
Abstract
A central mission of a healthcare organization is to provide equal access and excellent health outcomes to all populations, regardless of race and ethnicity. However, in the everyday practice of healthcare, organizations have fallen short of this primary tenant. Healthcare disparities in the Black community are well-documented in the literature. Although the reasons are multi-faceted, racial bias contributes to healthcare disparities, and eliminating those disparities should be a chief focus in improving the health and well-being of every community. This paper discusses healthcare disparities in the Black community and the complex cycle that enables gaps to persist despite best efforts among healthcare professionals, policymakers, and the general public. It concludes with a presentation of the Looking Glass Framework; an innovative onboarding and continuing education program using virtual reality and computer-based educational modules to reduce healthcare disparities within clinics, hospitals, and health systems.
Points for Practitioners
Persistent healthcare disparities are the result of a complex cycle of interrelated factors that lead to unequal treatment.
Implicit bias can negatively impact the patient-physician relationship, leading to low-quality clinical interactions and decision-making, reactive patient behavior, and ultimately, healthcare disparities.
Medical practitioner partnership is essential; The patient-physician relationship is a key lever that can either help to reduce or increase poorer outcomes in the Black community.
The Looking Glass Framework interrupts the disparity-producing cycle by leveraging perspective-taking, an effective strategy to reduce implicit bias.
Current State of Healthcare Disparities
Healthcare disparities in racial and ethnic minority populations are central issues in local, regional, and national conversation. Congress has long recognized the issue, which prompted the request for a study by the Institute of Medicine (IOM) to assess and evaluate healthcare in the United States. The result was Unequal Treatment, the landmark report from the IOM which concluded that most evidence shows healthcare disparities exist and remain persistent, even when socioeconomic and access-related factors are accounted for. Further, this report suggests that provider stereotyping and bias leads to the unequal treatment which helps enable health disparities to occur (Institute of Medicine [US] Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, 2003). Supporting these findings, a systemic review by Hall et al. (2015) suggests implicit racial bias is a contributing factor that affects clinician behavior and contributes to health disparities in minorities.
Since 2003, Congress has mandated the National Healthcare Quality and Disparities Report (NHQDR). The NHQDR, produced by the Agency for Healthcare Research and Quality, provides an annual snapshot of healthcare disparities in the system of care in the United States. It assesses how well the healthcare delivery system provides equitable, high-quality care to Americans using dimensions of race, ethnicity, and other demographic categorizations. The 2022 report highlights trends of disparities for minority populations and found stark differences in the Black population compared to Whites. The 2022 NHQDR reported that Black people received worse care compared to White people for 45% of quality measures and that disparities between Black people and White people improved for 7% of measures and worsened for another 7% of measures which demonstrates no net improvement (Boonyasai et al., 2022).
Cleary, healthcare disparities in the Black population highlight that healthcare in its current state is still not equitable. In part, because of the impacts of implicit bias on provider behavior and its intersection with patient reactions and health decisions. But how does this intersection perpetuate healthcare disparities? This paper describes the disparity-producing system (Figure 1) wherein provider implicit bias leads to poorer patient-provider relationships turning into poor clinical interactions and reactive patient behaviors. The results are persistent healthcare disparities.
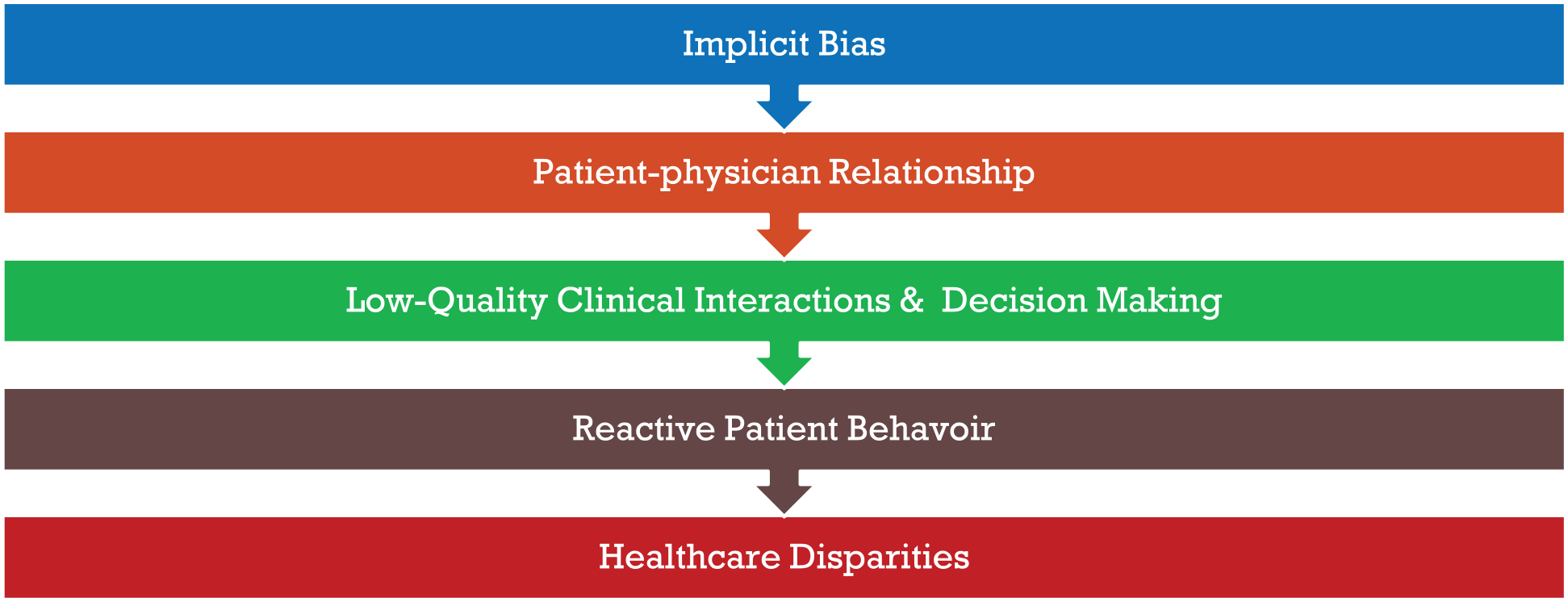
Structure of the disparity-producing system of healthcare.
Patient-Physician Relationship
The patient-physician relationship is a vital driver of quality healthcare to all communities. The four elements of the noted relationship are knowledge, trust, loyalty, and regard (Chipidza et al., 2015; Ridd et al., 2009). When these four elements exist in high-quality, the result is a strong patient-physician relationship. More specifically, strong patient-physician relationships are necessary for the prevention, diagnosis, and treatment of diseases. Further, high-quality patient-physician relationships are associated with better health and lower quality patient-physician relationships are associated with poorer health (Olaisen et al., 2020). Concrete examples of how this relationship may affect health outcomes for patients are represented in the literature (Saluja & Bryant, 2021). A cross-sectional study examined patient trust and medication adherence regarding racial associations and blood pressure control among 723 hypertensive African American and White patients at 119 primary care clinics. Researchers found that medication adherence and blood pressure control were associated with high levels of trust (Schoenthaler et al., 2014). A different analysis involving 16 primary care practices on patient engagement and patient-reported outcomes showed patient-centered culture was associated with fewer depression symptoms for Diabetic and Cardiovascular Disease patients (Shortell et al., 2017).
Conversely to positive impact, elements that negatively impact the patient-physician relationship can have undesirable effects. One important factor that negatively impacts the patient-physician relationship is implicit bias. Implicit bias occurs unconsciously and shapes the decisions physicians make regarding patient care. This type of bias develops from an early age due to experiences in society that reinforce stereotypes. Of note, the way in which physicians are trained in medicine also reinforces commonly held biases about minorities. Medical training focuses on population and group factors, which can cause repeated exposure to minorities in poor circumstances. Repeated exposure may help to reinforce negative stereotypes about a particular group or population (Chapman et al., 2013).
In cases where providers have bias toward patient groups, the result may be low-quality patient-physician relationships. The correlation between clinical outcomes and provider bias reveals poorer patient outcomes in a cause-and-effect manner. Providers are unaware of their implicit bias, but it may present itself in relationship attributes such as poor communication. For example, poor communication may lead to a provider taking an incomplete history or result in a patient that doesn’t understand the ramifications of their medical diagnosis, which can lead to a medical adherence issue (Blair et al., 2013).
Negative Consequences of Bias
Bias in healthcare interactions leads to poor consequences for patients and families. A 2016 study examined the effect of physician implicit bias on patient communication. The research included 18 non-black oncologists and 112 Black patients with cancer. Oncologists completed a baseline assessment of their implicit bias using the Implicit Association Test (IAT), which is a widely used instrument to measure implicit racial bias. Researchers video recorded patient meetings with their assigned oncologist to discuss cancer treatment. This interaction was the first to discuss cancer treatment options, and patients never previously met with the assigned oncologist. After the interactions with the oncologists, patients answered questions regarding their perceptions of the interactions, including recommended treatment options. Four people watched the recorded patient interactions and rated the oncologists in the following three categories: informativeness, supportiveness, and partnership-building. Finally, the study conducted follow up interviews with patients after the initial post-interaction interview (Penner et al., 2016).
The results of the research showed some troubling aspects of racially discordant patient-physician interactions. Oncologists, who scored higher in implicit bias, had shorter lengths of time in their patient interactions, and lower levels of patient confidence in recommended treatments. They were also associated with patients believing there was more difficulty in completing treatments. Patients who met with the higher scoring oncologists with greater implicit bias scores reported that they had enhanced difficulty remembering the conversations. In addition, observers who viewed the interaction videos reported that oncologists with higher levels of implicit bias had lower quality communication with Black patients. The researchers concluded that implicit bias of oncologists is a likely source of disparities. This occurs because the patient-physician interactions of those higher in implicit bias are associated with factors that affect communication and patient-centeredness. The negative impact of these interactions and communications unwittingly falls upon the patient leading to less understanding, less time with the oncologist, less confidence in treatment, and less confidence in the patient’s ability to complete treatment (Penner et al., 2016).
Further, a different study examined data to determine if Black death rates due to circulatory disease were related to the bias of White clinicians. Data analyzed in this study indicated that health disparities in communities with circulatory-disease related death are higher in areas where Whites have more explicit bias (Leitner et al., 2016).
Combating Racial Bias
Reducing healthcare disparities in minorities requires both an identification of the root cause and a solution that addresses the issue directly. Past research in this arena indicates that perspective-taking could be a useful strategy to combat expressions of racial bias (Galinsky & Moskowitz, 2000; Shih et al., 2009; Todd et al., 2011). Perspective-taking is the conscious action of thinking about how other people experience and feel in a particular situation. Indeed, five experiments assessed whether perspective-taking weakens automatic expressions of racial bias. Researchers asked participants to take the perspective of White individuals or Black individuals in different scenarios of everyday life. In one of the experiments, participants watched a video of discriminatory acts that occurred to a Black man (Glen) verses what happened to a White man in the same situation. The perspective-taking videos revealed the two different ways the men were treated in scenarios such as shopping at a department store, purchasing an automobile, and interacting with police. The study divided participants into three groups: perspective-taking other (visualized what Glen was thinking, feeling, and experiencing), perspective-taking self (imagine what they would think, feel, and experience if they were Glen), and objective-focus (remain objective and emotionally detached). The research used the IAT to gauge the level of racial implicit bias. The outcome of the study showed that the two groups who adopted the perspective of the Black man scored lower on the IAT. Researchers concluded that perspective-taking caused significantly reduced pro-white bias (Todd et al., 2011).
Virtual Reality and Video Gaming Solution
A hallmark of the U.S. healthcare system is the innovative use of technology to solve real-world problems that contribute to better health outcomes for patients. A study conducted at the University of Wisconsin-Madison examined whether perspective-taking activities in a video game will increase empathy and reduce implicit bias. Researchers created a game called “Fair Play,” where the main character, Jamal Davis, is a Black graduate student at a predominantly White college. Players experience typical academic challenges and encounter implicit racial bias in situations from Jamal’s perspective. Events included choosing a college advisor, defending yourself against accusations of plagiarism, being asked to be the voice of all black students (tokenism), and scenarios where the player is mistaken for a caterer. When the player encounters instances of implicit racial bias, an alert appears indicating the presence of bias, definition of bias, specific type, and other pertinent information (Gutierrez et al., 2014). The study participants were 125 non-black college students, who were 82% White, and randomized into two groups. The first group played the “Fair Play” game, while the second group saw images and read a narrative text with the same scenarios as the game. Following the experiment, participants completed the IAT and a survey that measured bias awareness, empathy, and perspective-taking. The results of the study showed that players with a high level of empathy had the least implicit bias. These findings support prior research that indicates perspective-taking creates higher empathy levels, which reduces implicit bias (Gutierrez et al., 2014).
A separate study conducted at the University of Barcelona investigated whether immersive virtual reality (VR) can change implicit attitudes of interpersonal groups. The study randomly distributed 60 light-skinned Spanish women into four groups: Embodied-Light-Skinned (EL), Embodied-Dark-Skinned (ED), Non-Embodied Dark-Skinned (ND), and Embodied-Alien-Skinned (EA). Prior to the experiment, participants completed an IAT for a baseline measurement of implicit bias. The participants wore a head-mounted display (HMD) and a body-tracking suit. The immersive virtual reality equipment caused the virtual bodies to move in response to the participant’s own body movements. Participants saw their virtual body in a mirror as part of the simulation. Additionally, they saw their virtual body and virtual body skin color when they moved their heads in the VR environment. The simulation lasted for about 11.5 minutes and involved activities to reinforce embodiment through the exploration of the VR environment. Following the experiment, participants completed another IAT, but while still wearing the HMD. They also completed a survey about the overall experience. At the conclusion of the research, light-skinned participants in the ED group showed a reduction in implicit bias compared to the other groups (Peck et al., 2013).
Research in the utilization of perspective-taking in conjunction with VR and video games provides an innovative solution to reducing racial bias. Healthcare systems can improve healthcare disparities by using perspective-taking technologies to lower levels of implicit bias in providers, which is a key root cause for persistent healthcare inequities in the Black population.
Looking Glass Framework
The healthcare industry and healthcare organizations need a solution to the core problem of healthcare disparities. This paper suggests understanding healthcare disparities lies within synthesizing the findings described earlier:
Healthcare disparities in the Black population (and others) exist and are persistent, even when accounting for factors like socioeconomic status.
Provider stereotypes and bias contribute to unequal treatment that creates healthcare disparities.
The patient-physician relationship drives health outcomes: both positively and negatively.
Low-quality patient-physician relationships negatively impact clinical decision-making and patient behavior, potentially leading to healthcare disparities.
This paper further hypothesizes that using this synthesized knowledge, the healthcare industry can interrupt this disparity-producing cycle. The author proposes an innovative framework, the Looking Glass Framework (LGF), that is designed to rewrite the existing cycle of healthcare disparities. The LGF interrupts the disparity-producing system (Figure 1) by using a series of steps that focus on how perspective-taking simulations lower levels of implicit bias. First, providers complete perspective-taking training where they take the viewpoint of Black patients and community members in specific healthcare-related scenarios. Second, this participation lowers the levels of implicit bias toward the group of interest (Blacks and African Americans), which, thirdly, leads to higher-quality patient interactions and relationships. Lower levels of implicit bias reduce the poor clinical decision-making that would be impacted by implicit bias. Since the patient-physician relationship and interactions have less bias, the patient reactivity to the relationship and interactions with the provider are more aligned with desirable traits to manage health conditions (such as medication adherence and belief that the patient can complete treatment). Finally, the domino effect of the LGF’s steps results in reduced healthcare disparities. The LGF, which is pictured below (Figure 2) disrupts the destructive disparity-producing system of healthcare and replaces it with a framework that promotes equity and reduces healthcare disparities.
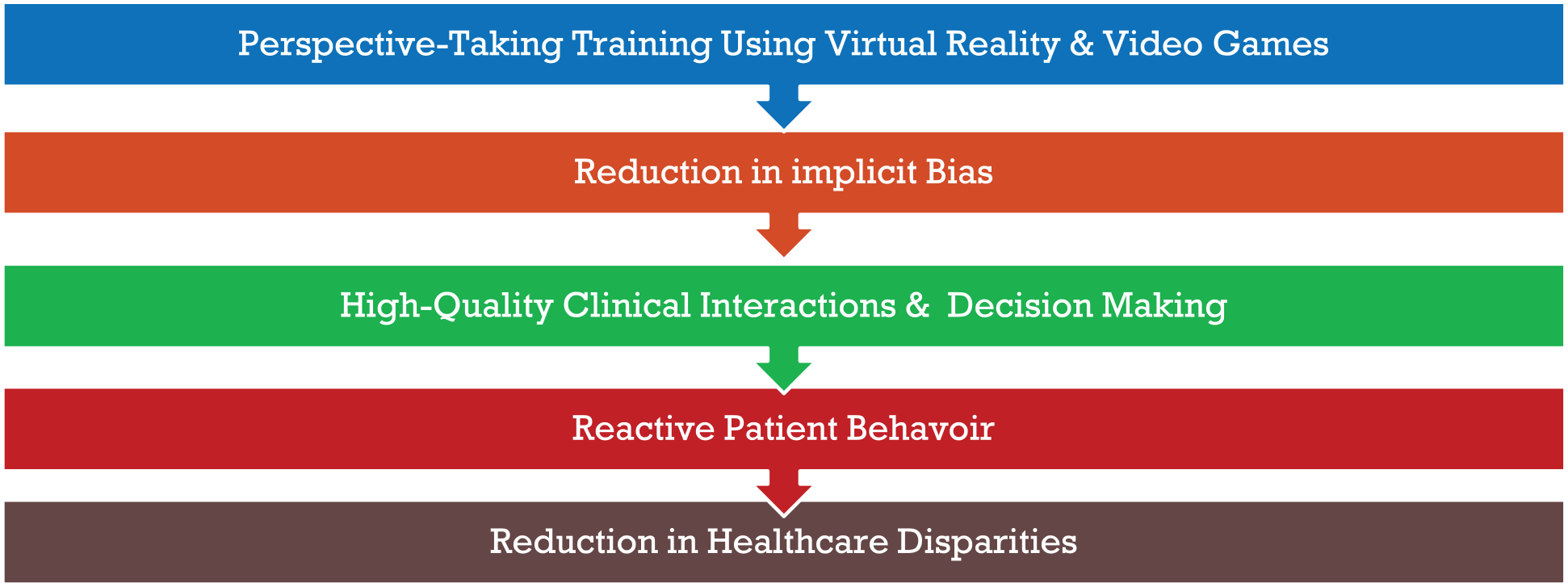
The Looking Glass Framework to reduce healthcare disparities.
There are four primary aims (Figure 3) within the blueprint of the LGF that include education, influence, cultural competency, and inclusivity. The first aim is to educate healthcare professionals about implicit racial bias. The second aim is to positively influence clinical decisions via the implicit bias reduction training. The third aim is to increase cultural competency in providers and other healthcare professionals. The fourth and final aim is to help foster a positive environment to further values of diversity, equity, and inclusion in the healthcare industry.
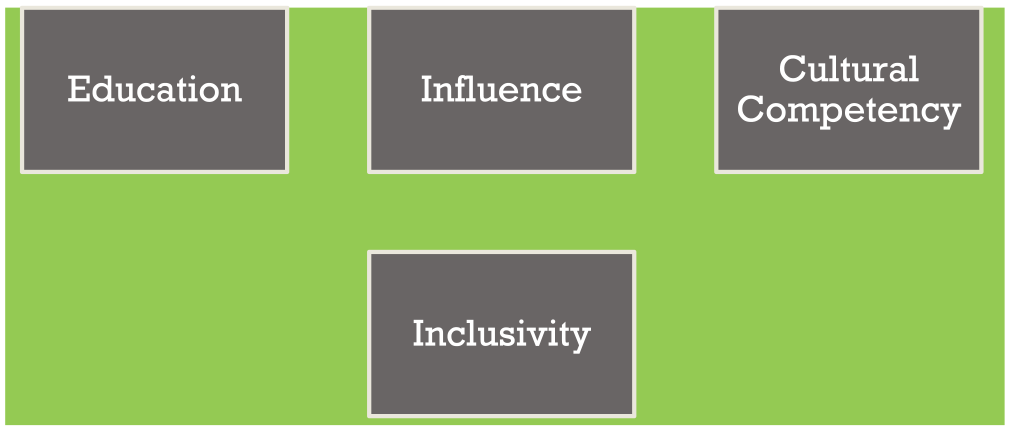
The four aims of the Looking Glass Framework.
The LGF achieves its four aims by the implementation of VR and video game educational modules at four distinct stages: medical resident education, the credentialing process for physicians, initial onboarding for all employees, and annual recertification. Targeting these four specific items will ensure that healthcare organizations do not miss opportunities to impact healthcare disparities within their facilities.
The LGF training uses perspective-taking simulations where the user embodies an African American named Jasmin. The player navigates through a multitude of healthcare scenarios as Jasmin. The simulations will include the following interactions: primary care office visit, specialist office visit, inpatient hospitalization, food service interactions, and registration. In addition to the healthcare-specific simulations, the player is exposed to Jasmin’s backstory and family history to humanize the experience. Simulations are based on the job description, enabling every role of a healthcare organization to have job-specific training to reduce implicit bias.
The LGF provides executives, healthcare professionals, and policymakers with a new roadmap to proactively address this issue within their communities utilizing an integrated technology and cognitive approach. At its core, the LGF is about repairing the patient-physician relationship, which this paper hypothesizes is a primary root cause of healthcare inequities.
Aim 1: Education
The LGF will achieve its’ first aim of healthcare professional education through the utilization of the training simulations. As physicians, nurses, office clerks, technicians, and other healthcare professionals navigate the scenarios as Jasmin, they will encounter educational checkpoints. Instances of probable implicit racial bias will be red-light activities within the gaming environment. During the red-light activities, factoids defining biased behaviors Jasmin encounters are accessed by the player. The player will need to read the informative statements and answer related questions to test their knowledge. Once the red-light activity is successfully completed, the simulation will enter green-light mode, and the player will continue the gameplay.
Aim 2: Influence
The ultimate outcome of the LGF is to reduce implicit bias and influence clinical decision-making, which will ultimately reduce healthcare disparities. The influence aim is accomplished by the reduction of implicit bias of healthcare professionals via the successful completion of the training modules. Sustained reduction of reduced implicit bias is maintained through retraining at set points during the year after the initial onboarding process.
Aim 3: Cultural Competency
The third aim of increasing cultural competency in providers and healthcare professionals serves as an important supportive measure to decrease healthcare disparities in African Americans. When an organization is culturally competent, aspects of the organization, including attitudes related to healthcare disparities, are positively impacted. A study published in Healthcare Management Review examined how a cultural competency initiative affected hospital performance metrics. Hospital employees completed pre-assessments, including surveys, team-conducted interviews, focus groups, and website analysis. The results of the pre-assessment data were collected and organized into a feedback report for the experimental group of hospitals. Next, a diversity coach reviewed these results with the CEO and hospital leadership team. The diversity coach and leadership team then collaboratively made an action plan to implement systemic diversity intervention (infrastructure development, executive coaching, training, individual action plans, and other interventions) in the organization. The research demonstrated that the experimental group hospitals showed improvements in diversity leadership and strategic human resource management. Notably, improvements occurred in diversity attitudes and implicit bias for Blacks. Results further indicated that overall performance improved in hospitals that adopted interventions to increase cultural competency (Weech-Maldonado et al., 2018). The work suggests that addressing healthcare disparities in African Americans has the potential to not only improve health in target populations, but it also positively impacts the overall organizational performance.
Aim 4: Inclusivity
The final aim of the LGF serves to address the role of implicit bias in healthcare disparities by encouraging an environment of inclusivity within healthcare organizations. Past research provides a rationale for utilizing inclusivity to combat racial bias. A 2018 study published in JAMA examined factors that lead to inclusive work and learning environments in healthcare. Researchers performed a qualitative analysis of responses to weekly email surveys within participating healthcare facilities. The study noted that many narratives made suggestions about implementing mandatory education on how to accept implicit bias and combat those biases. Another theme noted was that confrontation of persons who express microaggressions that are sexist or racist get deflected with humor or other comments. The narratives collected reveal a path forward for healthcare organizations to increase inclusivity that may reflect what their everyday employees would like to see within their organizations (Aysola et al., 2018).
The noted research further demonstrates that healthcare organizations have internal issues that affect inclusivity and implicit biases. It is a logical assumption to make that the mere existence of such issues internally could be leaking out onto the actions and clinical decisions that affect the presence of healthcare disparities. Hence, the importance of the final aim to increase and promote inclusivity through an organizational focus on reducing biases.
Implementation of the Initiative
Implementation of the Looking Glass Framework occurs in four distinct phases:
Phase 1: Pre-Organizational Roll-Out
A series of explanatory meetings of appropriate stakeholders to include the leadership team (C-Suite), human resource team, service line directors, individual unit managers, and other members of leadership. The meetings should occur at the highest levels first. After the initial group of explanatory meetings, the human resource team will coordinate with a specialized task force called the Looking Glass Impact Commission (LGIC). The LGIC will provide a time-sensitive training schedule for the entire staff population. Additionally, the LGIC will coordinate with human resources for added support, instructions, and resources during the initial implementation of the project.
The LGIC is tasked with collaborating with outside vendors to acquire the updated technical equipment. The LGIC will also contract with simulation software vendors to design appropriate computer-based learning modules and specialty video game technologies that utilize perspective-taking healthcare scenarios. It is important to note that the LGIC will need to purchase/lease the equipment from vendors (VR goggles, computer terminals, etc.) in addition to contracting with other vendors to customize software that plays the simulations on the purchased equipment.
The Looking Glass Framework’s highly flexible design allows for one of three implementation options: VR only, combination VR and desktop-based learning simulations (DBLS), and DBLS only. Organizations have the purview to determine which option (equipment, features, etc.) works best for specific goals and cost constraints of their business. VR, video games, and other simulation-based technology are already utilized in a variety of industries. So, while adopting the Looking Glass specifications do have inherent costs, they are by no means an unreasonable investment.
The LGIC will also assist the human resources team by designing and producing marketing materials that are distributed throughout the hospital. The LGIC will have the flexibility to be a continued task force working with human resources or a time-limited team utilized only during the initial roll-out, dependent upon the healthcare organization’s needs.
Phase 2: Limited Scope Roll Out
Specific populations within the hospital will be the target of the initial dissemination of the initiative. The first participants of the training will include the C-Suite leadership team and service line directors. The next target set will be physicians, nurses, patient care assistants, and others identified as directly giving patient care.
Phase 3: Full Roll-Out
The remaining staff will receive the Looking Glass Framework training. The LGIC and human resources will coordinate in a verification and audit process to ensure all identified staff have completed training.
Phase 4: Feedback and Recertification
The LGIC will design, distribute (electronically), and review a survey of staff to gauge their perceived opinions on the initiative. The LGIC will compile the results into an actionable report for C-Suite executives. Twice annual recertification of staff in the training program will be ongoing. In addition, a yearly review of the Looking Glass Framework continued training, and staff feedback will be distributed to the senior leadership team. Qualitative metrics examining facility-specific health outcomes in minority populations will accompany the report to verify the initiative’s success factors.
Conclusion
Healthcare disparities in African Americans is an issue that all healthcare organizations need to address directly. The complex nature of the problem resides in the interconnectedness of health systems, American society, and the disparity-producing system of healthcare. Pervasive racial biases affect clinical decision-making and patient behavior. This occurs even when healthcare professionals have the best intentions to provide high-quality healthcare and patients want the best possible clinical outcome.
Perspective-taking simulations alongside VR technology and video games provide an innovative way to reduce healthcare disparities through the reduction of implicit racial bias. The LGF uses this innovation to educate healthcare professionals, improve clinical decision-making, increase cultural competency, and foster an environment of inclusivity. Improving overall healthcare outcomes rests on an organization’s ability to ensure that regardless of their race, a patient will receive the best possible care and engage in a positive, high-quality relationship with healthcare professionals. Implementation of the LGF is a giant step forward in addressing healthcare disparities by improving clinical decision-making and showing communities nationwide that every single patient will receive equitable treatment and the promise of the best chance at a long life.
Footnotes
Acknowledgements
Some components of the Looking Glass Framework were developed while the author attended Xavier University. This work is adapted from the author’s original essay on the same topic which placed 2nd nationally in the American College of Healthcare Executive’s 2020 Richard J. Stull Essay Competition in Healthcare Management. The author thanks Dwight Ellingwood for his support during the writing process for the original essay.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.