
Abstract
Hypersexuality and impulsivity are regarded as risk factors for sexual offending against children. Studies exploring these factors in undetected men who offended or are at risk of offending are rare. This study aims to investigate hypersexuality and impulsivity in treatment-seeking men with and without a diagnosis of (exclusive) pedophilia who committed child sexual abuse (CSA), consumed child sexual abuse images (CSAI), or feel at risk of offending sexually. Data were obtained from three child abuse prevention projects in Bamberg, Germany. We employed self-report (BIS-11, HBI), objective measures (TSO), and risk assessment tools (STABLE-2007). We computed Bayesian ordinal logit and binomial generalized linear models to explore differences between groups and to predict lifetime CSA and CSAI. Hypersexuality scores were particularly pronounced in patients with exclusive and non-exclusive pedophilia. Patients without pedophilia scored similarly to nonclinical samples. Impulsivity measures did not consistently differ between groups. We could not predict lifetime CSA and CSAI using impulsivity and hypersexuality measures. Sexual rather than general impulsivity seems to be an issue in men with pedophilia. The motivation to offend in patients without pedophilia is discussed.
Keywords
Introduction
International studies suggest that around 12% of children experience child sexual abuse (CSA; Pereda et al., 2009; Stoltenborgh et al., 2011). In Germany, between 3.1% and 7.1% of adults report that they have experienced CSA (Brunner et al., 2021; Witt et al., 2017, 2019), and 0.8% of the male general population report that they have abused children (Dombert et al., 2016). In addition to CSA, the prevalence of the consumption of child sexual abuse images (CSAI) is an increasing issue (Seto et al., 2015; Steel, 2009). Dombert et al. (2016) report that 1.7% of respondents have seen CSAI before. The negative effects on victims of CSA and CSAI are well documented (e.g., Lippus et al., 2020). Considering the high prevalence of CSA and CSAI and the impact on the lives of the victims, it is crucial to understand and prevent CSA and CSAI offending.
In this study, we will examine hypersexuality and impulsivity as influential risk factors for sexual offending in a sample of treatment-seeking men with and without (exclusive) pedophilia using the motivation-facilitation model of sexual offending (MFM; Seto, 2019) as a theoretical framework. The MFM identifies factors that motivate offending behavior and factors that—if present—moderate the risk of offending. The model suggests that high sex drive is one of the factors that motivate sexual offending. However, a high sex drive on its own does not necessarily lead to an offense. It is moderated by facilitating factors such as self-regulation problems or other trait and state factors related to offending behavior. Other motivating factors are paraphilias, including pedophilia (sexual attraction towards prepubescent children) and hebephilia (sexual attraction towards early pubescent children).
Exclusive and Non-Exclusive Hebephilia and Pedophilia
Pedophilia is a distinct construct (Schmidt et al., 2013) and one of the paraphilic disorders described in both major international diagnostic systems (i.e., the DSM-5 edited by the American Psychiatric Association, 2022, and the ICD-10 edited by the World Health Organization, 2016). It has been regularly linked with CSA and CSAI offending and the risk of recidivism (Hanson & Morton-Bourgon, 2005; Seto et al., 2006). However, only around half of the individuals convicted of CSA and CSAI report a sexual attraction towards minors (Eher et al., 2019; Seto, 2008). Only 17% of incarcerated individuals who molested children were identified as exclusively pedophilic (sexual attraction to children only; Eher et al., 2010). Other estimates for exclusive pedophilia range from 7% to 36% in samples of men who are attracted to children (Bailey et al., 2016; Beier et al., 2015). In the general population, the criteria for an exclusive pedophilia diagnosis are only met by less than 0.1% of men, compared to 0.6% for the non-exclusive type (Dombert et al., 2016).
Men with a diagnosis of exclusive pedophilia report feeling more emotional distress (Dombert et al., 2016), an earlier onset of sexual attraction towards children (Briken et al., 2019), and are more likely to have fallen in love with a child (Martijn et al., 2020) compared to men who are equally attracted to children and adults. Romantic interest, in addition to sexual attraction, might increase the risk of offending in individuals with pedophilia (Bailey et al., 2016; Etzler et al., 2020). Accordingly, the rates for sexual recidivism were found to be five times higher in men with exclusive pedophilia who offended than in men with non-exclusive pedophilia who sexually offended (Bailey et al., 2016; Biedermann et al., 2023; Eher et al., 2015; Etzler et al., 2020). Furthermore, neuropsychological studies indicated that individuals with exclusive pedophilia showed more deficits in executing functions than other offending and non-offending groups (Turner et al., 2020).
Hypersexuality
High sex drive has been labeled with many different terms, such as hypersexuality, hypersexual disorder, sexual addiction, sexual impulsivity, or excessive sexual drive (e.g., Briken, 2016; Kafka, 2010). It is now represented as a new category of pathological sexual behavior introduced by the ICD-11, called Compulsive Sexual Behavior Disorder (World Health Organization, 2022).
Even though a total of more than seven sexual outlets per week (total sexual outlet [TSO]; meaning the number of orgasms per week regardless of how the orgasm is reached) is sometimes used as a rough indicator of high sex drive (Kafka, 2010; Kinsey et al., 1948; Seto, 2019). A study by Winters et al. (2010) showed that there was no difference in TSO between individuals seeking treatment due to sexual addiction and non-treatment seeking individuals. The results suggested a higher sexual desire and a lower sexual inhibition in treatment-seekers, which emphasizes the need to consider the interaction between hypersexuality and impulse control.
High Sex Drive and Offending Behavior
High sex drive is one of the three primary motivating factors for sexual offending (Seto, 2019) and has been linked to sexual offending behavior, increased long-term recidivism risk, and sexually coercive behavior against women (Hanson & Harris, 2000; Kingston & Bradford, 2013; Knight & Sims-Knight, 2003). Sexual preoccupation, a closely related construct, is commonly used as a predictor for risk assessment and shows good predictive validity for the prediction of sexual recidivism (Etzler et al., 2020; Hanson et al., 2007; Hanson & Morton-Bourgon, 2004; Knight & Thornton, 2007). However, looking at the number of TSOs per week, the picture is not as clear. While some studies found TSO to be higher in individuals convicted of sexual offenses than in nonclinical community samples (Kingston & Bradford, 2013; Marshall et al., 2008; Marshall & Marshall, 2006), other studies could not identify a direct connection between a high number of TSO and aggressive sexual behavior (Klein et al., 2015; Malamuth et al., 1995). More recent studies by Malamuth et al. (2021) indicate that problematic sexual behavior derives from a complex interaction between different factors and is not based on an increased sex drive alone.
High Sex Drive and Child Sexual Abuse
Klein et al. (2015) could not find a direct relationship between high sex drive and self-reported CSA in a community sample. However, high sex drive appeared to be a risk factor for CSAI. Kingston et al. (2008), using a sample of persons convicted of CSA, found that the use of deviant pornography, defined as the depiction of violence or CSAI, was a general risk factor for reoffending, while the frequency of pornography use in general—as an indicator for high sex drive—was only relevant in individuals with a relatively high risk for sexual reoffending. In contrast, Babchishin et al. (2015) showed that men who are attracted to children and have only committed CSAI offenses were more likely to have problems with sexual preoccupation and sexual self-regulation than men who are attracted to minors and who had committed CSA. Lastly, various studies suggest a generally increased sexual desire in men attracted to children (Gerwinn et al., 2018; Lampalzer et al., 2021; Santtila et al., 2015).
Self-Regulation and Impulsivity
Gerwinn et al. (2018) could differentiate individuals with and without a history of CSA using general impulsivity measures. This result corresponds to other findings indicating that impulsivity could be an essential risk factor for sexual offending behavior (Cohen et al., 2002, 2018; Jahnke et al., 2015; Krasowska et al., 2013; Turner et al., 2018). Furthermore, general self-regulation as well as sexual self-regulation, which are closely related to the construct of (sexual) impulsivity, are common dynamic risk factors for reoffending (Etzler et al., 2020; Hanson et al., 2007; Hanson & Morton-Bourgon, 2005). This is underlined by the finding that individuals who committed CSA had lower scores on higher executive functions than those who committed offenses against adults (Joyal et al., 2014; Turner & Rettenberger, 2020). In an inhibition performance task (go/no-go paradigm) that was combined with an fMRI assessment, men with sexual attraction towards children and lifetime sexual offending behavior showed more impulsive responses and reduced self-control than those without a history of sexual offending behavior (Kärgel et al., 2017). In constrast, a similar study could not distinguish between men who are attracted to children and those with and without a conviction history (Gibbels et al., 2019). Neutze et al. (2012) reported differences in sexual self-regulation between detected and undetected individuals who sexually offended children, which was due to a higher sexual preoccupation in undetected individuals who have committed sexual offenses. A study by Baltieri and Boer (2015) showed two clusters of participants convicted of CSA offenses, with one cluster scoring higher on impulsivity, sexual addiction, and sexual attraction to children compared to the second cluster.
However, it seems that general impulsivity is not related to attraction to children in general. The prediction of sexual attraction towards children in individuals who committed CSA offenses via self-reported impulsivity was not possible (Carvalho, 2018). Lampalzer et al. (2021) reported an increased degree of hypersexuality in men who are attracted to children, while impulsivity was comparable to a nonclinical sample. The authors argued, based on previous research (Reid et al., 2015), that not general impulsivity but context-specific impulsivity (i.e., sexual impulsivity) could be particularly relevant in hypersexual men. This assumption was confirmed by empirical results investigating the relationships between sexual excitation, sexual inhibition, general impulsivity, personality measures, and hypersexuality (Rettenberger et al., 2016).
Other Facilitating Factors
Among self-regulation, several other factors could facilitate sexual offending: Amongst others, emotional congruence with children (Konrad et al., 2018), social rejection (e.g., due to stigma; Jahnke et al., 2015), empathy deficits (Schuler et al., 2019), hostility towards woman (Ray & Parkhill, 2023), and intimacy deficits (Martin & Tardif, 2014) are all constructs that have been linked to (re)offending and are used to predict recidivism (Eher et al., 2012).
Present Study
The present study uses the MFM (Seto, 2019) as a theoretical framework to investigate the relationship between pedophilia, hypersexuality, and impulsivity in a sample of patients with and without (exclusive) pedophilia disorder who seek treatment because they offended sexually against minors or feel to be at risk of offending. To our knowledge, studies investigating hypersexuality and impulsivity in individuals with pedophilia did not differentiate between the exclusive and non-exclusive types. This study provides an analysis that distinguishes exclusive and non-exclusive pedophilia to investigate the relationship between hypersexuality, impulsivity, and exclusive pedophilia. Most studies in the field employ self-report measures to operationalize hypersexuality and impulsivity. In this study, we use three measures for hypersexuality, one self-report measure (Hypersexual Behavior Inventory [HBI]; Reid et al., 2011), an objective measure (total sexual outlets; TSO), and the therapists’ ratings (STABLE-2007; Hanson et al., 2007). Impulsivity is accessed by a self-report questionnaire (Barratt Impulsiveness Scale [BIS-11]; Patton et al., 1995) and again the therapists’ ratings (STABLE-2007). By combining the different methods, we aim to understand how the different perspectives affect the group differences.
In addition to comparing hypersexuality and impulsivity scores between groups, this study aims at predicting lifetime CSA and CSAI offending using hypersexuality and impulsivity measures. In doing so, the theoretical assumption that impulsivity, hypersexuality, and pedophilia contribute to offending behavior is empirically examined.
The leading research questions of the present study are: 1. Can hypersexuality measures differentiate between patients with exclusive pedophilia, non-exclusive pedophilia, and no pedophilia? 2. Can impulsivity measures differentiate between patients with exclusive pedophilia, non-exclusive pedophilia, and no pedophilia? 3. Can impulsivity and hypersexuality measures differentiate between lifetime CSA and CSAI offending in patients with exclusive pedophilia, non-exclusive pedophilia, and no pedophilia?
Methods
Participants
The participants were recruited from three child abuse prevention projects in Bamberg, Germany. The “Don’t Offend [kein Täter werden]” prevention project (1) provides treatment for men with pedophilia disorder. For inclusion in the project, patients are not allowed to be currently under investigation for CSAI or CSA (Beier et al., 2009). The “Bavarian Abuse Prevention Program” (2) targets people without pedophilia who have sexually offended children or feel at risk of offending and are not under investigation. The “Project Bright Field [Projekt Hellfeld]” (3) includes patients who offended minors after they received a criminal complaint but before conviction, regardless of the diagnosis. All three projects are voluntary.
The treatment starts with a two-hour-long exploratory interview with a trained psychologist or psychiatrist. Comorbidities, history of offending, substance abuse and sexual history are explored to diagnose paraphilias. The diagnosis of pedophilia (disorder) is based on the ICD-10 criteria (World Health Organization, 2016) and especially on the presence of sexual fantasies involving minors. Therefore, past offending behavior alone is not a sufficient criterion for the diagnosis. After the interview, therapists and patients answer a battery of questionnaires. For the present study, we used self-reported criminal histories, diagnosis of pedophilia, STABLE-2007 ratings, HBI and BIS-11 scores, and TSO per week.
Between October 2016 and June 2022, 222 exploratory interviews were conducted across all three projects. Two hundred and seven of those answered the diagnostic questionnaires. Of these 207 participants, 24 were excluded for the following reasons: four were female participants, five patients were under 18 years of age, and 15 participants had too many missing items. This resulted in a total of N = 183 participants. The demographics are shown in the freely accessible data repository (https://osf.io/mr5py/).
Research Ethical Approval
The ethics committee of the University of Bamberg approved the present study (29 October 2019, 30 July 2022).
Measures
HBI
The Hypersexual Behavior Inventory (HBI; Reid et al., 2011) is a questionnaire that assesses hypersexuality. The self-report measure consists of 19 items that have to be answered on a 5-point scale from never (1) to very often (5).” It has three subscales: Coping (seven items), Control (eight items), and Consequences (four items). In the English version, the HBI has a Cronbach’s α of 0.95 (Reid et al., 2011). The German version of the HBI has a Cronbach’s α of 0.90 (Klein et al., 2014).
BIS-11
The Barratt Impulsiveness Scale (BIS-11; Patton et al., 1995) is a self-report questionnaire to measure impulsivity. The 30 items are answered on a 4-point scale from rarely/never (1) to nearly always/always (4). The instrument consists of six factors: Attention (five items), Cognitive Instability (three items), Motor (seven items), Perseverance (four items), Self-Control (6 items), and Cognitive Complexity (five items). The Cronbach’s α in the English version varies between 0.79 and 0.82 (Patton et al., 1995). Preuss et al. (2008) revealed a Cronbach’s α of 0.69 for the German version.
TSO
TSO was defined as the number of orgasms per week over the last 6 months, regardless of how the orgasm was reached. It was measured using a 5-point ordinal scale from less than one orgasm per week to 7 orgasms and more.
STABLE-2007
The STABLE-2007 is an instrument for assessing the dynamic risk factors of people who are convicted of sexual offenses (Hanson et al., 2007). The therapist rates the patient on a scale from zero to two on 13 items addressing significant social influences, general self-regulation (e.g., poor problem-solving skills), sexual self-regulation (e.g., deviant sexual interests), intimacy deficits (e.g., lack of concern for others), and cooperation with supervision. All therapists completed an officially certified STABLE-2007 training. The intraclass correlation coefficients were previously estimated at .90 for the German version (Eher et al., 2012; Etzler et al., 2020).
Lifetime CSA and CSAI Offending Against Minors
In the diagnostic interview, therapists extensively explore the patients’ sexual behavior (including CSA, CSAI) and transfer it to a questionnaire.
Statistical Analysis
Analysis and modeling were performed in R 4.2.2 (R Core Team, 2022) using the Tidyverse collection of packages (Wickham et al., 2019). Models were programmed and sampled using Stan probabilistic programming language (Carpenter et al., 2017). A leave-one-out (LOO) information criterion was computed using the “loo” library (Vehtari et al., 2017).
We used Bayesian generalized linear models and characterized individual model terms using the samples from the posterior distribution. For each term, we computed the mean and a 97% credible interval (CI; also called compatibility interval), a range that contains 97% of the probability mass based on values from the sampled posterior distribution. We chose to use a 97% CI because it is close to the conventionally chosen 95% but it reminds us that such intervals are an arbitrary choice.
For behavioral data, we computed 97% percentile confidence intervals via non-parametric bootstrapping with 1000 iterations (Davison & Hinkley, 1997). For group confidence intervals, data were sampled with a replacement for each frame across all participants, averages were computed per participant, and the group average for the sample was calculated. The authors take responsibility for the integrity of the data, the accuracy of the data analyses, and have made every effort to avoid inflating statistically significant results.
Models for Outcome Variables on the Ordinal Scale
We used partial credit ordinal logit models to quantify the difference between groups for instruments that use ordered categorical (Likert) scales (Williams, 2016). This is one of the models developed as part of the Item Response Theory that explicitly accounts for both many-to-one mapping between implicit evaluation and explicit discretized response and for potential differences between response item locations. This is a recommended approach for analyzing ordered categorial data (here: data based on Likert scales), as these aspects cannot be accounted for by more restricted linear regression models, such as ANOVA.
For each instrument, we assumed that a continuous response (e.g., hypersexuality) is converted to discrete Likert points using a common set of cut-points. For convenience, both cut-points and continuous response are remapped to a continuum between 0 and 1, so that 0 corresponds to the minimal possible response (mapped to the lowest discrete response either 1 or 0, in the case of STABLE-2007 rating) and 1 corresponds to the maximal possible response (mapped to the higher discrete response, e.g., 4 for BIS-11 instrument, 5 for TSO, etc.). We opted for Bayesian implementation of the model, as it allows for the regularization of parameters via priors that reduces overfitting and simplifies statistical comparison via differences in posterior distributions. However, note that the results would be the same when the statistical model is estimated using frequentist procedures (apart from minute differences due to the stochastic sampling procedure in Bayesian MCMC approach).
Each group was characterized by its own independent average continuous response and the difference between groups was assessed by computing a posterior distribution of difference between the average continuous responses. In addition, we assessed whether group identity improves model fit using a LOO information criterion (Vehtari et al., 2017), which is interpreted the same way as other information criteria, such as AIC. We reported the difference in expected log predicted density (ΔELPD, mean ± standard error) relative to the model with group effect.
Models for Outcome Variable on the Binomial Scale
Lifetime CSA and CSAI were modeled using a binomial generalized linear model using HBI, BSI-11, TSO, and STABLE-2007 as ordered categorical predictors. Here, we assumed that discrete responses correspond to different levels of continuous response bound to 0 to 1 so that 0 corresponds to the minimal possible response (mapped to the lowest discrete response, either 1 or 0, in the case of STABLE-2007 rating) and 1 corresponds to the maximal possible response (mapped to the higher discrete response, e.g., 4 for BIS-11 instrument, 5 for TSO, etc.). The model fitted continuous response levels for intermediate discrete responses and used an average continuous response for each instrument as a predictor. We used variable intercept and slopes for each group.
The formal description of the models is provided in a data repository (https://osf.io/mr5py/).
Results
Summary Statistics of HBI, TSO, BIS-11, and STABLE-2007 by Group.
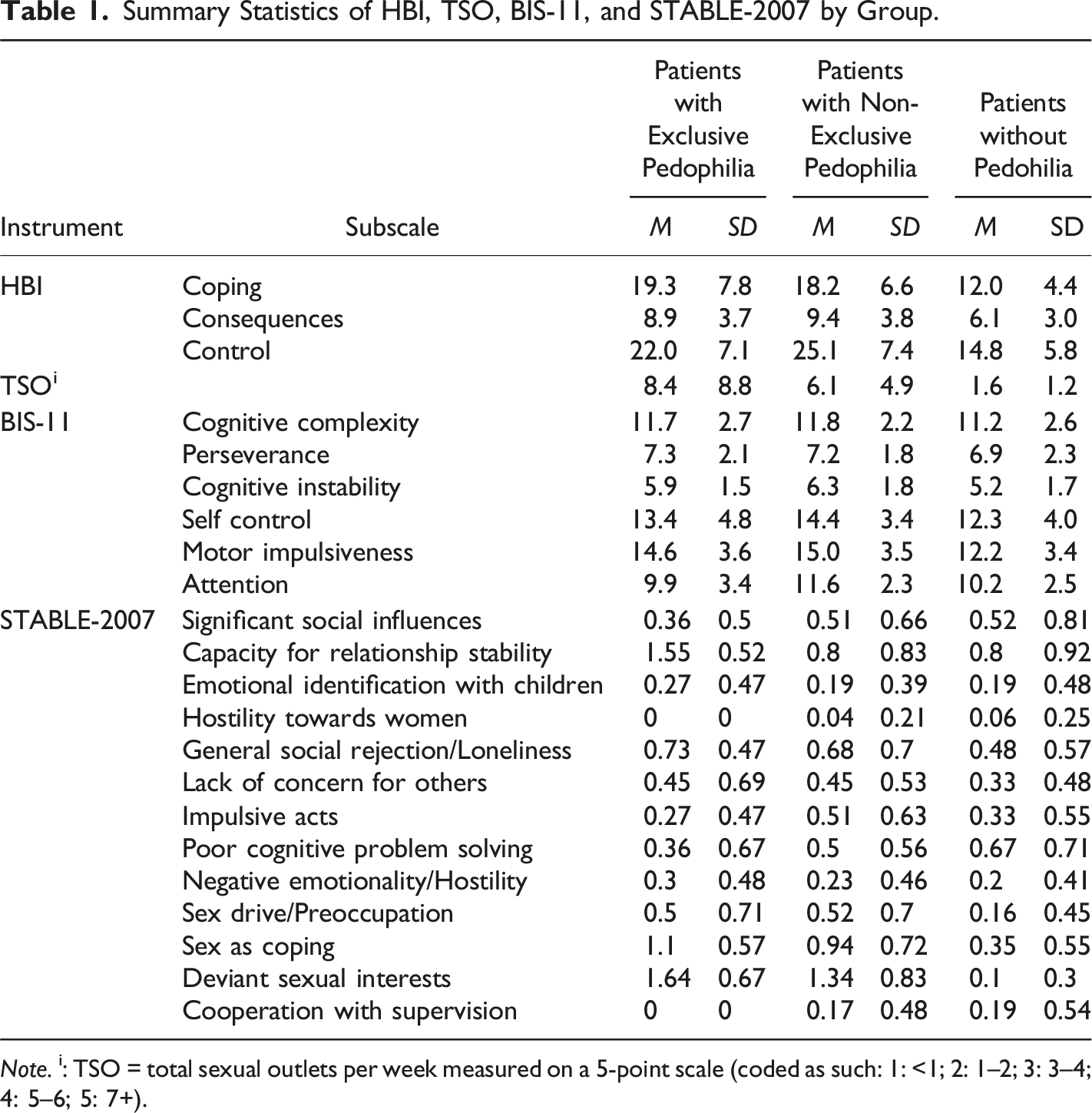
Note. i: TSO = total sexual outlets per week measured on a 5-point scale (coded as such: 1: <1; 2: 1–2; 3: 3–4; 4: 5–6; 5: 7+).
Using Hypersexuality and Impulsivity Measures to Distinguish Between Patient Groups
In the first step of the analysis, we aimed to discriminate between patients with exclusive pedophilia, non-exclusive pedophilia, and patients without pedophilia by using HBI, BIS-11, and STABLE-2007 data.
HBI
To examine whether the HBI can discriminate between patients with exclusive pedophilia, non-exclusive pedophilia, and patients without pedophilia, we modeled response for each group using multilevel ordinal logit regression with pooled random effects for individuals and independent intercept terms for each group. The latter corresponds to an average inferred continuous-scale response to HBI. The proportion of response levels and posterior predictions of the model are depicted in Figure 1(a). Posterior distributions of inferred average continuous-scale response per group are shown in Figure 1(c), and a summary of the posterior distribution of differences between pairs of groups is shown in Figure 1(b). HBI for patient groups.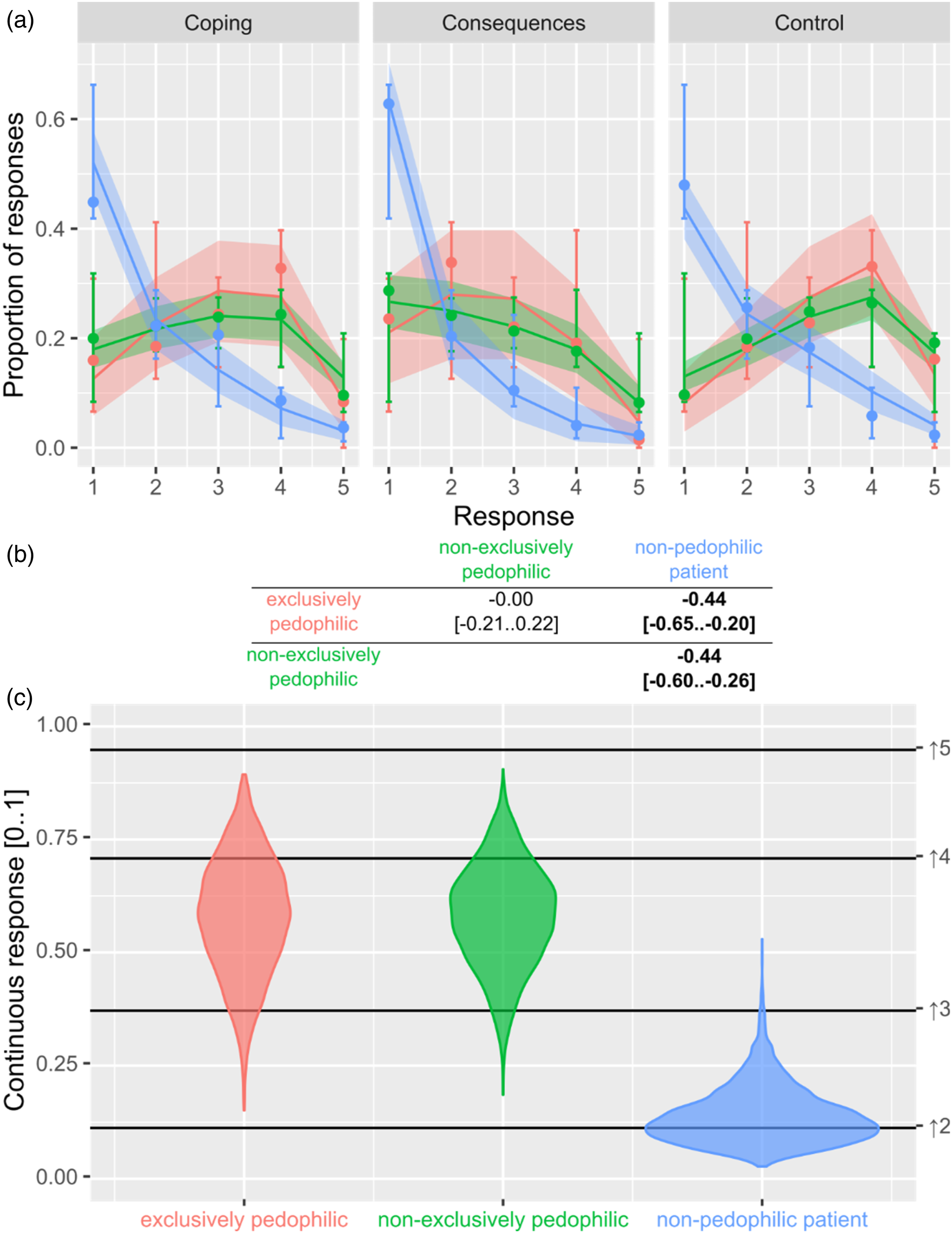
The analysis suggests that evaluations were very similar for patient groups with exclusive pedophilia and non-exclusive pedophilia compared to patients without pedophilia. Analysis via LOO information criterion indicates some overall influence of group information (ΔELPD = −0.5 ± 1.6 for the model with the main effect of the group) with significant differences between the (exclusive) pedophilia groups and the group without pedophilia (see Figure 1(b)).
TSO
Similar to the model above, we modeled responses for each group to investigate whether TSO measures allow discrimination between groups. Details of the model are shown in Figure 2. The results indicate higher scores in both pedophilic groups and lower scores in the non-pedophilic group. Between-group comparisons of the posterior distributions show significant differences between the non-pedophilic group and pedophilic groups. Analysis via LOO information criterion suggests the relevance of group information (ΔELPD = −4.0 ± 3.3 for the model with the main effect of the group only). TSO for patient groups.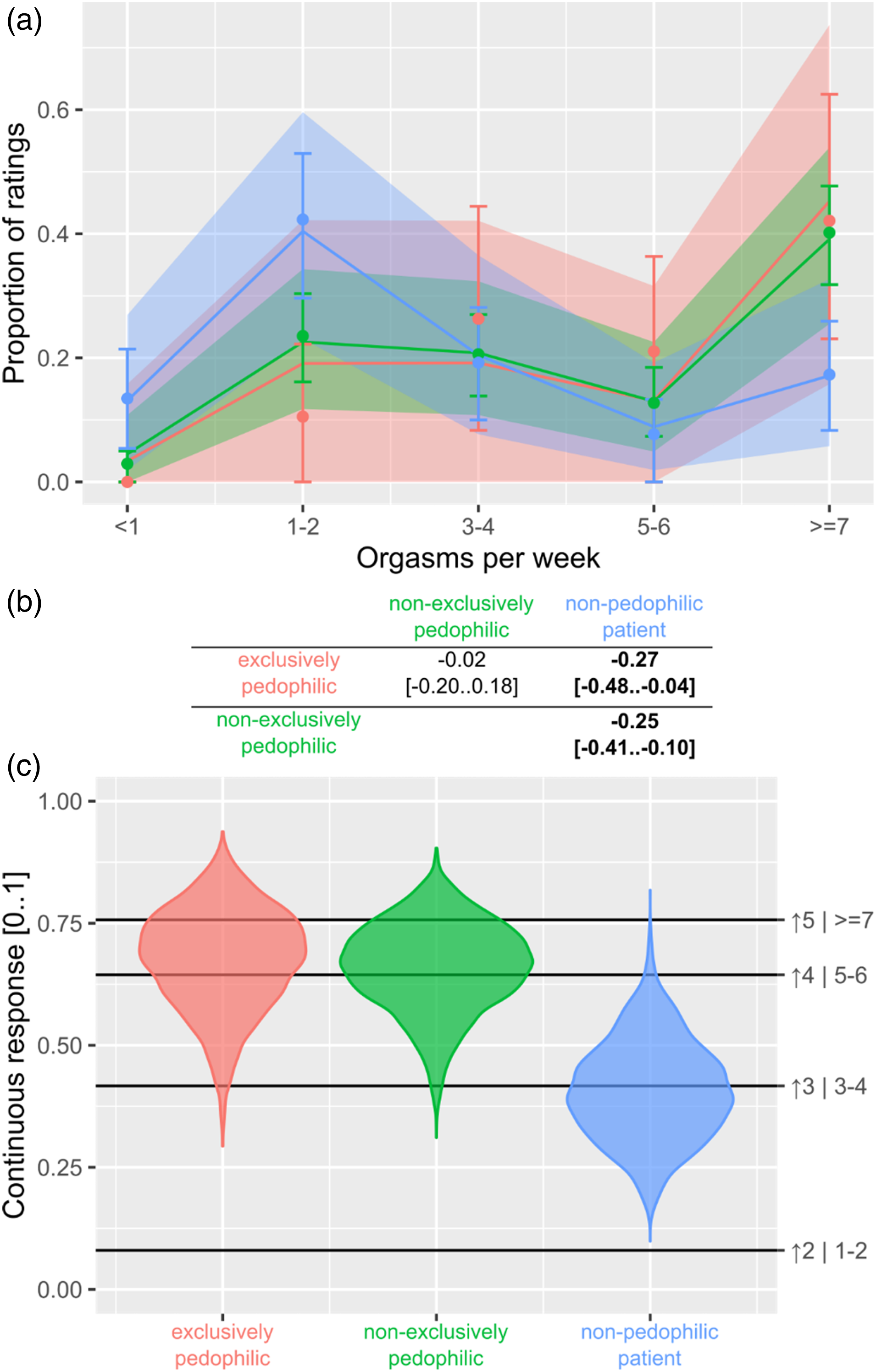
STABLE-2007
To test whether STABLE-2007 ratings can discriminate between groups, we calculated a similar model as for TSO and HBI above. The item Deviant Sexual Interests was excluded from the group comparison as it measures paraphilia and would confound with the grouping variable.
The analysis indicates that ratings for intimacy deficits and general self-regulation do not differ between groups (Figure 3 left and middle column). The data further suggest that therapists rate patients without pedophilia lower on sexual self-regulation than the two pedophilic groups (Figure 3 right column). This is supported by between-group comparisons of the posterior distributions (Figure 3(c)). Analysis via LOO information criterion suggests the relevance of group information (ΔELPD = −27.2 ± 6.9 for the model with no main effect on the group). The sum score of all STABLE-2007 items does not differ significantly between groups using a Krusksal-Wallis rank sum test, H(2) = 2.4107, p = .299 (see Figure 3(a)). STABLE-2007 for patient groups.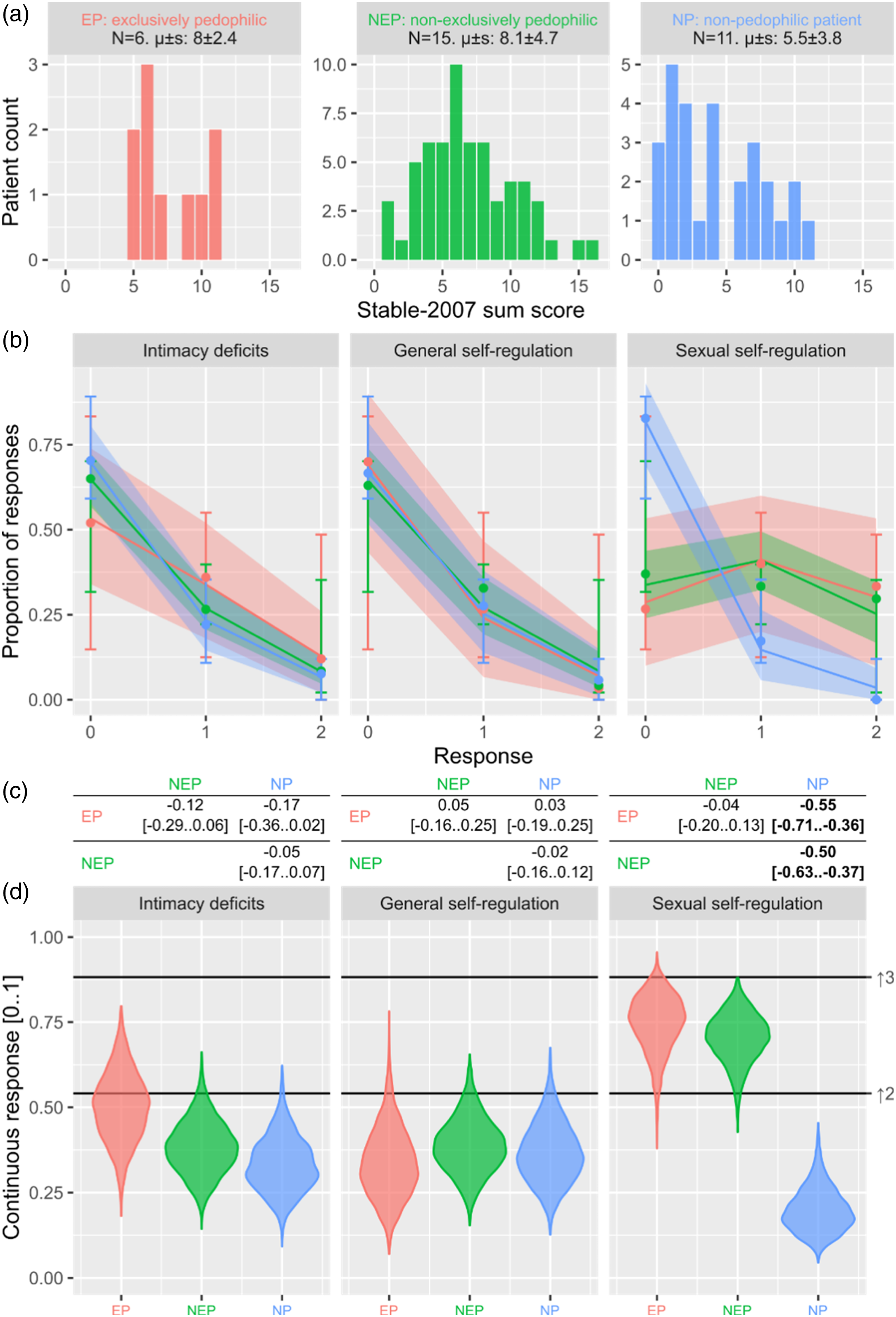
BIS-11
Finally and again similar to the models above, we modeled the response pattern for each group with the BIS-11 as the predictor (Figure 4). The analysis using information criterion comparison with a simpler model (ΔELPD = −0.1 ± 1.0 for the model with no main effect of the group) and for pairwise difference (Figure 4(c)), suggests that there were no consistent differences between patient groups. Only a weak significant difference between patients without pedophilia and patients with non-exclusive pedophilia was found. BIS-11 for patient groups.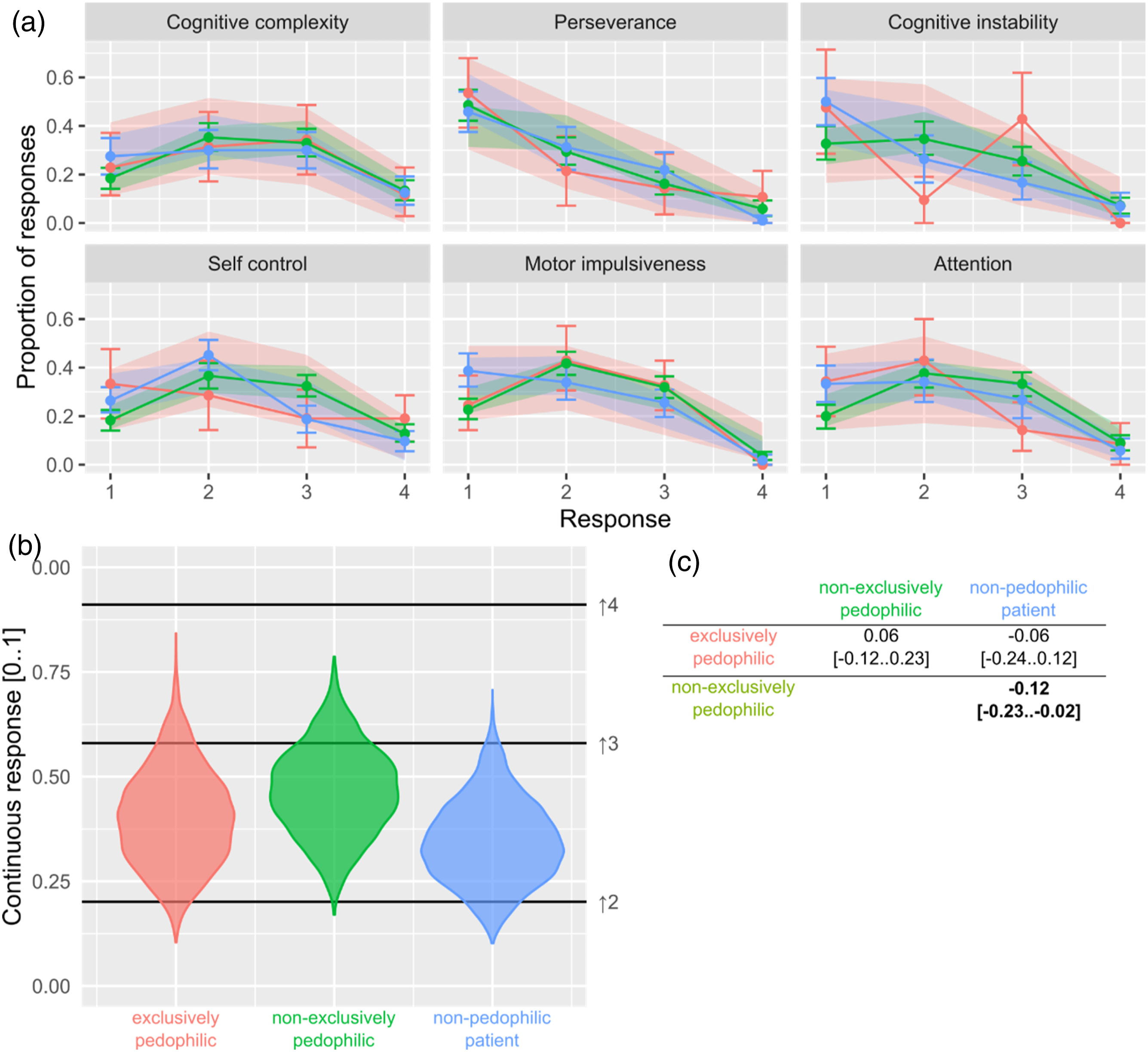
Using Hypersexuality and Impulsivity Measures to Differentiate Between Lifetime Offending
In this part of the analysis, we aimed to compute predictive models for lifetime CSAI and CSA offending with patient groups, BIS-11, HBI-19, and STABLE-2007, as predictors.
BIS-11, HBI, TSO, and STABLE-2007 ratings did not indicate lifetime CSA or CSAI offending. Looking at CSAI offending (Figure 5(b), right column), patients with exclusive pedophilia were most prone to CSAI consumption, followed by patients without pedophilia. In patients without pedophilia, CSAI prevalence was the lowest. The analysis suggests no differences in CSA offending between groups (Figure 5, left column). Lifetime CSA (LCSA) and CSAI (LCSAI) for patient groups.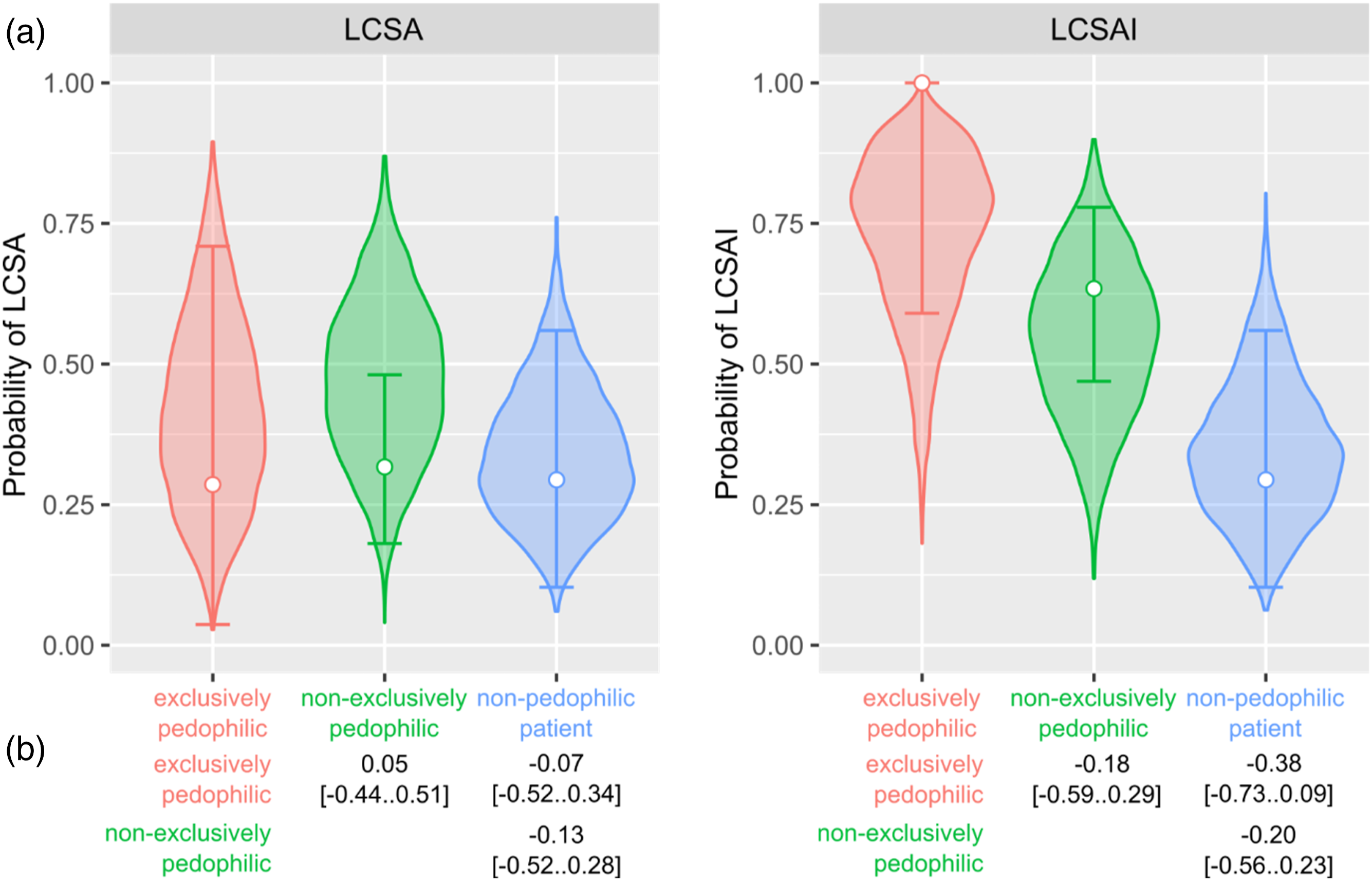
Discussion
In the present study, we analyzed hypersexuality and impulsivity in a unique sample of men with exclusive and non-exclusive pedophilia and no pedophilia. The sample consisted of people who sought treatment because they offended sexually against minors or felt at risk of offending. To examine hypersexuality, we did not solely rely on one measure but used self-report (HBI), risk assessment (STABLE-2007), and objective measures (TSO) to triangulate the construct of hypersexuality. Self-report (BIS-11) and risk assessment measures (STABLE-2007) were used for impulsivity.
All hypersexuality measures were able to differentiate between patients with (exclusive) pedophilia and patients without a pedophilia diagnosis. General impulsivity measures could not distinguish between patients with and without (exclusive) pedophilia. Neither hypersexuality nor impulsivity, regardless of the measure used were able to predict lifetime CSA or CSAI offending. Only the diagnosis of (exclusive) pedophilia corresponded to higher rates of lifetime CSAI offending.
Hypersexuality
In this study, as well as in others, patients with pedophilia who seek treatment showed notable results in specific measures related to sexual (dys-)regulation (Lampalzer et al., 2021; Reid et al., 2015). HBI scores were able to statistically differentiate between patients with and without pedophilia, with HBI scores significantly pronounced in the two pedophilic groups. When looking at the HBI sum score, 63% of patients with exclusive pedophilia and 55% of patients with non-exclusive pedophilia scored above the cut-off of 53, which could be used as a diagnostic indicator for hypersexuality disorder (Karila et al., 2014). These numbers are consistent with other studies (Engel et al., 2018; Lampalzer et al., 2021; Savard et al., 2021). The present study is one of the first to analyze HBI scores in men without pedophilia seeking treatment due to CSA and CSAI issues. This particular population showed no pronounced scores in the HBI, and only 10% of this subsample scored above the cut-off. Hence, patients without pedophilia were comparable to community samples (Klein et al., 2014; Olver et al., 2022; Reid et al., 2011). Similar group differences were found in TSO measures and STABLE-2007 ratings for sexual self-regulation.
As both ratings for coping in the STABLE-2007 and HBI were elevated in patients with (exclusive) pedophilia, we argue that utilizing CSAI for coping purposes might maintain a vicious circle of unpleasant emotions followed by sexual coping that again initiates pedophilia-related self-loathing and guilt, which could again lead to sexual coping behavior and, thus, higher TSO. Additionally, patients with pedophilia are generally more prone to depression and anxiety (Cohen & Galynker, 2002; Kafka & Hennen, 2002). The role of negative emotions and emotion regulation in such a vicious circle is also observed in other mental disorders, such as alcohol use disorder (Reichl et al., 2022).
Impulsivity
The analysis indicates that impulsivity scores (BIS-11 and STABLE-2007) cannot discriminate between patient groups and are not particularly pronounced compared to community samples (Fossati et al., 2001; Mulhauser et al., 2014; Reid et al., 2012). This result is comparable to previous findings on impulsivity in men with pedophilia (Engel et al., 2018; Gerwinn et al., 2018; Lampalzer et al., 2021; Savard et al., 2021). In the present dataset, 14% of patients with exclusive pedophilia and 33% of patients with non-exclusive pedophilia scored above the cut-off, indicating high impulsivity (>72; Stanford et al., 2009), compared to 11.1% in Lampalzer et al.’s sample of men with pedophilia (2021). Therefore, general impulsivity seems unrelated to CSA, CSAI, and pedophilia in a treatment-seeking sample. However, this result is contrasted by literature that found impulsivity to be a common risk factor for sexual offending (e.g., Cohen et al., 2002, 2018; Jahnke et al., 2015; Krasowska et al., 2013).
We argue that patients with pedophilia who seek treatment are not generally impulsive but struggle specifically to inhibit their sexual impulses. This is in accordance with Lampalzer et al. (2021), who argue that context-specific impulsivity (e.g., sexual impulsivity) might be a problem in men with hypersexuality. Context-specific impulsivity is also observed in patients with substance-use disorders who show no deficits in general impulsivity but react impulsively when confronted with substance-associated cues (Czapla et al., 2016). Future research should address these assumptions, for example, by using behavioral tasks that implement context-specific stimuli in a go/no-go task as has been done, for instance, in addiction research (e.g., Czapla et al., 2016).
CSA and CSAI Offending
In the present study, about 25% of patients reported a lifetime CSA offense. The prevalence did not differ between patients with exclusive pedophilia, non-exclusive pedophilia, and patients without pedophilia who sought treatment. For comparison, recidivism studies find pedophilia to be a discriminating factor for CSA reoffending (Hanson & Harris, 2000); other studies find that about half of people convicted of CSA have pedophilia (Eher et al., 2019; Seto, 2008), and in community samples, about 1% of people who are attracted to children committed CSA (Dombert et al., 2016). These findings emphasize that it is crucial to differentiate between convicted, treatment-seeking, and community samples when studying CSA and pedophilia. Apart from the diagnoses, lifetime CSA offending could neither be predicted by impulsivity nor hypersexuality measures nor by STABLE-2007 ratings, although some literature suggests a relationship between hypersexuality, impulsivity, and (re-)offending (Hanson & Harris, 2000; Kingston & Bradford, 2013; Knight & Sims-Knight, 2003).
A distinct difference between patient groups in lifetime CSAI offending was found. CSAI offending was prevalent in all patients with exclusive pedophilia, in about 62% of patients with non-exclusive pedophilia, and about 25% of patients without pedophilia. The high prevalence in patients with (exclusive) pedophilia can be explained by the motivation-facilitation model (Seto, 2019), where pedophilia is a strong motivating factor for CSAI offending. However, it must be emphasized that the current sample consists of patients who seek treatment; therefore, the findings cannot be generalized to all people attracted to children. Hypersexuality—another motivating factor—was also more prevalent in both groups of patients with pedophilia. However, we could not predict lifetime CSAI offending using hypersexuality (or impulsivity or STABLE-2007) measures.
In contrast to patients with (exclusive) pedophilia, we could not find motivating factors to offend children in the group of patients without pedophilia. Neither did this group show pronounced scores in hypersexuality nor impulsivity measures or met the criteria for paraphilias. Considering that about 25% of the patients without pedophilia reported CSA and about 25% CSAI, these results are particularly striking. While several studies find differences between individuals with and without pedophilia who sexually offend (Gerwinn et al., 2018; Sigre-Leirós et al., 2015), a motivating factor for this study’s sample is yet to be found. Future research could identify motivating, facilitating, and situational factors that lead to CSA in men without pedophilia.
Limitations
The first limitation of this study is the sample size. Readers must be cautious when interpreting data from patients with exclusive pedophilia, as 20 cases are not much data to draw from. However, as so little published data on patients with exclusive pedophilia exist, we decided to report the subsample regardless of the sample size.
Second, the data used in the present study is biased as individuals seeking treatment are motivated to change or suffer a certain amount of suffering. Consequently, individuals who do not problematize their sexual attraction and behavior and individuals who manage their sexual attraction to children themselves are not represented in this study.
Third, we subsumed nepiophilia, pedophilia, and hebephilia under the term pedophilia (either exclusive or non-exclusive) and ephebophilia, teleiophilia, mesophilia, and gerontophilia as no pedophilia (Seto, 2017). Although this estimation is common in research practice, it might bias the data as specific differences between these chronophilias might exist.
Fourth, this study relied on the self-reported offense history only. Therefore, although the prevention projects are anonymous, this study might underestimate the rate of offending behavior. However, research suggests that self-reported (sexual) offending seems reliable (Jolliffe et al., 2003; Krohn et al., 2010; Pham et al., 2021) and controlling for potential underreporting does not increase predictive validity (Kroner et al., 2007). Further, the operationalization of offending captures the lifetime prevalence of offending behavior, and future research should use a more nuanced measure of CSA and CSAI offending.
Finally, the STABLE-2007 is a well-established instrument designed to estimate the risk of reoffending (Brankley et al., 2021; Hanson et al., 2007). However, its reliability, objectivity, and validity for individuals seeking treatment is yet to be tested. Additionally, stereotypes and misconceptions of people with pedophilia and the knowledge of past offenses might lead to biases in the therapists’ ratings.
Conclusion
To treat patients who seek professional support because of past offenses or because they feel at risk of offending, each patient requires careful investigation and treatment of motivating and facilitating factors. This is especially important in patients without pedophilia. For this group pedophilia is not a motivating factor and practitioners might assume hypersexuality as the explanation for (potential) offending behavior. However, based on the present study, treatment-seekers without pedophilia show no pronounced hypersexuality scores. Therefore, practitioners should be cautious to assume any common motivating factors in such patients. It seems even more important to explore motivating factors for each patient individually, as the group of patients without pedophilia seems to be more heterogenous. For patients with (exclusive) pedophilia this study suggests generally higher prevalence of hypersexuality. Therefore, two motivating factors (pedophilia and hypersexuality) are prevalent in patients with pedophilia and practitioners should treat not only the pedophilia disorder but should also pay attention to symptoms of hypersexuality.
In contrast to forensic samples, general impulsivity seems to have a substantially lower relevance in treatment-seeking samples. In accordance with our finding on hypersexuality, practitioners should focus on sexual rather than general self-regulation, when working with men under voluntary treatment.
While well-studied tools exist to estimate the risk of (re)offending in forensic samples, community prevention programs lack such instruments. In consequence, practitioners often employ measures developed for forensic patients in non-forensic contexts, such as the prevention programs in Bamberg, Germany, using the STABLE-2007, although its effectiveness for this specific population remains uncertain. Findings from this study suggest no relationship between STABLE-2007 ratings and lifetime CSA and CSAI offending, which might indicate that the STABLE-2007 is not a valid risk assessment tool for treatment-seeking patients. Von Franqué et al. (2023) found similar results for reoffending and static risk factors. With the exceptions of the CPORT no instrument was able to predict recidivism in a sample of men under voluntary treatment. Practitioners should, therefore, be cautious when using forensic risk assessment tools in community programs as the predictive validity seems limited.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The child abuse prevention projects in Bamberg, Germany, are funded by the German national health insurance (“Spitzenverband der gesetzlichen Krankenversicherungen,” GKV-SV) and the Bavarian Ministry of Justice (“Bayerisches Staatsministerium der Justiz”). The funding organizations were not involved in the present research.