
Abstract
Since the first documented use of a tourniquet in 1674, the popularity of tourniquets has waxed and waned. During recent wars and more recently in Emergency Medical Services systems, the tourniquet has been proven to be a valuable tool in the treatment of life-threatening hemorrhage. However, tourniquet use is not without risk, and several studies have demonstrated adverse events and morbidity associated with tourniquet use in the prehospital setting, particularly when left in place for more than 2 h. Consequently, the US military's Committee on Tactical Combat Casualty Care has recommended guidelines for prehospital tourniquet conversion to reduce the risk of adverse events associated with tourniquets once the initial hemorrhage has been controlled. Emergency Medical Services systems that operate in rural, frontier, and austere environments, especially those with transport times to definitive care that routinely exceed 2 h, may consider implementing similar tourniquet conversion guidelines.
Introduction
Tourniquet application can save lives in the setting of life-threatening extremity hemorrhage. 1 Tourniquet use has been shown to be overwhelmingly safe and effective in military and civilian prehospital settings.2,3 However, there is some morbidity associated with prolonged tourniquet application.4,5 Most of the studies that show very low rates of complications from emergency tourniquet use are from large-populated urban centers and military conflict zones that actively work to decrease injury to surgery times. 6 Case reports and reviews of data from longer tourniquet applications demonstrate adverse effects. 6 To address the morbidity associated with prolonged tourniquet application, military prehospital organizations have developed rigorous guidelines including indications, contraindications, and procedural steps for tourniquet conversion to nontourniquet hemostatic dressings.5,7 The current guidance of military experts and the Committee on Tactical Combat Casualty Care recommends that “every effort should be made to convert tourniquets in less than 2 hours if bleeding can be controlled with other means. Do not remove a tourniquet that has been in place more than 6 hours unless close monitoring and lab capability are available.”8,9 Civilians working in extremely rural or wilderness environments with transport times that exceed the 2 h from the time of injury to hospital may consider implementing a procedure for tourniquet conversion into their clinical guidelines.10-13
Background
The known history of tourniquet use dates back to the Middle Ages, when Morel used a tourniquet during the Battle of Flanders in 1674.
14
Since then, the popularity of tourniquet use on the battlefield has waxed and waned, being seen as both a lifesaving tool and a limb-threatening adjunct.15,16 Over the years and the associated wars, tourniquets were gradually altered and improved. In 1941, Arnold Dwight Tuttle published the Handbook for the Medical Soldier, in which he discussed tourniquet application and established 4 rules for tourniquet use
16
:
Never cover over or bandage a tourniquet. Write plainly on the emergency medical tag the word ‘tourniquet.’ If the injured man is conscious, he should be instructed to tell every medical officer with whom he comes in contact that he has a tourniquet on. Lastly, remember, if a tourniquet is left on a wound for 6 hours the limb will surely die.
Tourniquets once again saw combat in World War II and the Korean and Vietnam wars, but their effectiveness was limited due to misapplication, misuse, and an overall negative perspective surrounding their value.
17
Tourniquets found immense popularity among fighters and medical practitioners in the conflicts in Afghanistan and Iraq/Sryia, which coincided with the development of more effective tourniquet devices. Combat medics initially designed the Combat Application Tourniquet and Special Operation Forces Tactical Tourniquet devices for use in the Middle Eastern conflicts, which were studied extensively for their viability as effective battlefield tourniquets.
18
Implementation of a Joint Theater Trauma System during the wars in Afghanistan and Iraq allowed for real-time, evidence-based process improvement. The Joint Theater Trauma System, its registry (Joint Theater Trauma Registry), and the Joint Combat Casualty Research Team in the theater soon generated evidence that confirmed not only the utility of tourniquets but also a survival benefit with their use. These data were quickly used in the development and distribution of commercially available tourniquets in 2005 and 2006.
14
In 2014, a study conducted by the American College of Surgeons Committee on Trauma built on data collected in a 2012 military review and showed survival benefits related to tourniquet use among civilians.19-21 Eventually, the American College of Surgeons Committee on Trauma developed a curriculum focused on hemorrhage control that could be taught to civilians similarly to cardiopulmonary resuscitation, preparing bystanders as emergency responders. This curriculum would go on to form the foundation for the STOP THE BLEED course.
21
Tourniquet use in Recent Military Conflicts
The conflicts in Iraq and Afghanistan saw a rise in explosive devices as the primary method of injury, leading to increased odds of death for military personnel. The shift toward explosive injuries has resulted in complex multiple-trauma cases affecting multiple body regions. In response, the military trauma system has introduced improved bleeding-control devices such as tourniquets that have proven to enhance survival rates, especially in cases of traumatic extremity amputation or vascular injury. The increased use and effectiveness of tourniquets have contributed significantly to improving casualty survival in modern conflicts.4,22 Over the past 2 decades there have been numerous investigations demonstrating the safety and efficacy of tourniquet use on the battlefield.2,15,23-26 Early and judicious use of tourniquets became the cornerstone of care on the battlefield and the centerpiece of the Department of Defense's Tactical Combat Casualty Care program.9,27 After the implementation of tourniquets across the Department of Defense, there was a 67% decrease in deaths due to limb hemorrhage. The overall reduction in deaths from preventable hemorrhage, specifically extremity trauma amenable to tourniquet placement, is a testament to benefits of standardized Tactical Combat Casualty Care training among military units. 10
Tourniquet use has consistently demonstrated significant benefits in mortality and morbidity in combat. A study of 4297 casualties with extremity injuries between 2001 and 2010 showed that there was a 10fold increase in tourniquet use from 4 to 40%. 26 This increase in use lead to a rise in casualty survival rates when injuries were amenable to tourniquet use, with a 98% survival rate in Abbreviated Injury Scale 3 (ie, serious injury) and a 76% survival rate for Abbreviated Injury Scale 4 (ie, severe injury). 26 A review of service members in Iraq and Afghanistan between 2003 and 2011 showed a 96% survival rate for soldiers with wounds treated by tourniquets, with open fractures being the primary reason for tourniquet application. 15 A large systematic review of tourniquet use in Iraq and Afghanistan demonstrated that tourniquet use improved survival in patients who experienced extremity trauma if they were used prior to the onset of shock. 1
The military use of tourniquets for battle casualties has been demonstrated to be safe with little risk to life or of significant long-term morbidity. 2 In 2008, Kragh et al published a review of tourniquet use in 232 patients who had 428 tourniquets placed on 309 critically injured extremities. The rate of transient nerve palsies was 1.7%. No amputations were directly attributed to tourniquet application. 3 Another study of tourniquets applied to 651 limbs found that rates of clot, myonecrosis, and nerve palsy were, respectively, 3, 1.5, and 1.4%. Again, no amputations or deaths were determined to have occurred directly from tourniquet placement. 3
Military Lessons Applied to a Civilian Setting
The positive results from military investigations of safety and efficacy lead to adoption of tourniquet use in many civilian settings. Initially, there were concerns within Emergency Medical Services (EMS) practice regarding lack of civilian specific research and a lack of application to the civilian medical setting.28-30 However, over time, civilian EMS felt that the totality of the military evidence demonstrated reasonable safety and efficacy. Furthermore, some data suggested that the prevalence of high-energy penetrating trauma was similar to injury patterns found in the military and common enough to justify tourniquet use. 31 Many services felt that it was prudent to train prehospital providers on tourniquet use and place them into service with careful oversight of data and patient outcomes.32,33 Analysis of the National Emergency Medical Services Information System database demonstrates a marked rise in the use of tourniquets between 2008 and 2016. In 2008, the database showed >3.1 million EMS activations and no documented instances of tourniquet application. 34 In 2016, there were >29.9 million EMS activations and 3995 documented events where a tourniquet was applied. 34
Part of the impetus for the adoption and use of tourniquets in the civilian world has been a dramatic increase in civilian trauma. Deaths from trauma in the civilian world have increased at twice the rate of population growth.32,35-37 Tourniquet use in some of these terrible circumstances has shown significant benefit. 38 A review of the Boston Marathon bombing showed no risk to life with tourniquet use and a complication rate of 2.1%. During the same event, bleeding time was controlled in 91% of patients with tourniquets. 39 Other publications regarding tourniquet use during the Boston Marathon bombing suggest that better training and implementation of military lessons learned may have resulted in even better trauma care at the point of injury. 40
Numerous other studies and reviews have demonstrated similar efficacy with tourniquet use in the civilian population. 41 In 2012, an ambulance service in North Carolina equipped its personnel with tourniquets. The experience of the organization was that no tourniquet-related complications were encountered, and there was a decrease in the incidences of shock, inpatient admissions, and blood transfusions. 42 Other services described similar findings. 39 Evaluation of the National Emergency Medical Services Information System database in 2019 by Hashmi et al demonstrated improved survival to hospital discharge when they retrospectively reviewed trauma activations for matched patient cohorts with extremity injuries that received tourniquets compared with those that did not. 43 Teixeria et al performed multivariable analysis of 1026 patients with major peripheral vascular injuries and found that tourniquet application was independently associated with survival to discharge. 44
While most of these studies were done in large urban areas and trauma centers with relatively short transport times, the benefits of tourniquet use in the wilderness and austere civilian settings may be significant. Under these circumstances, access to advanced trauma care may be prolonged and very limited. Despite the theoretical benefit in this environment, there is a remarkable knowledge gap. No good data exist regarding tourniquet use in the civilian austere, wilderness, or frontier medicine settings. What little literature is available extrapolates use from the more conventional EMS literature and military data.11,12 Given the body of evidence that exists, and taking into account the considerable benefit vs relatively low risk of intervention, the Wilderness Medical Society Practice Guidelines recommend tourniquet application for life-threatening arterial bleeding or bleeding that has not been controlled with less aggressive techniques. 13
An important aspect of civilian tourniquet use is the growing effort to train lay bystanders and civilian EMS personnel to use tourniquets in emergency situations. After the success rates of the wide use of tourniquets in the military, some efforts have focused on curricula, taught to civilians similarly to cardiopulmonary resuscitation, to train EMS personnel and prepare bystanders as first responders. The STOP THE BLEED course was developed as a collaborative effort between members of the American College of Surgeons Committee on Trauma and the National Association of Emergency Medical Technicians.19,21 Their efforts have increased awareness and education for the general public regarding tourniquet use and focus on four steps: call 911, apply pressure with hands, pack wound and press, and apply a tourniquet if the bleeding is still uncontrolled.19,21 Available data suggest that the program can effectively improve a layperson’s self-efficacy, willingness to apply a tourniquet, and ability to do so.20,45 Limitations may come from the length of the course, variability among instructors, the possible lack of recurring training, and the lack of education on tourniquet conversion.
Complications of Tourniquet Use
Despite the substantial benefits of tourniquets, there are some risks, morbidity, and complications associated with their use.15,26,39,42,46,47 Prolonged application of tourniquets (>6 h) has been known to result in fasciotomy, venous thromboemboli, nerve palsy, compartment syndrome, myonecrosis, and secondary metabolic effects of reperfusion injury.3,48 Available case studies, case series, and reviews have carefully documented these complications, and although these sources demonstrate the effective preservation of life, they express caution and recount the management of these complications.46,47,49 These adverse events are thought to be a result of direct tissue injury, venous congestion, and ischemia caused by arterial occlusion. The push to consider tourniquet conversion arises from the desire to reduce the risk of such complications.
Prolonged tourniquet placement can lead to ischemic injuries. Animal model experiments have shown that damage during ischemia may be mediated via superoxide overproduction and reduced antioxidant activity. 50 While in general a tourniquet applied between 6 and 8 h may result in significant morbidity, there is no clear consensus regarding precisely how long a properly applied tourniquet is safe. Based on data from animal models and extrapolation from orthopedic surgical procedures, the safe time falls between 1 and 3 h.47,51-54 Some authors, however, recommend caution applying the time frames reported in this literature and propose that safe ischemic time is likely shorter in a patient who has sustained significant injury, hemorrhage, and shock.8,55 The current recommendation for tourniquet conversion is to make every effort to convert within 2 h if bleeding can be controlled by other means.5,9,56
Another well-documented complication of tourniquet placement is pain.9,57,58 Most awake patients will require significant analgesia to tolerate tourniquet placement, and this increased need for analgesia may become a factor in resource-limited environments.5,9,59,60
Lastly, a significant issue of tourniquet application is incorrect or inappropriate application.6,9,45 Enhanced training and awareness (encompassing laypersons) have resulted in a rise in tourniquet use. Some authors have expressed concern that this is leading to overuse of tourniquets.6,9,45 While overuse of tourniquets is a concern to consider, the value that comes from tourniquet awareness far outweighs the detriment of overapplication. Most of the issues that arise from tourniquet use stem from ineffective tourniquet placement, which indicates a technique flaw that would be corrected with more effective training. Education on proper tourniquet administration should include proper assessment, indications for application, and, in certain cases, indications for conversion to pressure dressings. Increased emphasis on tourniquet placement technique and complete extinguishing of extremity pulses is needed. Reinforcing this skill during training will correct many of the negative outcomes that we see from tourniquet use while continuing to capitalize on the benefits of widespread awareness of tourniquet value. The need for tourniquet conversion training is increased in environments where the transport time is increased, especially in systems that actively train laypersons in tourniquet application.
Tourniquet Conversion for Prolonged Prehospital Times
Current military protocols for tourniquet conversion are available from the Committee on Tactical Combat Casualty Care, which state that “[e]very effort should be made to convert tourniquets in less than 2 hours if bleeding can be controlled with other means. Do not remove a tourniquet that has been in place more than 6 hours unless close monitoring and lab capability are available.” It is important to note that this guideline is the mandated standard for battlefield trauma care in the US military and specifically refers to extremity tourniquets. Most current guidelines state that limb and junctional tourniquets should be converted to pressure dressings as soon as possible or tactically feasible.5,9,30 The guidelines outline 3 requisite conditions prior to converting a tourniquet: 1) the patient is not in shock, 2) the wound can be monitored for rebleeding, and 3) the tourniquet is not placed above a traumatic amputation.
One important note regarding a contraindication to tourniquet conversion is if it has been in place longer than 6 h.5,8,9,61 In these circumstances, significant ischemia over a very long period can result in reperfusion injury and has been shown to cause acute lung injury.5,9,62 Acute kidney injury due to rhabdomyolysis is also a risk after prolonged tourniquet placement.5,9,63-65
Kidney injury in this setting could be severe and could result in acute metabolic acidosis as well as hyperkalemia.5,9,66-68 Therefore, the rationale for not converting a tourniquet in the field if it has been in place longer than 6 h is so that the patient can be closely monitored in a critical care setting with robust medical and surgical capabilities that can manage these complications5,7,9,63 (Figures 1 and 2).
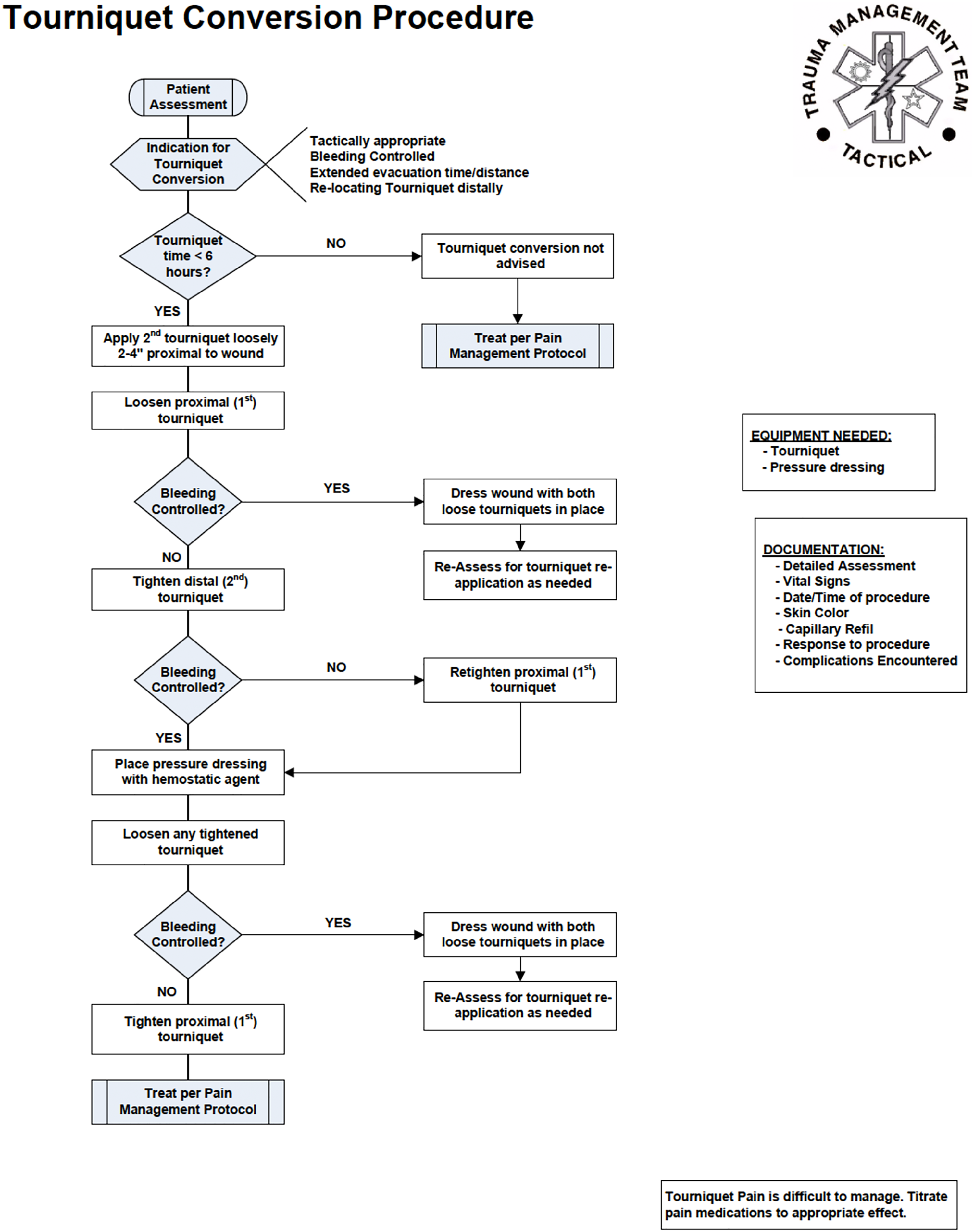
Ranger Medic Handbook tourniquet conversion procedure. 70
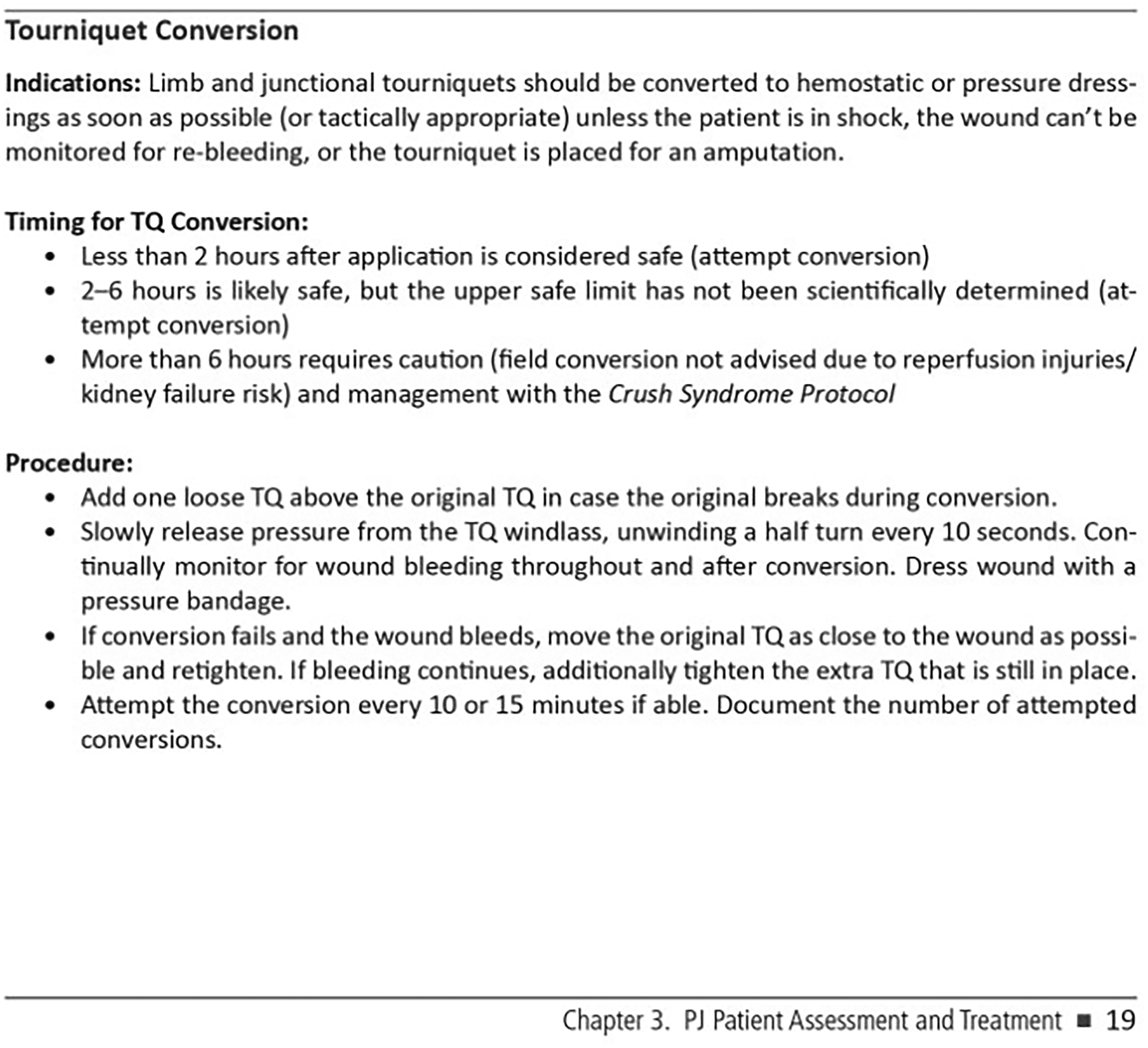
Pararescue Medical Operations Handbook (8th ed.). 71
Few guidelines currently exist for civilian agencies to perform tourniquet conversion. Doyle et al published a guideline outlining considerations for the procedure in a civilian EMS environment as early as 2008, and there are military protocols available that would need only minor adaptations.7,67 However, to our knowledge, no civilian EMS systems are actively performing this procedure. Levy et al recently published a safe and reasonable guideline for prehospital tourniquet removal in the emergency department, carefully reviewing clinical decision making as well as procedural steps in conversion. 68 The guideline that the interdisciplinary group of experts (ie, emergency medicine, trauma surgery, and military physicians) developed, however, was designed for emergency department physicians and staff. Generally speaking, the recommendations for considering tourniquet conversion were similar to those of the military.
Data on the safety and efficacy of tourniquet conversion are sparse and represent a knowledge gap. Several investigations have proposed algorithms for prehospital conversion.5,7,8 Lakstein et al published their experience with prehospital tourniquet application and conversion to nontourniquet hemostatic dressings with the Israeli Defense Force. 69 Seventeen attempts were made to convert tourniquets, and the Israeli Defense Force was able to maintain effective hemostasis in 76% of attempted conversions. All 17 tourniquet conversions where done on “non-injury-related” indications, defined by the Israeli Defense Force as extremity bleeding in care under fire situations, in total darkness, or during mass-casualty events. 69
More research is needed to conclusively determine whether tourniquet conversion provides patient-oriented clinical benefit in the civilian world. However, given the well-documented morbidity and complications from tourniquet placement, equipoise certainly exists for exploring this procedure further. This is particularly true given the relatively low risk of the procedure (if hemorrhage recurs, the tourniquet is simply reapplied) and the potential benefits of a reduction of adverse events. It is reasonable and prudent for civilian EMS agencies, such as search and rescue, the National Park Service, or extremely rural/frontier organizations, that may experience significant prehospital time to incorporate guidelines for tourniquet conversion (Figures 3 and 4).
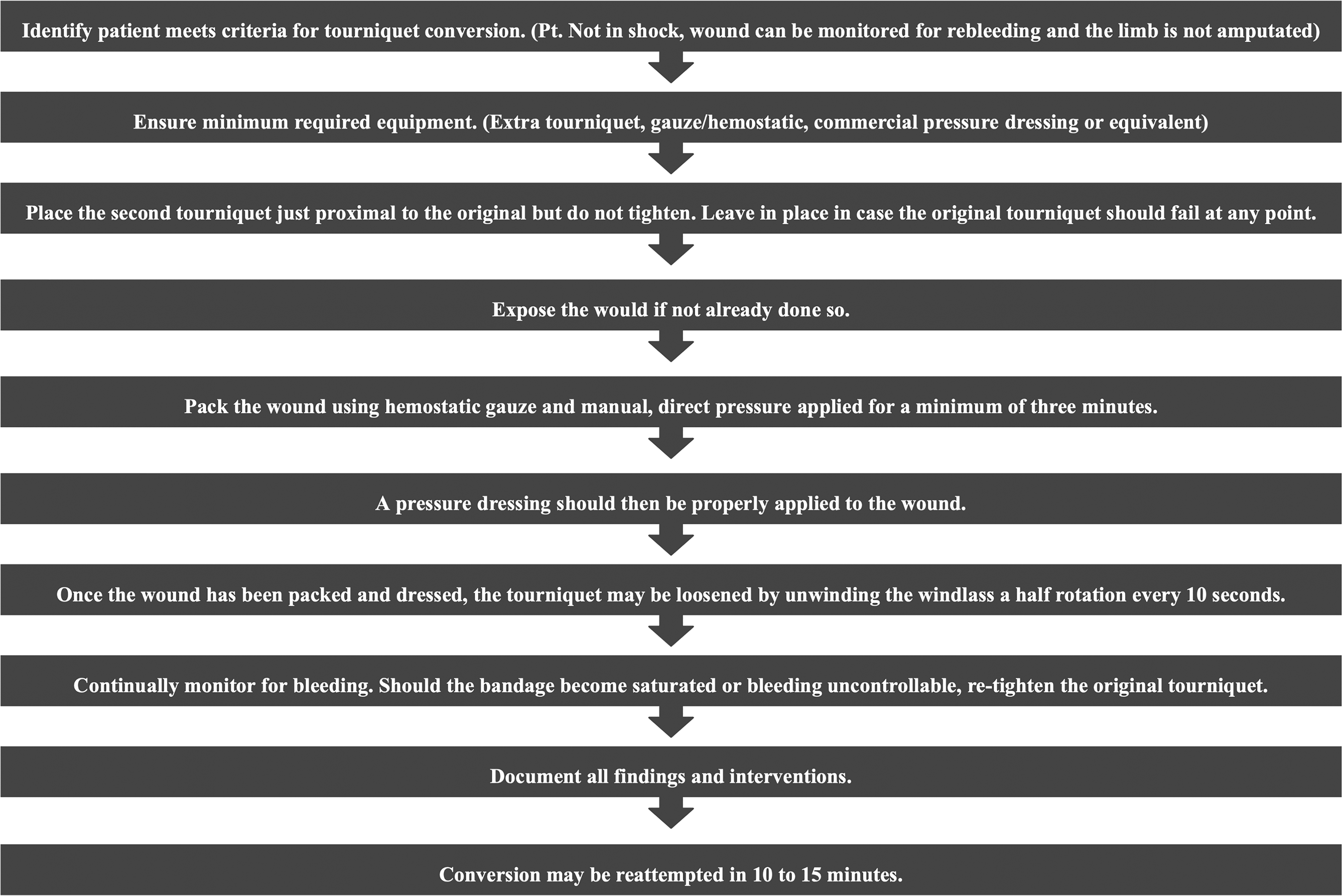
Suggested tourniquet conversion guidelines.

Conclusion
Tourniquet application can save lives in the setting of life-threatening extremity hemorrhage, and tourniquets have been shown to be overwhelmingly safe and effective in the military and civilian prehospital settings. Any medical service that is using tourniquets as a treatment measure needs to implement tourniquet conversion education into the tourniquet training. Implementing the US military's Committee on Tactical Combat Casualty Care's recommended guidelines for prehospital tourniquet conversion into the education and training programs for first responders and prehospital personnel has the potential to significantly reduce the adverse effects associated with life-threatening extremity hemorrhage.
Case Report
A 26-year-old male was BASE jumping in a remote canyon. A parachute malfunction led to an uncontrolled descent into a talus field, where the patient sustained a Grade 3 open left ankle trimalleolar equivalent fracture and dislocation with syndesmotic disruption. The open wound was compounded by spurting blood. The injury was sustained at 1918, and a tourniquet was applied by the patient. Due to the remoteness of the location, the paramedics did not arrive until 2134. Ketamine was administered, the tourniquet was converted to a pressure dressing (2 h and 17 min after application), and the open fracture was cleaned and splinted.
Search and rescue arrived at 2219, and the patient was packaged and extricated from the canyon by 0045 the following day and did not arrive at a hospital until 0302. Time from tourniquet application to hospital arrival was 7 h and 2 min.
The patient underwent surgical debridement and internal fixation of the left ankle lateral malleolus and left ankle syndesmotic disruption. At the 1-y follow-up, the patient had regained 95% of range of motion and use with mild hypoesthesia around the site of injury and closure.
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.