
Abstract
According to the Risk-Need-Responsivity (RNR) model, treatment effectiveness increases when treatment addresses all three associated core principles. While researchers have focused on the risk and need principles, responsivity remains under-investigated. The theoretical foundation of the RNR model and former research indicates low perceived self-efficacy and inadequate adult attachment styles as potential responsivity factors that can impede treatment of the underlying risk factors. This study assesses firstly whether these factors predict treatment attrition, and secondly changes in the assessed risk of sexual reoffending. Participants were N = 146 men sentenced for sexual offenses in a German social-therapeutic correctional facility. Younger age, higher number of previous convictions, and higher scores on the interpersonal facet of the Psychopathy Checklist-Revised are associated with a higher risk of treatment attrition. Unemployment prior to incarceration was found to be an aggravating factor, whereas substance abuse emerged as a mitigating factor, according reducing the risk of reoffending. Neither pre-treatment self-efficacy nor attachment styles revealed as responsivity factors in this study. Future studies should examine if the consideration of these factors during treatment might impact treatment outcomes.
Keywords
Introduction
The Risk-Need-Responsivity (RNR) model (Bonta & Andrews, 2017) provides a sound theoretical foundation for the effective treatment of people who have become delinquent. Such treatment aims to reduce the risk of reoffending and to enhance the chance of a pro-social lifestyle. Treatment effectiveness increases when treatment addresses all three core principles of the RNR model (Bonta & Andrews, 2017; Gannon et al., 2019; Hanson et al., 2009). While the Risk Principle (treatment intensity depends on the level of recidivism risk) and the Need Principle (treatment is based on individual criminogenic needs associated with delinquency) are well investigated, the Responsivity Principle is still insufficiently examined (e.g., Bonta & Andrews, 2017; Cohen & Whetzel, 2014; Jung & Dowker, 2016). The RNR model implies that the General Responsivity principle is met by treatment offers based on cognitive-behavioral and social learning approaches. Specific Responsivity is however defined rather vaguely: the model states that the better the treatment fits a client’s personality, cognitive style, skills and attributes, the more effective it is (Bonta & Andrews, 2017; Schmucker & Lösel, 2015). In other words, specific responsivity factors are individual characteristics that are not directly targeted as risk factors in correctional treatment but can hinder the client’s responsiveness to treatment if disregarded. Consequently, a sound consideration of specific responsivity factors can provide the basis for effective treatment and can help to ensure that the client gets the maximum therapeutic benefit from intramural treatment (treatment that takes place “within the walls” and is within the usual limits for imprisoned people).
One of the first steps with regard to treatment success lies in the ability to prevent the client of treatment noncompletion, as those who do not complete treatment are unlikely to derive its maximum benefits. For those who continue treatment, it is crucial to effectively address individual risk and need factors that are assessed shortly after imprisonment. Since the consideration of the responsivity factors may help to avoid treatment noncompletion, and seem to make the treatment of risk factors for recidivism more effective (e.g., Bonta & Andrews, 2017; Craig et al., 2013), a better understanding of specific responsivity factors is essential. Bonta and Andrews (2017) mention the importance of addressing self-efficacy and adult attachment styles in order to improve treatment responsiveness, and thus work on the underlying risk and need factors. The assumption is supported by findings from both non-forensic and forensic studies: perceived self-efficacy as well as appropriate adult attachment styles seem to increase treatment motivation and compliance, reduce the probability of treatment attrition, and correlate with treatment success (Bennett et al., 2011; Bernecker et al., 2014; Brenk-Franz et al., 2016; Marshall et al., 2008; McMurran et al., 1998; Sturgess et al., 2016; Taylor et al., 2015).
Perceived Self-Efficacy and Correctional Treatment
Perceived self-efficacy is based on the idea of internal causal attribution, that is, the assumption that people attribute their experiences of success and failure to themselves (Luszczynska et al., 2005; Schwarzer & Jerusalem, 1995). It describes a relatively stable personality trait that enables people in various areas of life to cope with critical situations (e.g., “I can solve difficulties on my own”; Schwarzer & Jerusalem, 1999). The extent of (pro-social) perceived self-efficacy is a central point in successful correctional treatment. It is understood as one of the clients’ mediating factor in preventing treatment attrition (Sturgess et al., 2016) and relapses after treatment (Hall, 1989; Marshall et al., 2008; Pollock, 1996; Tozdan et al., 2015). Bonta and Andrews (2017) recommend increasing self-efficacy to maximize the effectiveness of correctional treatment. This is underlined by a small number of empirical studies: People convicted of sexual offenses who participated in a preparatory program that especially focused on increasing self-efficacy were less likely to reoffend after release (Marshall et al., 2008). Convicted individuals with high self-efficacy who are on probation better meet the court obligations in a goal-oriented and committed manner (Bahr et al., 2010; Woldgabreal et al., 2016). In addition, in the case of treatment programs for people addicted to alcohol/drugs, participants with higher self-efficacy also tend to remain abstinent after participating (Disbury et al., 2015). A further study showed that the more convinced men with a sexual interest in children are in their ability to influence their sexual interest in children, the lower is their perceived and actually expressed sexual interest in children (Tozdan et al., 2018).
In total, these research findings indicate that perceived self-efficacy could be an important responsivity factor. Nevertheless, investigations regarding its relevance for the prevention of treatment attrition, and successfully reducing risk factors in the case of intramural treatment, are not common. Based on these findings, we hypothesize that low perceived self-efficacy might hinder the clients getting the maximum therapeutic benefit from treatment. Therefore, we investigate this factor as a specific responsivity factor.
Adult Attachment Styles and Correctional Treatment
Different adult attachment styles can be described in terms of higher or lower individual levels of attachment-related anxiety and attachment-related avoidance (Brennan et al., 1998; Strauß et al., 2016). People with a high level of attachment-related anxiety have a strong need for acceptance, support, and admiration, and also fear rejection and abandonment by others. The latter often goes hand-in-hand with lower perceived self-efficacy in social situations (Fraley et al., 2000, 2011; Neumann et al., 2007). People with a high level of attachment-related avoidance often feel uncomfortable in interactions that require intimacy, self-revelation and dependence on others. Thus, insecure attachment is represented by high scores on one or both dimensions, whereas individuals with secure attachment receive low scores with regard to both dimensions (Brennan et al., 1998; Smith et al., 2010). It has been found that men who committed sexual offenses are more likely to have high levels in both dimensions: attachment-related anxiety and avoidance (Lyn & Burton, 2004, 2005; Marsa et al., 2004).
In studies addressing intramural treatment, the consideration of attachment styles is important, as attachment-related anxiety and avoidance seem to influence the psychotherapeutic alliance (Asendorpf, 2018; Wei et al., 2005). Being avoidant or unable to trust others affects treatment engagement in a negative way, whereas being able to build a therapeutic relationship facilitates treatment engagement (Tetley et al., 2012). Especially in group therapies, which are a common treatment form in correctional facilities, the attachment style determines not only the relationship to the therapist but also to the other group members (Jennings et al., 2021; Sonkin & Dutton, 2003). The higher the attachment-related anxiety, the more negative the assessment of one’s own person; the higher the attachment-related avoidance, the more negative the assessment of the other participants (Rom & Mikulincer, 2003). Furthermore, it has been found that men who victimized children more often show insecure attachment styles compared to men who victimized adults (Lyn & Burton, 2004; Marsa et al., 2004). A meta-analysis involving three studies which compared attachment styles across different types of sexual offenses found that men convicted of child sexual abuse were more anxious in their attachment style, while men convicted of rape were more avoidant (Ogilvie et al., 2014). Therefore, adult attachment styles should be considered more with regard to group treatment programs, given that such groups often include members with various attachment styles, and therefore a range of potential attachment difficulties (Jennings et al., 2021; McKillop et al., 2016; Ogilvie et al., 2014).
However, the current state of research is ambiguous in that some studies contradict the findings mentioned above: Bennett et al. (2011) found that attachment-related avoidance was correlated with treatment attrition. In treatment programs for people who abuse substances, high anxiety and avoidance were associated remaining in treatment (Marshall et al., 2018). Marshall et al. (2018) discuss two suggestions as to why attachment-related anxiety might be supportive in specific group therapies, even though it might usually be a hindering factor. Firstly, the possible tendency of anxious people to maintain any type of relationship might motivate people to stay in contact and therefore in treatment. Secondly, the potentially hindering anxiety might be mitigated by downwards social comparison with the other group members (‘looking down’ on other group members as one part of attachment-related avoidance; also c.f. Rom & Mikulincer, 2003) which enhances the probability of remaining in treatment. The (non-forensic) systematic review by Smith and colleagues (2010) also shows inconsistencies with regard to the relationship between the dimensions of attachment-related anxiety and avoidance, therapeutic attachment, and the probability of treatment attrition. However, the authors assume that these inconsistent findings might be due to general issues concerning the inconsistencies in conceptualization and in the measurement of adult attachment styles. Because of the mixed study outcomes, we hypothesize exploratively that attachment-related anxiety and avoidance are associated with treatment noncompletion and success.
Study Aim and Rationale
The importance of believing in one’s own competencies, building a therapeutic alliance, and being able to function in groups of intramural correctional treatment led us to investigate if the pre-treatment levels of perceived self-efficacy and adult attachment styles are possible specific responsivity factors, and therefore decisive when it comes to successful treatment.
The success of treatment programs is predicated on the ability to retain clients through to treatment completion; those who do not complete treatment are unlikely to derive its benefits. Excluding non-completers from evaluation studies assessing the effectiveness of treatment can lead to a potential overestimation of treatment effects (e.g., Endres et al., 2016; Hatcher et al., 2012). Furthermore, treatment attrition is linked to higher recidivism risks in men with sexual offense histories compared to those receiving no treatment at all (McMurran & Theodosi, 2007; Olver et al., 2011). To prevent treatment noncompletion on the part of those clients who need it most (high levels of assessed risk and need), it is important to analyze those predictors that are associated with treatment attrition.
In research question I, we will therefore investigate the association of pre-treatment perceived self-efficacy and attachment-related anxiety and avoidance with the risk of treatment attrition. In research question II, we will investigate the association of pre-treatment perceived self-efficacy and attachment-related anxiety and avoidance with the change in the assessed risk of sexual reoffending after approximately 1.5 years of treatment, or after treatment completion.
In order to examine a valid model for predicting attrition and changes in assessed risk, other variables associated with a lack of treatment success known from former studies are also integrated into the analyses — although the present study focuses on perceived self-efficacy and attachment-related anxiety and avoidance. Previous studies and meta-analyses show that clients who do not complete treatment are younger when committing their first offense, are more likely to abuse substances and are characterized by more previous convictions, more frequent, and longer detentions (e.g., Brunner et al., 2019; Jewell & Wormith, 2010; Olver et al., 2011). In addition, a higher level of psychopathy (Hare, 2003), an increased risk of reoffending, and low treatment motivation are predictors of treatment attrition (Beyko & Wong, 2005; Hanson et al., 2009; Olver & Wong, 2009; Wormith & Olver, 2002). Some of these variables can be understood as both predictors for treatment attrition as well as specific responsivity factors. In line with the studies cited above, we hypothesize that the following variables are associated in a negative way with treatment completion and a reduction of the assessed risk of reoffending: younger age, no education, unemployment prior to incarceration, never married, life-time substance abuse issues, as well as higher number of prior convictions.
Method
Treatment Program
The present study is part of the ongoing research project “Evaluation of the Social-Therapeutic Correctional Facility Hamburg” (Brunner et al., 2016, 2019). In Germany, social therapy represents the primary form of correctional treatment in prisons and is regulated by legislation: admission to a social-therapeutic correctional facility (German: Sozialtherapeutische Anstalt, SothA) is mandatory for all men sentenced to a minimum of 2 years’ imprisonment for sexual offenses (§9 of the German Federal Penal Execution Code; StVollzG, Strafvollzugsgesetz; cf. Briken et al., 2019; Etzler et al., 2020).
Correctional treatment in a SothA is often based on the RNR model, and aims to reduce the risk of reoffending by providing adequate resocialization (Etzler & Rettenberger, 2020; Spöhr, 2009). It is meant for imprisoned clients who have acquired inappropriate forms of coping with their problems, or who have lost the confidence to achieve success with the use of lawful and pro-social behavior (Arbeitskreis Sozialtherapeutische Anstalten im Justizvollzug, e.V., 2016). During integrative social-therapeutic treatment, the entire living environment inside and outside the SothA is considered, including family, friends, partners as well as working out the further career, possible living situations and — if necessary — a professional aftercare post-release. Different coping strategies and dealing with stressful situations, as well as various forms of interpersonal relationships, should be considered within the therapeutic community (e.g., with regard to staff and other incarcerated clients). The clients should gain new insights, and learn and try out new behaviors and forms of relationships. In addition to further social skills, they should attain new ways of coping with life. In the last phase of the stay in the SothA, the imprisoned clients are usually given the opportunity to leave the prison for hours or even days to achieve specific rehabilitation goals, such as looking for an apartment, attending job interviews and preparing for their releases.
The SothA in Hamburg, Germany (SothA-HH) offers milieu therapy, individual therapy sessions, offense-specific group therapy (e.g., adaptions of the Sex Offender Treatment Program [see Friendship et al., 2003] and strength-based approaches for sexual offender rehabilitation [Marshall et al., 2011]) as well as general, offense unspecific treatments such as those that focus on substance abuse or trauma. If the purpose of the treatment cannot be achieved for reasons inherent in the client, a transfer to a general prison is initiated (treatment attrition).
Research Project and Data Collection
From December 2010 to March 2020, 194 men sentenced for sexual offenses (thus, sentenced under §§ 174–184 of the German Criminal Code) and serving their sentences in the SothA-HH have been evaluated in this project. Data was based on standardized pre-treatment ratings (within the first weeks of admission to the SothA-HH) and post-treatment ratings (after regular completion or approximately 1.5 years after the initial testing). Trained psychologists collected data derived from case file information (e.g., criminal record, court files, or psychological reports) and semi-structured interviews (oriented on the Psychopathy Checklist-Revised [PCL-R] and Stable-2007 interviews), which lasted approximately 2 hours per participant. Collecting and assessing all the information and ratings took approximately 2 days per case. Information about treatment attrition was provided by the SothA-HH administration. On a general level, transfer back to prison for reasons other than treatment attrition or a lack of cooperation during treatment included, for example, drug use or violations during day-release. A transfer back to prison for reasons independent of the incarcerated client were less common. Although we did not assess the reason for transfer to regular prisons on an individual level, we do know that completers and non-completers of the research project differ in relevant characteristics, and non-completers show higher assessed risk of reoffending (cf. Brunner et al., 2019). In addition, the annual publications by the Center of Criminology (German: Kriminologische Zentralstelle, KrimZ) on social therapy in the German prison system show that from 2010 to 2020, an average of 61% of the transfers back from the SothA-HH to the general prison were initiated by staff and 39% by the incarcerated clients themselves (Elz, 2014, 2015, Etzler, 2016, 2017, 2018, 2019, 2020, Niemz, 2010, 2011, 2013; Niemz & Lauwitz, 2012).
The research project is authorized and funded by the Ministry of Justice of the Hanseatic City of Hamburg, Germany and conducted by the Institute for Sex Research, Sexual Medicine and Forensic Psychiatry at the University Medical Center Hamburg-Eppendorf. The project was approved by the ethical committee of the Hamburg chamber of psychotherapists. Participants were informed about the purpose of the research project, and gave their written informed consent in accordance with the Declaration of Helsinki.
Measures
Demographic and offense Variables
This study includes the following demographic and offense variables that previous research has supported as being related to a lack of treatment success (cf. Brunner et al., 2019; Jewell & Wormith, 2010; Olver & Wong, 2009, 2011; Olver et al., 2011; Wormith & Olver, 2002): age at time of data collection, education (0 = secondary school diploma; 1 = no secondary school diploma), employment prior to incarceration (0 = employed or student/trainee; 1 = neither employed nor student/trainee) and marital status (0 = ever married; 1 = never married). Furthermore, substance abuse (0 = no; 1 = yes) was defined as a lifetime mental and behavioral disorder due to psychoactive substance use (International Classification of Diseases (ICD-10) criteria for harmful use or dependency syndrome; World Health Organization, 1992). The number of prior convictions was extracted from the central criminal register.
Psychopathy
The PCL-R (Hare, 2003; German Version: Mokros et al., 2017) measures psychopathic personality traits with the use of 20 items. Each of the 20 items is scored on a three-point scale (0–2) with total scores ranging from 0 to 40. The PCL-R consists of two interrelated factors which are further divided into two facets each: Factor 1 scores from 0 to 16 and describes interpersonal (Facet 1) and affective facets (Facet 2). Factor 2 scores from 0 to 20 and pertains to impulsive lifestyle (Facet 3) and antisocial behavior (Facet 4). Two items belong to neither of the two factors. The German cut-off score for the existence of a psychopathic personality is greater than or equal to 25 points (Mokros et al., 2017). The reliability, concurrent and predictive validity of the PCL-R have been supported by a substantive literature (Dahle, 2006; Eher, Rettenberger, et al., 2012; Hare, 2003; Hare et al., 2000; Stadtland et al., 2006). In the event of omitted items, prorated scores were used (Mokros et al., 2017).
Risk of Sexual Reoffending
The assessment of the relative risk of sexual reoffending was measured with the use of two instruments. The Static-99 1 (Harris et al., 2003; German Version: Rettenberger & Eher, 2006b) is a 10-item actuarial assessment instrument. The instrument assesses mostly unchangeable risk factors, for example, demographic information, information about prior offenses, and the people who were victimized. The total scores range from 0 to 12 and are assigned to four risk categories: low (0–1 point), low-medium (2–3 points), medium-high (4–5 points) and high (6–12 points).
In contrast, the Stable-2007 (Fernandez et al., 2012; German version: Matthes et al., 2012) measures stable-dynamic risk factors, thus deals with factors that are changeable but relatively stable without therapeutic interventions (e.g., significant social influences, hostility against women, general and sexual self-regulation, cooperation with supervision). Each of the 13 variables is scored on a three-point scale (0–2) with total scores ranging from 0–26 for individuals with sexual offense histories with child victims, and from 0 to 23 for individuals with sexual offense histories without child victims. The total score is assigned to three risk categories: low (0–3 points), medium (4–11 points) and high (≥12 points). The prognostic validity of the German versions of Static-99 and Stable-2007 are described as being moderate (Eher, Matthes, et al., 2012; Rettenberger & Eher, 2006a; Rettenberger et al., 2010).
The Stable-2007 is a sensitive instrument when it comes to assessing changes (increase or decrease) in the risk of reoffending (Fernandez et al., 2012). With regard to research question II, participants were identified as outliers, and were excluded from the following analyses, when the change from pre- to post-testing in this variable was more than two SDs of the sample mean. It is unlikely that changes to the extent of two SD are due to staying in and being in treatment in a social-therapeutic correctional facility; these changes are more likely due to a lack of information quality or change in information available between the first and the second assessment (e.g., subsequent convictions, documentation of inappropriate behavior during imprisonment).
Perceived Self-Efficacy
The General Self-Efficacy Scale (GSE; Schwarzer & Jerusalem, 1995; German version: Schwarzer & Jerusalem, 1999) assesses a general sense of perceived self-efficacy. The authors describe that the scale aims to predict coping with daily problems and adaptation after experiencing challenging life events. The scale contains 10 items (e.g., “I can solve most problems if I invest the necessary effort”), and responses are made on a 4-point Likert-scale (1 = not true at all; 4 = exactly true). The total score ranges from 10 to 40. Following the authors’ manual, sum scores were transformed into T-Scores (M = 50, SD = 10). A higher T-score reflects an optimistic self-belief, which implies an internal-stable attribution of success. We refer the scores of our sample to the non-clinical norm sample (n = 2019) from (Hinz et al., 2006). Previous studies confirm high reliability and criterion-related validity (Luszczynska et al., 2005; Scholz et al., 2002). In this study, Cronbach’s α as a measure of internal consistency was found to be high with α = .9 for the GSE.
Adult attachment style
The Experiences in Close Relationships-Revised scale (ECR-R; Fraley et al., 2000; German version: Ehrenthal et al., 2009) is a widely-used questionnaire to assess adult attachment styles. The instrument uses a seven-point Likert-scale (1 = strongly disagree; 7 = strongly agree) to answer each of the 36 items, and assesses the attachment dynamics along the two dimensions attachment-related anxiety and attachment-related avoidance in close relationships. (Fraley et al., 2000) reported that these factors were uncorrelated and produced highly-reliable subscales. Despite adult romantic attachment, it is also used for assessing attachment styles in other areas for scientific studies (e.g., assessing patient-physician working alliances, researching people addicted to drug and alcohol, or men who committed sexual offenses; Bennett et al., 2011; Lyn & Burton, 2004, 2005; Marsa et al., 2004; Marshall et al., 2018). We refer the scores of our sample to Ehrenthal and colleagues’ findings (2009) of a clinical norm sample (n = 225): attachment-related anxiety M = 3.71, SD = 1.41; attachment-related avoidance M = 3.08; SD = 1.27. A previous study confirms high reliability and criterion-related validity (Sibley & Liu, 2004). In this study, Cronbach’s α as a measure of internal consistency was found to be high with α = .9 for attachment-related anxiety, and α = .8 for attachment-related avoidance.
Sample
From December 2010 to March 2020, 194 men sentenced for sexual offenses were tested. All participants had already been admitted to the SothA-HH before participating in this study. In the following analyses, we were interested in the two subgroups of Completers and Non-Completers. Completion has been defined as either having remained in the SothA-HH for at least 1 year after the initial assessment, or having been released on a regular basis after at least a 1 year stay at SothA-HH. Non-Completers describe imprisoned clients who participated in the pretesting but were transferred back to general prison ahead of schedule. As we are only generally informed about the attrition status and not about the individual circumstances, attrition status can only be determined irrespective of the reasons for noncompletion.
Of those 194 participants tested, n = 48 men (25%) were excluded because they were tested less than 12 months before analyzing the current research data, or were regularly released less than 12 months after the pre-testing (due to their continuous but short duration of stay they could not be assigned to the Completers). Thus, the total sample of this study comprised N = 146 men sentenced for sexual offenses. Of those, 91% (n = 133) were convicted of contact offenses (98 times adult victims, 46 times child victims, multiple assignment within the current conviction was possible), 9% (n = 13) because of noncontact offenses (three times adult victims, 10 times child sexual abuse images), and 6% (n = 9) because of contact and noncontact offenses (one time adult victims, eight times child victims).
For the current study, the total sample of N = 146 participants is separated into n = 118 Completers (81%) and n = 28 Non-Completers (19%). Approximately 1.5 years after the initial assessment, or shortly before release, we asked all participants to take part in the post-testing. For n = 77 of the Completers, the risk of sexual reoffending was assessed again in the post-testing. Because the change in the assessed risk of reoffending from pre- to post-testing was greater than 2 SD from the samples’ mean, five of those participants were identified as outliers and were excluded from the analyses relating to research question II. Thus, the sample size of the participants whose post-testings are considered in the following analyses was n = 72.
Research question I considers the pre-treatment ratings of Completers and Non-Completers (N = 146). Research question II solely focuses on the ratings of the Completers who participated in the pre- and post-treatment testing (n = 72).
Data Analyses
The sample characteristics were compared using independent t-Tests and χ2-Tests, and effect sizes were calculated using Cohen’s d (small, medium, and large effect sizes are d = .20, .50, and .80; Cohen, 1992) and Cramer’s V (small, medium, and large effect sizes are V = .07, .21, and .35; Kim, 2017).
In research question I, the explorative predictors perceived self-efficacy (measured with GSE), attachment-related anxiety and attachment-related avoidance (measured with ECR-R), as well as previously-reported predictors of treatment attrition and lack of treatment success (age, education, employment, marital status, substance abuse, number of prior convictions, actuarial recidivism risk as well as all four facets of the PCL-R) were entered into a logistic regression with N = 146 participants (Vittinghoff & McCulloch, 2007). The outcome treatment completion status was coded as a binary variable (0 = completion; 1 = noncompletion).
In research question II, the explorative predictors perceived self-efficacy, attachment-related anxiety, and avoidance, as well as the same predictors of treatment attrition and lack of treatment success employed in research question I, were entered into a linear regression with those n = 72 Completers who participated in the pre- and the post-treatment testing. The outcome Stable-2007 change score (post-scores minus pre-scores) represents the change in the stable-dynamic risk of reoffending from pre- to post-treatment assessments.
For both research questions, the models with the best fit were identified using stepwise backward elimination per the Likelihood-ratio test, whereby variables were included in the analyses when α ≤ .05 and excluded when α > .10 for the analyses. All data analyses were performed using IBM SPSS Statistics 26 for Windows.
Results
Research Question I — Associations with Risk of Treatment Noncompletion
Sample Characteristics
Description of the Results of the Psychological Testing, Sample’s Socio-Demographic and Criminological Information, and Risk Assessment Characteristics for the Total Sample and Subgroups.
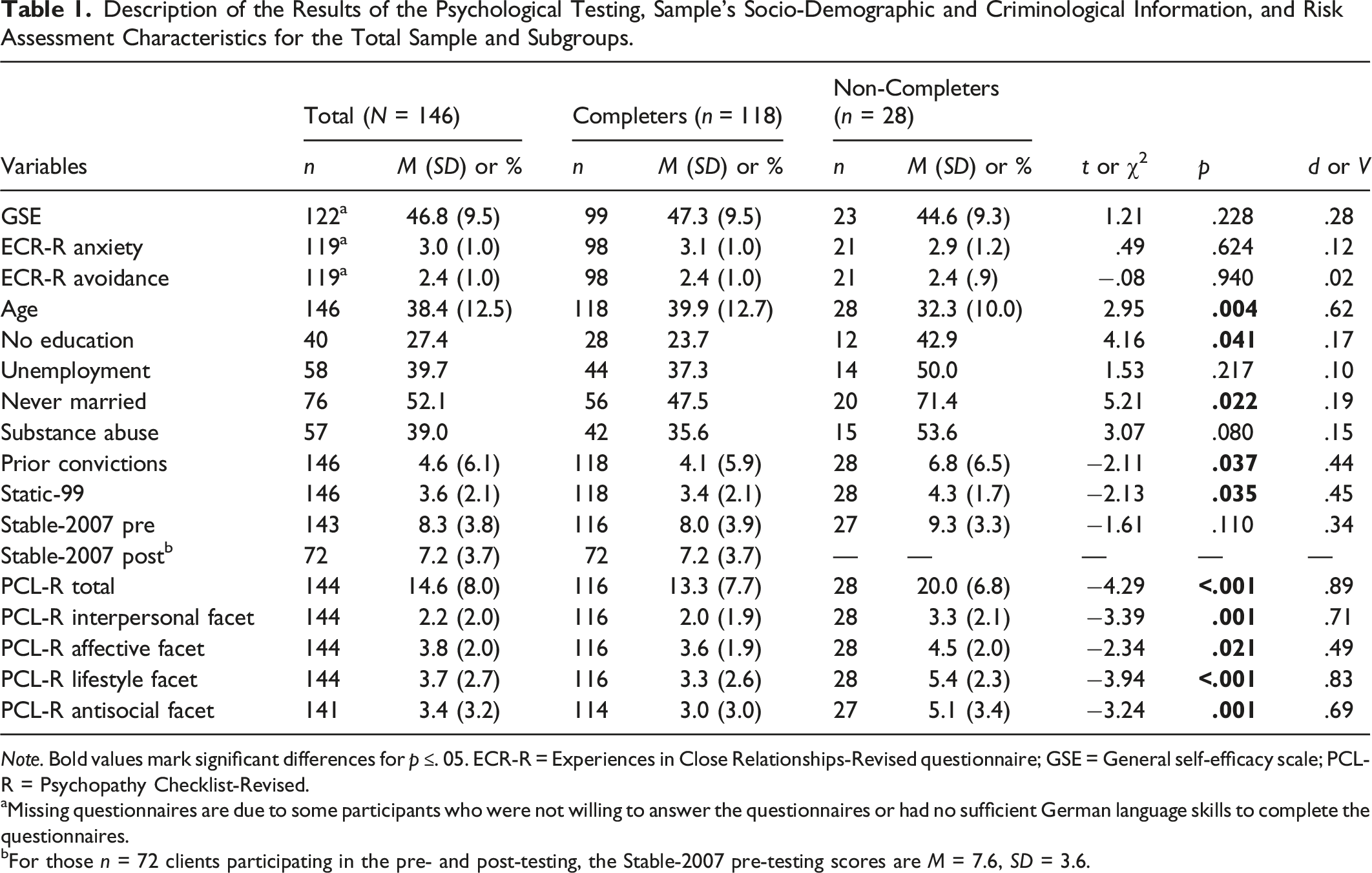
Note. Bold values mark significant differences for p ≤. 05. ECR-R = Experiences in Close Relationships-Revised questionnaire; GSE = General self-efficacy scale; PCL-R = Psychopathy Checklist-Revised.
aMissing questionnaires are due to some participants who were not willing to answer the questionnaires or had no sufficient German language skills to complete the questionnaires.
bFor those n = 72 clients participating in the pre- and post-testing, the Stable-2007 pre-testing scores are M = 7.6, SD = 3.6.
Distribution of Risk Categories Within the Subgroups.
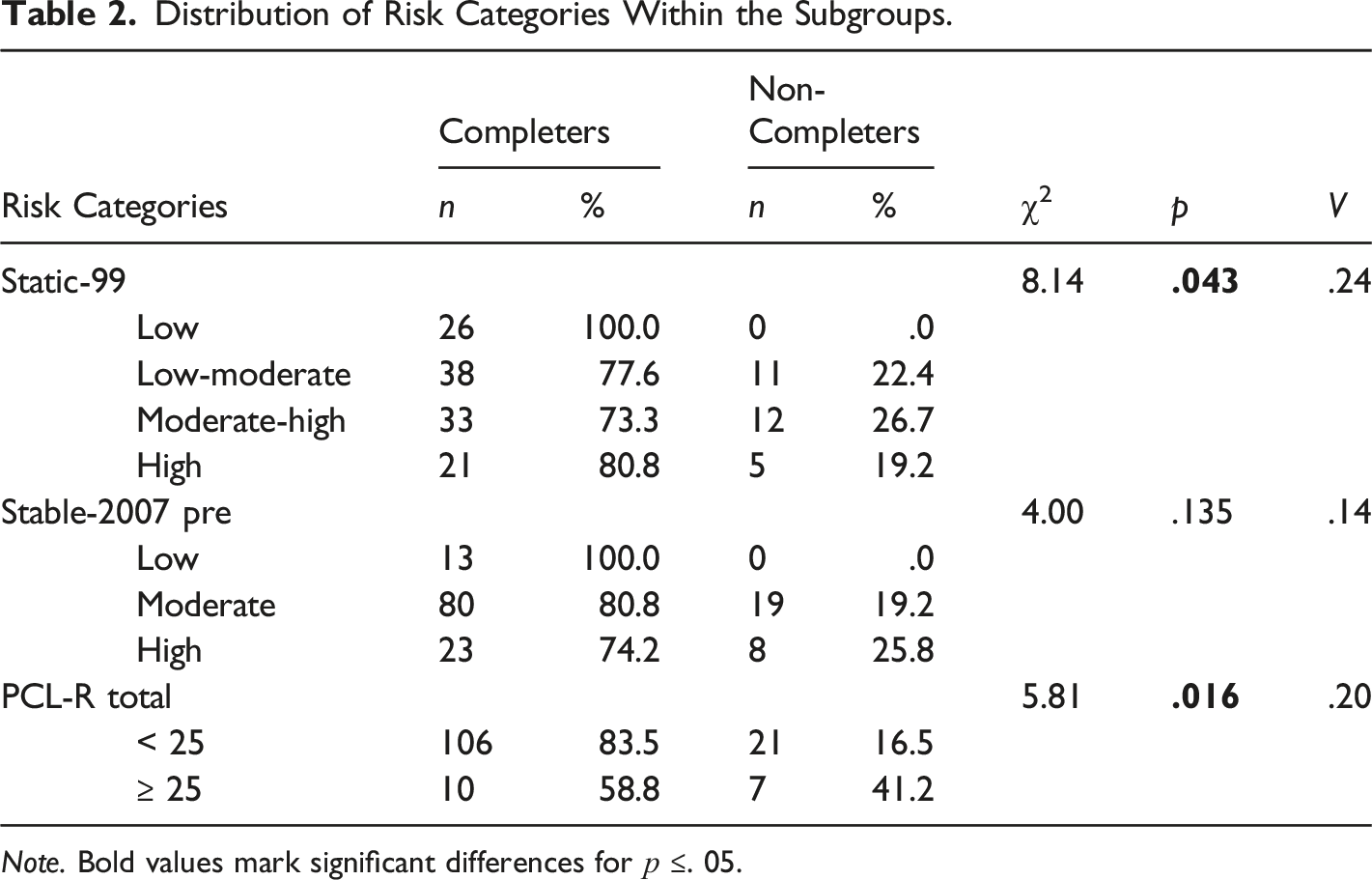
Note. Bold values mark significant differences for p ≤. 05.
Predicting Treatment Attrition
Logistic Regression Predicting Treatment Completion (n = 119).
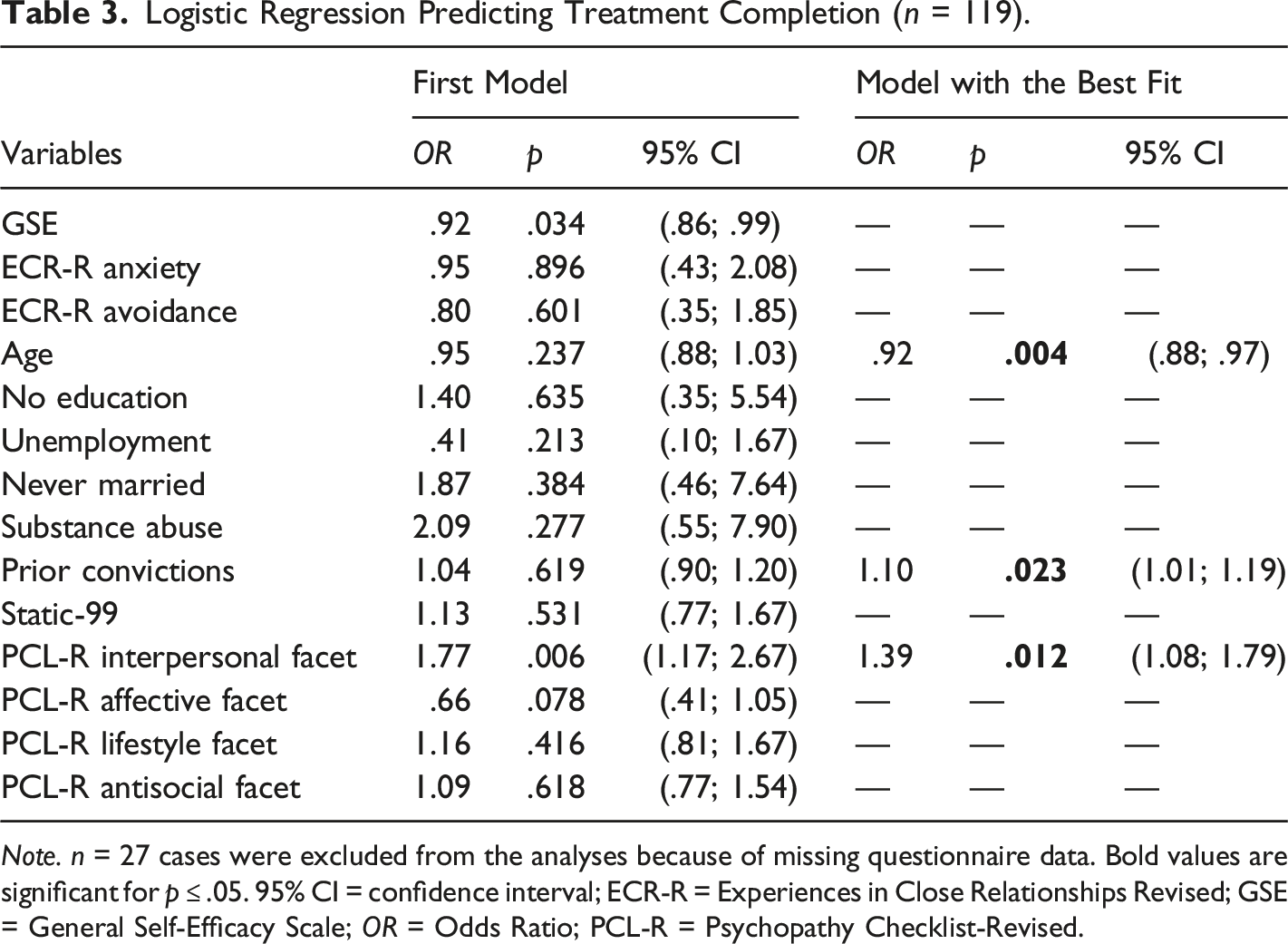
Note. n = 27 cases were excluded from the analyses because of missing questionnaire data. Bold values are significant for p ≤ .05. 95% CI = confidence interval; ECR-R = Experiences in Close Relationships Revised; GSE = General Self-Efficacy Scale; OR = Odds Ratio; PCL-R = Psychopathy Checklist-Revised.
Research Question II — Association with Risk of Sexual Reoffending
A comparison of the Stable-2007 scores from pre- to post-testing was only conducted for the Completers who participated in the post-testing. Of those n = 77 clients who participated in both assessments, the change score of five of the participants were identified as outliers, and were excluded from the analyses (see measures section). For the remaining n = 72 participants (cf. Table 1), a non-significant reduction of M = .39, SD = 1.8 points of the stable-dynamic risk was found (paired sample t-Test; t(71) = 1.84, p = .070, r = .21). For 46% of these Completers (n = 33) there was a decrease in the Stable-2007 scores from pre- to post-testing (M = −1.97, SD = 1.08), for 24% (n = 17) there was no change, and for 30% (n = 22) there was an increase (M = 1.68; SD = .78).
Multiple Linear Regression Predicting Changes in Risk (Stable 2007 Change Score) at Post Treatment (n = 64).
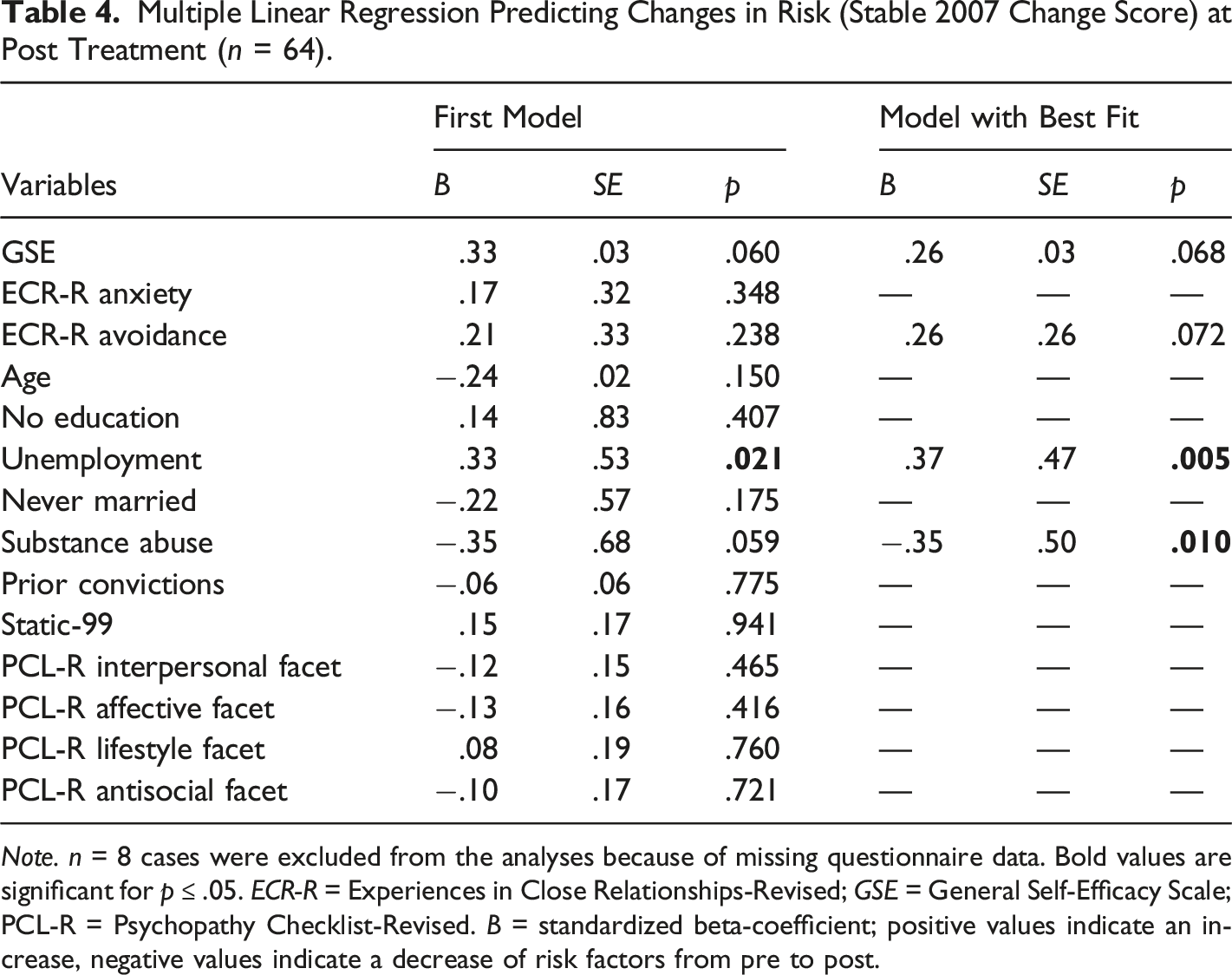
Note. n = 8 cases were excluded from the analyses because of missing questionnaire data. Bold values are significant for p ≤ .05. ECR-R = Experiences in Close Relationships-Revised; GSE = General Self-Efficacy Scale; PCL-R = Psychopathy Checklist-Revised. B = standardized beta-coefficient; positive values indicate an increase, negative values indicate a decrease of risk factors from pre to post.
Two-Tailed Pearson Correlations for Stable-2007 Change Scores and Its Predictors (n = 64).
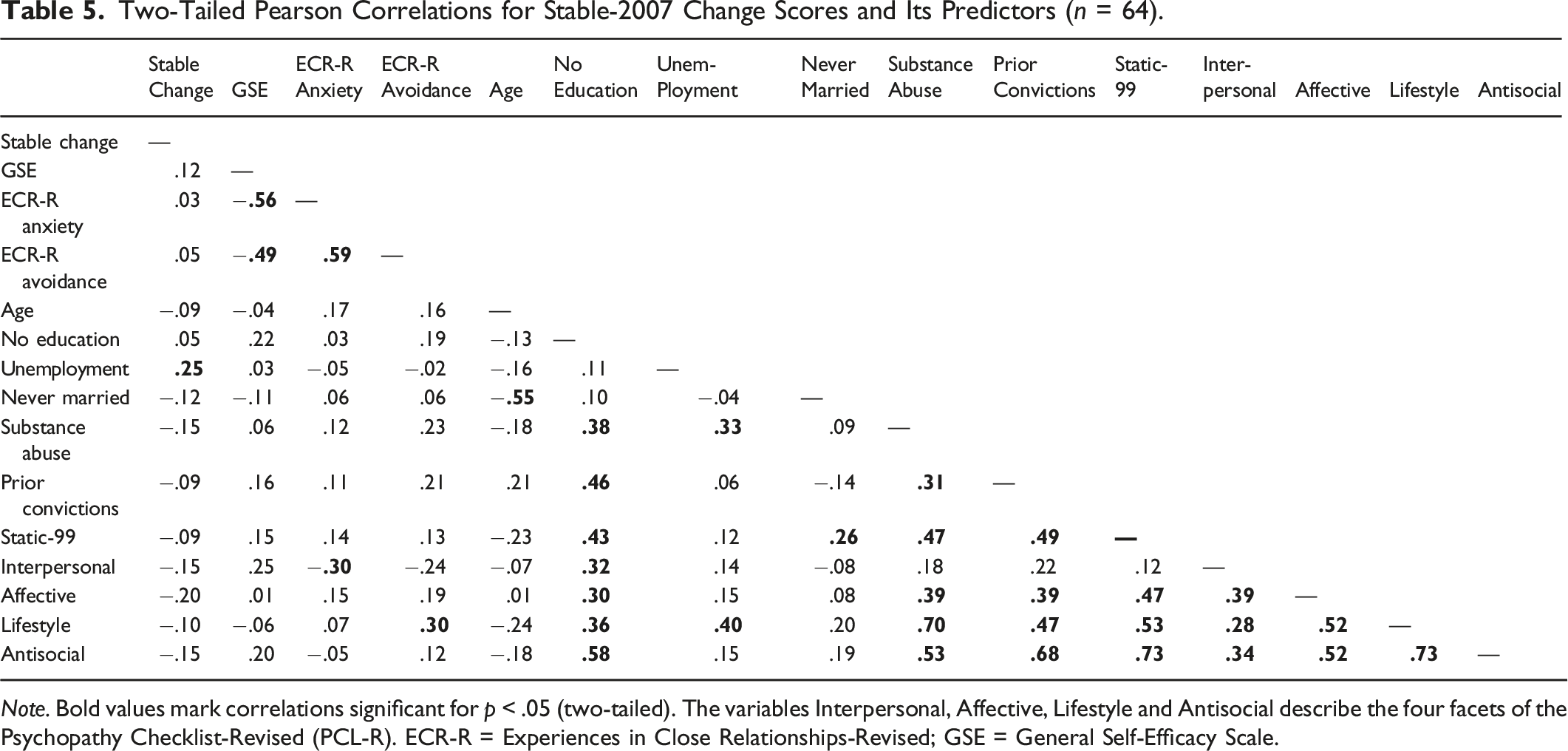
Note. Bold values mark correlations significant for p < .05 (two-tailed). The variables Interpersonal, Affective, Lifestyle and Antisocial describe the four facets of the Psychopathy Checklist-Revised (PCL-R). ECR-R = Experiences in Close Relationships-Revised; GSE = General Self-Efficacy Scale.
Discussion
The treatment of imprisoned clients who have committed sexual offenses aims to reduce the risk of reoffending. One of the first steps towards treatment success lies in the ability to retain the clients to treatment completion, as those who do not complete treatment are unlikely to derive its maximum benefits. For those who stay, it is crucial to address effectively the individual risk and need factors that are assessed shortly after imprisonment. Specific responsivity factors are understood as barriers to effective treatment and ones that have to be considered — and sometimes to be overcome first — to work on the underlying risk and need factors (Bonta & Andrews, 2017). Our hypotheses that perceived self-efficacy, as well as attachment-related anxiety and avoidance, are associated with both treatment attrition and change in the assessed risk of reoffending, could not be confirmed by the results of this study. However, our analyses found that age, criminal history and interpersonal facets are predictive of treatment attrition, and previous unemployment and substance abuse are predictive of risk change. In the following section, we will discuss our results in the context of intramural treatment and the RNR model.
Association with Treatment Attrition (Research Question I)
The results of our study show that neither the levels of perceived self-efficacy nor adult attachment styles before treatment are significantly associated with the risk of treatment attrition in this sample of men sentenced for sexual offenses. Our hypothesis based on the RNR model (Bonta & Andrews, 2017) and previous research, that clients with lower perceived self-efficacy are less likely to complete treatment (Marshall et al., 2008; Sturgess et al., 2016) could not be confirmed. Regarding adult attachment styles, the current state of research is ambiguous as to whether attachment-related anxiety and avoidance hinder or support treatment completion (Smith et al., 2010); in our study, none of the two attachment dimensions predicted treatment attrition. Furthermore, the univariate comparisons between Completers and Non-Completers show that our findings differ from those of previous studies that found high levels in both ECR-R dimensions in individuals with sexual offense histories (Lyn & Burton, 2004, 2005; Marsa et al., 2004): neither the mean scores of attachment-related anxiety nor avoidance are substantially higher than those of the norm sample (Ehrenthal et al., 2009), and Completers and Non-Completers exhibit nearly the same scores.
Nevertheless, the SothA-HH seems to focus its resources on those who should receive the most intensive treatment according to the risk principle of the RNR model (Bonta & Andrews, 2017). The SothA-HH mainly detains clients sentenced for sexual offenses with a moderate to high assessed risk of reoffending, and furthermore retains most of the high-risk/high-need clients in treatment. However, it is a known dilemma that those with greatest need for treatment often do not complete it (cf. Brunner et al., 2019; Jewell & Wormith, 2010; Olver et al., 2011; Sewall & Olver, 2019): in the present study, one fifth of the participants discontinued the diverse forms of treatment offered, and left the therapeutic community of the SothA-HH.
Although this noncompletion seems to be independent of the clients’ pre-treatment perceived self-efficacy and adult attachment style, we could replicate other significant factors relating to treatment attrition (Brunner et al., 2019; Jewell & Wormith, 2010; Olver & Wong, 2009, 2011): First, men who do not complete treatment tended to be younger than those who completed treatment, and increasing age is revealed as a significant protective factor regarding treatment attrition. As we know from previous research, age has not only been discussed as a demographic risk factor (Brunner et al., 2019; Olver & Wong, 2009) but also as a stage-of-life responsivity factor, representing variations in developmental maturity (Bonta & Andrews, 2017; Higley et al., 2019): A lack of maturity and ability to understand the need to change antisocial behavior and thus avert the detrimental effects on their future, could be understood as a barrier to effective treatment. Second, with an increasing number of prior convictions, the risk of treatment attrition increases. Third, Non-Completers score higher on all four facets of the PCL-R which is in line with previous findings indicating the association of interpersonal and affective facets, an impulsive lifestyle, and antisocial behavior with treatment attrition (e.g., Brunner et al., 2019; Olver & Wong, 2009). However, our main analyses show that the interpersonal facet is the only significant predictor within the PCL-R facets for treatment attrition. Superficial charm and a grandiose sense of self-worth, as well as pathological lying and manipulative behavior can be challenging for others and therefore harmful to establishing meaningful relationships with others, and developing strong therapeutic alliances. In contrast, potential “faking good” tendencies of the clients (if presented) do not seem to show success: Despite deceptive-manipulative characteristics, the clients do not retain in the SothA-HH but are transferred to regular prison. Wong and Olver (2015) discuss interpersonal and affective facets as important responsivity factors, and underline the need to carefully maintain treatment motivation and engagement to prevent treatment attrition.
In terms of the risk principle, age, number of prior convictions and psychopathic traits can be interpreted as risk factors that are difficult (or impossible) to change. Beyond that, they can also be interpreted as responsivity factors and thus as barriers that can be overcome when taken into account as part of correctional treatment. Thus, the results of our study illustrate once again how important it is to do the utmost to encourage the clients to remain until treatment completion, to individually adjust treatment intensity and style, and therefore to enhance the clients’ ability to derive the maximum therapeutic benefit from intramural treatment.
Association with Change in Dynamic Risk Factors (Research Question II)
Neither perceived self-efficacy nor adult attachment styles prior to treatment are significantly associated with the change in the assessed risk of reoffending in a sample of men sentenced for sexual offenses. Nevertheless, two of the risk factors we controlled for were significant predictors of assessed changes in the Stable-2007 scores: During SothA-HH detention, unemployment prior to conviction is a predictor of less therapeutic progress regarding the assessed risk of reoffending. Unexpectedly, a history of substance abuse diagnosis is linked to higher changes in the assessed risk of reoffending.
In line with former findings, where employment instability was predictive of recidivism (Hanson & Morton-Bourgon, 2005; Olver et al., 2011), unemployment prior to incarceration reveals as a hindering predictor of effective intramural offender treatment, and increases the assessed risk of reoffending. It might be that those individuals unable to hold down a job will probably show similar problems in a highly-structured and hierarchical facility such as a social-therapeutic facility that demands regular attendance, the acceptance of rules and authority, integration into a team or group, and displays of pro-social behavior. Treatment approaches based on the Good Lives Model would focus on employment to equip individuals with the capabilities to achieve outcomes that the majority of society consider desirable and beneficial (Ward et al., 2007). The importance of employment is moreover underpinned by a recent study stressing employment as a protective factor in terms of reducing the risk of sexual recidivism (Yoon et al., 2018).
Furthermore, lifetime mental and behavioral disorders due to psychoactive substance use reveals as a supportive predictor, and is associated with a decrease in the assessed risk of reoffending. We see two possible explanations for this unexpected finding, ones which are not investigated in this study: First, it can be hypothesized that alcohol/drug issues are addressed by means of a social-therapeutic facility and within the various forms of offense-specific as well as general, offense-unspecific treatment. Second, it might be that clients with alcohol/drug issues receive more intensive treatment than those without due to participating in some extra groups meant for people suffering from addictions; this would be in line with the risk principle and therefore increase treatment effectiveness (Bonta & Andrews, 2017).
Finally, for less than half of the Completers who participated in the pre- and post-testing, a reduction of the Stable-2007 scores was assessed. (Marques et al., 2005) found that even among completers of relapse-prevention programs for people who committed sexual offenses, there are meaningful differences based on which participants were assessed as having met program goals: individuals who “did not get” the treatment show higher recidivism rates than those who did. In a recent meta-analysis, (Gannon et al., 2019) indicate the impact of numerous program variables on treatment effectiveness (e.g., adhering to RNR principles, treatment by qualified psychologists, treatment intensity). In our sample, it might be assumed that there were differences in participation and progress between the groups of completers who showed decreases, no change, or increases in assessed dynamic risk. Because of the rather small sample size and due to not assessing program variables, it is not possible to make any inferences about what those differences might be. These should be considered in future studies.
Perceived Self-Efficacy and Adult Attachment Styles — Critical Appraisal and Outlook
We investigated if pre-treatment perceived self-efficacy and adult attachment styles are two factors that might explain why social-therapeutic treatment does not impact all high-risk/high-need clients to the same extent. Neither the mean values of the GSE (Schwarzer & Jerusalem, 1995; German version: Schwarzer & Jerusalem, 1999) nor of the ECR-R scale (Fraley et al., 2000; German version: Ehrenthal et al., 2009) in the participants of our study are substantially different from those of the norm samples. Furthermore, Completers and Non-Completers in our study reveal nearly the same scores with regard to both questionnaires. Finally, neither scale predicts treatment completion nor changes in the assessed risk of reoffending. In the following, we will discuss several reasons for these findings as well as implications for future research in terms of handling these issues.
With regard to perceived self-efficacy, we could not underline the results of former forensic studies where perceived self-efficacy is understood as a central point in treatment and a crucial factor with regard to reducing the risk of relapse after treatment (Hall, 1989; Pollock, 1996; Sturgess et al., 2016; Tozdan et al., 2015). The assumed positive effect of self-efficacy is especially supported by preparatory programs for people with histories of sexual offenses that build on strengthening self-efficacy to prepare the clients for their actual treatment of risk and need factors (Marshall et al., 2008). One issue of our study might be that, contrary to Tozdan et al. (2015) or Brezina and Topalli (2012), the GSE assesses general and not specific perceived self-efficacy. Thus, the participants in our study were not asked about their beliefs as to whether or not they could remain in treatment until the end and change specific risk factors (e.g., pedophilic interests), but whether or not they could manage general problems on their own, which might be a major difference. Consequently, future studies should investigate if (a) intramural treatment (also) changes the clients’ perceived self-efficacy and (b) if a change in perceived self-efficacy might be related to risk reduction and therefore to a positive legal prognosis after treatment (e.g., Hall, 1989; Marshall et al., 2008; Pollock, 1996; Tozdan et al., 2018), whereby (c) a distinction between specific and general self-efficacy is essential.
In line with this, even though the ECR-R is widely-used for assessing attachment styles in a variety of areas for scientific studies (e.g., assessing patient-physician working alliances, research on substance misuse, or men who committed sexual offenses; Bennett et al., 2011; Lyn & Burton, 2004, 2005; Marsa et al., 2004; Marshall et al., 2018), the questionnaire actually aims to assess romantic attachment. As previous research emphasizes, the attachment patterns can vary greatly depending on the reference person (Asendorpf, 2018; Caron et al., 2012). Additionally, the clients’ attachment styles not only influence the relationship to the therapist but also to the other members of the therapeutic group (Jennings et al., 2021; McKillop et al., 2016; Rom & Mikulincer, 2003; Sonkin & Dutton, 2003). Nevertheless, it is still open to question whether or not the use of the ECR-R is appropriate to capture the relationship to the therapist and other members of the therapeutic group in forensic settings. Furthermore, it should be investigated, if (a) the attachment styles change at all as a result of intramural treatment, (b) if the clients may solely learn how to adapt their behavior towards an appropriate attachment style without real, long-lasting changes, or (c) if the treatment is not useful when it comes to inducing change.
With regard to the inconsistent findings of former researchers, future studies should also investigate as to whether or not it is actually appropriate to increase perceived self-efficacy and “normalize” attachment-related anxiety and avoidance (in the sense of bringing it to an average level) in order to enhance treatment motivation and commitment to finally achieving the treatment goals in forensic settings (Bandura, 2012; Bennett et al., 2011; Marshall et al., 2018; Smith et al., 2010; Vancouver & Purl, 2017). A recent pilot-study on 50 men convicted of sexual offenses found that relationship-focused group therapy can have a significant positive impact on insecure attachment as a barrier to engage in correctional treatment (Jennings et al., 2021). Furthermore, responsivity factors were found to have a cumulative effect: The more responsivity issues clients show, the less likely they are to benefit from treatment (Hubbard & Pealer, 2009; O’Brien & Daffern, 2016). Initial findings regarding the relationship between self-efficacy and attachment-related anxiety/avoidance have already been published (e.g., Brenk-Franz et al., 2018; Fraley et al., 2000, 2011; ; Marshall et al., 2018; Neumann et al., 2007). Thus, it might be revealing to investigate the interactions between each of these factors and to examine their cumulative effect in future studies.
A further issue regarding our research design might be that we investigated if the pre-treatment levels of specific responsivity factors are decisive for treatment success (e.g., the higher the pre-treatment self-efficacy, the better the treatment outcome) in a rather general manner. This is one general limitation of the responsivity principle and how it has been largely investigated: most research focuses on the characteristics of the individual, and not on the consideration as to how the interventions should be tailored for that person. The results of our study, as well as the ambiguous state of research, indicate that an individual consideration of the various responsivity factors within every single treatment might be crucial (e.g., if the practitioners tailor the treatment to the individual level of self-efficacy of each client). Some exemplary studies that have already addressed some additions in terms of treatment programs are those by Wong and Olver (2015) for people with mental disorders, by Sewall and Olver (2019) for callous-unemotional features of high psychopathy clients, or by Marshall et al. (2008) within their preparatory program for clients with sexual offense histories. In future studies it might therefore be worthwhile to investigate whether or not relevant specific responsivity factors are taken into account by practitioners with regard to treatment tailored to the individual.
Limitations and implications for future research
The current study underlines the importance of investigating the role of responsivity factors as predictors of treatment outcomes in future studies, and elucidates possible pitfalls in studies about responsivity factors and treatment changes. Beyond the above-mentioned possible reasons for our non-significant findings with regard to the addressed possible responsivity factors, we will discuss several notable general limitations of our study that could additionally contribute to a better interpretation of the results.
In correctional facilities, there is a great heterogeneity in terms of the clients’ nationalities, spoken languages and skills in the official language. Sixteen percent of the total sample had to be excluded from the main analyses because of missing questionnaire data (mainly due to insufficient German language skills) which limits the generalizability of the results. The findings can therefore only be generalized for the German-speaking majority, but not for the total population of inmates with a history of sexual offenses in social-therapeutic facilities. This could be problematic as cultural differences in perceived self-efficacy and attachment styles have been discussed (e.g., Mastrotheodoros et al., 2015; Scholz et al., 2002). Beyond that, the motivation for participating in psychological testing, interviews and the treatment offered can vary greatly between individuals. In our sample, 35% (or 41 out of 118) of the pre-tested participants were not willing to participate in the follow-up testing. Both language skills and treatment motivation are responsivity factors (Bonta & Andrews, 2017; Harkins & Beech, 2007; Olver et al., 2011) that need to be better investigated in future research, and addressed in treatment programs. We also interpret the rather moderate variance explanation in both of the regression models as indicators to investigate further variables that might affect treatment effectiveness.
A further limitation of this study is that we were not able to collect data about the individual reasons for a transfer from the SothA-HH to a regular prison. Based on our experience, we have determined treatment attrition to be a negative treatment outcome. This might be problematic as there are many reasons for incarcerated clients and staff quitting treatment or ask for transfer to another facility — some reasons are not necessarily indicative of treatment failure. Furthermore, we were not able to collect change score information for the Non-Completers, which is why we cannot include them in our change analyses. From this general exclusion of Non-Completers, a bias in the findings (towards positive changes in the assessed risk of reoffending) could result that cannot be estimated. This is still a widely-discussed problem in forensic field research and, in contrast to strictly-controlled clinical trials, it cannot be addressed in this field study.
Conclusion and Outlook
Specific responsivity factors are individual characteristics that are not directly targeted in correctional treatment as risk factors but can hinder the participants’ responsiveness to treatment. Thus, a systematic and comprehensive consideration of responsivity factors is essential for the adequate planning, implementation and delivery of effective correctional treatment. Although responsivity is identified as the third core principle of the RNR model (Bonta & Andrews, 2017), research on this principle is still somewhat scarce (i.e., Bonta & Andrews, 2017; Cohen & Whetzel, 2014; Jung & Dowker, 2016).
The results of our study neither underline the findings of previous studies on self-efficacy nor do they resolve the former contradictory research findings on adult attachment styles. Overall, the results of our study, as well as the ambiguous state of research in general, indicate that a general investigation of pre-treatment levels of specific responsivity factors might not be decisive with regard to treatment success, but whether relevant specific responsivity factors are taken into account by practitioners within the individually tailored treatment. From a therapeutic perspective, it can still be argued that, in order to keep a client in treatment and to work on the underlying risk and need factors, it could be helpful to identify (among many other factors) the individual levels of self-efficacy, attachment-related anxiety and avoidance, and tailor treatment accordingly. Thus, studies that investigate whether or not taking these individual factors into account has a significant influence on the progress and outcomes of intramural treatment would be (a) an important step in terms of clarifying which individual factors of the clients are the key responsivity factors and (b) crucial to concretize the well-established RNR model with regard to how practitioners and clinicians should consider responsivity principles in their daily work.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is part of the research project “Evaluation of the social-therapeutic correctional facility Hamburg” which is funded by the Authority of Justice of the Free and Hanseatic City of Hamburg, Germany. ES was supported by a PhD scholarship of the Cusanuswerk.
Authors’ Note
The authors take responsibility for the integrity of the data, the accuracy of the data analyses, and have made every effort to avoid inflating statistically significant results. The authors would like to thank the team of the social-therapeutic correctional facility in Hamburg for the well-established collaboration. Furthermore, we thank our former colleagues and present cooperation partners Dahlnym Yoon and Martin Rettenberger for their efforts according to this research project. The authors also thank Marianne Ruhnau for data entry and giving helpful feedback on an earlier version of this article. The authors finally thank all participants for their willingness to participate in our study.
Author Contributions
ES, FB, and PB designed the study. ES and FB collected the data. ES analyzed and interpreted the data in consultation with FB and PB. ES wrote the initial draft of the manuscript in constant consultation with FB. All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of data analyses. All authors have contributed to, read, and approved the final version of the manuscript.