
Abstract
Introduction
To compare the effectiveness of a molded fleece jacket with that of a standard cervical collar at limiting movement of the cervical spine in 3 different directions.
Methods
This is a prospective study using 24 healthy volunteers to measure cervical flexion/extension, rotation, and lateral flexion with both the fleece collar and the standard cervical collar. A hand-held goniometer was used for measurements. The results were then analyzed for the 3 independent movements using a noninferiority test.
Results
The fleece collar was determined to be noninferior at limiting the designated motions. Comfort was greater while wearing the improvised fleece collar.
Conclusions
Our small study demonstrated that mountain travelers and rescuers may be able to use an improvised fleece jacket collar in place of a standard collar if spine trauma is suspected after a backcountry accident. Further research should examine different types of improvised collars, their ability to remain in place over extended evacuations, and when to apply collars to backcountry patients.
Introduction
In the backcountry, specific medical equipment and emergency medical services may not be readily available, posing obstacles in providing standard of care. These barriers are especially common for traumatic emergencies. Spinal cord injuries in the United States account for up to 3% of hospital trauma admissions per year. 1 The decision to apply spinal motion restriction in the wilderness and prehospital setting after a traumatic injury is determined by the mechanism of injury and clinical application rules. 1 Many prehospital providers apply the national emergency x-radiography utilization study (NEXUS) criteria, which determine that only patients with midline neck tenderness, focal neurologic deficits, altered mental status, intoxication, or a painful and distracting injury require radiographs to exclude spinal injury. 2 These patients are very unlikely have an injury and may not need spinal motion restriction. These principles have been studied in the prehospital environment and found to be safe and effective. 3
One study compared a structural aluminum malleable (SAM) splint-molded cervical collar as an improvised device for the backcountry with a standard Philadelphia cervical collar and found no statistical difference between the 2 devices. 4 Many times, neither a commercially made cervical collar (eg, Philadelphia collar) nor a SAM splint is available, and providers need to improvise and use equipment and techniques that are available. We identified a fleece jacket as an article of clothing that many backcountry participants carry on expeditions that could be used as an improvised collar. At least one wilderness first aid education company (Wilderness Medicine Institute of the National Outdoor Leadership School) teaches this method as an improvised cervical spine motion restriction technique. Our study compared the effectiveness of a fleece cervical collar versus a standard cervical collar at limiting movement of the cervical spine. We hypothesized that the backcountry fleece collar would provide noninferior cervical spine restriction while being more comfortable when applied.
Methods
We enrolled 24 healthy volunteers aged 25 to 45 y with no history of cervical spine problems or prior injury. Participants were fitted randomly with either the fleece jacket collar or the cervical collar while seated in the upright position. The fleece jacket collar was applied in the manner described in Figure 1, which parallels the method taught by Wilderness Medicine Institute of the National Outdoor Leadership School. The DeRoyal size-adjustable EMT Select Extrication Collar, adult size, was applied according to the instructions for the device. The DeRoyal collar was adjusted to fit neck size, and the participants were fitted as if they were being treated as a patient in the field.
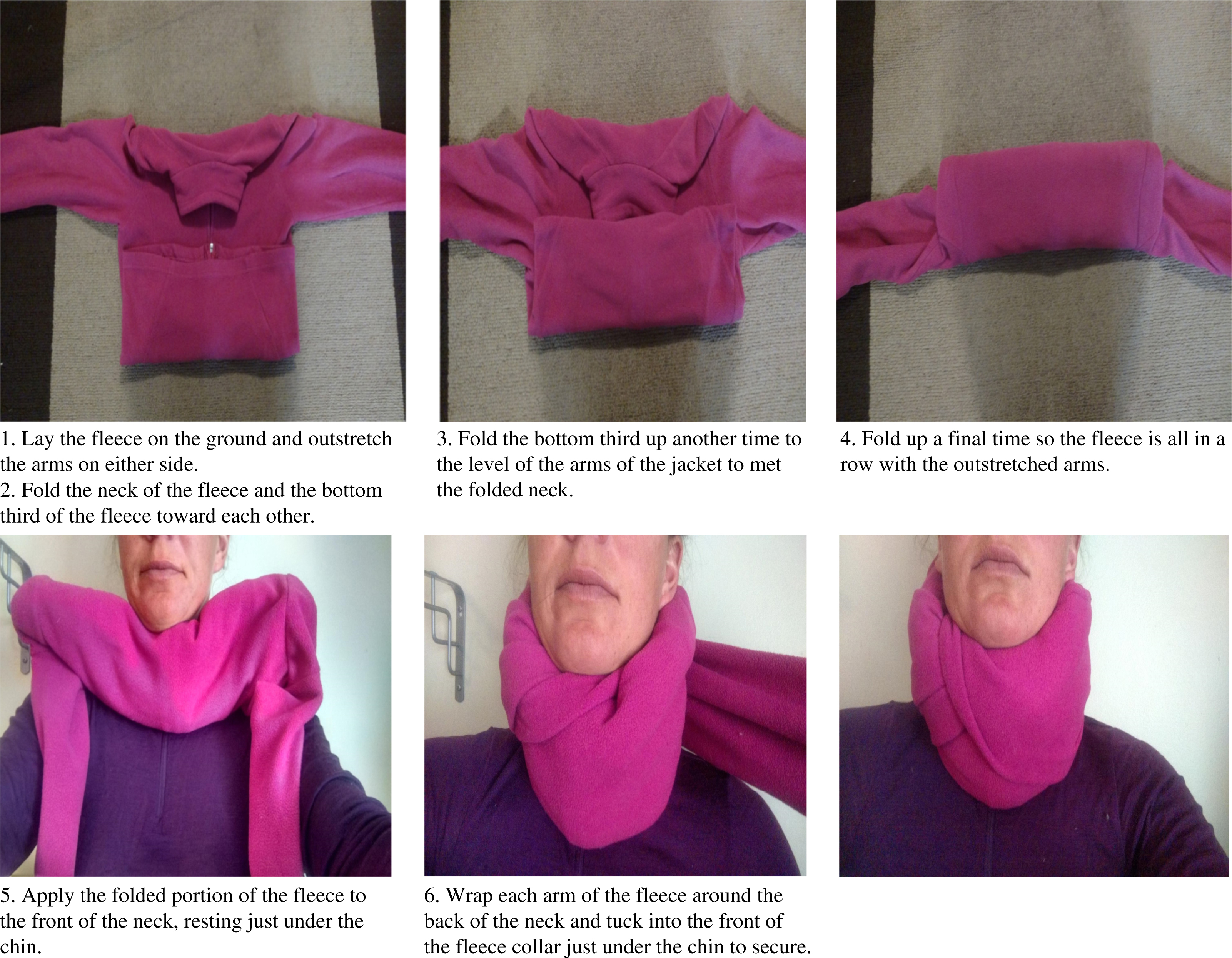
Application of the fleece cervical collar.
The patient started at a neutral position and facing forward. Using the handheld goniometer we were able to determine zero degrees and measured the degree of movement from there. Maximal flexion/extension, rotational movement, and lateral flexion were measured by the goniometer 3 times for each participant. Each movement value was averaged over 3 measurements. Data are presented as mean±SD.
Participants were given the following instructions: for flexion/extension and lateral, “let your head fall passively into these directions”; for rotation, “use gentle movements to rotate until passively stopped.” We instructed participants to use gravity to assist motions for which this was possible (flexion/extension and lateral) and instructed participants to actively assist in motions not affected by gravity (rotational). The same investigator (MD) performed all measurements to limit variations in technique and interpretation. The investigator followed measuring procedures described in Krusen’s Handbook of Physical Medicine and Rehabilitation 5 and underwent practice sessions overseen by members of the University of Utah Physical Therapy department.
A comfort level was recorded immediately after each collar was removed, with 1 = very comfortable, barely noticed; 2 = comfortable, noticed but not uncomfortable; 3 = moderately comfortable, noticed but not distressing; 4 = moderately uncomfortable, noticed and mildly distressing; 5 = very uncomfortable, intolerable. Subjects could not overhear answers given by other volunteers. Participants were then fitted with the other collar type and the procedures were again performed.
A linear regression analysis was used to compare cervical measurements for noninferiority. Based on estimated clinical differences and a previous study examining improvised spinal restriction, 4 we selected 10 degrees as the noninferiority margin. The actual number of degrees of motion restriction required for safe spinal restriction, however, is not known.
Comfort scores were evaluated using the Wilcoxon signed-rank test. This study was reviewed and approved by the University of Utah institutional review board.
Results
Comparisons of averaged measurements were nonsignificant (P > 0.05) across the 3 cervical motions, demonstrating noninferiority. Measurement results are shown in Table 1. Table 2 displays the statistical comparison between the collars. Figure 2 displays the movement averages via a box plot. The fleece collar was found to be more comfortable than the DeRoyal collar (P < 0.001) with an estimated difference in rankings of 1.5 (95% confidence interval, 1.5–2.0).
Cervical collar motion and comfort measurements
IQR, interquartile range; SD, standard deviation.
Comfort values measured on scale 1 to 5.
Statistical comparison of movements in each cervical collar
CI, confidence interval.
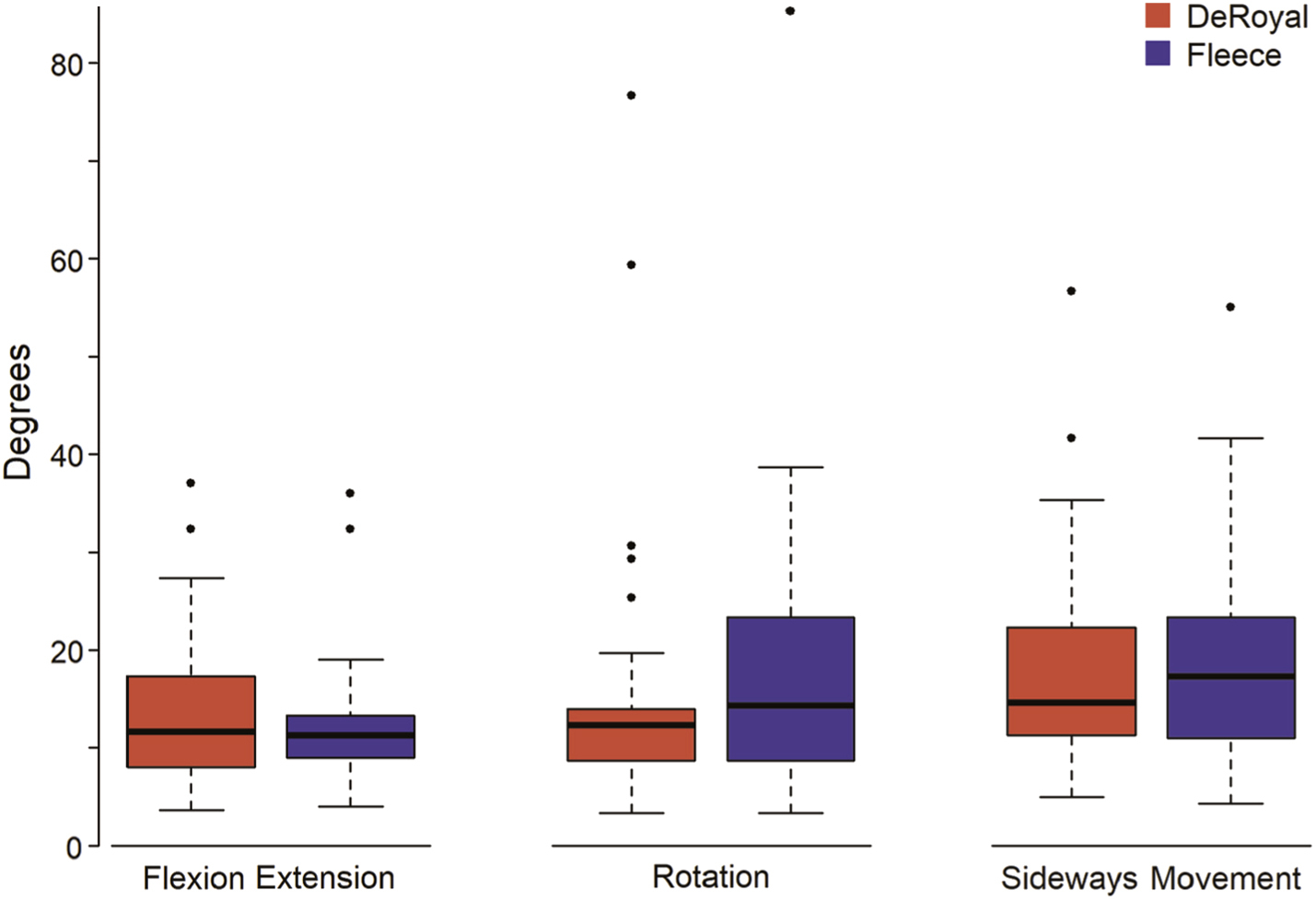
Comparison of movements of the cervical spine by type of collar.
Discussion
The results of our small study showed that the improvised fleece jacket cervical collar was noninferior to a commercial cervical collar in restricting cervical movement while also being more comfortable, thus confirming our hypothesis. This information gives backcountry travelers, search and rescue groups, and mountain medical providers evidence that an improvised fleece cervical collar could be used if a standard collar is not available in certain backcountry trauma cases.
Urban prehospital providers have historically placed trauma patients with mechanisms that could produce a spinal injury on a backboard with a rigid cervical collar. The Wilderness Medical Society guidelines for spine immobilization recommends immobilization of the spine if a victim has sustained “blunt trauma with mechanism suspicious for spine trauma and the patient is: severely injured, has altered mental status, neurological deficit, or other significant distracting injury, has significant spine pain, or not able to voluntarily flex, extend, and rotate the spine 30 degrees in each plane.” 1 These criteria are based on a number of other guidelines and have not been rigidly tested for sensitivity or specificity. The goal, historically, has been to attempt to immobilize the spine to prevent secondary injury.
The evidence for these prehospital spinal protection practices, however, is limited. 6 Over the last 5 to 10 y, the approach has evolved so that backboards may not be necessary for all trauma patients and that cervical collars can be selectively placed only on patients at higher risk of spinal injury. 7 Multiple studies have shown that backboards pressing against a supine patient can cause skin injury and back pain itself and can prompt medical providers to order unnecessary imaging. To mitigate these risks, vacuum mattresses are being used more in the back- and frontcountry settings. These devices reduce much of the pressure that backboards exert on the back and skin while providing extremity and cervical stabilization. Furthermore, the device can be carried more easily than a backboard, thereby facilitating extrication.
Similar to backboards, rigid cervical collars are being deemphasized in prehospital care. They can impede access to the neck when providing airway management, increase intracranial pressure, and be restrictive if the patient has anxiety or respiratory difficulties. 8 –10 The term “spinal motion restriction” is now preferred over immobilization because we recognize that immobilizing the spine is not practically possible and that restricting motion will likely accomplish the same purpose.
When in the backcountry, placing a trauma patient on a backboard and applying a cervical collar necessarily demands that the evacuation be accomplished by a helicopter or team carry out. If a patient needs to be carried out by a large rescue team, the speed of rescue is slower once the patient is committed to spinal motion restriction. Therefore, methods to decrease the use of and revise protocols toward backboard and rigid spinal restriction are advantageous in the backcountry.
Backcountry trauma patients who do not meet the NEXUS criteria should have their spinal motion restricted. Most backcountry travelers carry a minimal first aid kit that usually does not include spine motion restriction devices. If confronted with a trauma situation in the backcountry, we recommend following the Wilderness Medical Society spine guidelines and NEXUS criteria to determine whether and what type of spinal motion restriction is warranted. Data from our small study show that the improvised cervical collar may provide adequate motion restriction for backcountry trauma purposes.
Limitations
This study was applied to a small group of healthy volunteers without prior injuries, and results may not be generalizable to a wider population with true injuries. One investigator performed goniometry measurements; 2 or more investigator measurements would have potentially decreased bias by adding an interrelater reliability measurement. We do not have baseline measurements without cervical collars applied. Two different providers applied the cervical collars, which could have introduced bias in collar application. The structure of the fleece cervical collar could have had variability due to the application process and density of material. Many types of fleece jackets are worn in the backcountry, and we focused on one particular brand. Additional studies would need to be performed to test the efficacy of other jackets that might be worn in the backcountry. The investigators were not blinded to the results of the study. We performed the measurements in the upright seated position for the best readings of the goniometer and to parallel a previous study on this topic, but we recognize that this method does not measure collar use in other conditions, such as supine positioning. A patient with a head injury could be agitated and thus actively moving the head, which was not tested by passive movements for flexion/extension and lateral movements.
Conclusions
In the backcountry, lack of access to common medical equipment may challenge rescuers and medical providers to improvise. Unstable spinal trauma is an uncommon but potentially consequential injury. An improvised fleece jacket cervical collar may be able to be used as a substitute for a commercial cervical collar in these scenarios. Further studies will need to be performed to assess different providers’ ability to apply the improvised collar as well as its ability to remain in place over a prolonged rescue.
Footnotes
Acknowledgments
We thank the University of Utah Physical Therapy department for assistance as well as the study subjects for their time and efforts.
Author Contributions
SM conceived the study. AP, MD, SS, and LH, and SM designed the study, collected and analyzed data, and contributed to writing and reviewing the manuscript.
Financial/Material Support
None.
Disclosures
The investigators have no financial or other interest in the manufacturer of devices used in this study.
Presented in abstract form at the Wilderness Medical Society Summer Conference, Midway, UT, August 2018.