
Abstract
Research investigating potential pathways from Adverse Childhood Experiences (ACEs) to later self-harming and offending behaviours has inconsistent findings. Past research, however, has not fully explored the interplay between ACEs and modifiable psychological factors, such as shame and self-compassion. The present study explored the relationship between ACE, shame, and self-compassion to identify their role in explaining the variance in later harm in a sample of individuals who have committed sexual offences. Two hundred and fifty adults incarcerated for sexual offences participated. Multiple Regression and Mediation Analyses were applied to establish if ACE, shame and self-compassion explained the variance in harm and explore potential psychological pathways between ACE and harm, with shame and self-compassion as potential modifiable mediators. ACE, shame and self-compassion explained 55% of self-harm and 52% of psychological and physical harm variance. A more complex relationship was indicated for sexual harm, with only 19% of the variance explained by the model. The study increases our understanding of the relationship between variables and potential modifiable pathways between ACEs and later harming behaviours in a sample of individuals with sexual convictions. These modifiable psychological factors could be targeted to increase resilience, post-traumatic growth and reduce the risk of harm in later life.
Introduction
Adverse Childhood Experiences (ACEs) take the form of sexual abuse, emotional abuse, psychological abuse, physical abuse, or neglect (Vachon et al., 2015). There is empirical support for a relationship between ACEs and negative life sequelae, including both harm to the self (Hughes et al., 2017; Liu et al., 2018) and harm to others (i.e. psychological, physical and sexual aggression; Fox et al., 2015; Levenson & Grady, 2016; Levenson et al., 2014). There is also evidence of a relationship between ACEs and the risk of “dual harm” (Carr et al., 2020). Dual harm refers to those that have both caused harm to the self and harm to others (O’Donnell et al., 2015; Shafti et al., 2021; Slade, 2018). This evidence raises the question of whether there is a common pathway between ACEs and both harm to the self and harm to others. One of the most at-risk populations for dual harm are those located in custodial settings (Dixon-Gordon et al., 2012). Notably, for the research reported here, those with sexual convictions are at a higher risk of suicidality than those who received non-sexual, non-violent convictions (Gullotta et al., 2021).
ACEs and Sexual Offending
ACEs are more common in individuals with a sexual conviction (Levenson et al., 2014) than in the general population (Kahn et al., 2021). However, current research findings provide a confusing and contradictory picture of whether ACEs create a later risk of harm towards others, including sexual offending. The debate has been most controversial when considering whether those who have experienced abuse, particularly sexual abuse, are at greater risk of sexually harmful behaviours as adults. Although victims of sexual abuse are at increased odds of becoming a perpetrator, the vast majority of those who have experienced sexual abuse do not go on to become perpetrators (Jespersen et al., 2009). In fact, those who experience childhood adversity can go on to live healthy, fulfilled lives (Bearer et al., 2015; Trickett & Kurtz, 2004), experiencing post-traumatic growth and increased resilience (Bonanno, 2004; Kwong & Hayes, 2017; Poole et al., 2017). Therefore, the relationship between ACEs and later harmful behaviours is complex and likely to be mediated by other psychosocial factors. Theoretically, two such factors are shame and self-compassion.
Shame
We view shame as a self-conscious and aversive emotion (Tangney & Dearing, 2002), where there is a negative self-cognition (Tracy & Robins, 2004) and/or a negative appraisal of the self in a relational context (DeYoung, 2015; Gilbert & Andrews, 1998), which elicits shame related behavioural responses (Nathanson, 1992). Shame is postulated to be “an evolved elaboration of a defensive behaviour in the service of interpersonal interactions” as it increases sensitivity to actual or potential social threats and triggers defensive actions in order to avoid social rejection or loss of social rank (Gilbert & McGuire, 1998, p. 120). Shame may trigger submissive or dominant defensive behaviours to maintain or regain social connection and rank (Gilbert, 2000; Gilbert & McGuire, 1998; Tangney & Dearing, 2002).
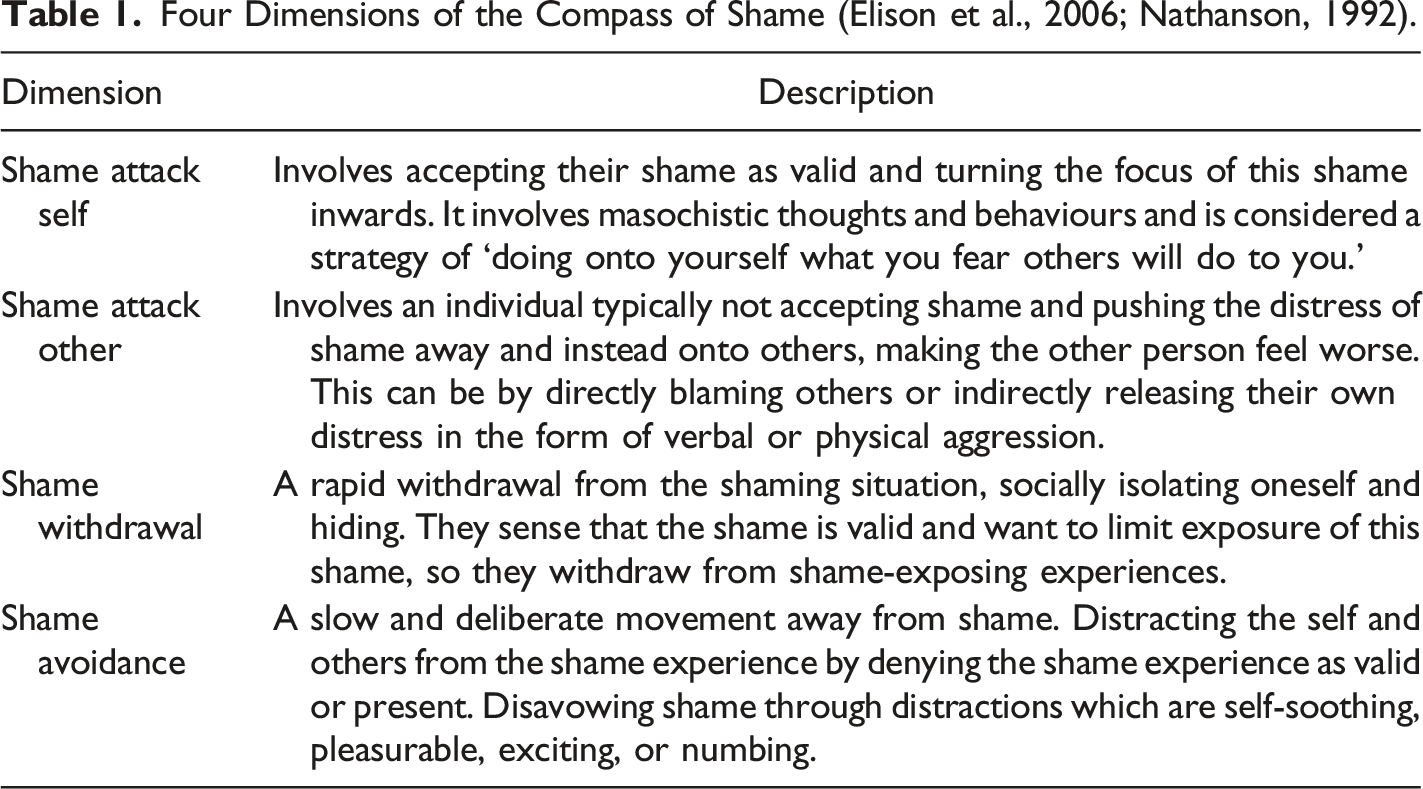
The compass of shame (Nathanson, 1992) provides a more detailed taxonomy of these defensive shame behaviours and highlights that shame can manifest in radically different behavioural phenotypes (see Figure 1). It describes four categories: withdrawal, avoidance, attack-self and attack-other (see Table 1). These behavioural manifestations ensure that “shame is reduced, ignored, or magnified, without addressing its source” (Elison et al., 2006, p. 222). The four categories in the compass can map onto the wider categories of submissive or dominant behaviours described previously (i.e. Gilbert, 2000; Gilbert & McGuire, 1998; Tangney & Dearing, 2002). For example, isolation to reduce further exposure to being shamed (i.e. shame-withdrawal) is a submissive response, whilst focusing on the flaws of others and denying one’s own (i.e. shame-attack-other) is a dominant response. Shame may also manifest as self-critical thoughts (i.e. attack-self) and increased substance use to numb the painful affect (i.e. shame-avoidance). The compass of shame model’s four behavioural manifestations of shame also share similarities with the overcompensation, avoidance and surrender strategies referred to in schema therapy as defences against shame (Young et al., 2003). Compass of shame (Elison et al., 2006; Nathanson, 1992). Four Dimensions of the Compass of Shame (Elison et al., 2006; Nathanson, 1992).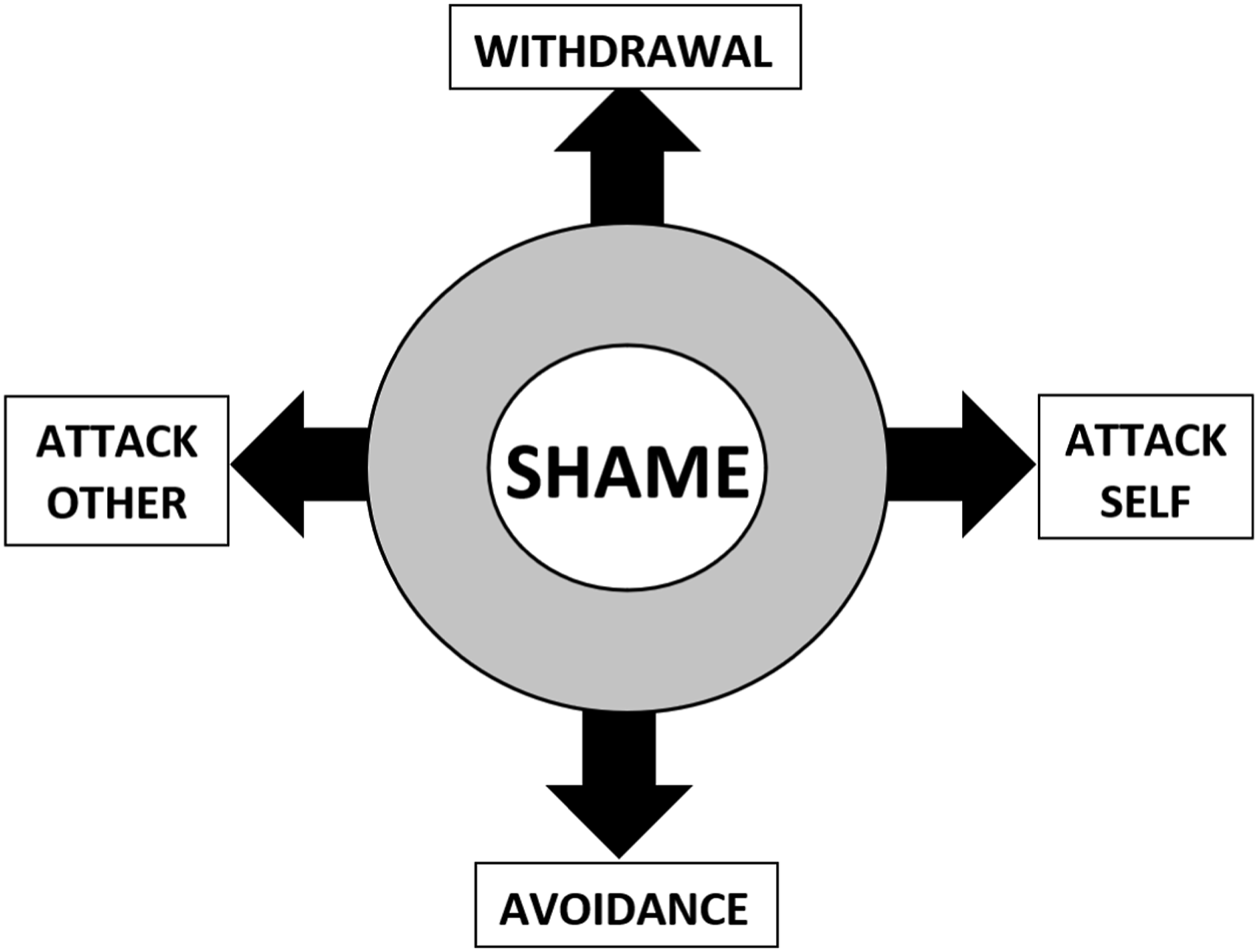
There is empirical support for each of the dimensions of the compass. Attack-self behavioural manifestations are reflected in research that associates shame with self-criticism, self-blaming (Castilho et al., 2017; Gilbert et al., 2004), pessimism (Lundberg et al., 2009), and self-objectification (e.g. seeing the self as an object to be used by others) (Miner-Rubino et al., 2002). The avoidance-based manifestations are reflected in research that associates shame with substance use, denial of responsibility, risky behaviours, and avoidance of situations that could result in failure (Dearing et al., 2005; Dunkley et al., 2003; Patock-Peckham et al., 2018; Stuewig et al., 2015). Withdrawal-based behavioural manifestations are reflected in research that found self-critics were less connected to others, did not find interacting with others pleasurable (Zuroff et al., 1999) and perceived others to be critical of them and less supportive (Dunkley et al., 2003). The attack-other behavioural manifestations are reflected in research that associated shame with anger and rage (Hejdenberg & Andrews, 2011; Keene & Epps, 2016; Tangney et al., 1996; Wright et al., 2008), blaming of others (Stuewig et al., 2010), narcissism (Keene & Epps, 2016; Morrison, 1989; Wurmser, 1987) and defensive ‘splitting’ (Gramzow & Tangney, 1992). For a more comprehensive description of the compass of shame, see Elison et al. (2006) and Nathanson (1992).
We acknowledge conceptual confusion between shame and other associated emotions, which is an area that continues to be debated. Despite a greater consensus on the distinction between shame and guilt (Tangney & Dearing, 2002), shame and terms such as humiliation are still being debated. Here, we consider shame as an emotion that can manifest in different behavioural responses, including attacking the other (Elison et al., 2006; Nathanson, 1992), and therefore we consider humiliation, as commonly described by others, as a variation of shame (DeYoung, 2015; Elison & Harter, 2007; Herman, 2014; Morrison, 2014; Nathanson, 1992). This fits with the compass of shame model’s understanding of shame (Elison et al., 2006; Nathanson, 1992) and Gilbert’s (2018) recognition that aggressive behaviour cannot distinguish shame from humiliation, as it can also be a defence against shame.
The compass highlights behavioural elements of shame that may form pathways from ACEs to harm, either by themselves or in combination. For example, harm to self may be through shame-attack-self, and harm to others may be through the shame-attack-other pathway.
Shame and Self-Harm
There is empirical support for a relationship between ACEs and shame (Karan et al., 2014; Messman-Moore & Coates, 2007) and shame with harm to self (Schoenleber et al., 2014; Xavier et al., 2016) in a variety of populations. More specifically, there is also evidence for a link between two behavioural pathways and self-harm, namely, attack-self and avoidance (Elison et al., 2006; Schalkwijk et al., 2016). Finally, there is also some initial evidence of shame mediating the relationship between ACEs and self-harm in forensic and community populations (Garbutt et al., 2022).
Shame and Psychological and Physical Harm to Others
There is also empirical support for the link between shame and increased risk of psychological and physical harm to others (Aslund et al., 2009; Gold et al., 2011; Harper et al., 2005; Kivisto et al., 2011). However, there remains inconsistency in this research, with other studies finding shame either has no relationship to harming behaviours towards others (Tangney et al., 2011) or inhibits delinquency (Spruit et al., 2016). A potential reason for these discrepancies may be due to different behavioural manifestations of shame being measured. For example, one study found that whilst shame-proneness had no impact on recidivism, a defensive and avoidant shame response increased recidivism (Tangney et al., 2014). Similarly, findings have been inconsistent when studies have investigated shame as a partial mediator between ACEs and harm to others, with some confirming shame as a partial mediator (Gold et al., 2011; Kim et al., 2009) and others finding no mediating relationship (Keene & Epps, 2016). Most recently, a large-scale study indicated that this inconsistency is because shame’s capacity to increase or decrease the risk of harm to others is influenced by the dimension of shame (i.e. shame-attack-other, shame-withdrawal etc.) (Garbutt et al., 2022).
Shame and Sexually Harmful Behaviours
A dearth of research has explored the relationship between shame and sexually abusive behaviours. One study found that shame correlated positively with sexually coercive aggression (Kivisto et al., 2011). Two potential pathways from shame to sexual offending have been theorised. One hypothesised pathway involves the use of sex as a self-soothing strategy to reduce emotional distress associated with negative emotions (e.g. shame) (Cortoni & Marshall, 2001; Reid et al., 2009; Uvnäs-Moberg et al., 2014). A second hypothesised pathway is that shame may also increase the likelihood of sexual offending as a result of shame-prone individuals’ potential tendency to withdraw from meaningful connections with others (Gilbert, 2003), particularly as social isolation and not having an intimate or emotionally meaningful relationship are considered risk factors associated with sexual recidivism (e.g. Farrington, 2003; Hanson & Bussière, 1998; Hanson & Morton-Bourgon, 2005; Marshall, 2010; Ward et al., 2000).
Self-Compassion
Self-compassion may also have the capacity to act as a mediator in the relationship between ACEs and harm. Self-compassion is using compassion (e.g. the ability to be kind, caring and understanding towards the suffering and difficulties of others) but directed towards the self. Neff (2011) describes self-compassion as mindfully recognising our own suffering, our common humanity and being kind to ourselves. Previous research has indicated that those who have higher levels of ACEs tend to have lower levels of self-compassion (Tanaka et al., 2011; Vettese et al., 2011) and self-compassion has been found to reduce shame (Au et al., 2017; Gilbert & Procter, 2006) by soothing the “threat system” (Rockliff et al., 2008).
Self-Compassion and Self-Harm
There is evidence that those who engage in self-harming behaviours have lower levels of self-compassion than those who do not (Gregory et al., 2017). However, it is possible that for a sub-group of this population, the function of self-harm may be self-compassionate by temporarily relieving emotional distress rather than as a method of self-punishment (Klonsky et al., 2014).
Self-Compassion and Harm to Others
Self-compassion has been found to be negatively correlated with aggression (Barry et al., 2015). Limited research explores the link between self-compassion and sexual harm, though self-compassion has been found to correlate negatively with hypersexuality (Phillips et al., 2019). It is also noted that, similar to shame, there has been conflicting research about self-compassion and harm. For example, although self-compassion has been found to negatively correlate with harm to others, it has also been considered to increase risk of harm to others by reducing an individual’s ability to accept their ‘immoral behaviours’ (Wang et al., 2017).
Despite mixed findings, there has been increasing use of shame-focused psychological therapies in forensic populations, such as schema therapy (Young et al., 2003), and an increased focus on the use of Compassion Focussed Therapy (CFT; Gilbert & Procter, 2006), which specifically targets shame through the use of self-compassion (Gilbert, 2014).
Current Study
The research here aims to explore ACE, shame and self-compassion within a sample of individuals who have committed sexual offences. It explores whether ACEs, shame and self-compassion are associated with harm towards self and others and the role that shame and self-compassion have in mediating the relationship between ACEs and harm (Figure 2). Path model ACEs to harm.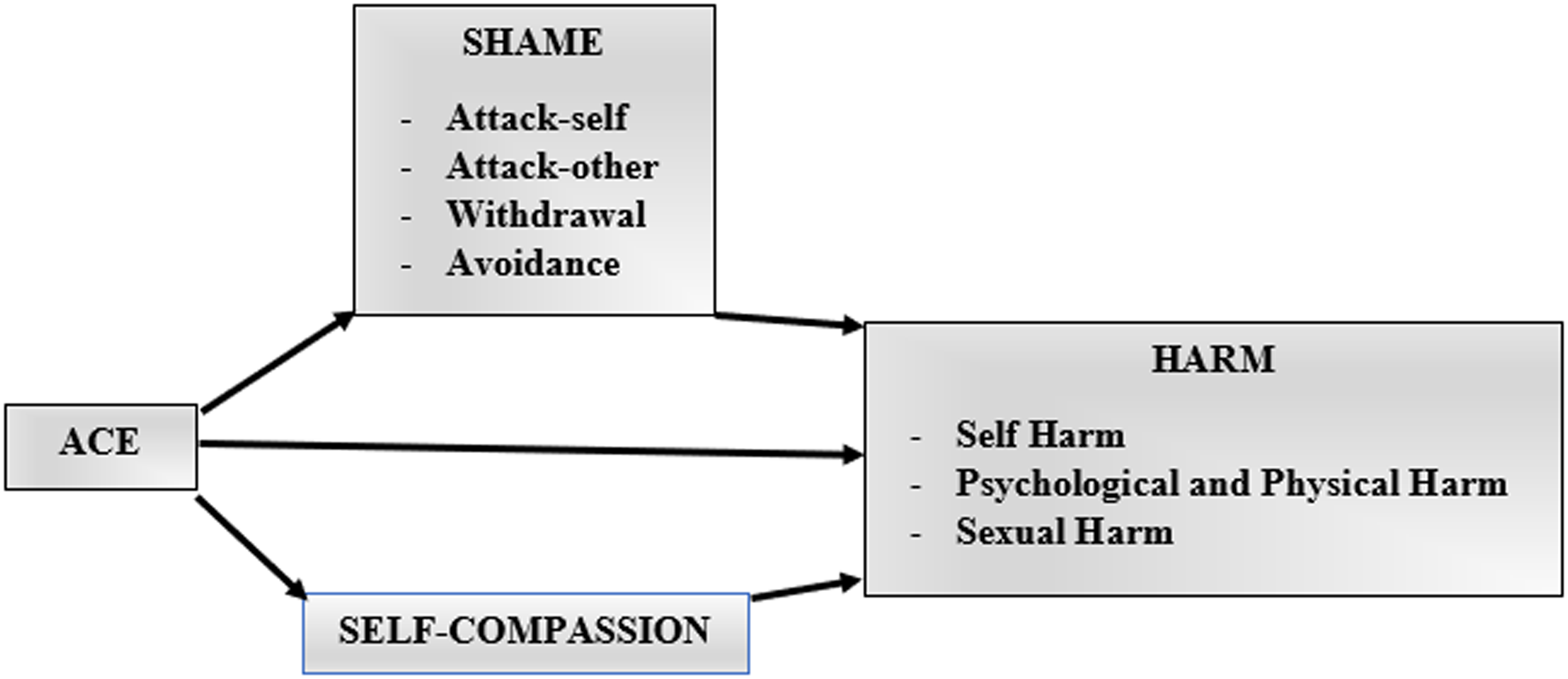
Method
In this section, we report how we determined our sample size, all data exclusion and manipulations (if any), and all measures in the study. This research adopts a cross-sectional design that involves current and retrospective data from a sample of adults who indicated that they had received a conviction for a sexual offence and were residing in a U.K. prison establishment at the time of data collection.
Participants
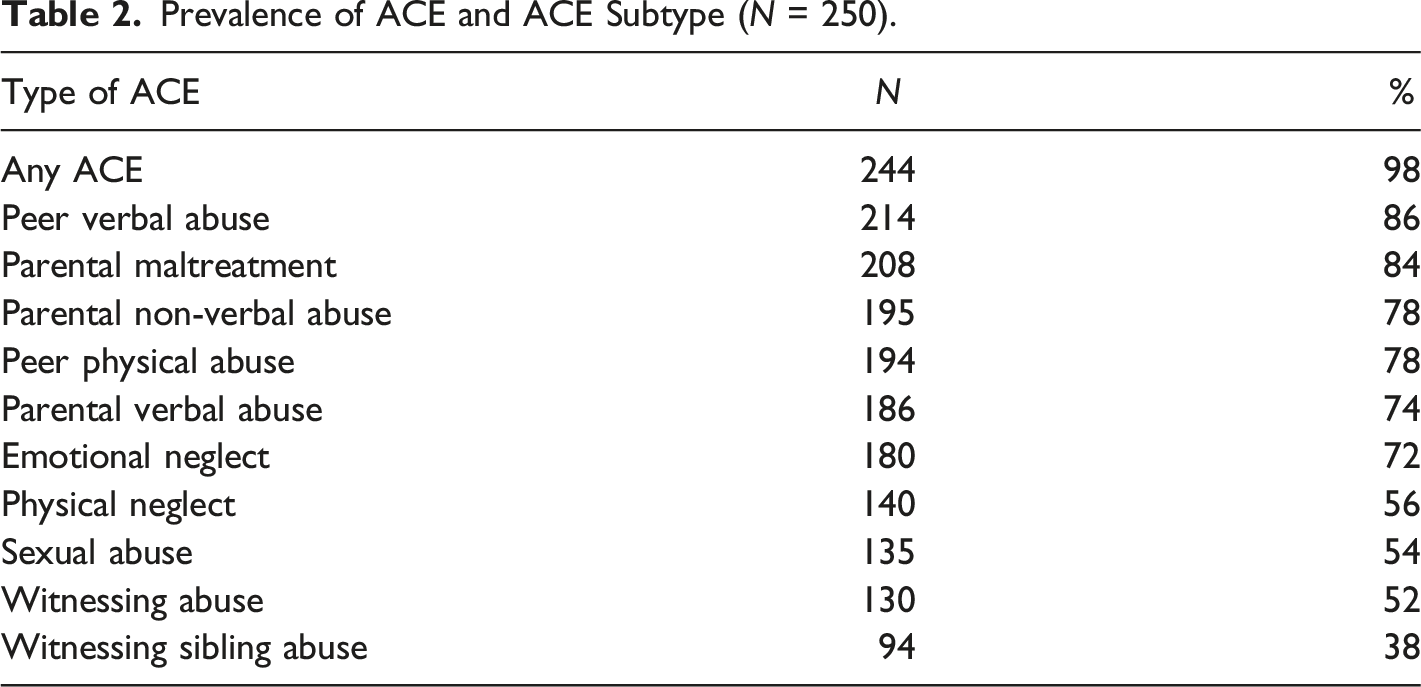
A purposive sample was gained (N = 250) from adults based within four prisons (three male establishments and one female establishment). All participants had a conviction for a sexual offence, with the majority having received convictions for contact sexual offences (87%). Participants indicated if they had committed contact or non-contact sexual offences. No further details were sought. The majority of the sample was male (n = 241), six were female, and a smaller sample of individuals were non-binary (n = 3). Participant data for the small number of both female and non-binary participants were retained to ensure data from underrepresented populations in sexual harm research were not excluded.
Prevalence of ACE and ACE Subtype (N = 250).
A priori power analysis indicated that a minimum sample of 146 was required to test the study hypotheses using regression analyses. Using a sensitivity power analysis, assuming 95% power and α = .05, the sample of 250 allowed for the detection of effect sizes corresponding to F2 = .08 (Cohen, 1992; Faul et al., 2007, 2009).
Measures
Data were collected through self-administered questionnaires, including demographic questions and items on ACEs, history of harm to self, history of harm to others, shame, and self-compassion. A summary of each measure is provided.
Adverse Childhood Experiences
The Maltreatment and Abuse Exposure Scale (MAES; Teicher & Parigger, 2015) was used to measure ACE. It consists of 52 questions designed to measure ten childhood adversity types. These include sexual abuse (familial and non-familial), parental physical maltreatment, parental verbal abuse, parental non-verbal abuse, witnessing physical abuse between parents, witnessing abuse towards a sibling, peer physical bullying, peer verbal abuse, physical neglect, and emotional neglect. Respondents indicated on a dichotomous scale whether they had experienced particular situations during childhood. The MAES provided a scaled cumulative ACE score. Ten ACE subtype scores can also be gained, and although not administered in this research, an additional feature of this measure is its ability to gain information about the developmental timing of abuse (MACES; Teicher & Parigger, 2015). Detailed scoring guidance can be gained from Teicher and Parigger (2015). The MAES has acceptable convergent validity (i.e. with the CTQ and ACE) and good test-retest reliability (Teicher & Parigger, 2015). A systematic review (Saini et al., 2019) established the MAES as one of the strongest ACE measures. Although a relatively new measure, it has also been validated in various populations, including community, clinical and forensic (Garbutt et al., 2022; Schalinski et al., 2016; Teicher & Parigger, 2015). Internal consistency was α = .95.
Harm to Self
The Self Harm Inventory (SHI; Sansone et al., 1998) measured harm inflicted on the self. It contains 22 items that assess self-harming behaviours on a dichotomous scale and are summed to give a total score. For example, have they ever intentionally ‘overdosed’, ‘burned yourself on purpose’, or ‘cut yourself on purpose.’ The SHI has been validated within clinical and nonclinical populations and is adept at measuring a broad continuum of self-destructive behaviours (Borschmann et al., 2012; Latimer et al., 2013). Internal consistency was α = .90.
Shame
The Compass of Shame Scale (CoSS; Elison et al., 2006) was used to measure shame. It describes 12 scenarios that typically evoke shame, and each is followed by four possible shame reactions to the scenario (e.g. attack-self, attack-other, withdrawal, avoidance). Respondents are asked how frequently they might react in that manner on a 5-point Likert scale ranging from never (0) to almost always (4). For example, a reaction to a rejection-based scenario could include “I avoid them,” “I soothe myself with distractions,” “I brood over my flaws,” or “I get angry with them.” Four scale scores are gained: attack self, withdrawal, attack other, and avoidance. The CoSS has been validated in a range of populations, including community, clinical and forensic (Dyer et al., 2017; Elison et al., 2006; Garbutt et al., 2022; Reid et al., 2009; Schalkwijk et al., 2016; Vagos et al., 2019). See Elison et al. (2006) for further details of this scale. The internal consistency for each scale was: Attack-self: α = .93, Attack-other: α = .93, Withdrawal: α = .93, and Avoidance: α = .80.
Self-Compassion
The Self Compassion Scale (SCS) - attitude subscale (Neff, 2003) was used to measure self-compassion. A six-factor model was initially proposed. However, greater support has been given to a two-factor model within the SCS, with a positive component reflecting a self-compassionate attitude and a negative component reflecting a self-critical scale (Costa et al., 2015). Of the 26 items of the SCS, thirteen reflect the self-compassionate attitude component; as such, only these items were administered. These items ask the respondents how frequently they act certain ways towards themselves. For example, ‘I’m kind to myself when I’m experiencing suffering,’ ‘I’m tolerant of my own flaws and inadequacies’ and ‘I try to be loving towards myself when I’m feeling emotional pain.’ Responses are given on a 5-point Likert scale ranging from almost never (1) to almost always (5). The SCS is a well-established measure validated in various populations, including community, clinical and forensic (Costa et al., 2015; Garbutt et al., 2022; Morley et al., 2016). Internal consistency was α = .95.
Psychological and Physical Harm to Others
Two measures of harm to others were combined and revised to capture harmful (psychological and physical) behaviours towards others (e.g. direct and indirect). The Indirect Aggression Scale (aggressor version) (IAS; Forrest et al., 2005) is the first measure. It consists of 25 items measuring indirect aggression. The Severity of Violence Against Women Scale (SVAWS) and Severity of Violence Against Men Scale (SVAMS) (Marshall, 1992a; 1992b) each consist of 46 items (e.g. mild to serious violence). Although there are two measures reflective of the gender of the respondent, the items are consistent across both measures (e.g. SVAWS; SVAMS) when using a total perpetrator score. For consistency, the measure will be referred to as the Severity of Violence Against Others Scale (SVAOS). The sexual aggression items were also removed (six items), which left 40 items reflecting threats of harm and actual harm. Minor revisions were made to the final measure to increase accessibility (e.g. by changing the word ‘partner’ to ‘someone’) and reduce floor effects (Warren & Clarbour, 2009). Participants were asked how often they tended to behave in each of the ways specified, and responses were on a 5-point Likert scale ranging from never (0) to very often (4). Both have been validated in a range of populations (Anguiano-Carrasco & Vigil-Colet, 2011; Davis & Renzetti, 2022; Forrest et al., 2005; Garbutt et al., 2022; Marshall, 1992a, 1992b; Temple et al., 2010). Internal consistency of the IAS (α = .95) and SVAOS (α = .97) combined to create a measure of psychological and physical harm was α = .98.
Sexual Harm to Others
Sexually harmful behaviours were measured using the Sexual Strategies Scale (SSS) (Strang et al., 2013; Struckman-Johnson et al., 2003). It contains 22 dichotomous items that ask participants what strategies they have used to gain sex when the other person does not want to. The items capture tactics such as the use of enticement, verbal coercion/emotional manipulation, use of older age or authority, use of intoxication and threats or force. For this research, the wording was amended to gender-neutral terminology as the measure was based on themes identified from research exploring male and female sexually coercive behaviours (Struckman-Johnson et al., 2003). The SSS measure was developed to measure a range of sexually harmful behaviours, rather than convictions, and has gained empirical support in community and forensic populations (Garbutt et al., 2022; Strang et al., 2013; Struckman-Johnson et al., 2003; Testa et al., 2015). Internal consistency was α = .89.
Procedure
Permission was gained to access four prison establishments within the U.K. as part of a larger data collection procedure in 2017. These establishments hold individuals with a range of offence types, which includes those with sexual convictions. Therefore, we were unable to gain precise response rates solely from the sample with sexual convictions. An information sheet and consent form were provided to all residents within each prison establishment, and they were provided with a return envelope. Individuals who returned their completed consent forms were sent a blank research survey containing no identifying information, and a self-addressed return envelope was provided. Participants then returned their completed questionnaires anonymously. Participants were informed that engagement in the research was voluntary, did not connect to their current incarceration status and that no compensation was provided. Participants were also aware of how confidentiality would be maintained to increase their confidence that their completed questionnaire could not be linked to them and that their data would be anonymised and not identifiable. Ethical approval was gained from the U.K. Prison and Probation Service (HMPPS) and Nottingham Trent University ethics boards. The authors take responsibility for the integrity of the data, the accuracy of the data analyses and have made every effort to avoid inflating statistically significant results.
Method of Analysis
Data were analysed with JASP (Version 0.16.3) computer software. The data were analysed using a Pearson product-moment correlation to test the relationship between variables, a multiple regression to establish if ACE, shame and self-compassion explained the variance in harm and mediation analysis to test the path between ACE and harm and the mediators in this relationship (i.e. shame and self-compassion). Each mediation analysis had six predictor variables: ACE, Shame-Attack-Self, Shame-Withdrawal, Shame-Attack-Other, Shame-Avoidance, and Self-Compassion. Each mediation model includes one harm-based outcome variable (self-harm, psychological and physical harm, sexual harm).
Assumptions for Pearson product-moment correlation, Multiple Regression and Mediation Analysis were assessed prior to analyses. The sample of 250 provides a sufficiently large sample size. The variables were not highly correlated (e.g. > .9) or combinations of each other; therefore, the multicollinearity assumption was met. The Durbin-Watson test highlighted the independence of the residuals (<2), and the assumption of collinearity was met with all VIF values under 10 (Meyers, 1990) and all tolerance values greater than .2 (Menard, 1995). Only a small proportion (<4%) of outliers were identified, and following inspection of these, they were retained. Although not all assumptions were fully met (i.e. normality and homoscedasticity), the large sample size and resampling methods (i.e. bias-corrected bootstrapping with confidence intervals) minimise the impact of these deviations (Ahmad & Ismaeel, 2022; Efron & Tibshirani, 1986; Tabachnick & Fidell, 2014; Waternaux, 1976). JASP Pearson product-moment correlation and Multiple Regression data were resampled 500 times to gain 95% confidence intervals (Efron & Tibshirani, 1986). JASP mediation analysis was used to estimate the Path Models using a maximum likelihood method of estimation with means and intercepts estimated. Total, direct and indirect effects were tested using resampling methods (MacKinnon et al., 2004) with the bias-corrected bootstrap. The data was resampled 500 times to gain 95% confidence intervals. We chose an alpha level of .05 to test for statistical significance. There is considerable debate about how alpha levels should be adjusted in multivariate statistical analyses to balance the risks of type 1 and type 2 errors. In this case, our main analysis uses mediation analysis where both the overall model and individual relationships must reach significance to support our predictions, and following Rubin (2021) alpha adjustment is not appropriate.
Results
Descriptive Statistics
The models included a maximum of nine observed variables. These included ACE, shame (attack-self, attack-other, withdrawal, avoidance), self-compassion, self-harm, psychological and physical harm to others and sexual harm to others. The majority (n = 219) of the participants checked at least one item on the self-harm scale. Therefore, a high proportion of the sample could be considered a dual-harm sample. Ninety-six percent (n = 241) of the sample rated at least one item of the psychological and physical harm measure; however, a notably large proportion of the sample (n = 122) did not rate any items of the sexual harm measure despite all having convictions for sexual offences.
Means, Standard Deviations and t test Differences Between Participants With and Without Contact Sexual Offences.
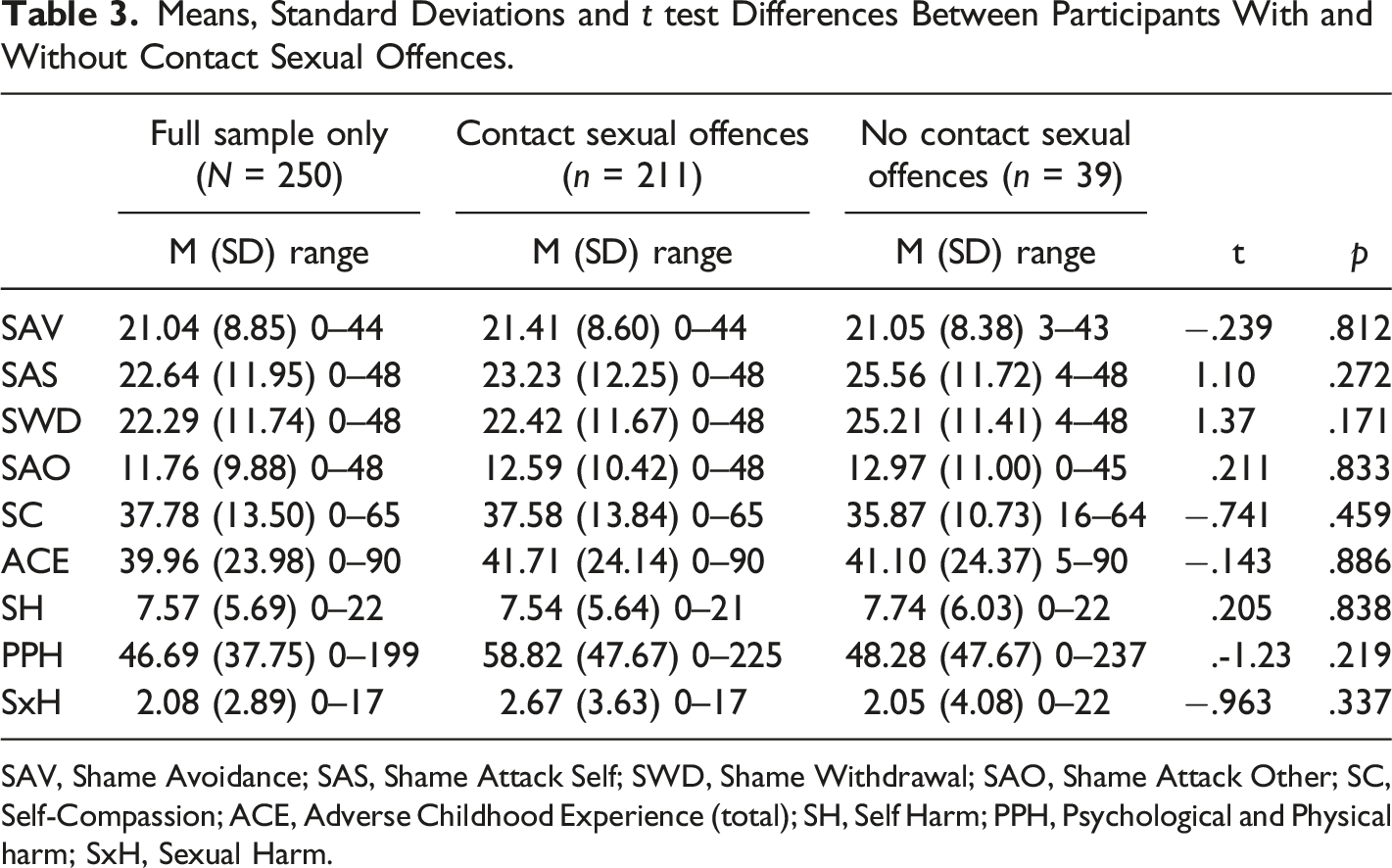
SAV, Shame Avoidance; SAS, Shame Attack Self; SWD, Shame Withdrawal; SAO, Shame Attack Other; SC, Self-Compassion; ACE, Adverse Childhood Experience (total); SH, Self Harm; PPH, Psychological and Physical harm; SxH, Sexual Harm.
Means and Standard Deviations for Male, Female and Non-binary Samples.
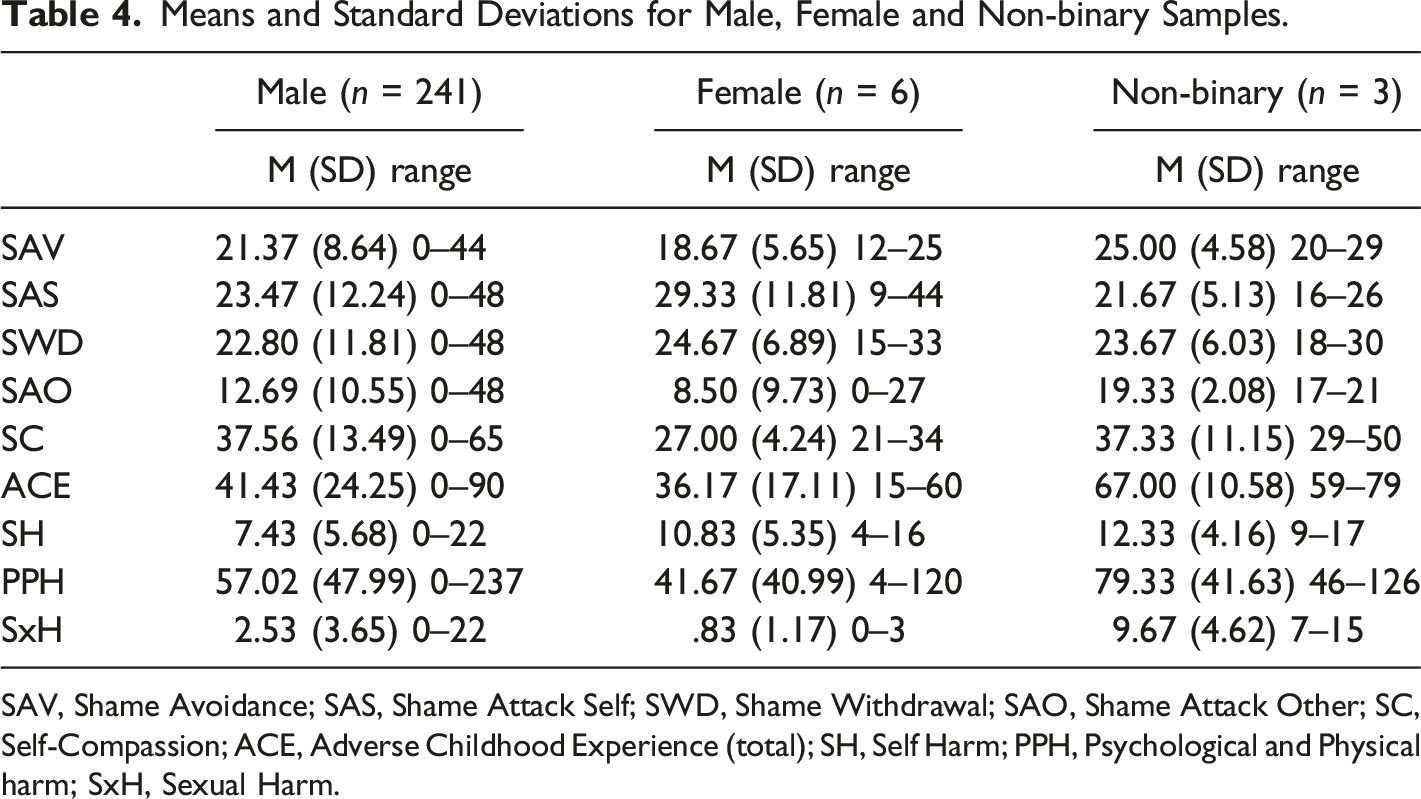
SAV, Shame Avoidance; SAS, Shame Attack Self; SWD, Shame Withdrawal; SAO, Shame Attack Other; SC, Self-Compassion; ACE, Adverse Childhood Experience (total); SH, Self Harm; PPH, Psychological and Physical harm; SxH, Sexual Harm.
Inferential Analysis
Intercorrelations Between Variables and 95% Confidence Intervals.
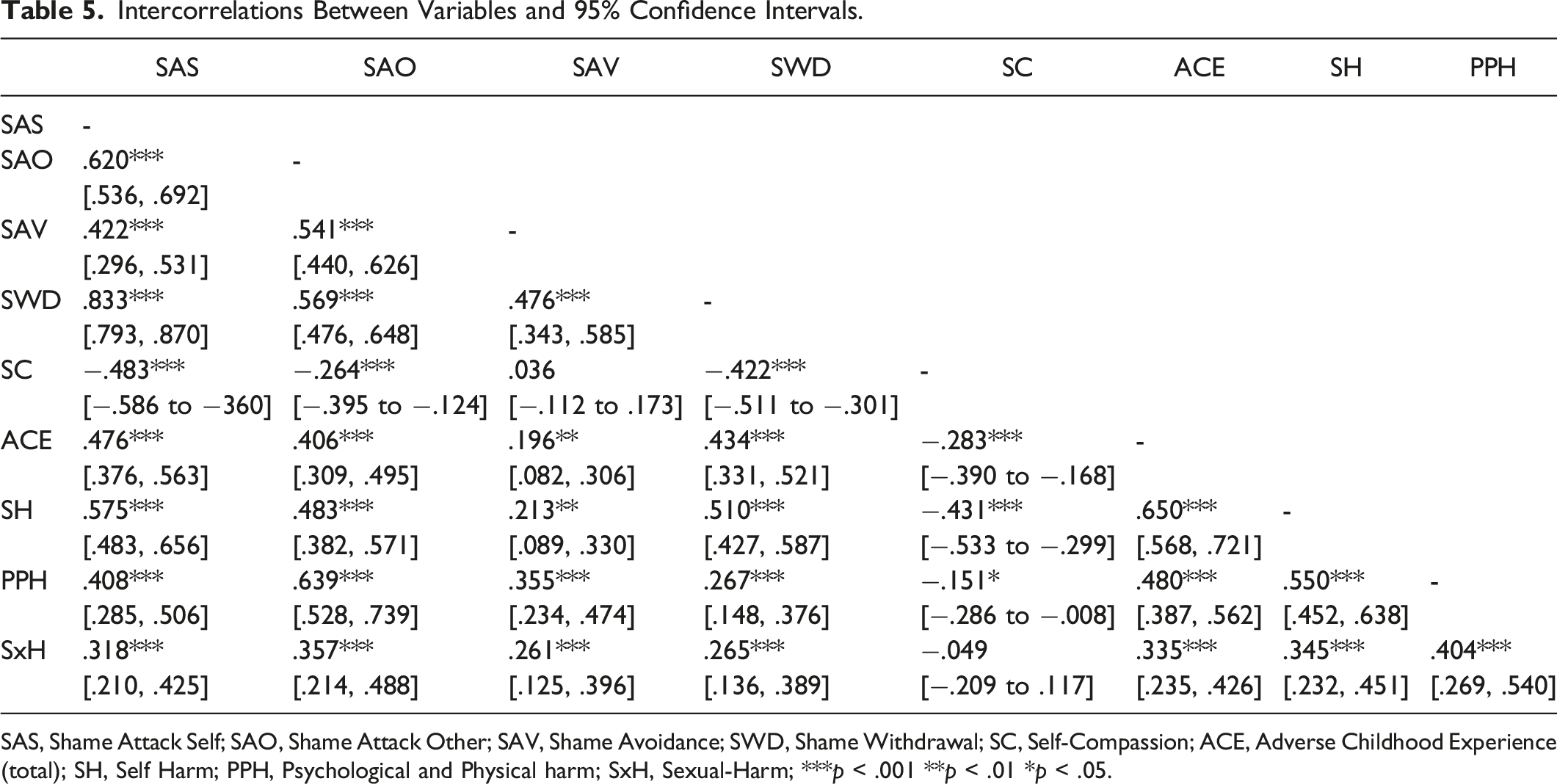
SAS, Shame Attack Self; SAO, Shame Attack Other; SAV, Shame Avoidance; SWD, Shame Withdrawal; SC, Self-Compassion; ACE, Adverse Childhood Experience (total); SH, Self Harm; PPH, Psychological and Physical harm; SxH, Sexual-Harm; ***p < .001 **p < .01 *p < .05.
ACE moderately correlated with three dimensions of shame (i.e. attack-self, attack-other, withdrawal) and correlated to a smaller degree with shame avoidance and self-compassion. Higher ACE was associated with higher levels of shame and lower levels of self-compassion. ACE also positively correlated with harm, with a strong correlation with self-harm and a moderate correlation with harm towards others (psychological, physical and sexual harm). All four dimensions of shame positively correlated with harm to self and others (psychological, physical and sexual harm). Self-compassion is negatively correlated with self-harm and, to a lesser degree, psychological and physical harm towards others. When a sub-group analysis was run on data from male participants only, the same relationships were observed.
Multiple Regression
Regression Associations Between Predictor Variables and Three Harm Types.
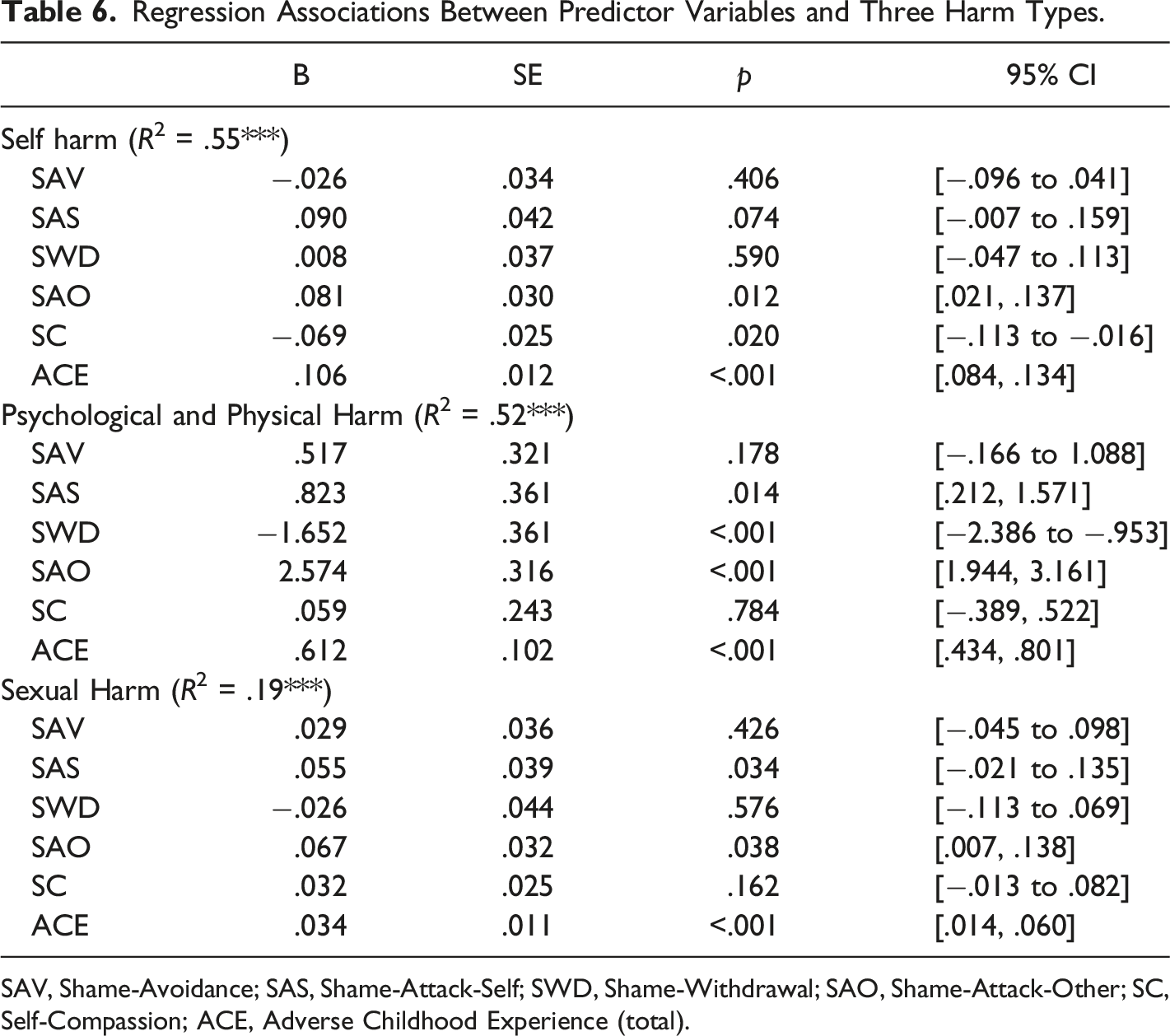
SAV, Shame-Avoidance; SAS, Shame-Attack-Self; SWD, Shame-Withdrawal; SAO, Shame-Attack-Other; SC, Self-Compassion; ACE, Adverse Childhood Experience (total).
ACE, shame and self-compassion predicted 55% of the self-harm variance (R2 = .55, F(6, 243) = 48.86, p < .001). Higher levels of ACE and shame-attack-other were associated with higher levels of self-harm. Higher levels of self-compassion were associated with lower self-harm. ACE, shame and self-compassion predicted 52% of the psychological and physical harm variance (R2 = .52, F(6, 243) = 43.82, p < .001). Higher levels of ACE, shame-attack-other and shame-attack-self are associated with higher levels of psychological and physical harm. Shame-withdrawal was negatively associated with psychological and physical harm to others. ACE, shame and self-compassion predicted 19% of the sexual harm variance (R2 = .19, F(6, 243) = 9.71, p < .001). Higher levels of ACE and shame-attack-other were associated with higher levels of sexual harm. When a sub-group analysis was run on data from male participants only, the same relationships were observed.
Mediation Analysis
Mediation Analysis Self Harm (R2 = .55).
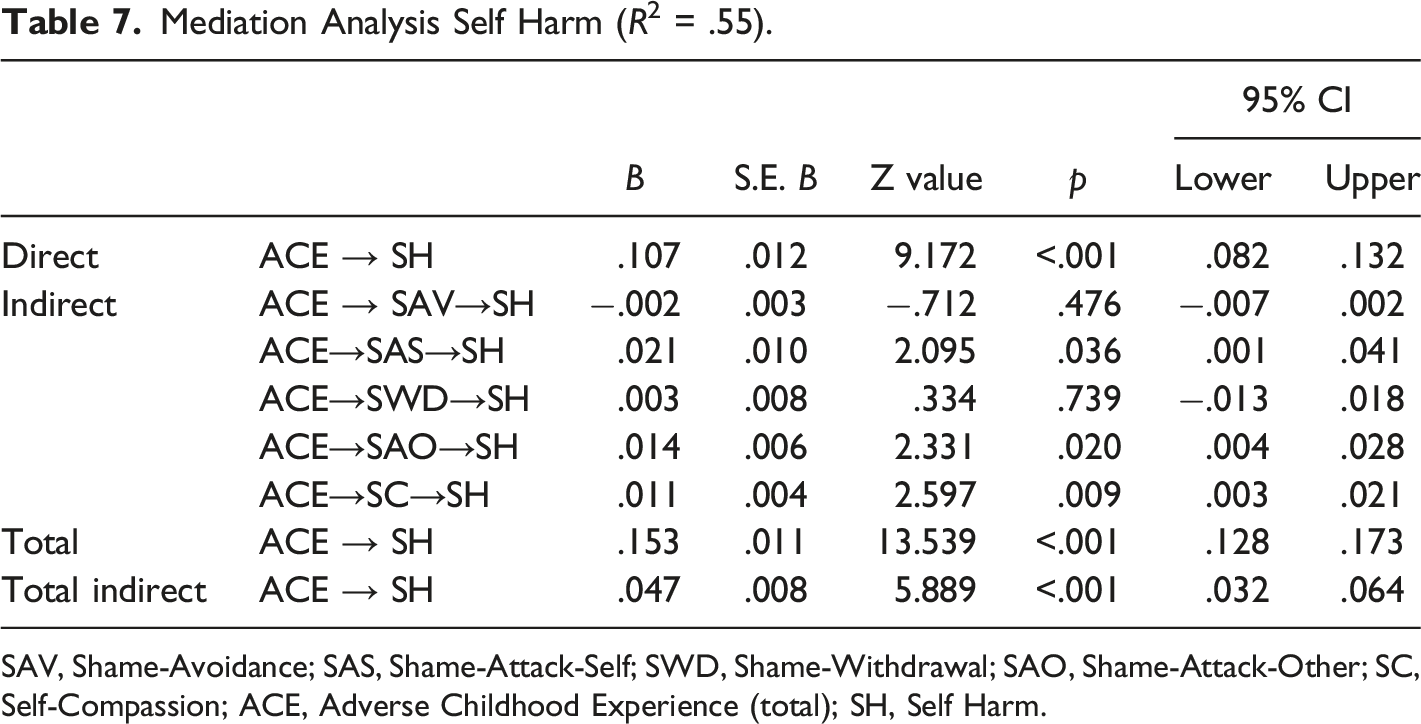
SAV, Shame-Avoidance; SAS, Shame-Attack-Self; SWD, Shame-Withdrawal; SAO, Shame-Attack-Other; SC, Self-Compassion; ACE, Adverse Childhood Experience (total); SH, Self Harm.
Mediation Analysis Psychological and Physical Harm (R2 = .52).
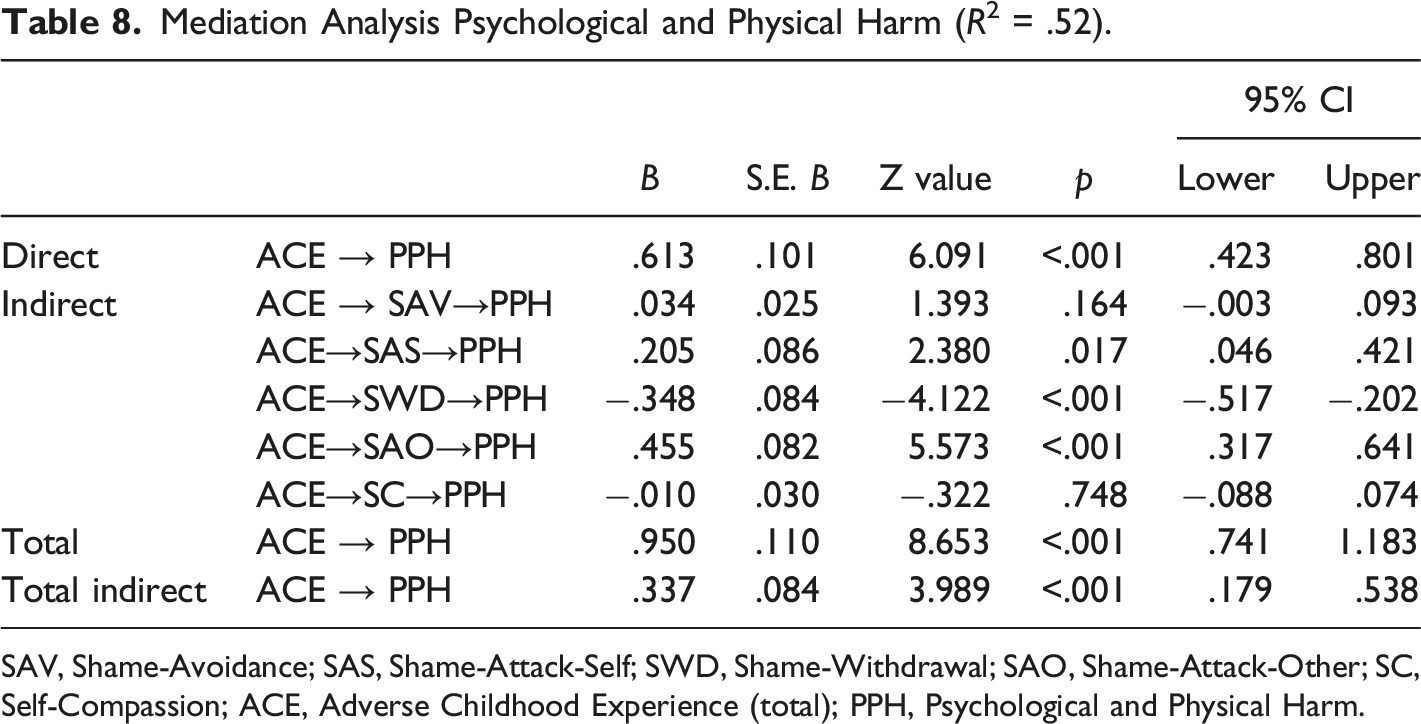
SAV, Shame-Avoidance; SAS, Shame-Attack-Self; SWD, Shame-Withdrawal; SAO, Shame-Attack-Other; SC, Self-Compassion; ACE, Adverse Childhood Experience (total); PPH, Psychological and Physical Harm.
Mediation Analysis Sexual Harm (R2 = .19).
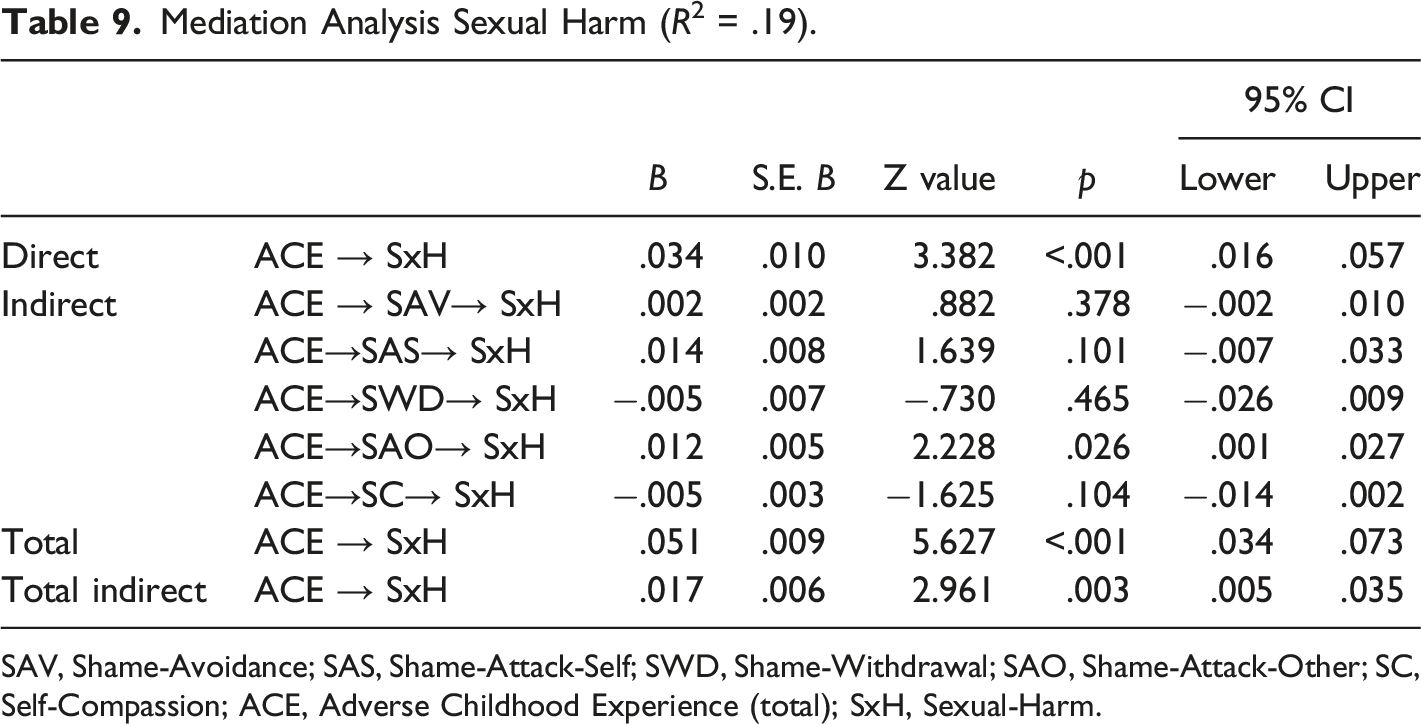
SAV, Shame-Avoidance; SAS, Shame-Attack-Self; SWD, Shame-Withdrawal; SAO, Shame-Attack-Other; SC, Self-Compassion; ACE, Adverse Childhood Experience (total); SxH, Sexual-Harm.
There was a significant direct relationship between ACEs and self-harm (B = .107). Shame-attack-self (B = .021), shame-attack-other (B = .014), and self-compassion (B = .011) were partial mediators in the relationship between ACEs and self-harm. Higher levels of ACE, shame-attack-self, shame-attack-other and self-compassion were associated with higher levels of self-harm. The total indirect effect (B = .047) contributed to the total effect (B = .15) of ACEs on the variance in self-harm. These associations were the same for the male-only sub-group analysis.
There was a significant direct relationship between ACEs and psychological and physical harm (B = .613). Shame-attack-self (B = .205), shame-attack-other (B = .455) and shame-withdrawal (B = −.348) were partial mediators in the relationship between ACEs and psychological and physical harm. Higher levels of ACE, shame-attack-self and shame-attack-other were associated with higher levels of psychological and physical harm. Higher levels of Shame-withdrawal associated with lower levels of psychological and physical harm. The total indirect effect (B = .337) contributed to the total effect (B = .95) of ACEs on the variance in psychological and physical harm. These associations were the same for the male-only sub-group analysis.
There was a significant direct relationship between ACEs and sexual harm (B = .034), and a total indirect effect (B = .017) contributed to the total effect (B = .051) of ACEs on the variance in sexual harm. Shame-attack-other (B = .012) was a partial mediator between ACE and sexual harm. Higher levels of ACE and shame-attack-other were associated with higher levels of sexual harm. These associations were the same for the male-only sub-group analysis.
Discussion
This research investigated pathways between ACE, different manifestations of shame, self-compassion and harmful behaviours in a sample of individuals who have committed sexual offences. The findings support the central prediction that ACE, shame and self-compassion are related to three forms of harm: harm to self, psychological and physical harm, and sexual harm. They also support the prediction that shame and self-compassion partially mediate the relationship between ACEs and harm. Finally, the research also supports the proposition that the direct and mediating role of shame can vary by the behavioural manifestation of shame. For example, shame that manifests as attack-other was associated with increased psychological and physical harm, whilst shame that manifests as withdrawal was associated with decreased psychological and physical harm. The findings contribute to our understanding of dual harm (Slade, 2018).
There was variation between the models for each form of harm at the level of different manifestations of shame. For self-harm, ACE, shame (attack-other) and self-compassion had a direct relationship with self-harm and explained over half of the variance. Shame that manifested as attack-other also partially mediated the relationship between ACEs and self-harm. These findings reflect previous research within forensic and community populations (Garbutt et al., 2022) and clarify the potential path from ACEs to self-harming behaviour. Surprisingly, shame that manifests as self-attack did not present as strongly associated with self-harm. However, it was a significant partial mediator between ACE and self-harm. This may reflect the various functions of self-harming behaviours, including the potential for self-harm to function as a way to soothe and gain relief (Klonsky et al., 2014) rather than solely causing direct harm to the self. The effect of the shame-attack-other manifestation on self-harm may reflect the notion that custodial professionals can experience some individuals who self-harm in prison as causing harm to those attending to them as well as themselves (Ireland & Quinn, 2007). This may be a result of the distress of shame being externalised as a way to soothe (i.e. reducing internalised distress) and may shine some light on the population referred to as those that “dual harm” (Slade, 2018).
For physical and psychological harm to others, higher levels of ACE and shame that manifests as attack-other and attack-self had the potential to increase harm, whilst shame that manifests as withdrawal had the potential to reduce harm. This opposing influence of shame depending on the manifestation of shame is an interesting finding and sheds further light on the conflicting findings in past research that have generally used a less complex conceptualisation of shame and not recognised it can manifest in different ways, similar to other emotions (e.g. fear can manifest as either fight, flight, freeze, or appease). Given this finding, future research would benefit from acknowledging the complexity of shame.
The model explained a lower proportion of the variance in sexually harmful behaviours compared to self-harm and psychological and physical harm to others. However, the direction of the effect was similar in that ACEs and shame had the potential to increase harm. This research, however, also highlights some concerns as to the utility of the SSS. The SSS was specifically selected to focus on behaviours rather than unhealthy sexual attitudes. However, nearly half of the respondents did not rate any items within this measure despite having received sexual convictions. Now, this, in part, could be a result of those with non-contact sexual offences (e.g. internet offending) being less likely to rate on some of the items within this measure. However, there was no significant difference between contact and non-contact groups on this measure (e.g. mean). Therefore, it is likely that participants denied harmful sexual behaviour, even with the assurance of anonymity and confidentiality. Future research may benefit from exploring barriers to open completion of this measure (e.g. lack of insight, openness, denial, etc.) as it is possible shame, particularly when it manifests as shame-avoidance or shame-attack-other, reduced reporting of sexually transgressive behaviours.
Past research has considered self-compassion as an antidote to shame. In line with this, this research also found that self-compassion was negatively correlated with shame that manifests as attack-self, attack-other and withdrawal. Self-compassion may, therefore, be best considered a moderator of shame. Unexpectedly, whilst higher self-compassion was associated with lower self-harm, this effect was inverted when self-compassion mediated the effects of ACEs on self-harm (i.e. higher self-compassion associated with higher self-harm). Future research may benefit from considering the impact of self-compassion further. This may include considering in greater depth the function (i.e. punitive or soothing) of self-harm. Alternatively, there may be some value in using an alternative conceptualisation and measure of self-compassion.
Overall, these correlational findings provide support for the further investigation of interventions that reduce shame (e.g. trauma-focussed, schema therapy, etc.) and also interventions that specifically use self-compassion to reduce shame (i.e. compassion-focussed therapy) with those who experienced ACEs and that are at risk of self-harm and/or harm to others (e.g. forensic populations). One of the most recent therapeutic approaches used within forensic populations, which has been gaining increasing interest, is Compassion-Focused Therapy (CFT; Gilbert & Procter, 2006). Whilst research into the application of CFT to forensic populations is still in its infancy, it has gained greater traction (e.g. Kolts & Gilbert, 2018; Taylor, 2017), including with those who have committed sexual offences (e.g. Taylor et al., 2020).
Limitations
This research has provided valuable insight into the association of ACEs with later harm. It also provides cross-sectional evidence that is consistent with a mediating role for shame and self-compassion. However, this research does have some limitations that would benefit from being addressed in replication studies. Firstly, it is difficult to evidence temporal relationships due to the concurrent measurement of variables, and therefore, causation can not be assumed. Secondly, the research uses retrospective measures of ACE, which may increase the potential for ACEs to be misremembered (Hardt & Rutter, 2004; Newbury et al., 2018). However, prospective measures have also similarly received criticism (Newbury et al., 2018). Thirdly, as well as the inherent difficulties associated with self-report measures, caution is warranted with the sexual harm measure. Either adaptations or alternative methods, including official data, should be considered in future research. More details about the nature of the offences would have also been useful, rather than solely establishing if the sexual offences were contact or non-contact. Similarly, alternative measures and conceptualisations of self-compassion may be beneficial. Fourthly, the difficulties in establishing a precise response rate may have had implications for how representative the sample was of the population of interest. Finally, although the sample is often an understudied population, the sample lacks diversity.
Future Directions
Our research would benefit from being replicated to further test the validity and generalisability of these findings and more directly explore the potential causal relationships. Future research would benefit from more temporally sensitive analyses, more robust measures of sexual harm and potentially alternative ways of measuring self-compassion. Future research would also benefit from a more sensitive exploration of the relationship between the different manifestations of shame and the various forms of sexual harm (i.e. more detailed in terms of the nature and victim type) and the different functions of self-harm.
Implications for Practice
ACEs are associated with shame and self-compassion, and shame and self-compassion may mediate the relationship between ACEs and harm. However, shame and self-compassion may develop from experiences beyond childhood, and this research highlights, through shame and self-compassion’s direct relationship to harm, and not solely mediating impact, that shame and self-compassion may be important in explaining the variance in later harm. This research, therefore, not only highlights the potential importance of targeting shame and self-compassion in children who experience adversity but also reducing the impact of other shaming experiences in later life. This could include shame developed from being the victim of abuse in adulthood, but also shame elicited from the justice system’s response to perpetrators of harm prior to sentencing (e.g. police, court proceedings), during the sentence (e.g. prison, probation, etc.) and when being reintegrated into society. Therefore, as well as developing and testing interventions to address shame for victims of ACEs and later abuse/adversity, further consideration should be made to the wider systems and procedures designed to punish, rehabilitate and reintegrate those that have inflicted harm on others if the intention is to reduce risk of harm in the future. If systems increase shame (e.g. shame-attack-self, shame-attack-other), they may inadvertently increase the risk of recidivism in custody and the community.
Footnotes
Author Contributions
K.G., as the main author, contributed to all aspects of the study from conception/design, through to acquisition/analysis/interpretation, and finally drafting and critically revising the manuscript. M.R. and M.G. contributed to research design, interpretation of the data analysis, and critical revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.