
Abstract
Objective
This study investigated the impact that motor vehicle travel along a newly constructed road has on altitude illness (including acute mountain sickness, high-altitude cerebral edema, and high-altitude pulmonary edema). The new road from Besisahar (760 m) to Manang (3540 m) in Nepal was completed in December 2014.
Methods
We enrolled all patients diagnosed with altitude illness at the Himalayan Rescue Association Manang clinic in fall 2016. Phi coefficients were calculated to test for an association between Nepali ethnicity and rapid ascent by motor vehicle. A retrospective review looked at all patients with altitude illness from fall (September-November) 2010 to spring (February-May) 2016.
Results
In fall 2016, more than half (54%) of patients with altitude illness traveled to Manang by motor vehicle, and one-third (33%) reached Manang from low altitude (Besisahar) in less than 48 hours. Nepali nationality had a significant association with motor vehicle travel (phi +0.69, P < .0001) as well as with rapid ascent to Manang (phi +0.72, P < .0001). Compared to previous seasons, fall 2016 saw the most patients diagnosed with altitude illness. The proportion of people with altitude illness who traveled by vehicle and reached Manang in less than 48 hours was significantly greater than the proportion prior to completion of the road (P < .0001 for both).
Conclusions
Rapid ascent by the newly constructed road from Besisahar to Manang appears to be related to a significant increase in the number of patients with all forms of altitude illness, especially among Nepalis. The authors believe that educational interventions emphasizing prevention are urgently needed.
Introduction
Altitude illness, including acute mountain sickness (AMS) and the life-threatening forms of high-altitude cerebral edema (HACE) and high-altitude pulmonary edema (HAPE), is a well-known occurrence among people traveling to elevations above 2500 m. Rapid ascent from low altitude is a known risk factor. 1 –5 Gradual ascent allows time for acclimatization and is a cornerstone of prevention of altitude illness. In December 2014, a new road was completed to Manang, Nepal (3540 m), along the Annapurna circuit, Nepal’s most popular trekking route. The road provides cheaper and faster travel to Manang for locals and tourists alike; however, traveling to Manang by motor vehicle usually entails rapid ascent from low elevations. Current guidelines recommend travelers spend 2 or more nights at elevations of 2500 to 3000 m before ascending further.1,2 Those traveling by jeep along the new road typically reach Manang (3540 m) in 1 or 2 days (ie, 1 night or less), putting them at high risk of developing altitude illness. 2
There are few data in the medical literature on the relationship between construction of new roads and altitude illness in Nepal. With massive road-building projects currently underway along the mountainous Chinese-Nepali border, the risks of rapid travel to altitude may increase in the future. This study explores a connection between the completion of Manang’s new road and cases of altitude illness diagnosed and treated at the Himalaya Rescue Association (HRA) Manang clinic.
The Region
Nepal’s Annapurna Conservation Area is the country’s largest protected area. Over 100,000 residents of various cultural and linguistic groups live within its boundaries. 6 Over 60% of trekkers in Nepal are drawn to this mountainous region to trek along the Annapurna Circuit, which circles the Annapurna massif. 6 The route passes through Manang, which in the past was typically reached by foot from low elevation (Besisahar, 760 m) over 4 or more days. Trekkers pass through Manang on the way to the highest point of the circuit, Thorong La (Thorong Pass, 5416 m), as well as to Tilicho Lake (5000 m).
Since 1981, the HRA has staffed a clinic in Manang during fall (September-November) and spring (February-May) with physicians trained in managing altitude illness. Altitude illness is common along the Annapurna circuit, both among the foreign tourists who have traditionally comprised the majority of the trekking population, as well as among Nepali trekkers, porters, guides, pilgrims, and locals. During most spring seasons, the clinic also sees altitude illness among Nepalis traveling from lower elevations to the Manang district to gather yarsagumba (Ophiocordyceps sinensis), a parasitic fungus used in traditional Chinese medicine.
The road from Besisahar to Manang was completed in December 2014 and quickly became a popular means of traveling to Manang by motor vehicle. In the few years prior to completion of the road, jeep or motorcycle travel was possible along certain portions of the route.
Patients and Methods
Study Design
With approval from the Nepal Health Research Council, reference number 1093, all patients seen in the HRA Manang clinic in fall 2016 who were diagnosed with AMS, HACE, and/or HAPE7,8 were automatically enrolled in the study. Diagnosis of AMS was based on the Lake Louise Score. 9 We collected demographic and diagnostic information, including detailed information on ascent profile, number of travel days from Besisahar to Manang, and means of travel. Additionally, we surveyed patients with altitude illness who traveled to Manang by motorized vehicle to assess preexisting knowledge regarding the risks of rapid ascent.
For the years 2010 to spring 2016, we conducted a retrospective review of HRA’s database and analyzed all clinic notes from the HRA Manang clinic. Information on demographics and ascent profiles was collected for all patients diagnosed with altitude illness during this time period.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics version 22 (IBM, Armonk, NY) statistical software. We used χ2 tests to look for an association between Nepali nationality and both a history of motor vehicle travel to Manang and having reached Manang from low altitude in less than 48 hours. Phi coefficients were used to measure the strength of association, with values of +1 denoting perfect agreement, –1 denoting perfect disagreement, and 0 denoting no association. To compare values from fall 2016 to the mean values from 2010 through 2014 (seasons prior to completion of the road) one-sample permutation tests were used to assess increases in the proportion of total clinic patients with altitude illness and in the proportion of patients with altitude illness who were diagnosed with AMS, HACE, and/or HAPE; who traveled by vehicle; who reached Manang in less than 48 hours; and who were Nepali. To control for family-wise error rates with multiple hypothesis tests, we used the Holm-Bonferroni Method to obtain corrected alpha levels. Only Holm-Bonferroni corrected values are reported.
Results
During fall 2016, 453 patients were evaluated at the HRA Manang clinic, of whom 91 (20%) were diagnosed with altitude illness. The demographic and diagnostic breakdown of the study population is shown in Table 1. Of these 91 patients with altitude illness, more than half (n = 49, 54%) traveled by motorized vehicle for at least part of their journey from low altitude to Manang. One-third (n = 30, 33%) reached Manang from Besisahar in less than 48 hours. Of those traveling by vehicle, 48 patients were diagnosed with AMS (58% of all patients with AMS), 2 patients were diagnosed with HACE (25% of all patients with HACE), and 5 patients were diagnosed with HAPE (100% of all patients with HAPE). Seven patients (8%) initially trekked to Manang on foot but then took a vehicle the rest of the way once they began to feel ill because of altitude symptoms, entailing further altitude gain.
Demographic and diagnostic characteristics of 91 patients diagnosed with altitude sickness in Manang, Nepal in fall 2016
AMS, acute mountain sickness; HACE, high-altitude cerebral edema, HAPE, high-altitude pulmonary edema.
Total percent does not equal 100 because several patients with HAPE were concurrently diagnosed with either AMS or HACE.
A total of 39 Nepali patients were diagnosed with altitude illness, comprising 43% of all altitude patients. Nepali patients comprised 27 trekkers, 4 guides/porters, and 8 locals/migrant workers (Table 1). Among Nepali patients with altitude illness, all but 3 (n = 36) traveled to Manang by motorized vehicle (92%), and 28 reached Manang from low altitude in less than 48 hours (72%). In comparison, among 52 non-Nepali patients, 12 traveled by motorized vehicle (23%), and only 2 patients reached Manang in less than 48 hours (4%). Nepali nationality was significantly associated with having traveled by motor vehicle (phi +0.69, P < .0001) and with having reached Manang from low altitude in less than 48 hours (phi +0.72, P < .0001). The 37 Nepali patients traveling by vehicle accounted for 76% of all altitude patients traveling by vehicle, including 1 of 8 patients (13%) with HACE and 4 of 5 patients (80%) with HAPE.
We surveyed 37 patients with altitude illness who had traveled to Manang by vehicle. Prior knowledge was assessed by asking if they knew that rapid ascent to altitude could be dangerous. Twenty were aware of the danger (54%), and 17 were unaware (46%). Those claiming to have had prior knowledge of the risks were questioned further, and the following reasons for traveling by vehicle were given: time limitations necessitated rapid travel to Manang; patients believed that previous time spent at altitude was protective; and some believed that being of Nepali nationality, specifically being from the Gurung or Manangi peoples who traditionally live at high altitude, was protective.
For the years 2010 to 2016, data were available for 11 out of 14 trekking seasons (Table 2). During this time period, the highest number of patients with altitude illness who had traveled to Manang by vehicle and reached high altitude in less than 48 hours was seen in fall 2016. The highest proportion of all clinic patients with altitude illness (20%) also occurred in fall 2016, significantly higher than the mean prior to completion of the road (P = .0125). The proportion with altitude sickness who traveled by vehicle and the proportion who reached Manang in less than 48 hours were both significantly higher (P = 0.0083 and 0.01, respectively). The number of patients with more severe forms of altitude illness (ie, HACE and/or HAPE) was second highest in fall 2016; however, the proportion of patients with these severe forms of altitude illness did not reach statistical significance when compared to seasons prior to completion of the road (P = .2418).
Demographic and diagnostic characteristics of patients evaluated in Manang, Nepal between 2010 and 2016
Some patients with HAPE were concurrently diagnosed with either AMS or HACE.
Over the time period analyzed, Nepalis made up the second highest proportion of all patients with altitude illness in fall 2016 (43%). This value failed to reach statistical significance when compared to seasons prior to completion of the road (P = .0166). The proportion of Nepali patients in fall 2016 was second only to that in spring 2014 (56%), during which the clinic saw a surge of Nepali yarsagumba gatherers with altitude illness. Among Nepali patients, the number of Nepali trekkers in particular was highest in fall 2016, as was their proportion among all altitude patients. As shown in the Figure, since completion of the road in 2014, there have been increases in the number of Nepali trekkers, the number of people traveling by motorized vehicle, and the number of people reaching Manang from low altitude in less than 48 hours. This trend was particularly pronounced in 2015 and 2016 after completion of the road.
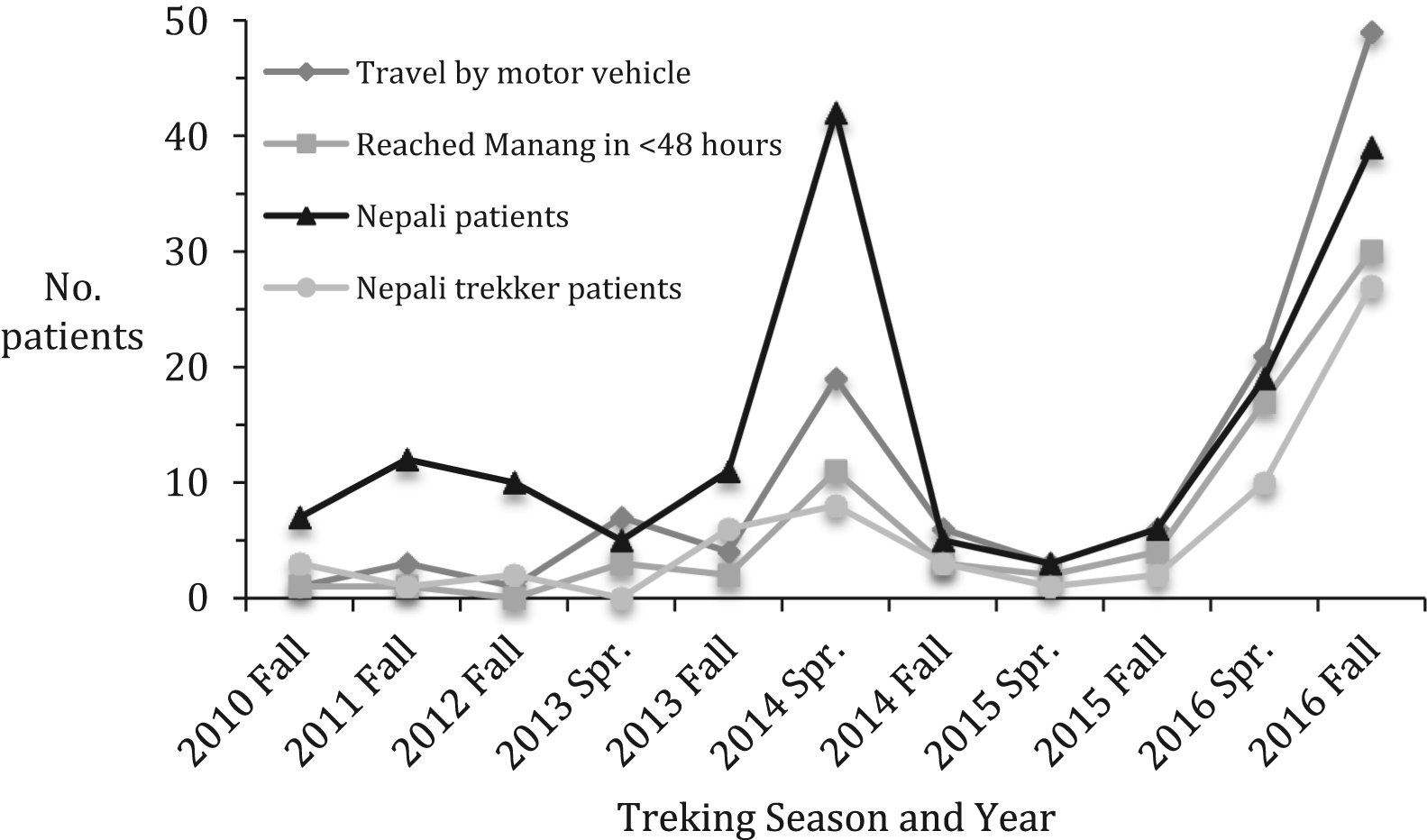
Trends in demographics and travel characteristics among patients diagnosed with altitude sickness (acute mountain sickness, high-altitude cerebral edema, and high-altitude pulmonary edema) in Manang, Nepal from 2010 to 2016.
Discussion
This analysis of patients with altitude illness seen in the HRA Manang clinic from 2010 to 2016 explored the potential impact of new road construction on altitude illness. Since completion of the road to Manang in December 2014, the number of patients with altitude illness has increased in tandem with the number of patients traveling by motorized vehicle and reaching Manang via rapid ascent, especially among Nepalis. It is particularly concerning that among patients with life-threatening forms of altitude illness in fall 2016, all patients with HAPE and 2 patients with HACE had traveled by vehicle. Furthermore, our survey showed a significant knowledge deficit regarding the importance of gradual ascent in preventing altitude illness. This finding is consistent with the results of a previous survey conducted among trekkers, porters, and guides in the Annapurna region, which showed that all groups lacked knowledge of altitude illness prevention and recognition. 10
In this study, travel by rapid ascent was more common among Nepali patients than among foreigners. Several other reports, including studies of Nepalis on religious pilgrimage to Gosainkunda Lake (4300 m), 11 –13 have also documented Nepalis ascending rapidly to high altitude, which suggests they are at particular risk of altitude illness. This is supported by a previous study from the Annapurna region, which found a significantly higher proportion of Nepalese staff and porters requiring evacuation compared with foreign nationals. 14 Although our study was not able to show a significant increase in the number of cases of HACE or HAPE, partly due to overall low numbers of severe altitude illness in Manang, we believe that due to the easy accessibility of travel by road, life-threatening forms of altitude illness 7 will be more readily encountered among Nepalis, who generally lack awareness of altitude illness and its prevention. 10 More altitude-related dangers may be relevant to this vulnerable population, especially if some continue on over Thorong La while ill with AMS.
Road access has complex socioeconomic implications for the Manang district. It provides cheaper and faster travel and transport of goods for the local population, as well as easier descent for medical care and more rapid evacuation of Nepalis, who can rarely afford the costs of helicopter evacuation. The road carries obvious dangers as well, and the availability of cheaper, faster travel by motor vehicle is likely related to the increasing number of Nepali patients diagnosed with altitude illness in the HRA Manang clinic. Although the precise number of Nepali trekkers traveling in the Annapurna region is not available, anecdotal accounts from hotel owners in Manang and surrounding villages suggest that since completion of the road in December 2014, there has been a dramatic increase in Nepali tourists visiting the Manang district. The numbers appeared to decrease transiently after the 2015 earthquake, which reflects the seasonal variability in Manang’s patient population. In particular, in 2016, a large number of university students from Nepal’s cities visited Manang during brief school vacations. Motor vehicle travel minimizes lodging and food costs, thereby offering a more attractive means of traveling to the Annapurna region. In 2016, travel to Manang and Mustang, a neighboring mountainous region, was common enough to become a social media phenomenon among urban Nepali young adults.
Although the road allows Nepalis to see the natural grandeur of their own country more easily, an experience that was once cost-prohibitive and mostly limited to foreigners, the dangers of the road are significant. As we found in our study, the road also offers an easy way for tired or ill trekkers to finish the journey to Manang by motor vehicle, which further increases the risk of developing serious altitude illness.2,7
Educational interventions such as press releases in popular media or more prominent and strategically placed signs posted along the road and in tea houses may help increase awareness of altitude illness prevention strategies among those traveling to Manang by motor vehicle. In light of our findings, interventions should be directed toward educating Nepali travelers and should emphasize the dangers of rapid ascent, that Nepali nationality is not protective, and that acclimatization to altitude is lost after about 2 weeks at lower elevations.
The relationship between new road construction and altitude illness is relevant given the significant road-building activity along the China-Nepal border. Wu et al documented altitude illness aboard the region’s Qinghai-Tibet railroad line, much of which is situated above 4000 m, 15 so the results of this study are not surprising. China embarked on a massive road-building project into Tibet beginning in the 1950s and is currently extending that project into Nepal. At the time of publication, construction is proceeding along 8 different roadways connecting Nepal and China across the Himalayas, with 2 roads damaged in the 2015 earthquake being upgraded and 6 new roads being built. 16
Limitations
The study population was limited only to those presenting to the HRA Manang clinic, which likely represented a small proportion of all individuals traveling to Manang and developing symptoms of altitude illness. Although patients who become ill prior to reaching Manang can now easily finish the journey by motor vehicle, this would have been more difficult prior to completion of the road, and these patients would likely not have been seen in the Manang clinic. This may account for some of the increase in patients with altitude illness seen in Manang since 2014. The study may also be limited by the timing of yarsagumba gathering, which continues after the Manang clinic closes for the spring. Anecdotal reports suggest that the number of Nepali trekkers has increased in several regions of Nepal in recent years, indicating that the road may not be solely responsible for the increased number of patients seen in Manang. Furthermore, seasonal variation in travelers to Annapurna is significant and was severely affected by natural disasters in 2014 and 2015.
Conclusions
We believe that travel by motor vehicle to Nepal’s Annapurna region, which first became possible in 2014, is contributing to an increase in altitude illness, especially among Nepalis. Educational interventions focusing on altitude illness prevention and the dangers of rapid ascent by motor vehicle may help increase awareness among travelers to Annapurna. Given accelerating road construction across the China-Nepal border, new roads may contribute significantly to increases in altitude illness in future years.
Acknowledgments: The authors thank Thaneshwar Bhandari and Indira Ojha for their support of the HRA Manang clinic.
Author Contributions: Study concept and design (JR); drafting of the manuscript (JR); acquisition of the data (DD); analysis of the data (DD); critical revisions of the manuscript (BB); and approval of final manuscript (JR, DD, BB).
Financial/Material Support: None.
Disclosures: None.