common problems. A total of 846 people from 47 countries attended the daily altitude lectures. Only 5% of attendees were Nepali. Electrical supply interruptions and limitations in medical evacuation options were among the challenges of providing care at a high altitude clinic and preventing altitude illness using educational lectures. Altitude illness remains a common and potentially life-threatening problem, with risks increased by rapid ascent enabled by new road access and by ignorance of risks of altitude among travelers, especially Nepalis. Language barriers in educational outreach call for novel approaches and interventions that will ensure the effectiveness of altitude education.
Introduction
The Himalayan Rescue Association (HRA) is a nonprofit organization established in Nepal in 1973 with the objective of reducing casualties in the Nepal Himalaya and in particular preventing and treating altitude illness. The HRA has operated aid posts that are open twice yearly during spring and fall, staffed by volunteer doctors. The aid posts deliver 24-h clinical care to trekkers and local Nepali people and also provide education about altitude illness.
The first HRA aid post opened in 1973 in Pheriche, a village in the Khumbu (Everest) region at an altitude of 4250 m. The second aid post opened in 1981 in Manang in the Annapurna region at an altitude of 3550 m. Since 2003, the HRA has also operated temporary aid posts at Everest Base Camp (“Everest ER”) for the spring climbing seasons. The Association also has run an annual temporary clinic at Gosaikunda (4380 m), visited by thousands of pilgrims during the Janaipurnima Festival every year.
Tourism in Nepal has changed substantially since the HRA was founded in 1973, when 68,047 people visited Nepal. In 2019, the last year before the disruption caused by COVID-19 from 2020 to 2022, nearly 1.2 million people visited Nepal. Visitors from India (21%) and China (14%) were the most numerous, followed by the United States (8%) and the United Kingdom (5%). Of the 1.2 million visitors in 2019, 172,000 (14%) came for trekking or mountaineering. 1 Data obtained from the Annapurna Conservation Area office reveal that in 2023 the region welcomed a record number of 191,558 tourists from 173 countries, with half of them hailing from India alone. Following India, the largest groups of tourists came from France, Germany, the United States, and the United Kingdom, each accounting for ∼4% of the total, with China contributing 3%.
The numbers and nationalities of those visiting the HRA aid posts now are very different from when the posts were founded. During the 1970s and 1980s, trekking and climbing were largely a pursuit of Westerners. Now trekkers and climbers come from countries across the world. In addition, Nepali tourism to high altitude destinations also has increased for religious reasons, such as pilgrimages to Gosaikunda and Muktinath, or by the draw of obtaining compelling social media images, as with Tilicho Lake in the Annapurna region.
The purpose of this report was to describe the activities, clinical problems, and lecture attendees of the HRA aid post in Manang over one season. We also aimed to highlight the evolving challenges of providing care at a high altitude clinic and preventing altitude illness using educational lectures.
Background and Setting
Manang village is situated in the northern part of the Manang district, one of the most sparsely populated districts of Nepal, with a total population of 5658 spread unevenly over an area of 2246 sq km.2,3 Manang (3550 m) is on the Annapurna circuit on the way to Thorong Pass (5416 m). Most trekkers rest for a day in Manang to acclimatize to high altitude. The HRA aid post is strategically situated to serve porters, trekkers, and local Nepalis.
In the past, reaching Manang from Besisahar required a week-long trek. The construction of a new road suitable for 4-wheel-drive vehicles began in 2010 and was completed in 2014. Many trekkers now skip portions of this historic route, with some taking a 7-h drive from Besisahar to directly reach Manang or Khangsar (3750 m).
In the fall of 2023, the Manang aid post was staffed with four volunteer doctors: one Nepali medical officer, two UK doctors (one intensive care specialist with additional skills in musculoskeletal medicine and one infectious disease specialist), and one Australian rural general practitioner. The normal clinic hours were 0900 to 1700 every day, with emergencies seen at any time. Consultations during regular hours were set at US $45, off-hour consultations cost US $80, and follow-up visits cost US $20. Additional charges are applied for medical tests, medications, and inpatient services. All Nepali patients were charged a nominal fee of NPR 50 (equivalent to US $0.38), covering the entirety of their medical services.
The free daily lectures on the prevention and treatment of altitude-related illnesses were advertised by distributing flyers around the town. Some trekkers were also brought to the lectures by their guides. The doctors took turns giving the lectures. The talks were given in English at 1500 in the clinic lecture hall.
The logistics and overall operations of the clinic were managed by a permanent HRA staff member. The team also included an experienced expedition cook who kept the clinic clean and the staff well fed.
The clinic and living quarters are in the same complex. The clinic consists of one outpatient consultation room, an overnight 2-bed room with a heater and 2 oxygen concentrators, a storeroom, a pharmacy, and an office. Each of the rooms in the living quarters has a double bed and attached bathroom.
The main power supply comes from a nearby small hydroelectricity power plant. The clinic also has a small solar system with battery backup for emergencies. The diagnostic and treatment facilities are limited. Apart from instruments and devices to measure vital signs, including a Nonin 8500 pulse oximeter, the clinic has a Schiller CARDIOVIT AT-102 Plus electrocardiograph, a Butterfly iQ Portable Ultrasound, urine dipstick kits, a blood glucose monitor, and urine pregnancy kits. A wide range of emergency equipment and drugs is available. The closest radiographic and pathology service is at Manang District Hospital in Chame, a 2-h ride (∼30 km) in a 4-wheel-drive vehicle. For tourists with travel insurance and for people who can afford the cost (∼US $2500), helicopter evacuation to a larger city (Kathmandu or Pokhara) is an option, although only in daylight and in good weather conditions.
Data Collection and Analysis
As part of routine clinic procedure, we collected data prospectively on a predesigned paper form from all the patients who visited the clinic. Anonymized data with the diagnoses and nationalities were then transferred to an electronic database that formed the basis for our analysis. Diagnoses were cross-verified by a second volunteer doctor. Established guidelines were used for the diagnosis of illnesses, especially acute mountain sickness (AMS), high altitude pulmonary edema (HAPE) and high altitude cerebral edema (HACE).4,5 When a patient had multiple diagnoses, we recorded them all in our database. For this reason, the number of diagnoses exceeded the total number of patients. We excluded follow-up visits from the analysis.
We obtained data on lecture attendance from the attendee register. The attendees wrote their names and nationalities in a book as they arrived. To ensure an accurate total count, including those who did not register, we supplemented the recorded names with an additional count conducted by HRA staff or volunteer doctors during the lectures.
Permission to report the clinic's activities was obtained from the HRA Board of Directors.
Clinical Activity
The clinic opened on September 24 and closed on November 30, 2023. During that period, we saw 376 individual patients, of whom 233 (62%) were Nepali. The rest were international trekkers from 35 different countries (Figure 1). The majority of patients (207; 55%) were 20 to 39 years of age, ∼10% were 0 to 19 years of age, and 10% were >60 years of age.
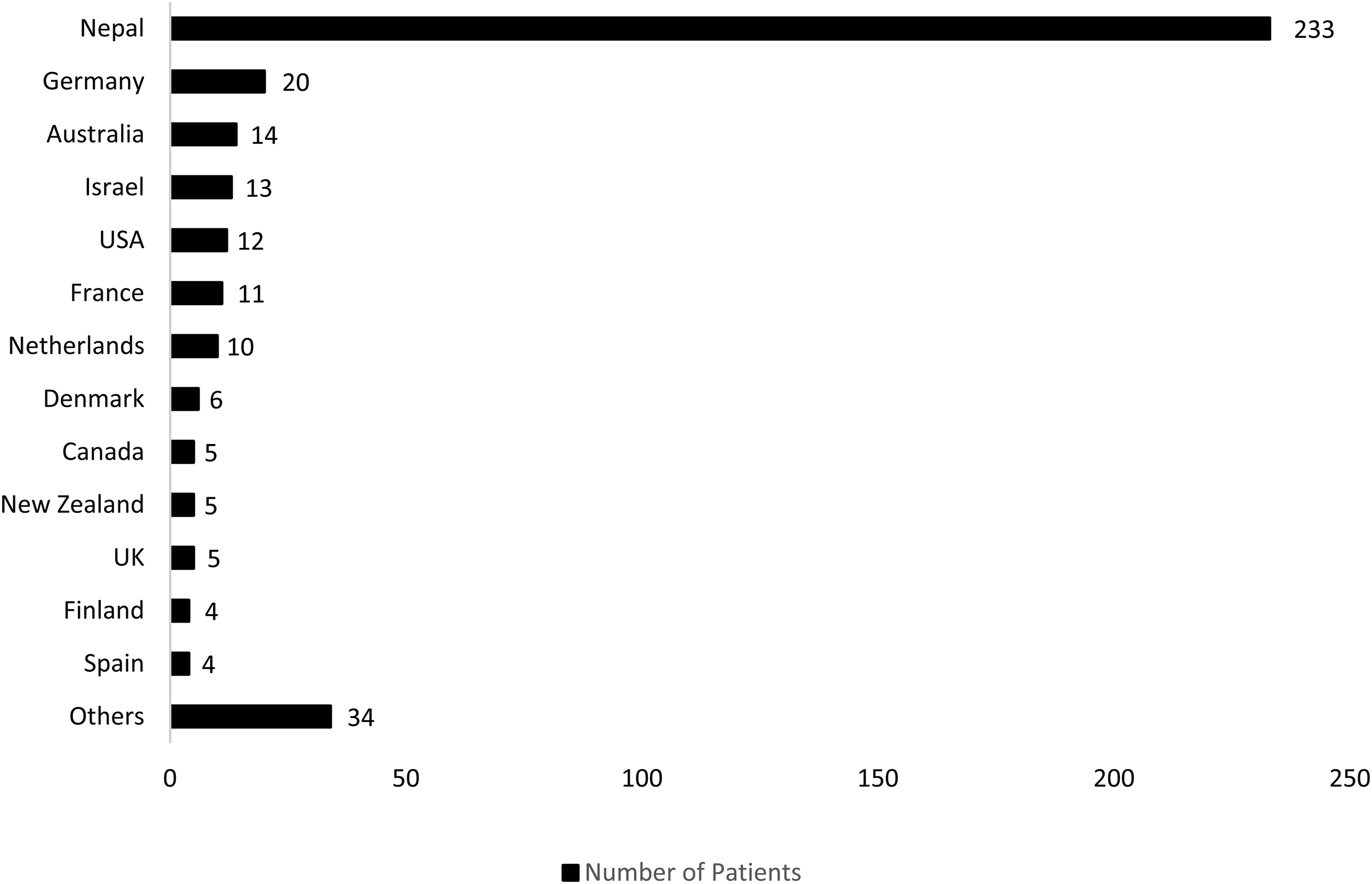
Distribution of patients seen in the clinic by nationality.
The most common diagnoses were infectious diseases (42%), with upper respiratory infections responsible for 101 (60%) of the infectious disease consultations (Table 1). Gastrointestinal infection was the next most common category, with 26 consultations (16%), of which 16 (62%) were international trekkers with traveler's diarrhea. Other less common infectious diseases were skin and soft-tissue abscesses, dengue (acquired in Kathmandu), and severe cases of scabies. Musculoskeletal problems also were common, mostly related to trekking. These comprised 10% of the caseload.
Distribution of diseases by diagnostic category and the categories of infectious disease diagnoses.
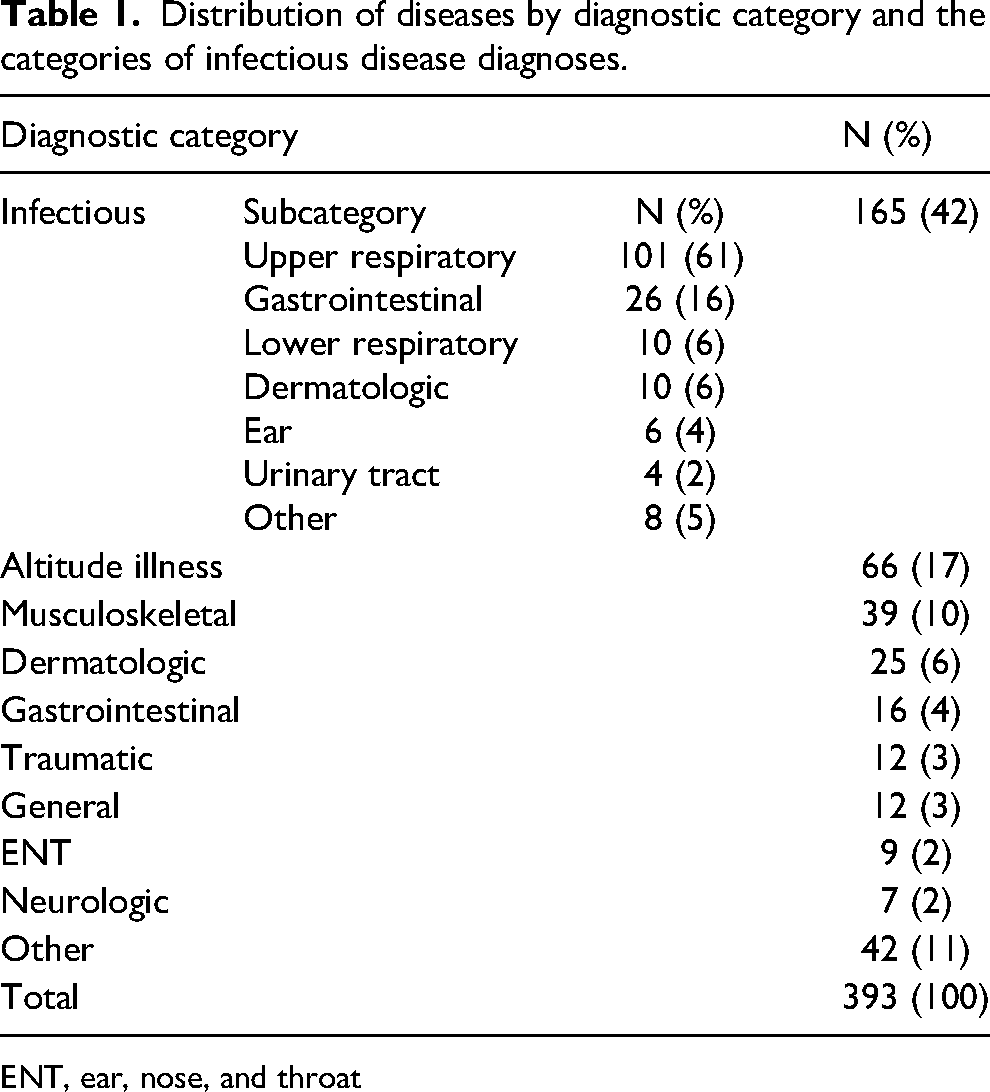
ENT, ear, nose, and throat
Altitude illness was the second most common reason for consultation, occurring in 64 patients (16%). Of these patients, we diagnosed 57 (90%) with AMS, 5 with HAPE, 1 with AMS and HAPE, and 1 with HAPE and HACE. We also saw 4 patients with high altitude cough and 1 patient with ventricular bigeminy, presumably related to altitude. We did not see any patient with HACE alone.
During the Nepali festival season, from October 15 to November 16, many Nepali visitors traveled from low altitude directly to Khangsar (3750 m), a village ∼5 km beyond Manang, using 4-wheel-drive vehicles or motorcycles. Many of them then ascended rapidly to Tilicho Lake (4919 m), putting themselves at high risk for altitude illness. Although we observed increased numbers of patients with altitude illness during the festival period, most of them were international trekkers (Figure 2).
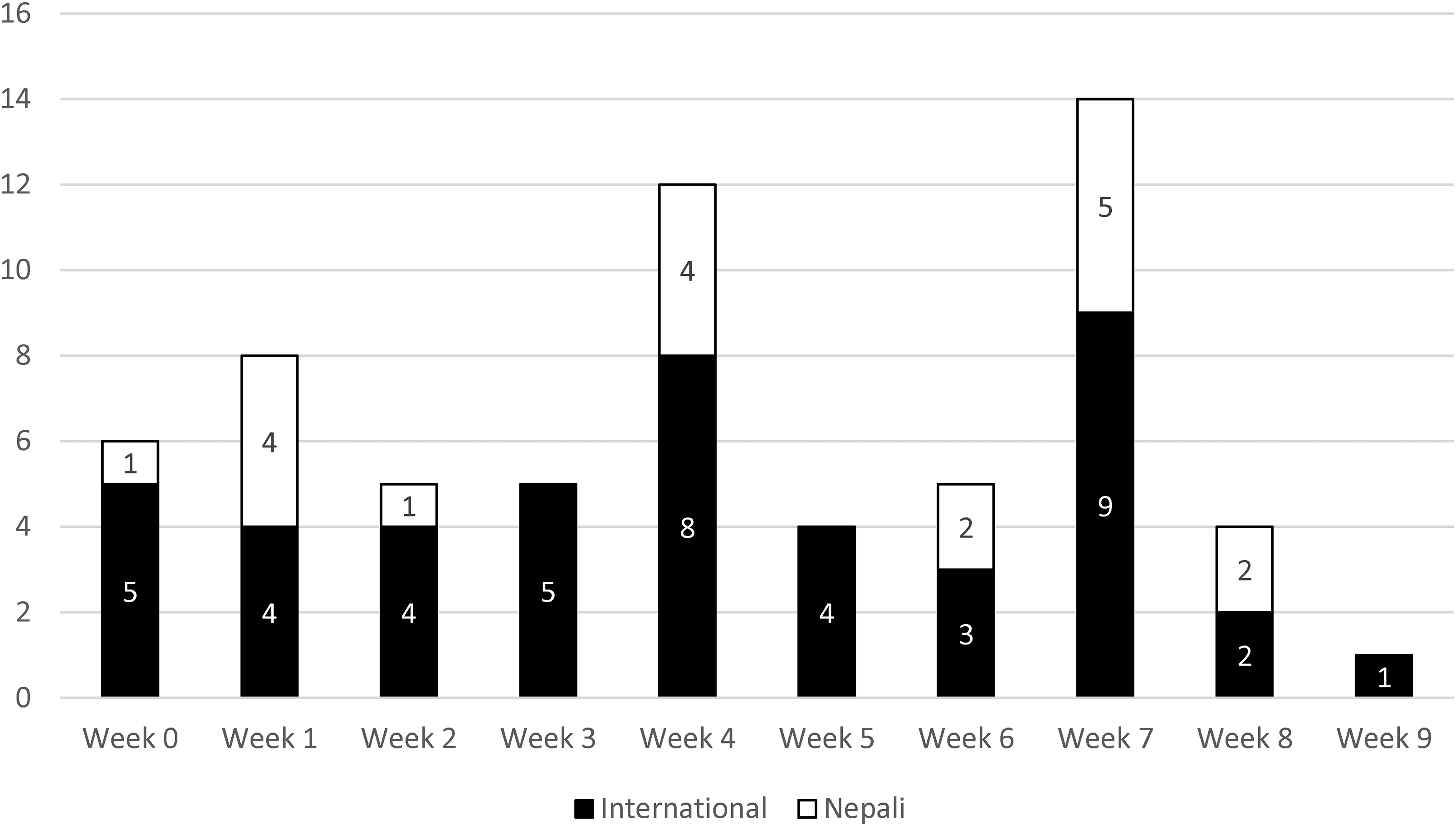
Distribution of patients with altitude illness by week. Week 0 started on September 4, 2023, and Week 9 terminated on November 30, 2023. The Nepali festival season spanned from Week 3 to Week 7, during which we had expected the cases of altitude illness to rise among Nepalis. However, the two spikes in Weeks 4 and 7 were mostly attributable to international patients.
The majority of the emergency presentations and overnight stays were altitude related. Other emergency presentations included acute appendicitis in a local Nepali requiring a 12-h evacuation by road to Kathmandu, a child who fell face first from a 3-m-high roof, a patient with acute anaphylaxis, and several cases of trauma related to motor vehicle crashes.
Educational Lectures
A total of 846 people from 47 countries attended the altitude lectures during the season (Figure 3A). Of 846 total attendees, 677 filled the attendee register providing their nationalities. Figure 3B presents the breakdown of nationalities. Only 5% of attendees were from Nepal. Many of these were guides accompanying groups of international trekkers.
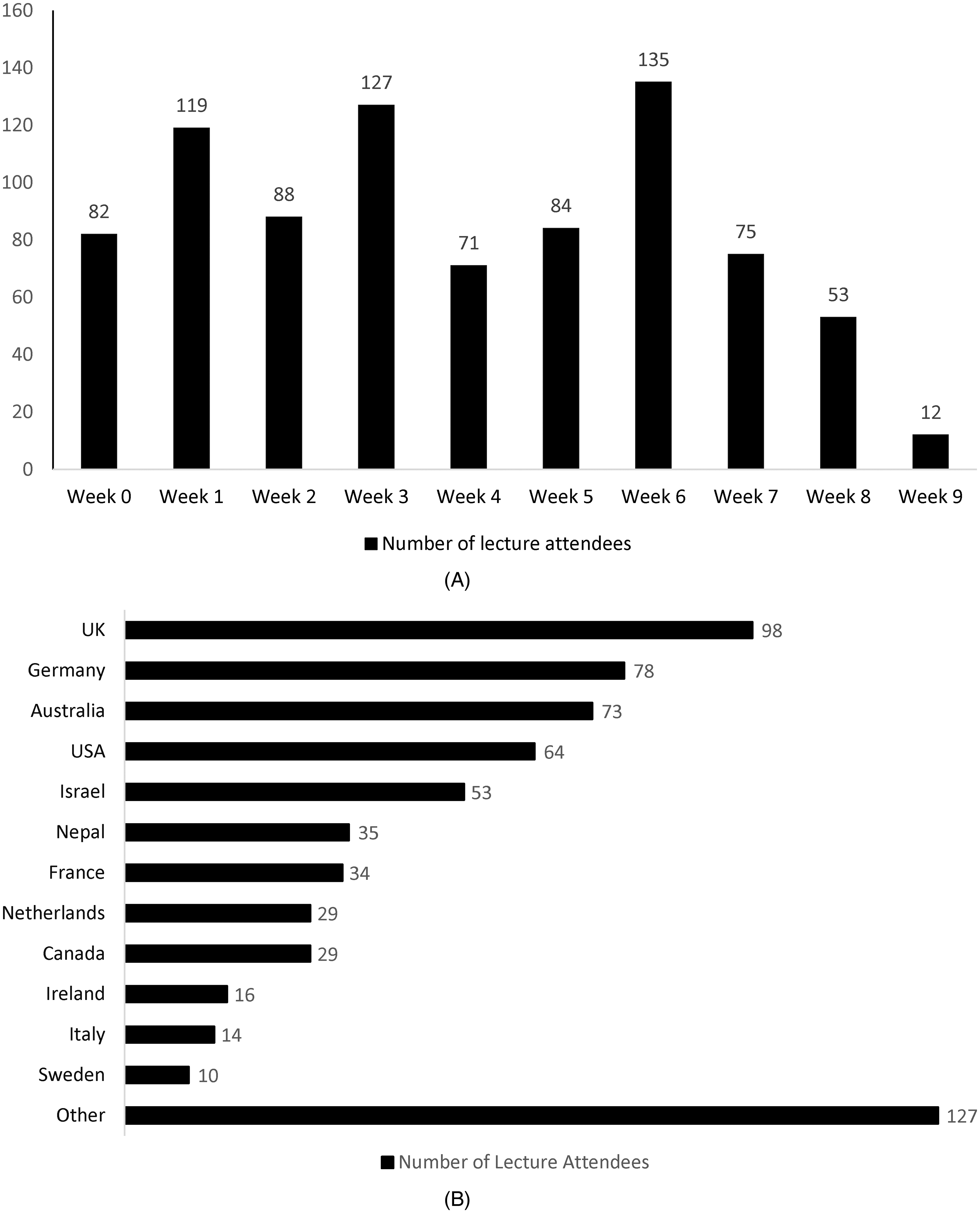
Lecture attendance by week (A) and nationality of attendees (B).
Challenges
Intermittent electricity was a significant issue, especially when the hydroelectric power supply took 4 wk to be repaired. Fortunately, the clinic solar system kept most of the vital services running. One morning the clinic electricity was exhausted by overnight use of the oxygen concentrator to treat a patient with HAPE.
Urgent evacuation was challenging because helicopters were unable to fly at night or in adverse weather. Most Napali and many foreign trekkers had no helicopter insurance. Getting a helicopter was expensive and required upfront payment. The road to Manang was another option, but only for high-clearance vehicles. Travel took 7 h to the nearest paved road and 12 h to a hospital in Kathmandu (260 km).
Implications
The HRA has been operating aid posts in the high Nepal Himalaya for 50 years. Much has changed over that time with respect to visitor numbers, nationalities, and access to the mountains. There are many more people from China and India traveling to Nepal. New roads, such as the one to Manang, make the passage to high altitude far easier and faster than just a few years ago. As a result, the clinical and educational challenges also have increased. Because there are little published data concerning the daily workload of clinics such as the one in Manang, our objective was to describe the clinical workload and the numbers and nationalities of those attending the lectures to help anticipate future needs and challenges.
A report from 1999 found that from 1983 to 1985, ∼6% of all patients who visited the Manang aid post were diagnosed with AMS and 0.3% were diagnosed with HAPE and/or HACE. 6 Comparing our findings with that report, we observed higher percentages of patients diagnosed with altitude illness: 15% of patients were diagnosed with AMS, 2% with HAPE, and 0.3% with HACE. This increase in altitude illness may have been caused by the completion of a new road to Manang in 2014, facilitating faster and easier passage to high altitude. A study conducted in 2016 to assess the impact of the newly constructed road to Manang on altitude illness also concluded that the newly constructed road significantly contributed to an increase in altitude illness, especially affecting a substantial number of Nepalis who undertook rapid ascents. 7
During the 2023 Nepali festival season, a considerable number of Nepalis drove directly to Khangsar (3750 m). However, there was no marked increase in Nepali patients with altitude illness at the clinic. One explanation could be that most Nepalis bypassed Manang to reach Khangsar directly and remained unaware of the HRA clinic in Manang. Many of them may have sought medical attention at health posts in Khangsar or Tilicho Base Camp.
Religious pilgrims in the Himalayas vastly outnumber trekkers and climbers. 8 Rapid ascent to Muktinath (3800 m) in the Annapurna area has become easier because of new roads. Even without roads, many pilgrims ascend rapidly on foot to reach Gosaikunda (4380 m). This quick climb is dangerous, as reported by several studies, which show that a substantial proportion of these pilgrims ranging from 34 to 68%, experience AMS.9,10
The accessibility of roads and the changing demographics of visitors are changing the nature of medicine in the high altitude Himalayan districts of Nepal. Infectious diseases, even those with short incubation periods, contracted in the lowlands, can become symptomatic at high altitude. We saw a patient who we suspect had acquired dengue in Kathmandu and who subsequently traveled to Manang by vehicle. We also saw 2 victims of motor vehicle crashes who required evacuation.
The daily altitude lectures at HRA, an important means of imparting altitude education to trekkers, are delivered in English. A growing number of trekkers with limited understanding of English cannot benefit from the lectures. To bridge this gap, we should explore the possibility of having the daily lectures in English and Nepali and having altitude illness leaflets in most of the popular languages. The Strengthening Altitude Knowledge consensus statement that describes 28 learning objectives laypersons should know before traveling to altitude could be used as a guiding tool for this purpose. 11 Additionally, leveraging social media campaigns and high-quality content can be instrumental in disseminating information and raising awareness about altitude. These digital strategies can complement traditional educational methods, ensuring wider reach and engagement, particularly among trekkers who may not attend the lectures.
Conclusion
Altitude illness is a common problem at the HRA aid post in Manang, second only to infectious diseases. Rapid ascent by road has increased altitude illnesses in trekkers and tourists and posed other challenges, including vehicular trauma. Our study underscores the necessity for tailored educational interventions, particularly targeting Nepali trekkers and others with limited understanding of English, to mitigate altitude-related risks. As Himalayan tourism evolves, adapting educational strategies and addressing the associated healthcare challenges are increasingly imperative for organizations such as the HRA.
For more detail on the HRA and volunteering, visit https://www.himalayanrescue.org/potential-volunteers.
Footnotes
Acknowledgments
The authors thank Wangchhe Sherpa for his excellent cooking and care for the clinic. We also thank Ken Zafren for his support during the season and his guidance concerning the development of this paper. We also thank the community of Manang for their support and friendship.
Author Contribution(s)
Study concept and design (all authors), data acquisition (all authors), data analysis (ST, GEH, CLT, GET), drafting and critical revision of the manuscript (all authors), and approval of final manuscript (all authors).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. GET and CLT are supported by the Wellcome Trust, UK.