
Abstract
The Wilderness Medical Society reconvened an expert panel to update best practice guidelines for spinal cord protection during trauma management. This panel, with membership updated in 2023, was charged with the development of evidence-based guidelines for management of the injured or potentially injured spine in wilderness environments. Recommendations are made regarding several parameters related to spinal cord protection. These recommendations are graded based on the quality of supporting evidence and balance the benefits and risks/burdens for each parameter according to American College of Chest Physicians methodology. Key recommendations include the concept that interventions should be goal-oriented (spinal cord/column protection in the context of overall patient and provider safety) rather than technique-oriented (immobilization). An evidence-based, goal-oriented approach excludes the immobilization of suspected spinal injuries via rigid collars or backboards.
Keywords
Introduction
Techniques for immobilization and extrication of the patient with a real or potential spine injury have been implemented for decades, albeit without high-quality evidence supporting their use. Such techniques addressed well-intentioned concerns about inflicting further serious injury, but there is increasing evidence that such interventions may be harmful. Historic principles of out-of-hospital spinal injury care have been more influenced by medicolegal implications and untested theory than by clinical or scientific evidence. The high cost of defensive medicine in this regard—in terms of dollars, resources, and risk of patient injury—is unlikely to be justified in the nonwilderness environment. In wilderness environments, any decision to immobilize a spine is even more significant and can be directly associated with the potential for further injury to the patient and to rescuers. When a person is injured in the wilderness, rescuers may be risking their own lives to provide safe extrication. Under these circumstances, the need for sound evidence in clinical decision-making is even more paramount. This is especially true for interventions that may introduce vastly more complex operations, such as converting a walkout of a nonimmobilized patient into a carryout of an immobilized patient.
To develop proper guidelines for spinal cord protection (SCP) in the wilderness environment based on the best existing evidence, an expert panel was convened in 2011 to develop evidence-based guidelines. 1 The guidelines were revised in 2014 2 and again in 2019. 3 This current publication marks the 2024 update to the 2019 guidelines. A key philosophical difference introduced in the 2019 update was a movement away from technique-based principles, determining when and how to immobilize, to goal-based principles, determining how to best protect the spine from initial or secondary injury. The 2024 update includes an algorithm, introduction of new evidence, and studies completed since the last update, and a revised and simplified discussion.
Methods
The original practice guidelines were created by experts in the field who convened at the Wilderness Medical Society meeting in 2011 and published their findings in 2013. 1 Members of the current revision team have a variety of professional backgrounds: 1 orthopedic surgeon, 2 paramedics active in academics and field medical care (1 military and 1 civilian), 1 emergency and emergency medical services (EMS) physician, 1 military/tactical clinician, 1 wilderness EMT, and 1 family practitioner with sports medicine fellowship training. (Throughout these guidelines, we use the term “clinician” to refer to the conglomerate group of any personnel who deliver health care, and the term “practitioner” to refer to the conglomerate group of physicians, PAs, and advanced practice registered nurses [APRNs] who have prescribing capability and varying degrees of autonomous or semi-autonomous practice. We don’t use the term provider. This follows nomenclatural standards of the National Association of EMS Physicians, 4 the Western Journal of Emergency Medicine, 5 the American Medical Association, 6 the Association of American Medical Colleges, 6 and Wilderness Medicine Magazine. 7 )
Relevant articles were identified through the PubMed and Cochrane Collaboration databases using keyword searches with the appropriate terms corresponding to each topic. Peer-reviewed studies related to spine immobilization and SCP, including randomized controlled trials, observational studies, and case series, were reviewed, and the level of evidence supporting the conclusions was assessed. Abstract-only reports were not included. Conclusions from review articles that did not perform systematic meta-analysis, textbooks, and other publications were not considered in the formulation of recommendations but may be cited to provide context. When no relevant studies were identified, the expert panel recommendation was based on risk/burden versus benefit perceptions derived from patient care experience, case studies, and topical review publications. The panel used a consensus approach to develop recommendations regarding management of potential or actual spinal injuries in the wilderness.
These recommendations have been graded based on clinical strength as outlined by the American College of Chest Physicians (online Supplementary Table). 8
Scope of the Problem
Historically, the incidence of spinal cord injury (SCI) in the United States has been estimated at 54 cases per million people per year, representing 3% of hospital trauma admissions.9,10 The National SCI Statistical Center found that 38% of these injuries were due to vehicle accidents, 32% from falls, and 14% from violence. A Norwegian epidemiologic study 11 revealed an incidence of cervical spine fractures of 12 out of 100,000 per year. The incidence of open surgery for these injuries was 3 out of 100,000 per year.
Previous studies have shown that 2% to 10% of patients with SCI will demonstrate neurologic deterioration (ascending SCI) after initial neurologic testing. Factors attributed to neurologic deterioration include initiation of traction/immobilization and intubation (early [<24 h]), sustained hypotension (delayed [2–7 d]), and vertebral artery injury (late [>7 d]). Effectiveness of prehospital care and method of immobilization/transport have not been linked to neurologic deterioration.12–14
Many articles have been repeatedly quoted in the literature as offering case evidence of neurologic deterioration in the presence of SCI secondary to inadequate out-of-hospital immobilization.15,16 Careful review of these cases, however, reveals that virtually all represent missed or late diagnoses after hospital admission or deterioration that occurred while under treatment for a known diagnosis.
Authors have noted an improvement in the neurological status of patients with spinal cord injury arriving in emergency departments over the past 30 y. During the 1970s, 55% of patients referred to SCI centers arrived with complete neurologic lesions, whereas in the 1980s, that number decreased to 39%. 17 This improvement in neurological status has been attributed to EMS initiated in the early 1970s. However, there is no specific evidence to support the belief that this improvement has anything to do with EMS protocols. It is likely that improvements in automobile safety and design, along with compulsory seat belt use laws, are at least partially responsible for these observations. Review of data from the national automotive sampling system data files between 1995 and 2001 revealed 8412 cases of cervical spine injury. 18 Approximately half (45%) were unrestrained occupants, and the remainder consisted of belted only (38%), airbag only (9%), and both (8%) restraint systems.
The focus of these guidelines is to present an evidence-based approach to out-of-hospital care in wilderness environments that minimizes the possibility of neurologic deterioration or injury exacerbation in the presence of an existing or potential SCI from the time of extrication to arrival at a medical facility.
Spinal immobilization itself is not a benign procedure. In addition to the risk of further injury to the patient because of increasing the danger of rescue, spinal immobilization itself is associated with documented risks and rather extreme discomfort. Although the expert panel was unable to identify a single well-documented case in the literature of out-of-hospital neurologic deterioration as a direct consequence of improper or inadequate immobilization, many cases have documented severe morbidity, and even mortality, secondary to immobilization itself.10,19–32
It is important to recognize and/or attempt to differentiate 5 types of spinal injury scenarios:
an uninjured spine a stable spine injury without existing or potential neurological compromise an unstable, or potentially unstable, spine injury without apparent neurologic compromise an unstable spine injury with neurologic compromise an injured patient with unknown spinal injury status
Historically, if immobilization were to be used, it was thought to be indicated for numbers 3, 4, and 5. However, a close reevaluation of the evidence calls into question whether spinal immobilization is helpful in the wilderness out-of-hospital environment for any of these types of patients.
The phrase “clearing the spine” has many definitions depending on circumstances and the training level of the provider. It is generally regarded as more vernacular than academic. For instance, depending on the environment and caregiver, a “cleared” patient may have no evidence or suspicion of spine injury whatsoever, a low enough probability of injury to not need to have vertebral or SCI considered and not need radiographic imaging based on decision rule criteria (eg, national emergency x-radiography utilization study [NEXUS]), 33 or radiographic imaging with no demonstrable injury. Furthermore, some wilderness medicine educational organizations teach that “clearing” the spine is performed only for determining evacuation modality and not for determining the presence or absence of spinal injury. Such definitive determination is only made at a receiving facility.
In the modern era of out-of-hospital trauma care, any discussion regarding “clearing the spine” (ruling in or out possible spinal injury) relative to immobilization is a moot point anyway. If there is no evidence that spinal immobilization helps patients but increasing evidence that it hurts patients, it should not be considered as an intervention in the first place. Identifying potential vertebral or spinal cord injuries then assumes its rightful place as one among many considerations in managing a traumatized patient. All that is required is the intuitive consideration of reducing motion if injury is suspected.
Most importantly, the philosophy and biomechanical physics behind the concept that spinal immobilization is a desired goal has been questioned.34,35 A more recent theoretical argument maintains that spinal motion restriction (SMR) should be the desired goal and not strict immobilization.35,36 Although these sound similar, motion restriction is very different from immobilization, both theoretically and in terms of technique. This concept of SMR has gained popularity in out-of-hospital care. The American College of Surgeons Committee on Trauma (ACS-CT), American College of Emergency Physicians (ACEP), and the National Association of EMS Physicians (NAEMSP), as well as other endorsing agencies, have published a joint position statement advocating for SMR rather than immobilization in the trauma patient. 37 A main point of consensus is that current practices do not provide true immobilization of the spine, but with the goal of SMR, a potentially injured spine may be protected by minimizing unwanted movement. 36
Although it may have fewer risks and may vastly simplify the logistics of wilderness rescue operations, there is no evidence that SMR is any more protective of the spinal cord than spinal immobilization. Cadaver studies suggest that physiological movement is unlikely to result in further SCI in a patient with possible or actual vertebral or SCI. 34 Therefore, critical to our analysis of the literature is the understanding that the greater the degree to which an intervention produces absolute immobilization, the less desirable it may be.
This runs counter to the out-of-hospital standard of care for the past half-century, but it appears to be a more evidence-based perspective. 31 Given the scant evidence that physiological motion, in fact, causes further injury, simply replacing SI with SMR may reduce risk but may not actually be helpful either as a mechanism.
This supports the idea that we should move from simply describing mechanisms (“spinal motion restriction,” “spinal immobilization”) and toward goals. This mirrors other evolutions in health care, where “intubation” is now more generally categorized within “airway management,” and “CPR” is now more generally categorized within “resuscitation.” 38 Most authors following this principle have adopted the goal-oriented terminology of “spinal cord protection.” The basic gist of this argument is that we know our goal is to protect the spinal cord, but evidence is lacking with regard to how this should be performed. Most authors using the goal-oriented term SCP believe the evidence suggests SMR is the best current mechanism to accomplish that goal and that the mechanism of spinal immobilization specifically does not meet the goal of SCP.39–41
Indeed, there appear to be consistent themes in the treatment of possible SCI that transcend the operational environment and are universal to out-of-hospital care. 42 In the sports medicine discipline, the National Athletic Training Association (NATA) has been working with cervical spine injuries consensus statements and is currently considering SMR not only for sports in wilderness environments but also on the sideline and courtside environments as well. NATA's consensus recommendations for prehospital care of the injured athlete with a suspected catastrophic cervical spine evaluated 8 questions regarding spinal cord injuries. One of these questions was, “What method of transfer and spinal-motion restriction is associated with the best outcomes for athletes with suspected CSIs in both the supine and prone position?” The group found that vacuum splints were equivalent to rigid collars regarding spinal motion restriction. 43
Preferred Position for the Injured Spine
Although no studies have specifically evaluated an optimal generic position for the injured spine, clinical evidence from decades of operative spine surgery (derived from imaging and patient care experience with traction, manipulation, and operative reduction) would strongly suggest that neutral alignment is preferred.
In cases of airway compromise or the need to establish an airway, a jaw thrust is preferable to head tilt/chin lift due to its superior airway clearance and decreased neck movement. 44
Methods of Extrication with Possible Cervical Spine Injury
Analysis of neck motion during extrication from an automobile using an infrared 6-camera, motion-capture system revealed that strategies permitting individuals to exit the vehicle under their own volition with cervical collar in place resulted in less motion of the cervical spine than extrication by experienced paramedics. 45 A similar biomechanical study corroborated these findings. 46 Dixon et al also reinforced self-extrication as the method of choice; self-extrication from a motor vehicle resulted in less spinal motion compared with different extraction methods.
Their study included self-extraction with no cervical collar and only verbal instructions, extraction with a cervical collar and physical assistance, extraction with spine board through the rear and passenger side of the vehicle, and short ejection jacket through the driver door. Six trained emergency professionals assisted with each method, reflective markers were placed on the victim's bony prominences, and motion was tracked using circumferential cameras. They concluded that self-extraction with verbal instructions and no assistive devices was the most stable extraction method. Of note, the use of backboards resulted in more motion, which was increasingly the case as the victim's body weight increased. 47 A more recent study showed cervical collar application without instructions applied to self-extrication from a vehicle was more effective at reducing cervical spine movement than the same procedure without a collar, but neither subjects nor vehicle were injured, raising the question of how applicable this would be to an injured population. 48
A radiographic comparison showed superior immobilization of the normal cervical spine during extrication from an automobile with a Kendrick extrication device (KED) plus Philadelphia collar compared with short board, tape, and collar. 49 Similar benefits have been demonstrated in other studies with the KED, as well as comparable devices.50–52 Alternately, Gabrieli et al in 2020 found that cervical spine motion was reduced by applying a rigid cervical collar but not an extrication device. 53
However, all this presupposes that immobilization is a desired outcome. Should the desire simply be motion restriction, it is likely that many options are equally viable. The most important principle in spinal injury management would be to not cause further harm to the patient.
Currently, our author group cannot find case studies in which harm was caused by failure to place a cervical collar or a backboard, but we found increasing evidence, both actual and theoretical, that these interventions can cause harm. Furthermore, with clear instructions, patients appear capable of maintaining a stable neck for extrication without a cervical collar. 48 Soft collars may play a role in reminding patients of this as well as improving comfort, provided they don’t interfere with the airway or medical care. Porter et al demonstrated that a soft collar could be improvised in a wilderness setting by molding a fleece jacket; prospectively studying movement in 24 healthy volunteers, they found that an improvised fleece collar was noninferior at limiting motion compared to a rigid cervical collar and was more comfortable. 54
If injuries or other circumstances such as unconsciousness prevent controlled self-extrication, patients’ cervical spines should be packaged to reduce passive motion, and the airway should be adequately managed without a goal of absolute immobilization. There is no requisite role for commercially made or improvised rigid cervical collars in an out-of-hospital environment.
Moving the Patient with Real or Potential Spine Injury
Manual cervical traction is the standard technique for moving patients with known spine trauma in the hospital setting. This is done to keep the spine in the anatomic position and to prevent distortion of the spine, which might occur otherwise. Traction is often used for stabilization and reduction of unstable spine injuries. In the monitored hospital setting, up to 68 kg of cervical traction has been used safely in the reduction of unstable spine injuries. 55 Excessive traction can be dangerous in a grossly unstable spine injury and, therefore, should be avoided in the unmonitored setting. Lift and slide transfer to a backboard results in superior stabilization of the entire spine compared with log-roll. One study also compared 2 methods of providing additional manual cervical spine stabilization relative to maintaining simultaneous stabilization of the thoracolumbar spine: the head squeeze and the trap squeeze. With the head squeeze maneuver, the lead rescuer lets the patient's head rest in his or her palms, with hands on both sides of the head with fingers placed so that the ulnar fingers can grab the mastoid process below and the second and third fingers can apply a jaw thrust if necessary. With the trap squeeze, the rescuer grabs the patient's trapezius muscles on either side of the head with his or her hands (thumbs anterior to the trapezius muscle) and firmly squeezes the head between the forearms with the forearms placed approximately at the level of the ears (Figure 1). The trap squeeze was superior to the head squeeze in this study, particularly with simulation of an agitated patient. 56

Demonstration of trap squeeze technique for manual cervical spine stabilization. (Quinn et al. 2 Reprinted with permission from the Wilderness Medical Society. ©2014 Wilderness Medical Society.)
The superiority of the lift and slide transfer over the log-roll in providing stabilization of the entire spine has also been demonstrated in other studies.57,58 We are unaware of any evidence that would preclude transportation in the lateral decubitus position. Patients with spine injury are frequently placed in the lateral decubitus position without ill effect when hospitalized.
Lateral positioning is of interest because airway protection is paramount, and traumatic brain injuries may occur concurrently with potential or actual cervical spine injuries. In a cadaver study, unstable C5-6 motion was monitored with electromagnetic sensors as 4 participants performed log-rolled transfer, and 2 participants used lateral position. The study concluded that in 5 of 6 planes there was no significant difference in range of motion. However, in the medial to lateral plane, 1.4 mm of motion was recorded and was found to be statistically significant. These results suggest that lateral positioning is appropriate in certain situations. 59
Effectiveness of Spinal Immobilization in Reducing the Incidence of Neurologic Sequelae
A Cochrane review found no randomized controlled trials of spinal immobilization. The authors of that review concluded that the effect of spinal immobilization on mortality, neurological injury, spinal stability, and adverse effects in trauma patients remains uncertain. 10 Because airway obstruction is a major cause of preventable death in trauma patients and spinal immobilization can contribute to airway compromise, the authors concluded that the possibility that immobilization may increase morbidity and mortality cannot be excluded.
Another study retrospectively reviewed all patients reporting to 2 university hospitals with acute blunt traumatic spinal or spinal cord injuries transported directly from the injury site to the hospital. One hospital was in New Mexico (US), and the other was in Malaysia. None of the 120 patients treated at the Malaysian university hospital had spinal immobilization during transport, whereas all 334 patients treated at the US university did. There was less neurologic disability in the patients who were not immobilized (odds ratio 2; P = 0.04). 60
In 2022, a large multicenter trial by Chen et al (representing The PATOS Clinical Research Network) found that prehospital spinal immobilization was not associated with favorable functional outcomes in patients with spinal injury, although very specific subgroup analysis did suggest it might be beneficial for patients without traumatic brain injury but with cervical spine injury. This study is notable both for its size (759 patients), its geographic breadth (14 Asian countries), and the fact that retrospectively 41% of patients were not immobilized—this represents a practice pattern that would be unusual in the United States and thus ideal for studying this question. 61
In the United States, EMS systems that studied their own progression from immobilization protocols to SMR protocols did not see any increase in disabling spinal injuries in their patients with a transition to SMR protocols. 62
Effectiveness of the Cervical Collar in Immobilization of the Cervical Spine
Although use of the cervical collar is considered the gold standard in immobilization of the cervical spine, little evidence exists to indicate its effectiveness in immobilizing the cervical spine or that immobilization of the cervical spine is helpful in either patient field management or patient outcome.
An assumption exists that the neutral anatomical position is desired with an injured spine and that the cervical collar accomplishes this goal. However, 1 study demonstrated that more than 80% of adults require 1 to 5 cm of occipital padding in addition to a cervical collar to maintain the cervical spine in the neutral position relative to the torso, dependent upon physical characteristics and muscle development. 63
A separate assumption exists that the cervical collar restricts motion of the cervical spine. When studied, the use of a cervical collar was better than no immobilization, but it did not effectively reduce motion in an unstable spine model. 64 Another study analyzed cervical motion with no collar and with 3 different cervical collar types. 58 Although there was a decrease in the amount of motion generated in every plane of motion as a result of wearing each of the 3 collars, none of the changes proved to be significantly different. In another study, a rigid cervical collar combined with a backboard reduced cervical motion to 34% of normal. 65 Use of head blocks and a backboard reduced motion to 12% of normal. The addition of a rigid cervical collar to the use of head blocks provided no added immobilization benefit, but it did limit mouth opening.
These results have been somewhat contradicted by Podolsky et al, 66 who demonstrated in a similar study that neither collars alone nor sandbags and tape provided satisfactory restriction of cervical spine motion. In their study, the addition of a rigid cervical collar to the sandbags and tape resulted in a statistically significant reduction in neck extension. Lador et al 67 demonstrated cervical distraction at the site of injury with the use of a rigid collar, as well as creation of a pivot point in the cervical spine where the collar meets the skull and shoulders. Others have also demonstrated abnormal separation between vertebrae with the use of cervical collars in the presence of a dissociative injury. 68
Should ligamentous and bony structure integrity be compromised, traction that would normally pull the spine into neutral alignment may simply place tension on the spinal cord. Ivancic 69 performed a biomechanical investigation of 2 types of cervical collars and 2 types of cervicothoracic orthoses. Even though this study demonstrated the increasing effectiveness of immobilization with the more constrained devices, particularly with middle and lower cervical spine flexion and extension, the most restrictive device still allowed 58% of axial rotation and 54% of lateral bending. Another study showed that ski patrollers' use of cervical collars and the removal of ski helmets led to significant cervical spine movement. The authors recommended against helmet removal and cervical collar use. 70 There is a tremendous variety of helmet designs, and each may have its own benefit or risk regarding a cervical spine injury. Each also may have its own method of fastening and removal. Therefore, in keeping with goal-oriented SCP, removal of a helmet may not be in the patient's best interest.
Grenier et al note that the biomechanical benefits of a cervical collar are marginal in the ski environment, cervical collar use negatively affects rescue time, and manual in-line stabilization (motion restriction) had less cervical spine motion than applying a cervical collar. 71 Rigid cervical collars are also difficult to apply correctly and are often incorrectly applied even by those who believe they are competent in this skill. When studied, 89% of providers made at least 1 error in placement, and competence was not related to confidence. 72
Independent of whether cervical collars are effective, their use may be associated with complications related to the collar itself. Cervical orthoses can increase the risk of aspiration and impede the ability to establish an adequate airway. These devices have also been shown to directly compromise respiration. Ay et al 25 demonstrated decreases in forced expiratory volume in 1 s (FEV1) and forced vital capacity with both the KED and long spinal backboard. Another study showed a 15% decrease in FEV1 with a cervical collar and backboard and noted that respiratory restriction was more pronounced with age. 73 Others have demonstrated similar findings.22,23,25 Cervical collars have also been associated with elevated intracranial pressure,30,74–77 pressure ulcerations,78–82 increased venous congestion complicating global brain injury, 83 unintentional strangulation by a cervical collar after attempted suicide by hanging, 83 and concealments of important physical findings such as soft tissue injuries, tracheal deviation, or subcutaneous air.30,78–81,84 These could all complicate evaluation and management of patients in wilderness medical care.
Furthermore, rigid cervical collars have been linked to unnecessary imaging upon arrival at medical centers. 85 A recent systematic review of eighteen studies comparing no collar, soft collar, and rigid collar could not confirm any difference in neurological outcome for any of these interventions. 86 Another multicenter consecutive case series comparing soft collars against rigid collars showed no risk for secondary spinal injury. 87 Two different explorative, biomechanical studies showed no increased benefit to neck movement with additional application of rigid cervical collar—one comparing its application to backboard or vacuum splint, another comparing its application to self-extrication.53,88
Although the expert panel remains unaware of any specific cases of documented neurologic deterioration occurring secondary to absent or inadequate out-of-hospital immobilization, many cases of documented neurologic deterioration, and even death, have now been reported with the use of a cervical collar in patients with ankylosing spondylitis.26,27,89 In these patients with bony vertebral bridging, the rigid collar places focused stress on unstable portions of spine, thus increasing risk of neurologic injury; use should be considered contraindicated. Overall, rigid cervical collars have numerous identified risks and no demonstrated benefit.
We recommend that if the medical history is known, use of any rigid cervical collar is contraindicated in ankylosing spondylitis. Patients with suspected injury should have their necks supported in a position of comfort. Strong recommendation, moderate-quality evidence.
Use of Backboard
Several studies have demonstrated that a vacuum mattress provides significantly superior spine stability/motion restriction, increased speed of application, and markedly improved patient comfort when compared to a backboard90–95 and a cervical collar alone 96 (Figure 2). Alternately, Roessler et al ran a simulation study showing that vacuum mattresses took longer to apply. 97 However, the difference was 3 min in ideal conditions and 4 min in realistic conditions, which may not be clinically significant in a wilderness setting. Vacuum mattress immobilization of the potentially injured spine is the current recommendation of the International Commission for Mountain Emergency Medicine. 98

Demonstration of patient with spinal cord protection implemented via spinal motion restriction of the neck and back using a vacuum splint rather than rigid cervical collar and long board. (Hawkins et al. 3 Reprinted with permission from the Wilderness Medical Society. ©2019 Wilderness Medical Society.)
Immobilizing the Cervical Spine
Anderson et al 99 performed a meta-analysis of data regarding immobilization of the asymptomatic cervical spine in blunt trauma patients. Their analysis revealed that an alert, asymptomatic patient without a distracting injury or neurologic deficit who can complete a functional range-of-motion examination may safely avoid cervical spine immobilization without radiographic evaluation (sensitivity 98%; specificity 35%; negative predictive value 100%; positive predictive value 4%). Although the sensitivity and negative predictive values quoted provide reassurance that clinically relevant injuries are not being missed, the low specificity and positive predictive value would indicate that many patients (96%) are being immobilized unnecessarily.
NEXUS prospectively evaluated 5 parameters in selected emergency department patients with blunt trauma: no midline cervical tenderness, no focal neurologic deficits, normal alertness, no intoxication, and no painful/distracting injury. 33 Approximately 34,000 patients were evaluated. Cervical spine injuries were identified in 818, of which 578 were clinically significant. All but 8 of the 818 patients were identified using the criteria (sensitivity 99%; specificity 13%; negative predictive value 100%; positive predictive value 3%). Only 2 of the 8 had a clinically significant injury, 1 of which required surgery. As with the immobilization data, the positive predictive value would indicate that 97% of patients are still subjected to unnecessary immobilization and imaging.
EMS data were prospectively collected on 8975 patients regarding 5 out-of-hospital clinical criteria—altered mental status, neurologic deficit, spine pain or tenderness, evidence of intoxication, or suspected extremity fracture—the absence of which identifies out-of-hospital trauma patients without a significant spine injury. The authors identified 295 patients with spine injuries (3%). Spine injury was identified by the out-of-hospital criteria in 280 of 295 (94%). The criteria missed 15 patients. Thirteen of 15 had stable injuries (stable compression or vertebral process injuries). The remaining 2 would have been captured by more accurate out-of-hospital evaluation. 100 A similar prospective study with the same criteria collected data on 13,483 patients. 101 Sensitivity of the EMS protocol was 92%, resulting in nonimmobilization of 8% of the patients with spine injuries, none of whom developed neurologic compromise.
Maine has used a prehospital selective spine assessment protocol since 2002. Patients with qualified mechanism of injury (axial load, blunt trauma, motor vehicle collision, adult fall from standing height) are not immobilized if they are reliable (no intoxication or altered mental status), have no distracting injury, have a normal neurological examination, and have no spine pain tenderness. During one 12-month study period, only 1 patient with an unstable spine fracture and 19 stable fractures was found to have been not immobilized by the protocol in approximately 32,000 trauma encounters. 102 The protocol had a sensitivity of 94%, negative predictive value of 100%, specificity of 59%, and positive predictive value of 0%. The single unstable spine injury occurred in an 86-y-old female who injured her back while moving furniture 1 week prior to calling EMS; she had a T6-7 subluxation requiring fixation and was without neurologic injury. Elderly patients (>65 y of age) represented the largest number of stable spine fractures without neurologic compromise but also demonstrated a higher risk of complications (pain, pressure sores, respiratory compromise) from spinal immobilization.
Further data from the same study population published separately revealed that 1301 of 2220 patients were immobilized on the basis of the protocol: 416 (32%) were unreliable, 358 (28%) were considered to have distracting injuries, 80 (6%) had an abnormal neurologic examination, and 709 (54%) had spine pain or tenderness. 102 Of the 2220 patients, only 7 acute spine fractures were identified, of which all were appropriately immobilized under then-current guidelines.
Studies have also validated the prehospital use of the Canadian C-spine protocol.103–113 This protocol investigates 3 questions relevant to whether a patient requires cervical spine radiographs:
Is a high-risk factor present (age >65 y, dangerous mechanism, paresthesia)? Is a low-risk factor present that allows safe assessment of range of motion (simple rear-end motor vehicle accident, ambulatory at any time since injury, sitting position in the emergency department, delayed onset of neck pain, absence of midline cervical spine tenderness)? Is the patient able to actively rotate the neck 45° to the left and right?
In 1 study, the NEXUS criteria were compared to the Canadian C-spine criteria by 394 physicians evaluating 8283 patients, with an overall incidence of 169 (2%) of clinically important spine injuries.
110
The Canadian C-spine rule was more sensitive (99 vs 91%; P < 0.001) and more specific (45 vs 37%; P < 0.001) at detecting spine injuries. A study of 6500 patients evaluated the relationship between mechanism of injury and spinal injury.
114
The authors concluded that the mechanism of injury does not affect the ability of clinical criteria to predict spinal injury. It should come as no surprise that this is the case and that no specific mechanism of injury will prove predictive in a meaningful capacity. There are certainly many cases in which minimal trauma can result in profound cervical spine injury with neurologic deficit (eg, an elderly patient following a minor fall). On the other hand, individuals often escape serious injury even after high-energy trauma.
Konstantinidis et al 115 reported on 101 evaluable patients with cervical spine injury. Distracting injuries were present in 88 patients (87%). Only 4 patients (4%) had no pain or tenderness on the initial examination of the cervical spine. All 4 patients had bruising and tenderness to the upper anterior chest. None of these 4 developed neurologic sequelae or required surgical stabilization or immobilization.
Work by Rahmatalla et al suggests that, if motion restriction is desired, a vacuum splint (Figure 2) is more effective than a cervical collar at limiting cervical spine motion. 96
Penetrating Trauma
Clinically significant spinal injury is rare in the setting of a stab wound but not uncommon following a gunshot wound (GSW).116,117 Neurological deficit from penetrating assault is generally established and final at presentation.21,118,119 In the civilian setting, where GSWs are predominately low velocity, spinal instability rarely occurs. DuBose et al reviewed 4204 patients sustaining GSWs to the head, neck, and torso in a civilian setting. 119 None of the 4204 patients demonstrated spinal instability, and only 2 of 327 (1%) required any form of operative intervention for decompression. They concluded that routine spinal imaging and immobilization is unwarranted in examinable patients without symptoms consistent with spinal injury.
High-velocity penetrating injury of the cervical spine is associated with a high incidence of major vascular injury and airway injury requiring advanced airway protection. Cervical spine immobilization has been associated with a higher incidence of morbidity and even mortality when used in the presence of penetrating cervical trauma.19,21,24,28,120–123 Haut et al evaluated 45,284 patients with penetrating trauma and showed overall mortality to be twice as high in spine-immobilized patients (15 vs 7%; P < 0.001). 21 A common observation in these studies is that cervical spine immobilization could mask important clinical signs, such as tracheal deviation, expanding hematoma, and diminished or absent carotid pulse, and may impair successful endotracheal intubation.19,28,122
The Committee on Tactical Combat Casualty Care recommended a balanced approach to cervical spine precautions when a significant mechanism of injury exists.123,124 The Prehospital Trauma Life Support Executive Committee concluded that there are no data to support routine spine immobilization in patients with penetrating trauma to the cranium, neck, or torso. 124 More recently, ACS-CT, ACEP, and NAEMSP, 42 as well as the Eastern Association for the Surgery of Trauma, 125 published joint position statements recommending that spine immobilization not be used routinely for adult patients with penetrating trauma. This is also consistent with recommendations from leading wilderness EMS/medicine textbooks.38,39
Discussion
The practice of spinal immobilization has been predicated entirely on philosophical, theoretical, and medicolegal grounds, and the justification for its use remains unchanged despite nearly a half-century of widespread use. Despite a lack of evidence clearly supporting spinal immobilization, an absence of documented cases of neurologic deterioration because of inadequate immobilization, and accumulating data challenging both the philosophical and theoretical grounds of immobilization, no randomized controlled trials have yet been performed to validate its ongoing use or stratify any risk/benefit ratio. The financial harm to the system is likely enormous, measured in both direct and indirect costs. Conversely, the routine use of spinal immobilization in the wilderness environment not only increases the financial cost of rescue operations, it also greatly increases the time, logistics, danger, and complexity of the operation, thereby also exacting a cost in terms of increased morbidity and mortality to not only the patient but to rescue personnel as well.
In the wilderness environment, the goal of spinal assessment and care should not be to definitively rule out or recognize all forms of spine injury. Rather, the goal should be to minimize the risk of missing and/or exacerbating a potentially unstable spine injury. The risk of missing such an injury should be appropriately calibrated against the risk of exposing rescuers to the potential for serious injury or causing further injury to the patient. It appears the NEXUS criteria and components of the Canadian C-spine rule are overly restrictive, particularly regarding the mechanism of injury, when used in the wilderness environment to evaluate cervical spine injury. Although similar algorithms have not been developed for the thoracolumbar spine, one could argue that similar rules and conditions would be appropriately applicable.
It is fortuitous and insightful that the vacuum splint has become popular in the rescue environment. Not only is this device portable and rapidly deployable, but it appears quite likely to provide superior spine motion restriction (should that be desired) in addition to its other packaging and evacuation benefits, not the least of which is enhanced patient comfort and a decrease in the likelihood of complications associated with a cervical collar and backboard (Figure 2).
After meticulous review of the literature, and in combination with the collective expertise of the authors, we recommend that there is no medical role for rigid backboards or rigid cervical collars in a wilderness environment.
Definitive spinal evaluation can and should be performed upon arrival at an appropriate medical center but is not a feasible goal for wilderness medical care. When patients have sustained blunt trauma, with or without concomitant penetrating trauma, the mechanism of injury must be evaluated as it relates to the overall context of the patient and scene. Judgment regarding the likelihood of associated spinal injury should be individualized, as no reasonable guidelines are practical given the wide and disparate combinations of trauma and injury. As previously discussed, in appropriate circumstances, severe spine trauma can result from minimal trauma (particularly in the elderly), yet patients can often escape serious injury following the most dramatic trauma and do not appear to require any more aggressive intervention than passive motion restriction with soft interventions like padding or encouragement of conscious patients not to move in any way that is painful, all of which should be intuitive interventions anyway.
If the patient is suspected of having a serious spinal injury, it is likely even more important that the spine not be immobilized. This principle may appear counterintuitive, but the chance of immobilization causing harm increases the less alert a patient is (regarding airway or delay in care attempting to immobilization) and the more injured the spine is (an actual vertebral or SCI is more likely to have significant deleterious effects from spasming and inflammation than a strain, sprain, or contusion). All patients with evidence of neurologic deficit should have SCP principles implemented, avoiding total immobilization.
Since our 2019 recommendations that rigid cervical collars and spinal immobilization had no requisite role in wilderness EMS or rescue operations, numerous organizations have followed suit with similar recommendations, guidelines, and protocols. 126
In 2022, Geduld et al designed a scoping review of 42 articles that explored possible barriers to implementation of SCP (manifested as SMR) in low resource settings versus older models of universal immobilization. Key issues they identified include confusion in terminology, poor guideline compliance and implementation, and a lack of context-specific evidence. We agree these issues need further attention in the literature and hope our own clinical practice guidelines here offer support to overcome those barriers. 127
Previous practice guidelines, including our own, have presented algorithms suggesting a range of motion testing as a tool for evaluating the need for attention to possible SCI. The premise for range of motion testing is based on the well-validated use of flexion/extension cervical spine radiographs to clear a cervical spine. For years (prior to magnetic resonance imaging), this procedure served as the “gold standard” used to definitively clear the cervical spine in a medical center, based on the knowledge that a standard lateral c-spine x-ray may appear normal in the presence of significant soft tissue injury with underlying spine instability. Flexion/extension cervical spine radiographs have been routinely performed under the direct volition of the patient under the premise that alert patients will not cause themselves neurologic harm in the presence of an injury with the capacity to do so. To our knowledge, no adverse patient reaction has been reported after many years of use, and this further argues against the necessity for immobilization. The ability to perform the maneuver, and the extent to which range of motion should occur, should be left entirely to the alert patient; pain alone should not be used as a disqualifier to interrupt the maneuver. This technique may remain useful as another tool in determining whether SMR is even desirable in the first place.
In our 2019 update, we eliminated algorithms on the assumption that if the only intervention was reduction of painful movement, this would be intuitive and not require special direction. 3 However, since 2019, we’ve received extensive feedback that an algorithm would be helpful. Some have built their own based on our recommendations. Just before the turn of the century, an algorithm that could selectively exclude people from requiring spinal immobilization was extreme. Now it is so commonplace that not having an algorithm is radical. To ease this transition, we have built an algorithm for suspected spinal injuries that reflects current recommendations and accommodates familiar elements of NEXUS, Canadian c-spine rule, and existing selective spinal exam criteria frequently in use (Figure 3). Deciding whether to explore SCP measures can be safely accomplished by clinicians with at least a basic working knowledge of the fundamental elements. That is, the clinician should be able to recognize degrees of major trauma, identify mechanisms of injury with the potential to cause spinal injury, perform a basic physical examination of the spine and neurologic system, recognize distracting injuries, and consequently recommend passive SMR or soft padding or vacuum splinting.
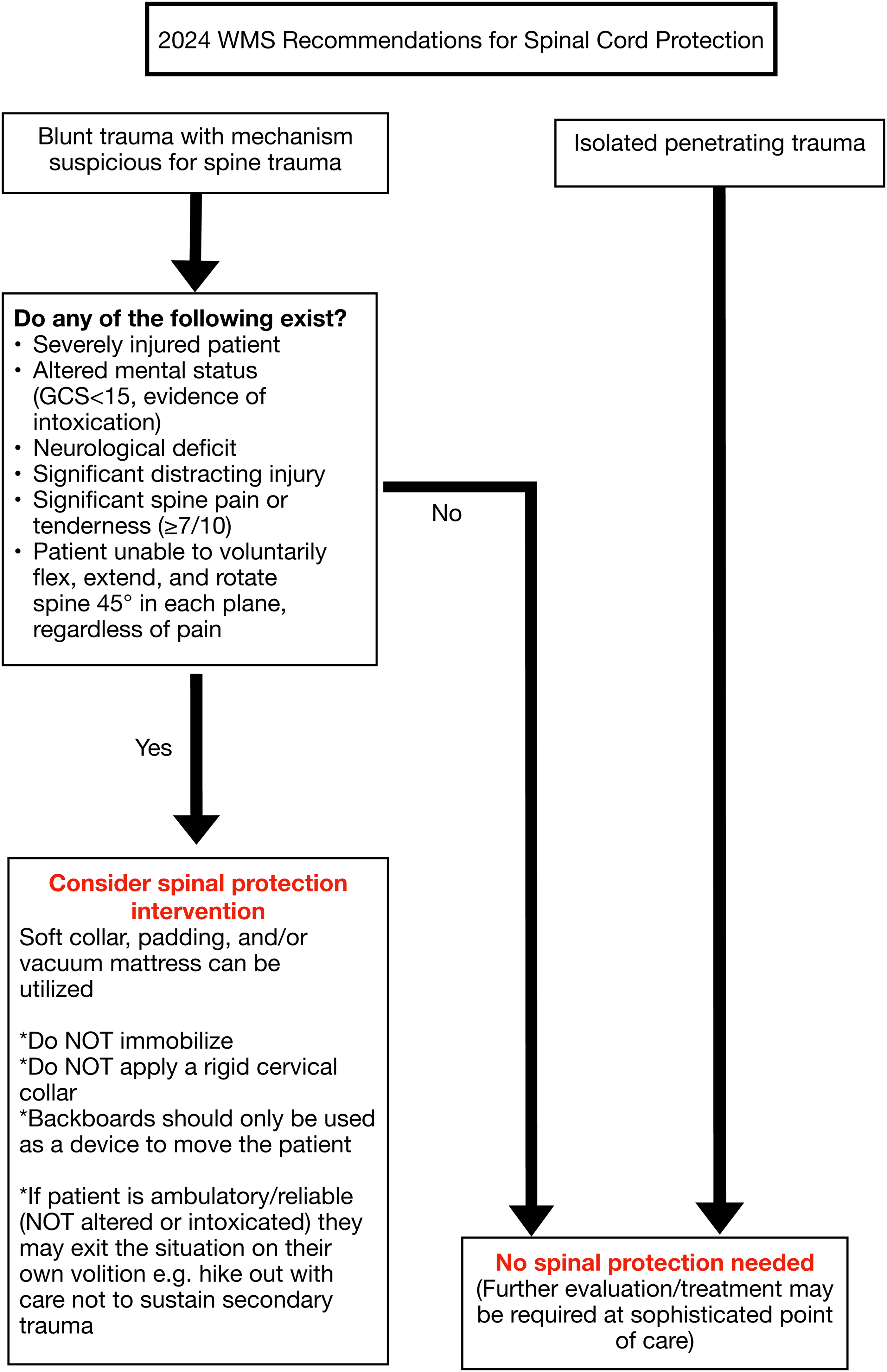
2024 WMS algorithm for spinal cord protection.
Conclusions
The scant and low quality of scientific evidence available does not support the current rationale for immobilizing a potential spine injury in the wilderness environment. The authors believe that a goal-oriented approach offers the best compromise between unnecessary immobilization and the risk of causing further damage in the presence of spinal injury. The goal-oriented approach would set SCP as the ultimate treatment goal. Although the best techniques to achieve this goal are not yet clear and require further research, current evidence suggests that SMR may be the most appropriate mechanism currently available. Current evidence also suggests that rigid immobilization via collar or backboard is not an effective or safe means to accomplish this goal and can result in a worse patient outcome in both blunt and penetrating trauma. Although these guidelines cover many of the relevant issues related to spine injury, questions remain that should serve as a focus for future research. We would suggest this research should be equally goal oriented and focus on the best techniques to prevent occurrence or exacerbation of spinal column or SCI and not spring from an a priori assumption that immobilization is necessary.
Supplemental Material
sj-pdf-1-wem-10.1177_10806032241227232 - Supplemental material for Wilderness Medical Society Clinical Practice Guidelines for Spinal Cord Protection: 2024 Update
Supplemental material, sj-pdf-1-wem-10.1177_10806032241227232 for Wilderness Medical Society Clinical Practice Guidelines for Spinal Cord Protection: 2024 Update by Seth C. Hawkins, Jason Williams, Brad L. Bennett, Arthur Islas and Robert Quinn in Wilderness & Environmental Medicine
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.