
Abstract
Self-harm, suicide, and harm inflicted on others (e.g., victimization) remain key areas of public concern. Past research has explored the link between adverse childhood experiences (ACEs) and later self-harming and offending behaviors. However, research has not fully explored the interplay between ACEs and modifiable psychological factors, such as shame and self-compassion, that could be targeted to reduce the risk of harm and increase resilience and capacity for post-traumatic growth. The present study explored the relationship between ACEs, harm, shame, and self-compassion. A total of 1,111 adults participated. Approximately 49% were female, 45% male, and 2% nonbinary. Just under a third of the sample were incarcerated. We adopted a cross-sectional survey design and included current and retrospective data. The relationship between the variables was analyzed using Pearson product-moment correlation, and structural equation modeling was applied to explore the potential psychological pathways of causation. The model predicted just under 50% of the harm to self (i.e., self-harm) variance and just over a third (35%) of the harm to others (i.e., psychological and physical aggression) variance. ACEs, shame, and self-compassion had varying roles in mediating the relationship between ACEs and harm. The study increases our understanding of modifiable causal pathways between ACEs and later harming behaviors. Additionally, it indicates the importance of understanding the different dimensions of shame when considering ways to reduce the potential long-term negative consequences of ACEs.
Introduction
Harm inflicted on the self (e.g., self-harm and suicide) and harm inflicted on others (e.g., psychological and physical harm/aggression) are serious societal concerns. They have consequences that span individuals, families, communities, and society as a whole. For example, within the United Kingdom, each year, there are approximately 1.8 million violent offences (Office for National Statistics, 2022a), 5500 deaths by suicide (10.5 deaths per 100,000), and self-harm incidents are much higher, though harder to record reliably (Office for National Statistics, 2022b). One of the most at-risk populations for harm (i.e., self-harm, aggression, and dual harm) are those located in custodial settings (Dixon-Gordon et al., 2012; Slade, 2018). For example, approximately 80 incidents of suicide (90 deaths per 100,000), 53,000 incidents of self-harm, and 20,000 assaults are reported annually in the UK prison system (Ministry of Justice, 2022). This occurrence of high rates of suicide and self-harm in a group where aggression and harm to others are also high has been described as “dual harm” (Slade, 2018). A recent systematic review of 123 studies found evidence that aggression and self-harm are positively associated (O’Donnell et al., 2015).
Understanding factors that increase the likelihood of behaviors that inflict harm on the self and others (e.g., psychological and physical harm) has great value, particularly those that can be addressed in order to avoid the significant irreversible impact of self-harm, suicide, and harm to others. Alongside this, the phenomenon of dual harm also raises two important questions: do self-harm and harm to others share a common etiological pathway; and can interventions effectively address both self-harm and harm to others? A recent review (Shafti et al., 2021) suggests there is evidence of a common pathway and identifies a number of candidate processes that likely interact, including distal factors such as adverse childhood events (ACEs) and personality and proximal factors such as cognitive schemas, emotional dysregulation in the context of negative emotion, and the immediate social context. We report here a model of harm that combines distal and proximal factors derived from theories of shame and self-compassion. This model seeks to aid our understanding of pathways from ACEs to self-harm and harm to others, and potentially further our understanding of dual harm. For the purposes of our research, “harm to self” used synonymously with “self-harm” is defined as self-destructive behaviors that cause damage or harm to oneself (Sansone et al., 1998) regardless of underlying motivation (NICE, 2012). “Harm to others” used synonymously with “aggressive behavior” refers to “any behavior directed toward another individual that is carried out with the proximate (immediate) intent to cause harm” and the belief that the behavior will harm a target who was motivated to avoid harm (Anderson & Bushman, 2002, p. 28). Our research includes both psychological and physical aggression and harm. Should such a model have empirical support, it would lend itself to potential interventions for harm based on the developing body of shame focussed psychological therapies such as compassion focussed therapy (Gilbert & Procter, 2006) and schema therapy (Young et al., 2003).
The model we tested starts with adverse childhood experiences (ACEs) acting as a distal cause of harm. ACEs describe various negative events, including sexual, emotional, psychological, and physical abuse, neglect, loss, and illness (Vachon et al., 2015). A cumulative effect has also been identified, with the greater number of ACEs increasing the risk of negative life sequelae, including self-harm (Hughes et al., 2017; Liu et al., 2018) and harm to others (Fox et al., 2015).
Although ACEs are associated with later harm inflicted on the self and others, it is also recognized that some children transcend the abuse they experienced and go on to live a healthy fulfilled life (Bearer et al., 2015; Trickett & Kurtz, 2004). In fact, there can be post-traumatic growth and increased resilience (Bonanno, 2004; Kwong & Hayes, 2017; Poole et al., 2017). Therefore, negative sequelae associated with ACEs, such as harm inflicted on the self (self-harm and suicide) and harm inflicted on others (e.g., psychological and physical harm), are potentially preventable.
The next part of our model is shame, which could account for the pathway from ACEs to harm. Adverse childhood experiences have been linked to higher levels of shame (Karan et al., 2014; Messman-Moore & Coates, 2007). We adopt an integrated conceptualization of shame that encompasses the affective, cognitive, relational, and behavioral elements of shame (see Garbutt, 2018, pp. 31–44, for further discussion). We view shame as a self-conscious and aversive emotion (Tangney & Dearing, 2002), where negative cognition is focused on the self (Tracy & Robins, 2004) and/or the negative evaluation of the self in a relational context (DeYoung, 2015; Gilbert & Andrews, 1998), which elicits shame-related behavioral responses (Nathanson, 1992).
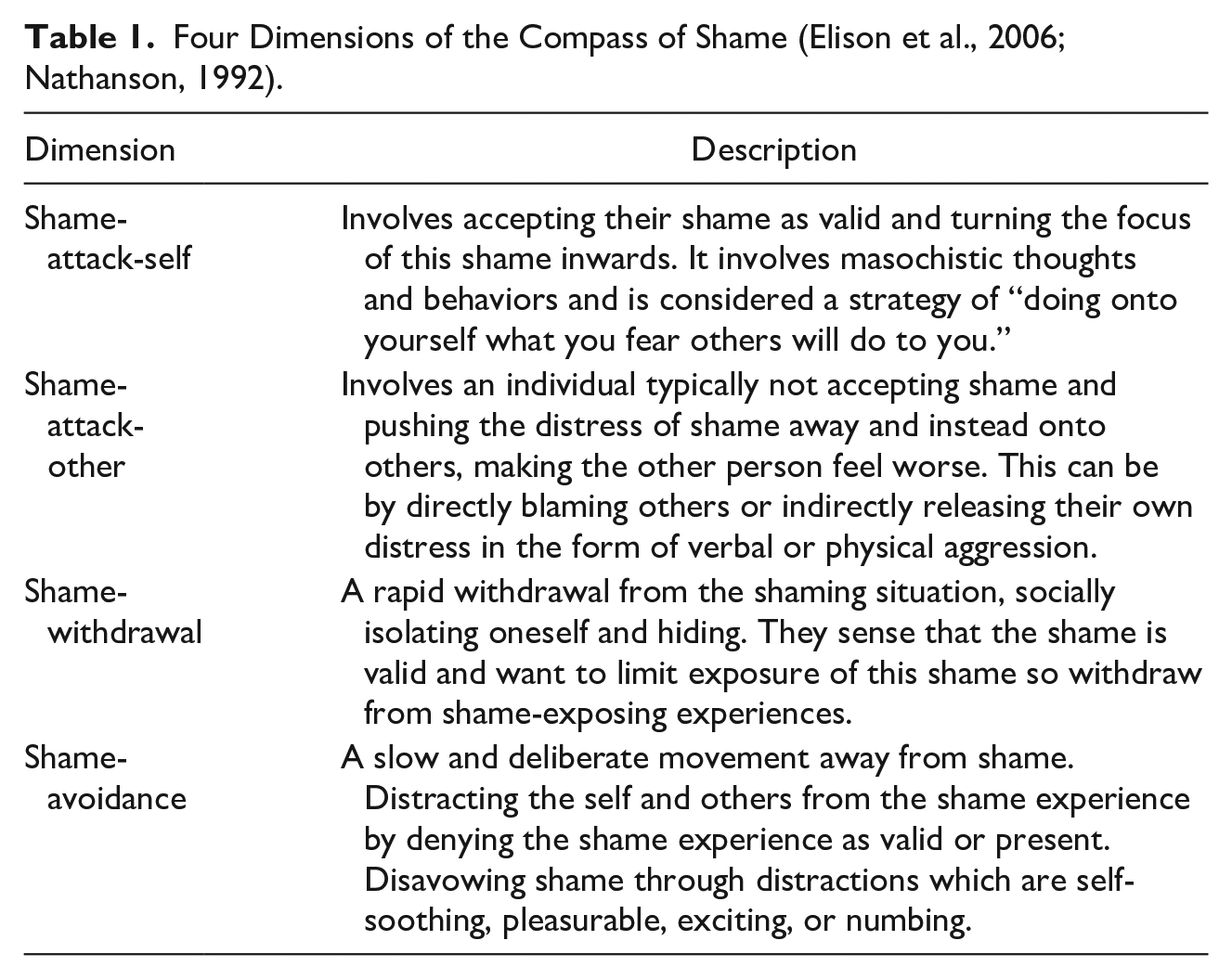
The compass of shame (Figure 1; Nathanson, 1992) provides a framework that helps conceptualize the relationship between shame and later sequelae, such as harm to self and others. In particular, the compass highlights behavioral elements of shame that may form proximal pathways to harm either by themselves or in combination (Table 1). For example, self-harm may be through shame-attack-self and shame-avoidance pathways, while harm to others may be through the shame-attack-other pathway. This framework highlights that shame can manifest differently, in the same way that fear can present as fight, flight, freeze, or fawn.
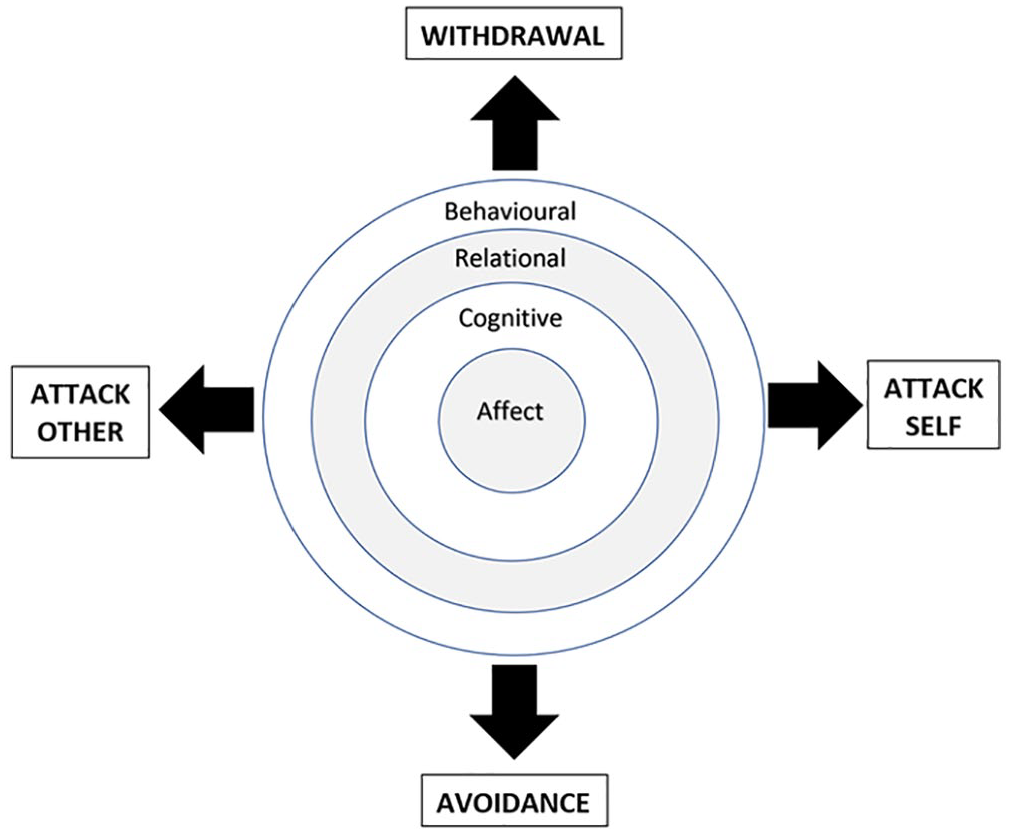
Integrated conceptualization of shame and compass of shame combined (Garbutt, 2018).
Four Dimensions of the Compass of Shame (Elison et al., 2006; Nathanson, 1992).
There is empirical support for a positive relationship between shame and self-harm (Schoenleber et al., 2014; Xavier et al., 2016). There is also evidence for a link between two specific behavioral pathways described in the compass of shame and self-harm: attack self and avoidance (Elison et al., 2006; Schalkwijk et al., 2016). Finally, there is some initial evidence for the full pathway connecting ACEs to self-harm via shame processes. A study of 94 adolescents found a relationship between emotional neglect and self-harm, with self-criticism partially mediating the relationship (Glassman et al., 2007).
There is also empirical support for the link between shame and risk of harm to others. Shame has been linked with physically aggressive behaviors (Aslund et al., 2009; Gold et al., 2011), psychologically aggressive behaviors (e.g., verbal aggression) (Harper et al., 2005; Kivisto et al., 2011), and recidivism (Hosser et al., 2008). However, findings in this literature have been inconsistent. Shame has also been found to either inhibit delinquency (Spruit et al., 2016) or as having no real relationship with harm to others (Tangney et al., 2011). One explanation for these discrepancies is that the relationship between shame and harm to others is mediated by the particular behavioral manifestation of shame at that time. For example, one study found that shame-proneness and negative self-appraisal had no impact on recidivism, while shame combined with a defensive shame response and behavioral avoidance increased recidivism (Tangney et al., 2014).
Contradictory findings have also been reported, with some studies identifying shame as a partial mediator between certain forms of ACE and harm to others (e.g., aggressive conflict, verbal and physical aggression, violent delinquency) (Gold et al., 2011; Kim et al., 2009; Kissee, 2012) and others finding no mediating relationship (Keene & Epps, 2016).
The final element of the model we investigate here is self-compassion—a psychological construct that describes the ability and willingness to mindfully recognize our own suffering, our common humanity, and to be kind to ourselves (Neff, 2011). Adverse childhood experiences may interrupt the development of self-compassion (Tanaka et al., 2011). In addition, self-compassion is thought to reduce shame because it has the potential to deactivate the threat system (Gilbert, 2010), buffer against negative affect triggered by a threat to the ego (Neff et al., 2007), and strengthen emotional resilience (Vettese et al., 2011).
Our proposition is that self-compassion is implicated in the pathway from ACEs to harm as a mediator and via a moderating effect on shame. Empirically there is evidence that those that engage in self-harming behaviors are found to have lower levels of self-compassion than those that do not (Gregory et al., 2017) and that self-compassion is negatively correlated with aggression (Barry et al., 2015). However, despite these findings, another study found that those with higher levels of self-compassion were less likely to accept their own “immoral behaviors” (Wang et al., 2017), which highlights some inconsistency in past research. Although self-compassion has been increasingly studied and explored in connection to shame, to the best of the authors’ knowledge, there do not appear to be any studies that have considered self-compassion as a mediator within the relationship between ACEs and harm.
The Current Research
In summary, the psychological mechanism connecting ACEs to later harm is not yet fully understood. One candidate mechanism with some empirical support is shame and its constituent elements, together with its potential “antidote” self-compassion. There is empirical support for these links, but this is patchwork in nature, and there still remain clear gaps in our understanding. This is particularly important given prevention is not always possible, and especially for those that have already experienced ACEs and are currently suffering from the psychological consequences. If modifiable psychological factors such as shame and self-compassion mediate the relationship between ACEs and harm to the self and others, then it provides treatment pathways to support those that are already experiencing the trajectory from ACEs to harm and those where prevention of childhood adversity is not successful.
We postulate that ACEs will be related to harming behaviors through the mediators of shame and self-compassion. There will also be a direct relationship between the variables (i.e., ACE, shame and self-compassion) and harm.
Method
We adopted a cross-sectional design and gained both current and retrospective data from a sample of adults from community and custodial settings.
Participants
Adults based in the community and within five prisons (four male establishments and one female establishment) were approached to take part in the study. A large purposive sample was gained (N = 1,111). One-third of the sample (n = 331) is from custodial settings. Of the total sample who were aged between 18 and 95 years of age, 45% were female, 49% were male, and 2% were nonbinary. Although a generally diverse sample, the majority of the sample were white British/Irish (74%), single (49%), and considered themselves Atheists (48%). Using a sensitivity power analysis, assuming 95% power and α = .05, the sample of 1,111 allowed for the detection of small effect sizes corresponding to F2 = 0.02 (Cohen, 1992; Faul et al., 2007, 2009).
Materials
Data was collected through a set of self-administered questionnaires, which included demographic questions and items on adverse childhood experiences, history of harm to self, history of harm to others, shame, and self-compassion. A summary of each measure is provided.
Adverse childhood experiences
ACEs were measured using the Maltreatment and Abuse Exposure Scale (MAES; Teicher & Parigger, 2015), which consists of 52 questions designed to measure exposure to 10 types of maltreatment in childhood. These include sexual abuse (familial and nonfamilial), parental verbal abuse, familial nonverbal emotional abuse, parental physical maltreatment, witnessing physical abuse between parents, witnessing abuse toward a sibling, peer verbal abuse and ostracism, peer physical bullying, emotional neglect, and physical neglect. Respondents were asked on a dichotomous scale whether they had experienced particular situations during their childhood. The MAES provided a scaled cumulative ACE score. Internal consistency was α = .94.
Harm to self
Harm inflicted on the self was measured using the Self Harm Inventory (Sansone et al., 1998), which is a 22-item measure that explores a range of self-harming behaviors on a dichotomous scale to gain a total score. For example, have they ever intentionally or on purpose: “overdosed,” “burned yourself on purpose,” or “cut yourself on purpose.” Internal consistency was α = .90.
Shame
Shame was measured using the Compass of Shame Scale (Elison et al., 2006), which included 12 scenarios that evoke shame (e.g., as an affect, cognition, and/or behavior). Each scenario is followed by four possible shame reactions to the scenario (e.g., withdrawal, avoidance, attack self, attack other). Participants were asked how frequently they react in that way on a 5-point Likert-type scale ranging from 0 = Never to 4 = Almost Always. Four scale scores were gained: attack self, attack other, withdrawal, and avoidance. The internal consistency for each were: Attack-self: α = .95, Attack-other: α = .91, Withdrawal: α = .92, and Avoidance: α = .72.
Self-compassion
Self-compassion was measured using the Self-Compassion Scale (SCS)—attitude subscale (Neff, 2003). Although a six-factor model was initially postulated, stronger support has been given to a two-factor model within the SCS, with a positive dimension reflecting a self-compassionate attitude and a negative dimension reflecting a self-critical scale (Costa et al., 2015). Of the 26 items of the SCS, 13 items reflected the self-compassionate attitude factor, and as such, only these items were selected. These items asked the respondent how frequently they acted in certain ways toward themselves. Responses were given on a 5-point Likert-type scale ranging from 1 = Almost Never to 5 = Almost Always. Internal consistency was α = .95.
Harm to others
Two measures of harm to others were combined and revised to capture both psychologically and physically harmful behaviors toward others (e.g., direct and indirect). The first of these measures is the Indirect Aggression Scale (aggressor version) (IAS; Forrest et al., 2005), which contained 25 items that measured indirect aggression. The Severity of Violence Against Women Scale (SVAWS) and Severity of Violence Against Men Scale (SVAMS) (Marshall, 1992a, 1992b) contained 46 items each. Although there are two measures reflective of the gender of the respondent, the items are consistent across both measures (e.g., SVAWS and SVAMS) when using a total perpetrator score. For ease of reference, the measure will therefore be referred to as the Severity of Violence Against Others Scale (SVAOS). The sexual aggression items were also removed (6 items), which left 40 items reflecting threats of harm and actual harm (i.e., psychological and physical harm only). Sexual aggression was considered, using an alternative measure, as part of a wider research project that is reported elsewhere (e.g., Garbutt, 2018; Garbutt et al., 2022). Minor revisions were made to the final measure to increase accessibility (e.g., the word “partner” was changed to “someone”) and reduce floor effects (Warren & Clarbour, 2009). Participants were asked how often they tended to behave in each of the ways specified, and responses were on a 5-point Likert-type scale ranging from 0 = never to 5 = very often. Internal consistency of the IAS (α = .95) and SVAOS (α = .97) combined to create a measure of psychological and physical harm was α = .98.
Procedure
Two data collection protocols were used to ensure questionnaires could be completed anonymously. Those in custodial settings were provided with paper copies of the questionnaire pack, and the community sample accessed these online through Qualtrics® (2018, Qualtrics, Provo, UT, USA). We advertised the research to all individuals in the custodial settings and within a number of locations (e.g., social media platforms, forums, university psychology research participation schemes, Listservs, etc.) in order to distribute within a range of community-based populations.
Method of Analysis
Data were analyzed with SPSS version 24 and AMOS version 24. Pearson product-moment correlation tested hypotheses focussed on the relationship between variables. Secondly, structural equation modeling tested hypotheses exploring the path between ACEs and harm and the mediators in this relationship. Assumptions for Pearson product-moment correlation and structural equation models were assessed prior to analyses. The assumptions were met for the self-harm model. However, a number of outliers were identified within the “harm to others” variable, and therefore, they were removed from the harm to others model. Analyses conducted after outliers were removed indicated excess skewness (1.25) for the “physical and psychological harm” variable. However, the large sample size (e.g., over 200) minimized the impact of this (Tabachnick & Fidell, 2014; Waternaux, 1976).
Structural equation model (SEM) approaches are appropriate for developing probabilistic causal models and analyzing mediating relationships between variables. SPSS and AMOS were used to estimate the SEMs using a maximum likelihood method of estimation with means and intercepts estimated. Total, direct, and indirect effects were tested using resampling methods (MacKinnon et al., 2004) with the bias-corrected bootstrap. The data was resampled 500 times to gain 95% confidence intervals. The χ2 to degrees of freedom ratio (CMIN/df; <5, nonsignificant), Comparative Fit Index (CFI, >.95; Bentler, 1990), and Root Mean Square Error of Approximation (RMSEA, <.08; Steiger, 1990) were used as measures of global fit. The χ2 measure is sensitive to sample size, with large samples (e.g., over 200) tending to indicate a significant probability level (Schumacker & Lomax, 2016). Given the large sample size within this study, models were not rejected if significant.
Results
Descriptive Statistics
The models included a maximum of eight observed variables. These included ACE, shame (attack-self, attack-other, withdrawal, avoidance), self-compassion, self-harm, and harm to others (i.e., psychological and physical). Of the total sample, 87% of the sample (n = 970) rated on both measures of harm (e.g., had positively indicated on at least 1 item of both the self-harm and harm to others measures). Within the sample, there was no notable difference (Cohens d = .06) between levels of self-harm when comparing those that had a conviction (n = 397, M = 8.45, SD = 6.09) with those that did not (n = 672, M = 8.17, SD = 2.51). The sample with convictions had higher levels of ACEs (n = 397, M = 42.81, SD = 24.08) when compared to those that did not (n = 672, M = 34.67, SD = 20.89); however, the effect size was small (Cohens d = .361).
Inferential Analysis
The Pearson product-moment correlation coefficients (two-tailed) analyzed the relationship between variables (Table 2).
Correlations (Pearson r) Between Variables (n = 1,068).
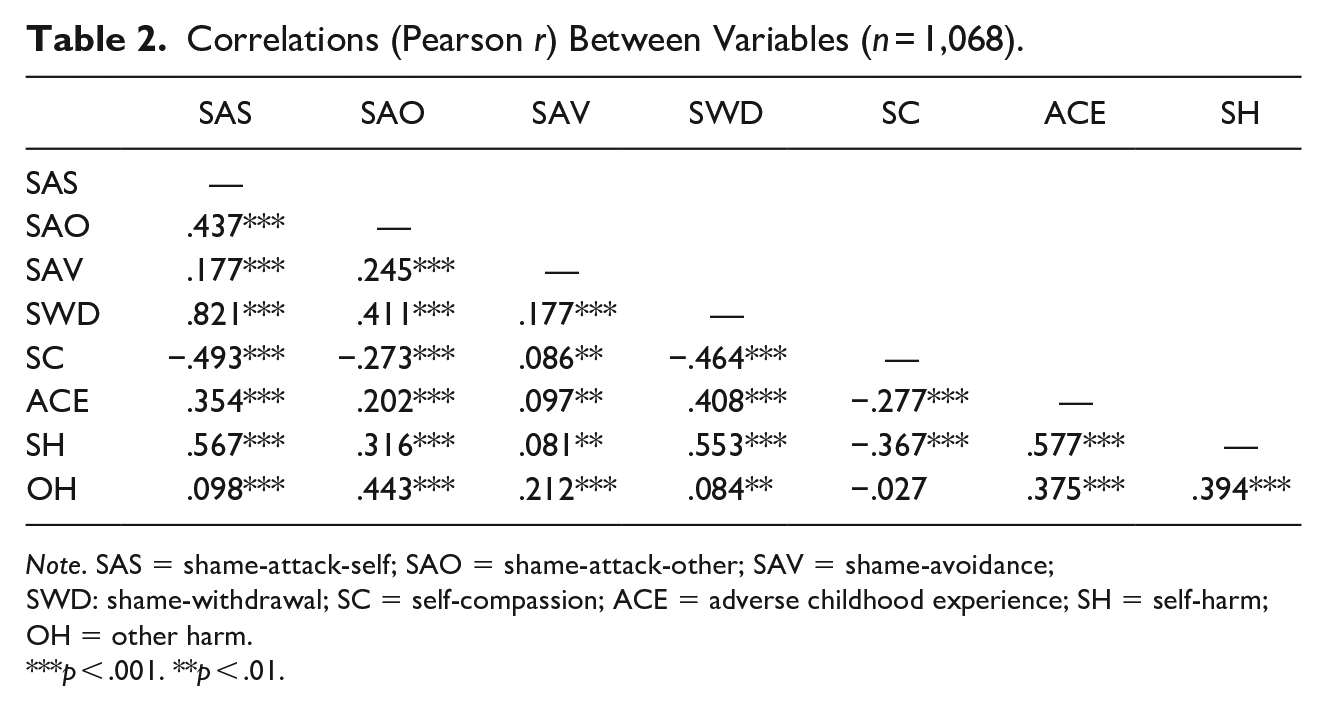
Note. SAS = shame-attack-self; SAO = shame-attack-other; SAV = shame-avoidance; SWD: shame-withdrawal; SC = self-compassion; ACE = adverse childhood experience; SH = self-harm; OH = other harm.
p < .001. **p < .01.
Structural Equation Modelling
A confirmatory factor analysis was undertaken to confirm “high shame and low self-compassion” as a latent factor. All four shame variables and the self-compassion variable were included, but shame avoidance was removed due to poor contribution and fit. The latent factor model with the specified indicator variables (i.e., attack-self, attack other, withdrawal) provided a good fit with the data for both self-harm, χ2 (df = 2, N = 1,111) = .70, p = .705; CMIN/df = .350, CFI = 1.0, RMSEA = .000, PCLOSE = .972, and harm to others models, χ2 (df = 2, N = 1068) = 1.166, p = .558; CMIN/df = .583, CFI = 1.0, RMSEA = .000, PCLOSE = .942. Exploratory SEM analyses, using principles of parsimony, identified a pathway model from ACEs to harm to self and harm to others. Both have theoretical grounding, significant relationships between variables and adequate goodness-of-fit.
SEM: ACE to self-harm
The model was a good fit for the data: χ2 (df = 7, N = 1,111) = 30.22, p = .000; CMIN/df = 4.31, CFI = .992, RMSEA = .055, PCLOSE = .316 (Figure 2). Just under 50% of the self-harm variance (R2 = .49, p = .006) is predicted by the model.
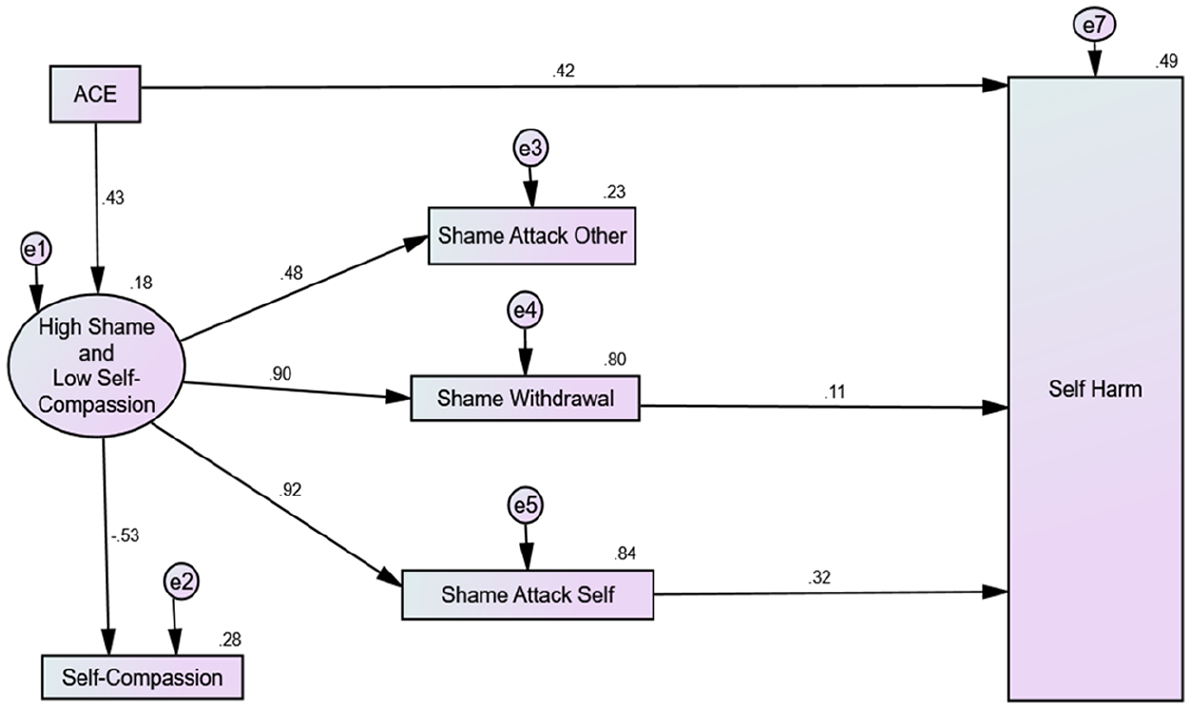
SEM path from ACE to self-harm. SEM = structural equation model.
ACEs had a direct (β = .421, 95% CI [.339, .464], p = .007) and indirect path (β = .167, 95% CI [.143, .198], p = .003) to self-harm. The indirect path from ACEs to self-harm was increased through partial mediators shame-attack-self (β = .033, 95% CI [.024, .043], p = .010) and shame-withdrawal (β = .011, 95% CI [.003, .020], p = .005). Overall, ACEs had a large total effect (β = .589, 95% CI [.546, .625], p = .007) on self-harm, combining both direct and indirect paths. Shame-attack-self (β = .319, 95% CI [.244, .406], p = .002) and shame-withdrawal (β = .110, 95% CI [−.030, .185], p = .014) had a direct path to self-harm. In summary, within the harm-to-self model, ACE, shame-attack-self, and shame-withdrawal all have a direct positive path to self-harm. Shame-attack-self and shame-withdrawal are both significant partial mediators in the relationship between ACEs and self-harm. However, shame-attack-self and shame-withdrawal only explain a small amount of the total effect.
SEM: ACE to harm to others
The model was a good fit for the data: χ2 (df = 6, N = 1068) = 24.46, p = .000; CMIN/df = 4.08, CFI = .992, RMSEA = .054, PCLOSE = .352 (Figure 3). Over a third of the variance (R2 = .35, p = .012) within the harm to others variable was explained by the model.
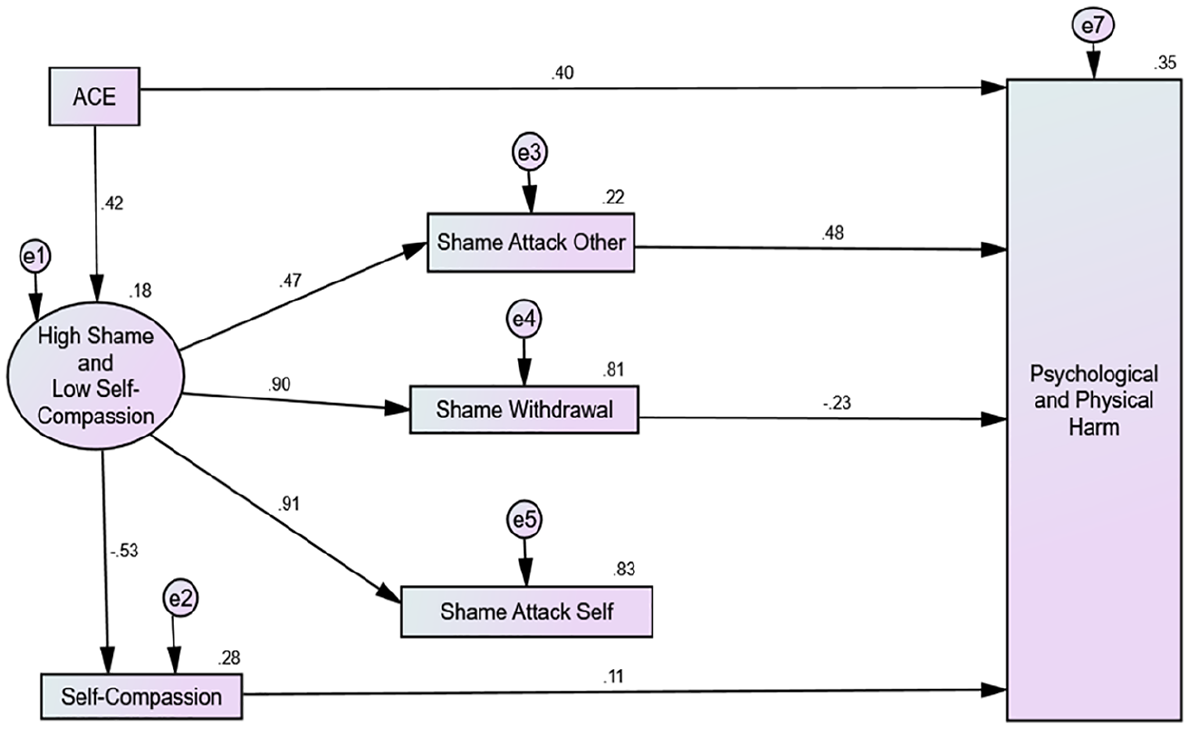
SEM path from ACE to harm to others. SEM = structural equation model.
ACE had a direct path to psychological and physical harm toward others (β = .399, 95% CI [.338, .454], p = .005). The indirect path from ACEs to harm was increased through shame-attack-other (β = .136, 95% CI [.108, .167], p = .004) and decreased through shame-withdrawal (β = −.122, 95% CI [−.166, −.082], p = .005) and self-compassion (β = −.035, 95% CI [−.054, −.018], p = .004). Overall, ACEs had a moderate total effect (β = .384, 95% CI [.336, .438], p = .002) on harm, combining both direct and indirect paths. Shame-attack-other (β = .484, 95% CI [.432, .531], p = .005) and self-compassion had a positive direct path to harm to others (β = .110, 95% CI [.056, .168], p = .003), while shame-withdrawal had a direct negative path to harm (β = −.227, 95% CI [−.291, −.162], p = .006). In summary, within the harm-to-others model, ACE, shame-attack-other, shame-withdrawal, and self-compassion all have a direct path to harm. With ACE, shame-attack-other and self-compassion increasing harm toward others and shame-withdrawal decreasing harm. Shame-attack-other, shame-withdrawal, and self-compassion are also significant partial mediators in the relationship between ACEs and harm. However, they only explain a small-to-moderate amount of the total effect.
Discussion
We postulated that ACEs would be related to harming behaviors through the mediators of shame and self-compassion. We also predicted that there would also be a direct relationship between the variables (i.e., ACEs, shame, and self-compassion) and harm. These findings support the central prediction that ACEs are related to harm and that this effect is mediated by shame. They also suggest that self-compassion has a potential role in moderating this effect rather than independently linking ACEs to harm. Our findings also support the proposition that the direct and mediating role of shame can vary, depending upon the behavioral manifestation of shame. For example, shame-attack-other increases psychological and physical harm, while shame-withdrawal decreases psychological and physical harm.
Our findings on the role of self-compassion, shame and harm were mixed, similar to previous findings (Gregory et al., 2017). Our models suggest that self-compassion can both increase and decrease the risk of harm. The relationship between self-compassion and shame generally reflects previous research findings (e.g., Zhang et al., 2018), with self-compassion having a negative relationship with shame in the forms of shame-attack-self, shame-attack-other, and shame-withdrawal. However, a positive relationship presented between self-compassion and shame avoidance. This may reflect conceptual overlap and, therefore, possible measurement error. It may be beneficial for future research to consider the different elements of self-compassion, or alternatively, other conceptualizations of self-compassion could be utilized.
Our research also sheds further light on the complex multidimensional nature of shame, in that it has the ability to decrease the risk of harm as well as increase it (e.g., Spruit et al., 2016). Therefore, these findings suggest that making distinctions between the forms of shame that are experienced is critical to understanding the pathway between ACE, shame, and harm. The importance of these distinctions is particularly apparent within the psychological and physical harm model, where shame-attack-other increased the risk of harm toward others, and shame-withdrawal decreased it. Unexpectedly, the shame-attack-other variable had a moderate positive relationship with self-harming behaviors. This may reflect self-harming behaviors as an externalization of shame (e.g., shame-attack-other), which serves as a way to reduce painful affect, but that can also be experienced as a negative behavior directed toward others (e.g., punitive, controlling, manipulative, disruptive and aggressive; Ireland & Quinn, 2007). Therefore, our research may support the notion that self-harming behaviors can present as externally harmful despite the function of this behavior being to reduce a person’s own distress. This is particularly important for those that dual harm (e.g., hurt themselves and others; Slade, 2018) as individuals that are considered to be disruptive/aggressive and self-harm are more likely to be responded to with negative attitudes and punitive behaviors (Ireland & Quinn, 2007), which in turn could heighten the risk of self-harm (Towl & Forbes, 2002) and suicide (Nock et al., 2006). The relationship between shame-attack-other and self-harm needs to be explored further.
Despite this original research having a number of key strengths, including the large sample size, the inclusion of community and custodial samples, and the robust psychometric measures used, it also has a number of limitations. Firstly, an inherent limitation of cross-sectional studies is the difficulties in evidencing temporal relationships due to the concurrent measurement of variables, and this is particularly important within SEM (Gollob & Reichardt, 1991). Future research would benefit from more temporally sensitive analyses. Secondly, measuring childhood adversity using a retrospective methodology has received criticism (Hardt & Rutter, 2004; Newbury et al., 2018). Retrospective measures are more likely to miss ACEs that participants have forgotten or that they chose not to disclose; however, prospective measures can also miss ACEs that are not recognized or reported during childhood (Newbury et al., 2018). Finally, although the study has gained a large sample size, which included forensic and community populations, our research would have benefitted from a more diverse sample. For example, the majority of the sample considered themselves to be white British. Similarly, our research would have benefitted from a greater number of women within the forensic population. However, it is noted that this proportion reflects the smaller proportion of women within custody, with females representing approximately 5% of the UK prison population (Official Statistics: Prison Population Figures, 2017). Future research would benefit from gaining a larger sample of females that have received convictions and a more diverse sample.
Our findings highlight the importance of investing in strategies that prevent childhood adversity and the need for supportive interventions for those that have already experienced childhood adversity. For example, strategies that reduce shame (i.e., shame-attack-self and shame-attack-other) can reduce the risk of a potential trajectory toward harm (i.e., harm to self or harm to others) and aid post-traumatic growth and resilience. Our findings also indicate that interventions and risk-management strategies for adults who harm themselves or others need to be non-shaming, with a specific focus on reducing shame-attack-self and shame-attack-other manifestations. For example, in adult “dual harm” populations, risk management interventions that evoke shame, intentionally or unintentionally, in order to reduce offending behaviors can instead, through specific manifestations of shame, increase the risk of harm to the self and/or others.
Future Directions in Research
Our research needs to be replicated to further test the plausibility of the models presented and increase the generalizability of these findings. Replication studies need to ensure they use a multifaceted and multidimensional conceptualization of shame, and they would also benefit from considering alternative ways of measuring self-compassion. Research would also benefit from exploring other potential psychological factors of causation, beyond shame and self-compassion, that may explain more of the variance within the presented model. In addition, including other variables that may help to further increase resilience and post-traumatic growth following ACEs (e.g., a supportive adult figure, intelligence, etc.) and other forms of ACE not captured within our research would add helpful insights to theories linking ACEs to harm. Finally, future research would benefit from including further consideration of the age at which ACEs occur and, therefore, potentially aiding more precision in directing prevention and treatment strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.