
Abstract
Wild boar–inflicted nerve injuries have been very rarely reported in the literature. A 62-year-old man was attacked by a wild boar in eastern Turkey and brought to the emergency department. He had 5 lacerations on the lower extremities and 2 on the posterior thoracic region. In addition to soft tissue lacerations, he sustained a complete laceration of the left common peroneal nerve with a foot drop. The common peroneal nerve was repaired primarily the day after the attack. The patient was discharged after a short hospital stay without any immediate complications; however, at the 10-mo follow-up, he still had a left foot drop.
Introduction
The wild boar is a mammal with a widespread distribution in Eurasia. 1 There are several subspecies of wild boars, and Sus scorofa lybica is the subspecies found in Turkey. 2 Wild boars may be up to 1 m in height, up to 1.8 m in length, and 200 kg in weight. 3 They can run up to 40 km/h and can jump up to 1 m. 1 The male wild boars have very sharp lower tusks that can reach up to 6–10 cm in length.1–3 The interaction between wild boars and humans has been increasing due to the intrusion of humans into wildlife areas and the increasing population of wild boars over the last 30 y in Asia, America, and Europe.1,2 Wild boars may attack humans, which can lead to life- or limb-threatening injuries.3,4 Wild boar attacks on humans may be unprovoked or a result of a human encountering a wounded or threatened boar (such as during hunting). 5 Wild boar attacks occur more frequently in the winter due to rutting season and in mid-morning between 0900 and 1100. 5
In the literature, there are limited cases of nerve injuries due to wild boar attacks.1–3,6–10 Previous studies have described femoral, sciatic, and tibial nerve injuries.1,6,10 In the current case report, we describe a wild boar attack that led to a common peroneal nerve laceration and subsequent foot drop.
Case Report
A 62-year-old man was brought to the emergency department (ED) of Turgut Ozal Medical Center, unconscious, following a wild boar attack in December at 1930. According to the son of the patient, the patient had gone for a walk in a rural area around 1030 on the day of the attack. Since the patient hadn’t come back from his walk by the end of the day, his family went searching for him. The patient was found by family members around 1800. He was found unconscious and with numerous skin lacerations noted on the posterior aspect of his body. The family members called an ambulance to the field, and the patient was directly transferred from the field to our hospital. On the way to the hospital, intravenous fluids were administered, and compression was applied to the wounds.
Upon arrival, the patient was unconscious and hypothermic (34 °C), blood pressure was 100/60 mm Hg, and hemoglobin level was 11.9 g/dL. On physical examination, the patient was noted to have 2 lacerations on his back at the level of both scapulae (4 and 10 cm long, respectively), 2 lacerations on the posterior and posteromedial aspect of the left thigh (8 and 15 cm long, respectively), 1 laceration (8 cm long) in the left popliteal region, and 2 lacerations (4 cm long) in the rural areas bilaterally (Figure 1). No vascular injuries were noted upon initial examination. A full neurological exam could not be performed as the patient was unconscious.
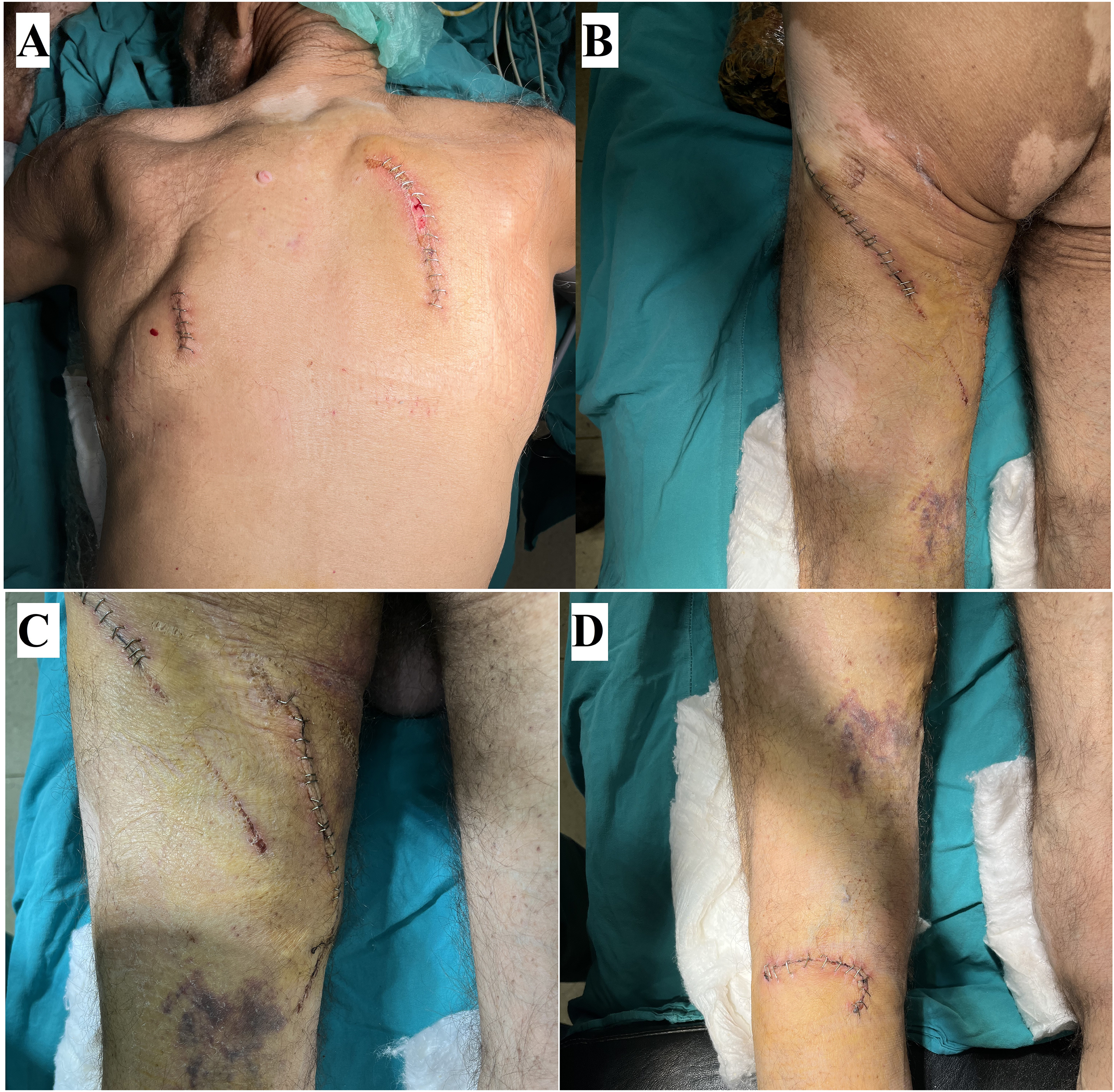
Sutured wounds of the patient. A, Posterior thoracic region. B, Posterior thigh. C, Posteromedial thigh. D, Popliteal region.
Initial investigations, including x-rays and computed tomography scans, were performed and showed left-sided 4th, 5th, and 6th rib fractures and a left hemopneumothorax (Figure 2). Immediate treatment in the ED included chest tube thoracostomy, wound irrigation with saline, wound closure with sutures, (intravenous) antibiotic treatment (cefazolin 1 g × 3 doses, gentamicin 160 mg × 1 dose, and metronidazole 500 mg × 3 doses), tetanus, and rabies prophylaxis. The patient was heated with a patient warmer and was hospitalized in the orthopedic ward.
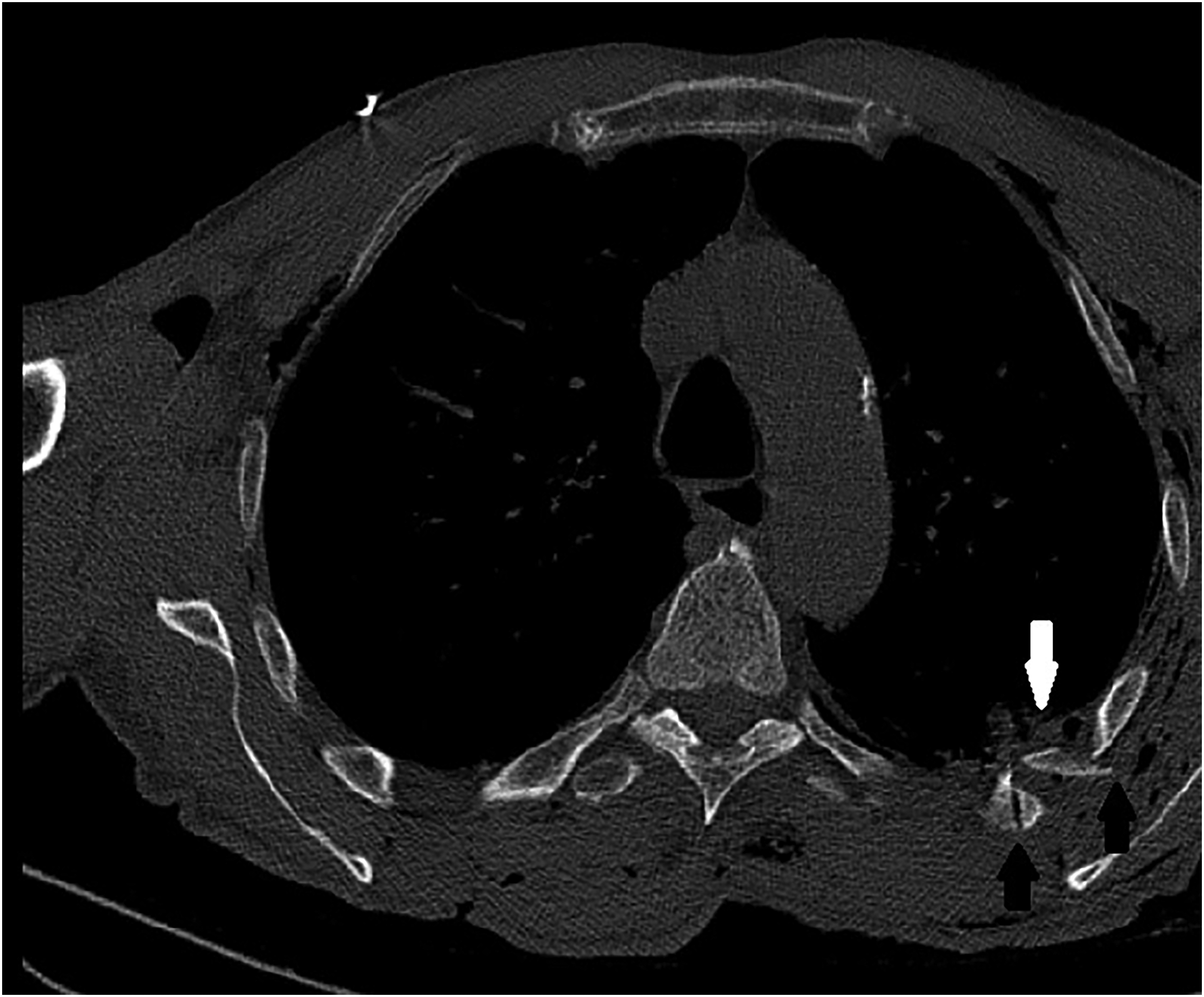
Computed tomography slide showing left side hemopneumothorax (white arrow) and left 5th and 6th rib fracture (black arrows).
The following day, the patient had regained consciousness, and a more detailed physical exam could be conducted. A left foot drop was noted at that time. Surgical exploration was therefore organized and conducted the same day to look for a potential nerve injury. The patient was operated on under general anesthesia in the prone position. The wounds of the proximal thigh and popliteal region were explored. The sciatic nerve was found to be intact, and the hamstring muscles were partially ruptured (Figure 3). The left common peroneal nerve and lateral head of the left gastrocnemius were found to be completely ruptured (Figure 4). A primary repair of the left common peroneal nerve, left lateral gastrocnemius tendon, and left hamstring muscles was done under loop magnification. The wounds were sutured in standard fashion. A knee brace and drop foot orthosis were applied. The chest tube was removed 2 days after surgery. The patient was discharged on the 5th postoperative day without any immediate complications.
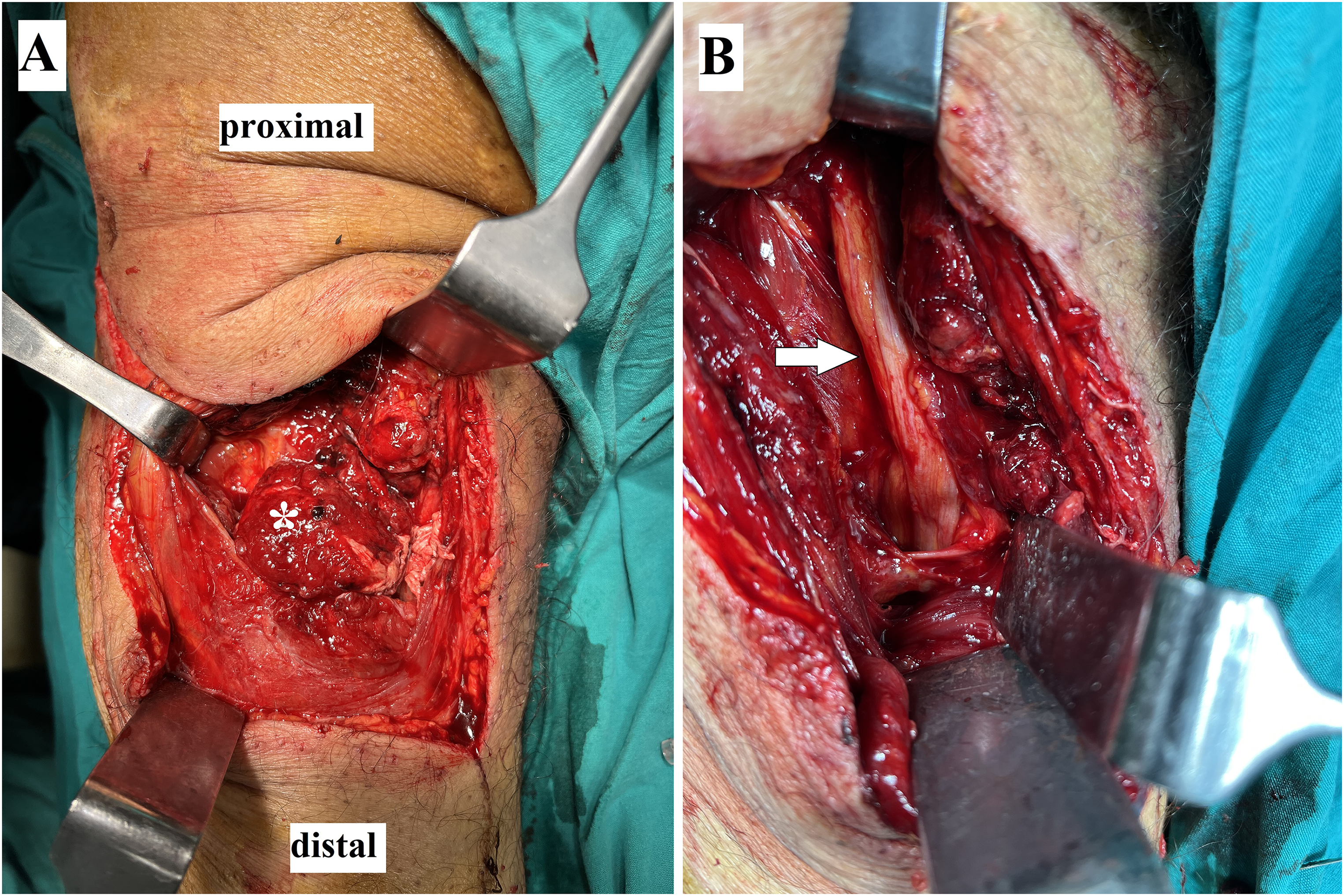
A, Partially ruptured hamstring muscles (*). B, Uninjured sciatic nerve (white arrow).
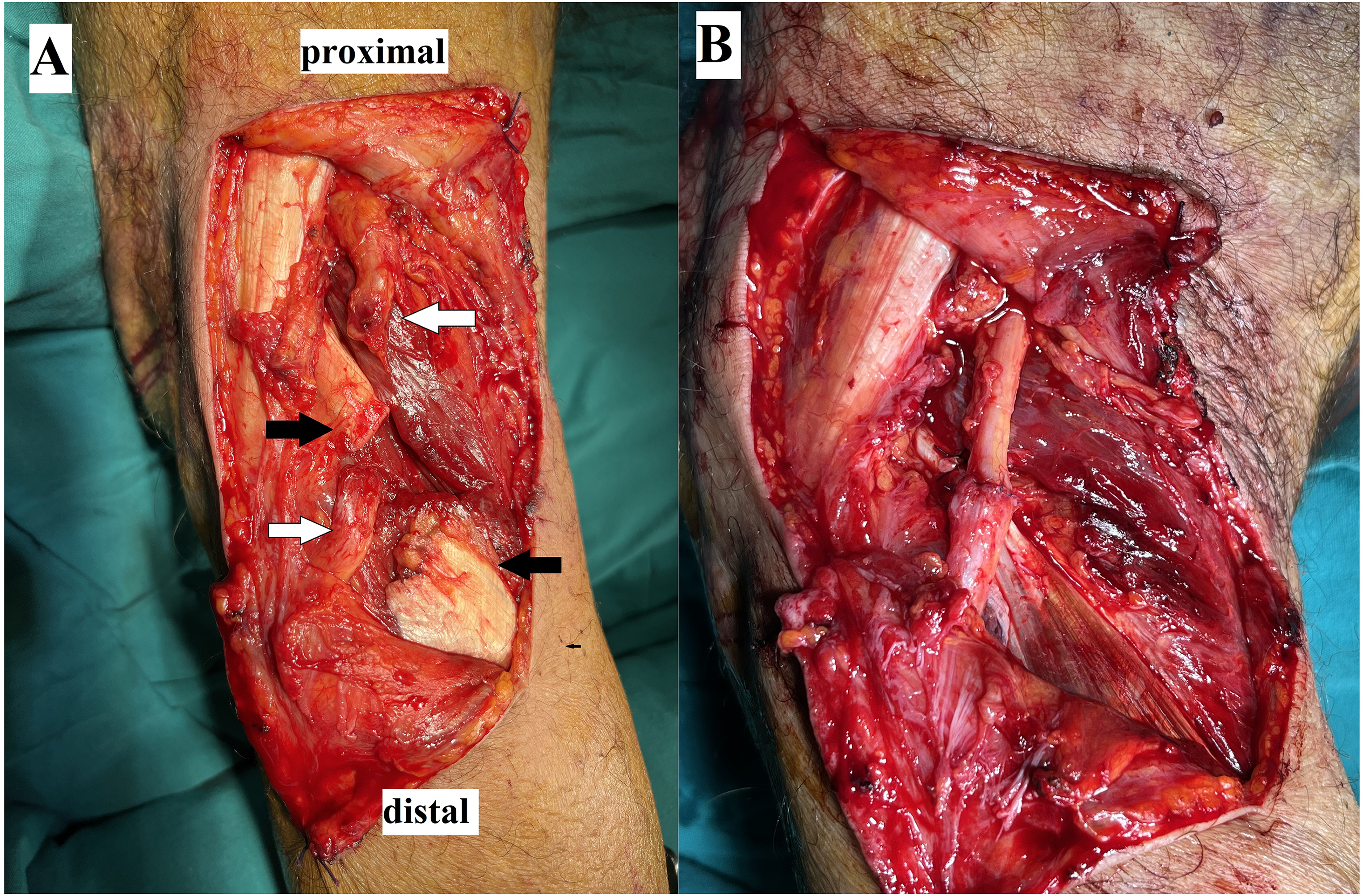
A, Proximal end distal ends of totally ruptured common peroneal nerve (white arrows) and lateral head of the gastrocnemius muscle (black arrows). B, After primary repair.
Postsurgical follow-up included removal of sutures at 2 wk post-op and initiation of passive range of motion exercises at 3 wk post-op. The patient moved to another city because our city was affected by the earthquakes in February 2023. We contacted the patient via phone. He reported no wound complications or infections during follow-up. At 10 mo follow-up, the patient still had a drop foot and was using a drop-foot orthosis.
Discussion
While wild boar attacks are rare incidents, nerve injuries caused by wild boar attacks are even less frequent. The posterior aspect of the lower extremities is the most commonly reported injury side.6,11,12 Facial, upper extremity, and perineal injuries have also been reported.1,7,8,12 The most common injury type is soft tissue lacerations.6,11,12 Nerve injuries caused by wild boar attacks have been very rarely reported.1,6,10 To the best of our knowledge, our case is the first reported case of common peroneal nerve injury caused by a wild boar attack in the literature.
In our case, the patient was attacked in the morning in December. Winter is the season when wild boar attacks have been most commonly reported.2,5,11 Winter is the rutting season of wild boars, and they are more aggressive during rutting, 5 and midmorning (9:00-11:00) is the most commonly reported time of attack.6–10,12,13 Wild boars are normally more active at night than in the daytime. 5 It has been claimed that human activities such as disturbing a boar's bedding sites or hunting during the daytime may be the main cause of wild boar attacks.5,6
The victims of wild boar attacks frequently suffer from soft tissue lacerations of the posterior thigh.2,5,6,11 Considering the size of a wild boar and a human's common reaction of running away from the animal, the injury site is logical. After the first attack, the victim typically falls to the ground, and the wild boar attacks repeatedly, which causes additional injuries2,11 Maxillofacial, rectal, abdominal, thoracic, hand, and wrist injuries are probably caused by these secondary attacks.1,2,7,8,11 Our patient had 5 lacerations on the lower extremities and 2 on the posterior thoracic region. Although soft tissue lacerations have been reported as the most common injuries due to wild boar attacks, big tusks of the wild boar may also cause fatal injuries.10,14,15 Fatal injuries as a result of wild boar attacks have been rarely reported in the medical literature; however, some deaths inflicted by wild boars have been documented in the news and magazines.11,16 Abdominal, cranial, and femoral artery injuries have been previously documented as the cause of death.10,14,15 Our patient did not have a fatal injury, but the attack left him unable to move, and he was hypothermic, which could have led to death had he not been found.
To the best of our knowledge, there have been only 3 nerve injuries documented in the literature from wild boars. Tumram et al detected a femoral nerve injury concomitant to femoral artery injury during the autopsy of a victim killed by a wild boar. 10 Sprem et al detected a tibial nerve injury by electromyoneurogram 2 mo after a wild boar attack on a hunter. 6 They did not notice nerve injury during initial wound exposure. Okano et al reported a partial sciatic nerve concomitant with anorectal injury. 1 They repaired the nerve primarily. In our case, we detected a drop foot at the second look, and we explored the wounds at the thigh and popliteal region, detected a total rupture of the common peroneal nerve, and repaired primarily under loop magnification.
After a wild boar attack, the wound should be irrigated and cleaned carefully. The wound can be closed primarily. However, if there is any suspicion of high contamination, delayed closure should be considered. 11 Antibiotic treatment should also be added as wild boars and domestic pigs may harbor many infectious pathogens.2,5,11 Combination of amoxicillin-clavulanic acid is the recommended first-line antibiotic treatment. 6 Tetanus prophylaxis should be administered if the patient has not received a booster recently. Additionally, a rabies vaccine should also be administered.2,12
Acute nerve injuries should be repaired when detected. In open injuries, it has been recommended to repair in the first 72 h, if possible. 17 If the primary repair is not possible due to a gap between nerve ends, nerve grafting (commonly using the sural nerve autograft) is indicated. In the literature, good results after primary repair, if performed within 6 mo, have been reported in 44% of cases. 18 Tendon transfer may be used if the drop foot persists 1 year after repair. 17 In such a case, the tibialis posterior tendon can be transferred to cuboid or cuneiform. In our case, we repaired the nerve the day after the injury, and the drop foot persisted in 10 mo follow-up.
Conclusions
Wild boar attacks are rarely seen but may cause very serious damage and even death. Due to the increasing population and shrinkage of their natural habitat, the number of wild boar–inflicted injuries is likely to increase. Careful examination and management of these injuries should be performed to detect any associated injuries, such as nerve lacerations. The second look examination should be kept in mind if the patient is not well-oriented during the initial examination.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.